
Abstract

S
In this study, we present a case of a patient with metastatic MTC with somatic testing demonstrating RET M918T mutation by commercial assay. The variant allele frequency (VAF) was 38%. The patient was previously treated with vandetanib (2 months, discontinued for progressive disease), cabozantinib (8 months, discontinued for progressive disease and intolerance) and later treated with selpercatinib on a clinical study. Selpercatinib therapy resulted in partial response and was continued for 12 months, well tolerated, and ultimately discontinued for progressive disease.
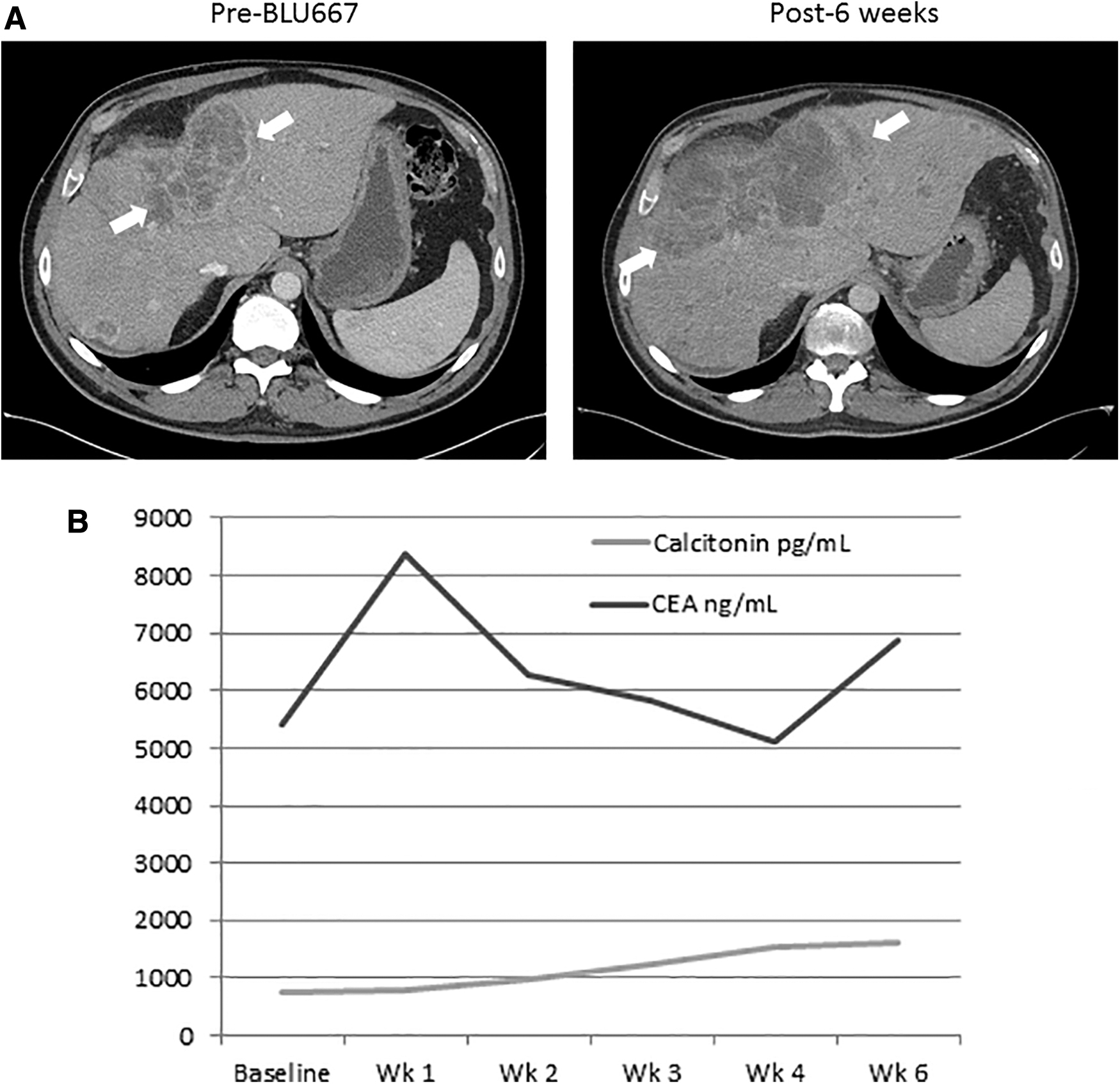
He was counseled on further therapy, including cytotoxic chemotherapy versus salvage therapy with another selective RET inhibitor. He agreed to the latter and signed an informed consent form and successfully underwent screening and enrollment on a phase 1/1b study of pralsetinib. Initially, a clinical response was noted with improvement in both the patient's symptoms and liver metastases on physical examination. However, six weeks after initiating therapy he showed sudden and rapid deterioration in his symptoms with worsening liver metastases on imaging consistent with progressive disease (Fig. 1A). The tumors markers showed mixed changes (Fig. 1B). Next-generation sequencing from a tumor biopsy obtained at enrollment (post-selpercatinib and pre-pralsetinib) demonstrated RET M918T (VAF 28%), RET V804M (22%), RET G810S (11.9%), and CDKN2A loss of heterozygosity in addition to this original RET mutation (RET M918T; VAF 38%). Both RET V804M and RET G810S have been shown to be resistant clones that emerge during selpercatinib or other MKI therapy (2 –4). Both selpercatinib and pralsetinib have inhibitory activity against RET V804M; therefore, the observed clinical resistance could be mediated by the newly emergent RET G810S mutation (2).
(
In this study, we demonstrate emergence of resistant clones in MTC during highly selective RET inhibitor therapy. Most importantly, the clinical course of this particular patient suggests subsequent highly selective RET inhibitor therapy may not be efficacious in all MTC patient previously treated with another highly selective RET inhibitor. Based on the preclinical studies and clinical experience published so far, RET G810S appears to be a gatekeeper mutation and thus unlikely to respond to further highly selective RET inhibitor therapy. Additional clinical experience from ongoing trials hopefully will inform us more definitively. While we await these data, clinicians should be observing patients closely for progressive disease with symptom assessment and cross-sectional imaging. Repeat somatic testing for assessment of gatekeeper mutation may be considered.
Footnotes
Author Disclosure Statement
A.V.C. reports funding for clinical trials from Kura Oncology, Inc., and Eisai, Inc., (institutional) and serves on advisory board for Kura Oncology, Inc., (institutional). J.Y.B. and K.C.B. have no relevant financial disclosures.
Funding Information
No funding was received for this article.