
Abstract
Introduction:
Thyroid lobectomy reduces risks of surgical complications and need for levothyroxine (LT4). We aimed at identifying the clinical course and risk factors for postlobectomy hypothyroidism to optimize surgical counseling and management in pediatric patients undergoing lobectomy.
Methods:
Clinical and biochemical presentations pre- and postlobectomy were retrospectively reviewed for 110 patients who underwent thyroid lobectomy between 2008 and 2020 at the Children's Hospital of Philadelphia.
Results:
Approximately 28.2% of patients (31/110) developed postlobectomy hypothyroidism defined by an elevated thyrotropin (TSH) level, including 24.5% (27/110) with subclinical hypothyroidism (TSH >4.5 and <10.0 mIU/L) and 3.6% (4/110) with overt hypothyroidism (TSH >10.0 mIU/L). LT4 was initiated in 12.7% (14/110) of cases. Most patients (81.6%; 84/103) recovered euthyroidism within 12 months postlobectomy. When excluding patients with autonomous nodule(s), median preoperative TSH was 1.09 (interquartile range [IQR] = 0.70–1.77) mIU/L and 1.80 (IQR = 1.02–2.68) mIU/L in euthyroid and hypothyroid patients, respectively, with multivariate logistic regression confirming the association between an increased preoperative TSH and postlobectomy hypothyroidism (odds ratio = 1.8 [confidence interval 1.08–3.13], p = 0.024). Of the patients who underwent thyroid lobectomy and developed postoperative hypothyroidism (n = 31), 38.7% (12/31) had a preoperative diagnosis of an autonomously functioning thyroid nodule.
Conclusions:
Thyroid function should be evaluated postlobectomy to assess the need for LT4. LT4 should be considered if the TSH remains elevated, especially if an upward trend is observed or TSH is >10.0 mIU/L. Suppressed preoperative TSH associated with autonomous nodules is an independent risk factor for postlobectomy hypothyroidism.
Introduction
Thyroid lobectomy, or hemithyroidectomy, is a routinely performed operation that involves removing half of the thyroid gland. Lobectomy is generally recommended for unifocal nodular disease with benign or indeterminate cytology, autonomous nodule(s), and low-risk differentiated thyroid cancer (1 –5). With increased recognition of the benefits of thyroid lobectomy in reducing risks of surgical complications and need for lifelong thyroid hormone replacement with levothyroxine (LT4) compared with total thyroidectomy, the decision to pursue this procedure, as the optimal surgical approach, is expanding in clinical care (1 –6).
While patients should retain normal thyroid function after lobectomy, 15–30% of adults report the development of postlobectomy hypothyroidism (7 –11). An increased risk of hypothyroidism after lobectomy has been reported in patients with elevated preoperative serum thyrotropin (TSH), anti-thyroglobulin antibody, and/or anti-thyroid peroxidase antibody concentrations as well as patients with lymphocytic infiltration within the thyroid gland on postsurgical pathology (7,8,12 –14).
Despite reports evaluating the incidence of and risk factors for the development of postlobectomy hypothyroidism in adults, there are limited data addressing postlobectomy hypothyroidism in children and adolescents. Long-term consequences of LT4 noncompliance exist in pediatrics as in adults, including weight gain, fatigue, neuropsychiatric symptoms, and an increased risk for cardiovascular disease (12), with further concern over the potential negative impact on linear growth in pediatric patients post-thyroidectomy. Therefore, identifying pediatric populations best suited for lobectomy over thyroidectomy is an area of interest and an important addition to optimize care.
In this study, we report the incidence and clinical course of postoperative thyroid function tests (TFTs) in patients who underwent thyroid lobectomy at the Children's Hospital of Philadelphia (CHOP). Pre- and postsurgery TFTs were reviewed to (i) determine the number of patients requiring thyroid hormone replacement, (ii) identify the period of recovery for the remaining gland to achieve normal thyroid hormone production, and (iii) identify the risk factors for postlobectomy hypothyroidism. The goal of the study is to enhance the understanding of the risk for postlobectomy hypothyroidism to identify opportunities to improve preoperative counseling and management.
Materials and Methods
A retrospective chart review of patients who underwent thyroid lobectomy at CHOP between 2004 and 2020 was performed. The case list was cross-referenced with the CHOPs Thyroid Center clinical registry, yielding a total of 176 patients. Sixty-six patients were excluded from the study due to the following: completion thyroidectomy performed within 12 months from lobectomy (n = 25), lack of postoperative thyroid function studies (n = 21), thyroid lobectomy performed over 19 years of age (n = 7), prescription of LT4 after lobectomy while euthyroid and asymptomatic (n = 7), or diagnosis of Hashimoto's thyroiditis and/or prescription of LT4 before surgery (n = 6). A final cohort of 110 patients younger than 19 years of age at the time of thyroid lobectomy between January 2008 and December 2020 was included in the data analysis (Fig. 1).
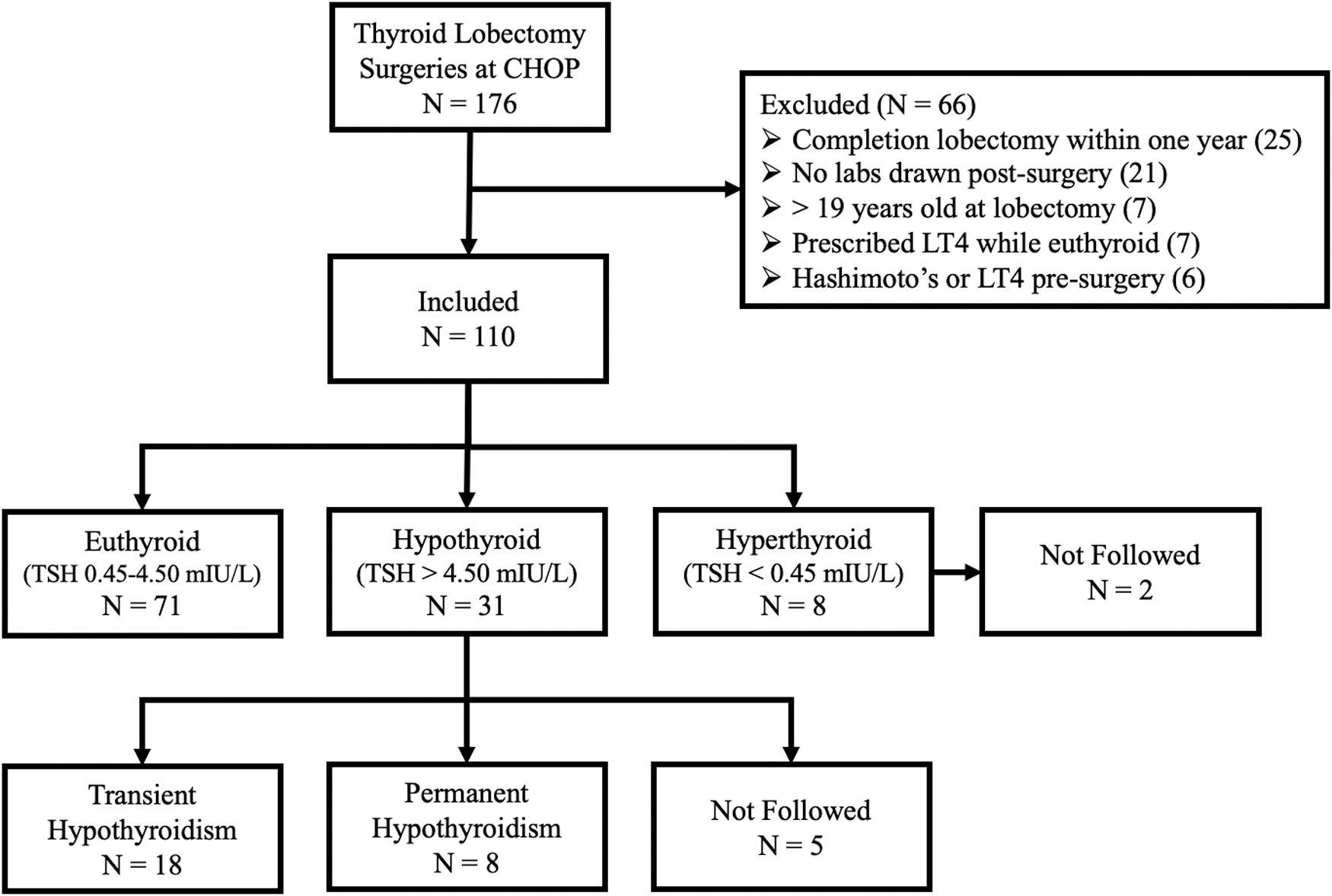
Study flowchart.
The electronic medical records were searched to collect and analyze information pertaining to patient demographics, previous medical history, and clinical and biochemical presentations pre- and postlobectomy. Preoperative and postoperative thyroid function analyses, including serum TSH concentration, total and free thyroxine (fT4) concentration, total and free triiodothyronine (fT3) concentration, anti-thyroglobulin, and anti-thyroid peroxidase, were recorded, if available. The TFTs were performed at CLIA-certified laboratories and evaluated based on insurance capitation and proximity to the patient's home or primary care institution. Thyroid ultrasound (US), fine-needle aspiration cytology, and surgical pathology reports were recorded and reviewed.
Patients were categorized as euthyroid, subclinical hypothyroid, overt hypothyroid, or hyperthyroid according to their postoperative serum TSH concentrations. Euthyroidism was defined as TSH levels within the reference range 0.45–4.5 mIU/L throughout follow-up care. Hyperthyroidism, subclinical hypothyroidism, and overt hypothyroidism were defined as TSH levels less than 0.45 mIU/L, within 4.51–10.0 mIU/L, and above 10.0 mIU/L, respectively, at any point during follow-up care.
Transient hypothyroidism was defined as a temporary elevated TSH (>4.5 mIU/L) with recovery of normal thyroid hormone production within 12 months of lobectomy. Permanent hypothyroidism was defined as a persistent elevated TSH without recovery of normal thyroid hormone production throughout follow-up care and/or initiation of LT4 replacement therapy secondary to postlobectomy overt hypothyroidism to achieve postoperative euthyroidism. Thyroid hormone replacement was prescribed to patients with a TSH >10.0 mIU/L or a TSH that remained >4.51 mIU/L for more than 12 months after lobectomy. Duration of follow-up was defined as the time between thyroid lobectomy and last clinic appointment and/or thyroid function evaluation.
Statistical analyses were run in R 4.0.5 and R Studio 1.4.1106 by using packages tidyverse, ggpubr, plotrix, and rstatix. Data with parametric distributions are reported as mean ± standard deviation, and data with nonparametric distributions are reported as median (interquartile range [IQR] = Q1–Q3). Clinical features between euthyroid and hypothyroid patients were compared by using Mann–Whitney U and Welch's two-tailed t-test for nonparametric and parametric data, respectively. Categorical variables were compared by using two-tailed Fisher exact test.
Univariate logistic regression was performed to determine the influence of clinical features on the development of postlobectomy hypothyroidism as well as the association between autonomous nodule status and preoperative TSH. Statistically significant variables (p < 0.05) in univariate analysis were included in multivariate logistic regression for the development of postlobectomy hypothyroidism, and results are reported with odds ratios (ORs), confidence intervals (CI), and p-values. Proportion of patients with postlobectomy hypothyroidism between all patients and excluding patients with autonomous nodule(s) were calculated and compared for patients with preoperative TSH values ≤0.45 mIU/L and >0.45 mIU/L by using two-tailed Fisher exact test. p-Values <0.05 were considered statistically significant.
This retrospective study involving human subjects was reviewed and approved by the Children's Hospital of Philadelphia Institutional Review Board (CHOP IRB #17-014224). Written informed consent from the participant and/or participant's legal guardian was not required per CHOP IRB; a waiver of consent/parental permission has been approved per 45 CFR 46.116(d).
Results
Patients who underwent thyroid lobectomy
In this study, 94 females and 16 males between 4 and 19 years of age, with a mean age of 14.9 ± 2.5 years, underwent thyroid lobectomy at CHOP (Table 1). The diagnosis that led to thyroid lobectomy included indeterminate cytology of nodule(s) (n = 43), diagnosis of an autonomous nodule (n = 33), elective intervention (n = 30; increase size of a nodule/22 and elective discontinuation of surveillance/8), nondiagnostic cytology of nodule(s) (n = 2), and malignant cytology of nodule(s) (n = 2). The median duration of follow-up care in our cohort was 12 months (1–62 months), with a median duration between thyroid lobectomy and initial TFT at 5.6 weeks (0.9–74.6 weeks).
Demographic and Clinical Features of Patients Who Underwent Thyroid Lobectomy (N = 110)
Development and incidence of postlobectomy hypothyroidism
After thyroid lobectomy, 71 patients (64.5%) remained euthyroid, 27 patients (24.5%) had subclinical hypothyroidism (TSH >4.5 and <10.0 mIU/L), 8 patients (7.3%) had hyperthyroidism (TSH <0.45 mIU/L), and 4 patients (3.6%) had overt hypothyroidism (TSH >10.0 mIU/L). Of the patients who underwent thyroid lobectomy and developed hypothyroidism, 38.7% of patients (12/31) had a preoperative diagnosis of an autonomously functioning thyroid nodule (Table 2). Hypothyroid patients presented with TSH elevation between 0.5 and 26 months, with a median time frame of 1.7 months. Nine of the 31 patients (9/31, 29.0%) presented with elevated serum TSH concentrations within 1-month postsurgery, 10 patients (10/31, 32.3%) within 2-months postsurgery, 8 patients (8/31, 25.8%) within 12-months postsurgery, and 4 patients (4/31, 12.9%) beyond 12-months postsurgery (Fig. 2).
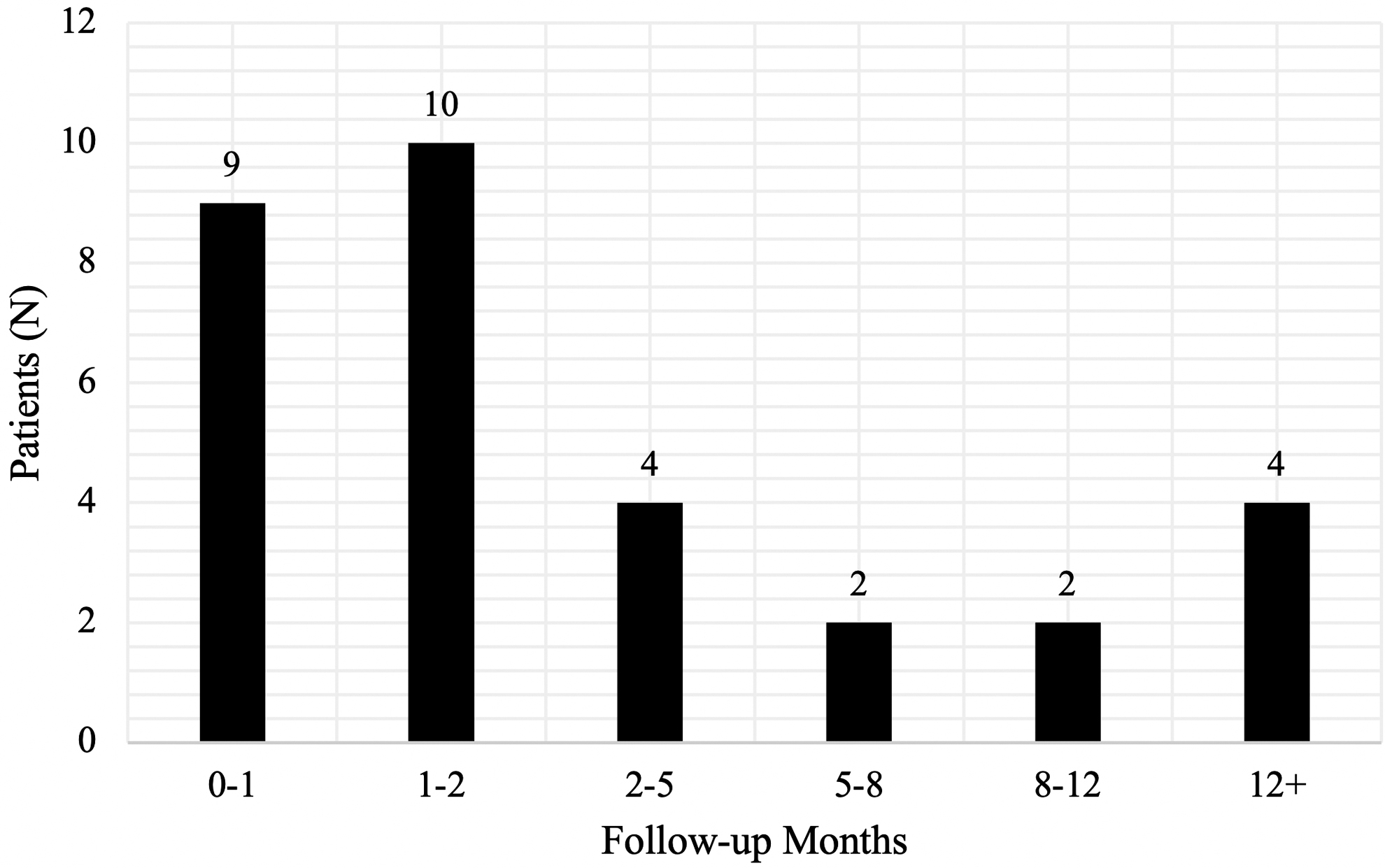
Time between thyroid lobectomy and the development of postoperative hypothyroidism (N = 31).
Comparison of Clinical Features Between Euthyroid and Hypothyroid Patients Including and Excluding Those with Autonomous Thyroid Nodules
p-Value <0.05 using Mann–Whitney U for nonparametric continuous variables and two-tailed Fisher's exact test for categorical variables.
Welch's two-tailed t-test for parametric continuous variables. Refer to the Materials and Methods section for additional information.
BMI, body mass index; IQR, interquartile range, SD, standard deviation; TSH, thyrotropin.
Ultimately, 17.5% of patients (18/103) were diagnosed with transient hypothyroidism, including 12.6% of patients (13/103) recovering to euthyroidism within 12 months after lobectomy and 4.9% of patients (5/103) recovering to euthyroidism after 12 months after lobectomy. Patients with transient hypothyroidism presented with elevated TSH for a median duration of 1.0 month (1–22 months) and achieved euthyroidism at a median of 7.5 months (1–36 months) after lobectomy (Fig. 3). Approximately 7.8% of patients (8/103) had permanent hypothyroidism after lobectomy. The remaining five patients in the hypothyroid group had one set of labs performed at CHOP within the first month after surgery and were surveilled thereafter by a local institution (Fig. 1).
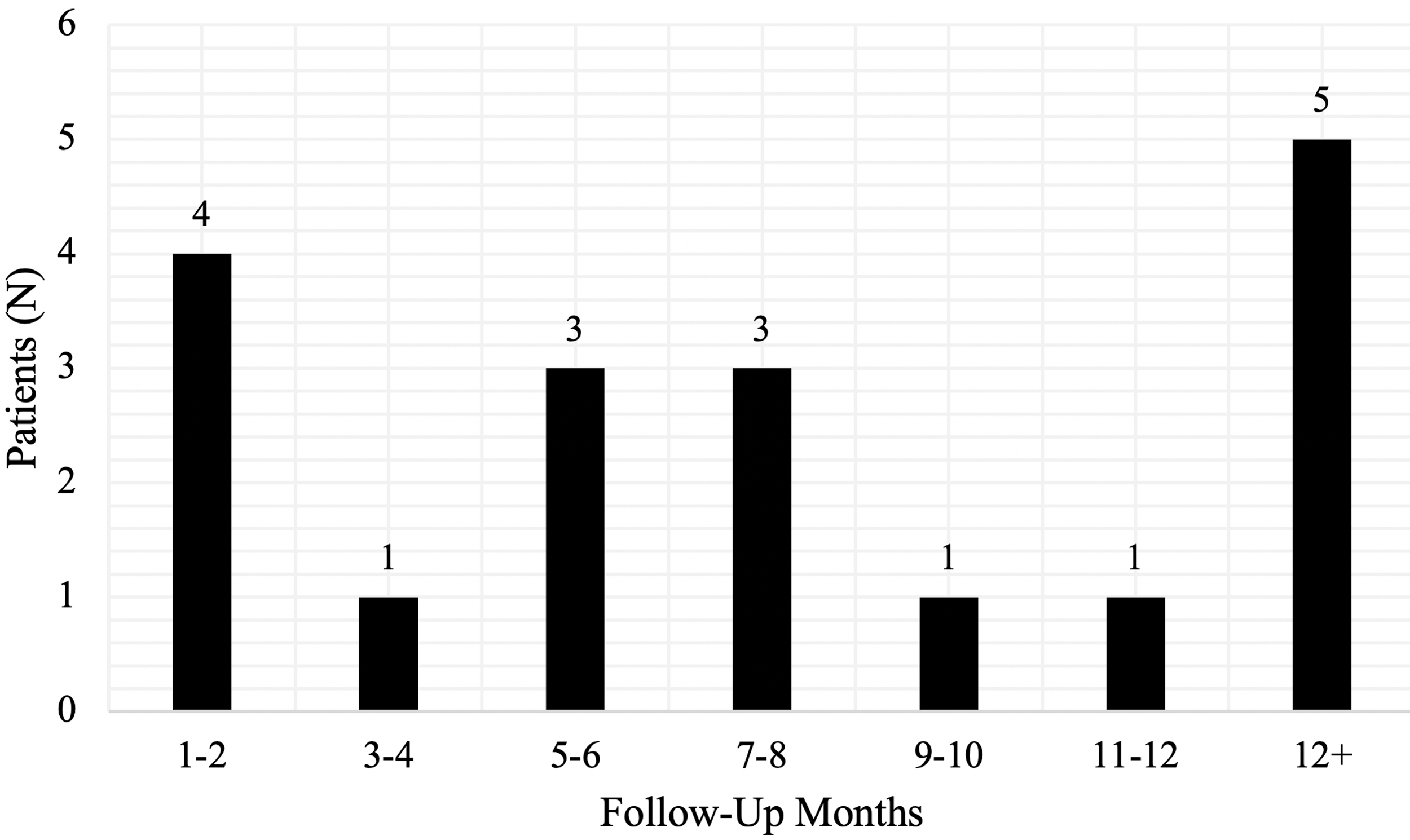
Time between thyroid lobectomy and recovery of normal TSH production (N = 18). TSH, thyrotropin.
Of the eight patients who had TSH <0.45 mIU/L after lobectomy, five patients had a persistent suppressed TSH associated with a preoperative diagnosis of an autonomously functioning nodule, two patients were unexpectedly found to have a mildly suppressed TSH on postoperative laboratory assessment but were lost to follow-up at CHOP based on chart-review, and one patient presented a suppressed TSH and subsequently converted to euthyroidism during follow-up care.
Treatment of postlobectomy hypothyroidism
Fourteen of the 110 patients (12.7%) were treated with thyroid hormone replacement, with the majority prescribed LT4 within the first month after surgery (Table 1). Ten of 14 patients (71.4%) were prescribed LT4 within 1-month postsurgery, 2 patients (14.3%) within 12-months postsurgery, and 2 patients (14.3%) beyond 12-months postsurgery. Approximately 42.6% of patients (6/14) discontinued thyroid hormone replacement at 5 months (n = 2), 8 months (n = 1), 13 months (n = 1), 16 months (n = 1), and 37 months (n = 1) after lobectomy and maintained a TSH level in the normal range after discontinuation of LT4.
Risk factors for the development of postlobectomy hypothyroidism
Analysis of clinical features of patients who remained euthyroid (n = 71) compared with those who developed postlobectomy hypothyroidism (n = 31) at any point during follow-up care revealed a significant difference in nodule dimension on preoperative US. Mean nodule dimensions were 2.73 ± 1.32 cm for euthyroid patients and 3.42 ± 1.49 cm for hypothyroid patients (p = 0.033; Table 2). Large nodule dimension on US was significantly associated with the development of postlobectomy hypothyroidism in univariate analysis (OR = 1.4 [CI = 1.04–1.98], p = 0.028).
Twelve of the 31 patients who developed postlobectomy hypothyroidism were diagnosed with an autonomously functioning thyroid nodule, with a mean nodule dimension of 3.53 ± 1.71 cm. No additional associations were identified between euthyroid and hypothyroid patients, including the previously published risk factors of sex, age, body mass index, family history of hypothyroidism, autonomous nodule(s), surgical pathology, and weight of resected thyroid tissue (Table 2).
Median preoperative TSH levels were 0.92 (IQR = 0.50–1.41) mIU/L for euthyroid patients and 0.99 (IQR = 0.01–2.06) mIU/L for hypothyroid patients; a comparison of medians between euthyroid and hypothyroid patients revealed no significant difference (Mann–Whitney U, p = 0.985; Table 2). However, autonomous nodules were significantly associated with a suppressed preoperative TSH in univariate logistic regression (OR = 0.1 [CI = 0.03–0.25], p < 0.001).
In light of these results, a comparison of clinical features between postlobectomy euthyroid patients (n = 55) and hypothyroid patients (n = 19) excluding those with autonomous nodules (n = 28) was performed. When excluding patients with autonomous nodules, preoperative serum TSH concentration and nodule size recorded at US presented significant differences in distribution between euthyroid and hypothyroid groups (Table 2).
Univariate analysis revealed an association between a high preoperative TSH concentration and the development of postlobectomy hypothyroidism (OR = 1.9 [CI = 1.11–3.10], p = 0.019), which was confirmed by multivariate analysis (OR = 1.8 [CI = 1.08–3.13], p = 0.024). The association of large nodule size and postlobectomy hypothyroidism was significant in univariate analysis (OR = 1.5 [CI = 1.02–2.26], p = 0.041) but not in multivariate analysis (OR = 1.4 [CI = 0.87–2.11], p = 0.173). No additional associations were identified between postoperative hypothyroidism and previously mentioned risk factors in this group.
Based on these observations, preoperative serum TSH concentration was stratified into two groups, TSH ≤0.45 mIU/L and TSH >0.45 mIU/L, to assess the proportion of patients with postlobectomy hypothyroidism before and after the exclusion of patients with autonomous nodules. The proportion of patients who developed postlobectomy hypothyroidism with preoperative serum TSH concentrations ≤0.45 mIU/L was observed to be higher in the inclusion group while patients who developed postlobectomy hypothyroidism with preoperative serum TSH concentrations >0.45 mIU/L did not differ based on autonomous nodule inclusion (Fig. 4). However, patients with preoperative TSH concentrations ≤0.45 and >0.45 mIU/L revealed no significant differences on the proportion of patients who developed postlobectomy hypothyroidism between the inclusion and exclusion of patients with autonomous nodules (p = 0.370; p = 1.000; Fig. 4). These findings suggest that suppressed TSH in the context of autonomously functioning thyroid nodules may be an independent risk factor for the development of postlobectomy hypothyroidism.
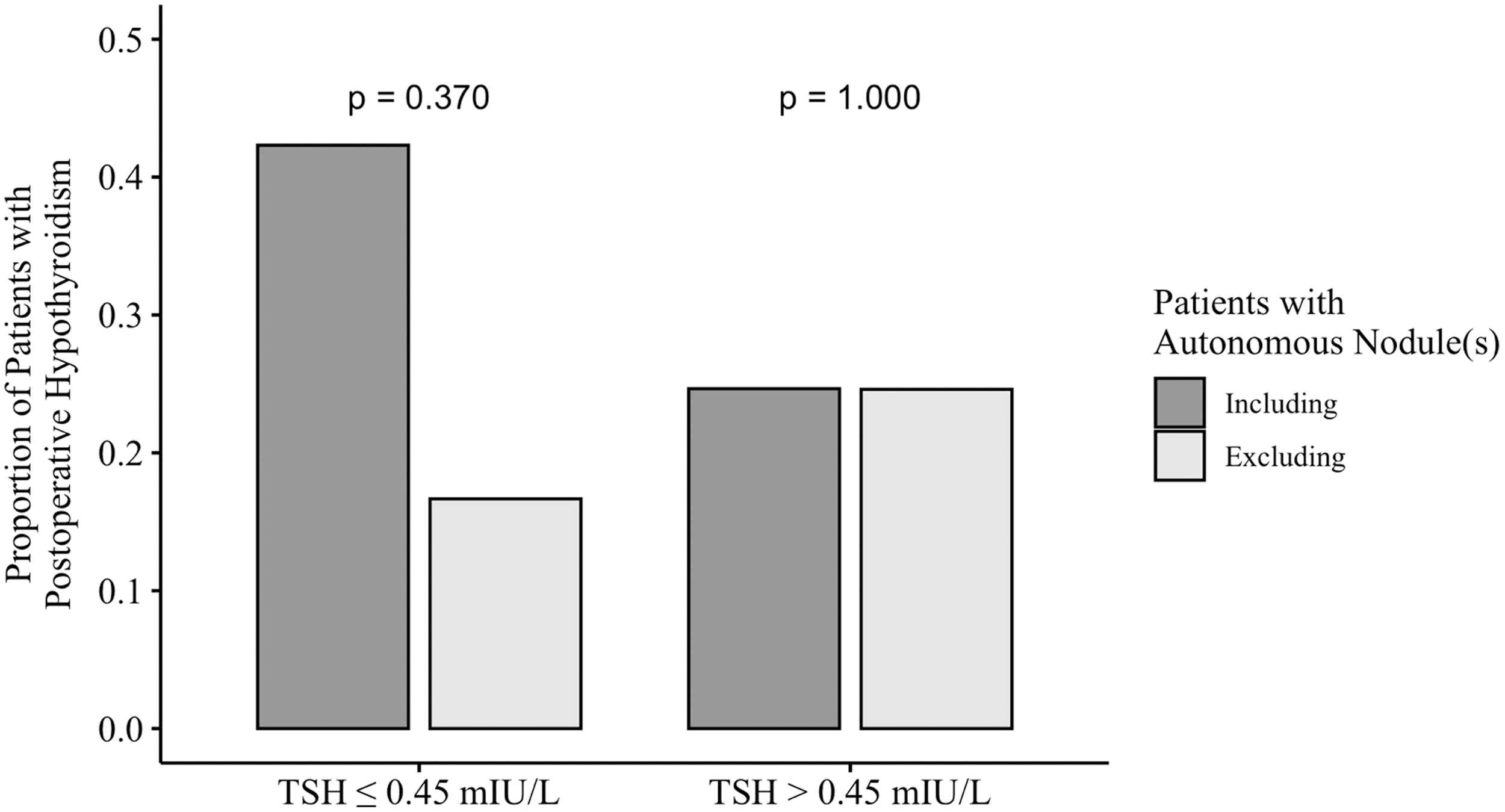
Proportion of patients with postlobectomy hypothyroidism stratified based on the preoperative TSH group before and after the exclusion of patients with autonomous nodule(s). The proportion of patients who developed postlobectomy hypothyroidism with preoperative serum TSH concentrations ≤0.45 and >0.45 mIU/L before and after the exclusion of patients with autonomous nodule(s) by two-tailed Fisher's exact test (p = 0.370 for patients with TSH ≤0.45 mIU/L; p = 1.000 for patients with TSH >0.45 mIU).
Discussion
Our study assessed the prevalence and clinical risk factors for developing hypothyroidism after thyroid lobectomy in patients <19 years of age at the time of surgery. Previous studies were limited to the development of postlobectomy hypothyroidism in an adult population or comprised smaller pediatric cohorts, with only one pilot study evaluating long-term thyroid function after lobectomy in 43 children and adolescents (1,6,8,9,12,15). In the present study, 28.2% of patients (31/110) developed hypothyroidism defined by a serum TSH concentration above the upper limit of the normal range after thyroid lobectomy.
Approximately 17.5% of patients (18/103) exhibited transient hypothyroidism, with the majority of patients (72.2%; 13/18) achieving euthyroidism within the first 12 months after thyroid lobectomy (Fig. 3). The overall incidence of postlobectomy permanent hypothyroidism was 7.8% (8/103). This observation is consistent with previous reports (16 –18). Long-term LT4 replacement therapy postlobectomy was indicated in 12.7% of cases (14/110) in this cohort as defined by a TSH >10.0 mIU/L or a TSH that remained >4.51 mIU/L for more than 12 months after lobectomy (Table 1).
Our findings corroborate a previous report identifying 25.6% of pediatric patients developing elevated serum TSH concentration after lobectomy, with 16.3% of the 43 patients ultimately requiring LT4 replacement therapy (7,12). Published reports in adult patients demonstrate a broad incidence of postlobectomy hypothyroidism, with a range from 11% to 43% (7,12,14,16,19). Our results suggest that for the majority of patients the development of hypothyroidism in the early postoperative stages in pediatric patients likely represents a transient state involving a compensatory adjustment in the hypothalamic-pituitary-thyroid axis to the resection of one lobe rather than a permanent state of hypothyroidism (7,19).
Previous studies have shown that postoperative hypothyroidism typically develops between 3.2 and 4.3 months after lobectomy, providing support for the compensatory adjustment of the thyroid axis (1,12,19). Nevertheless, our observation that 7.8% of patients (8/103) did not recover normal thyroid hormone production during the period of this review warrants recognition and underscores the importance of establishing guidelines for monitoring thyroid function in pediatric patients postlobectomy, particularly for patients who present risk factors for developing postlobectomy hypothyroidism.
In our study, a higher preoperative TSH level was independently associated with the development of postlobectomy hypothyroidism by univariate and multivariate analysis when excluding patients with autonomous nodules. However, while previous studies have demonstrated correlations between preoperative TSH and the development of postlobectomy hypothyroidism, the clinical utility of this observation remains in question based on the majority of preoperative TSH levels being in the mid-normal range, including TSH levels of 1.5 mIU/L (6), 1.7 mIU/L (1), 2.0 mIU/L (10, 19), and 2.2 mIU/L (12).
As we observed postoperative hypothyroidism in patients with preoperative TSH throughout the entire normal range (0.45–4.5 mIU/L), it appears unlikely that a mild variation of TSH within the normal range serves as a useful, independent clinical predictor of postlobectomy hypothyroidism in the pediatric population.
Patients with postlobectomy hypothyroidism presented significantly larger nodules on US before surgery than euthyroid patients when including and excluding patients with autonomous nodules (Table 2). Although the association between nodule dimension and postlobectomy hypothyroidism was confirmed by univariate and multivariate analysis in the inclusion of all patients, the association was confirmed only by univariate analysis when patients with autonomous nodules were removed from the analysis, identifying autonomous nodules and suppressed TSH associated with autonomously functioning thyroid nodules as the most significant factors associated with a high risk for developing postlobectomy hypothyroidism.
Thirty percent (30%) of our patients (33/110) underwent thyroid lobectomy for treatment of an autonomous nodule, with 38.7% of patients (12/31) developing postlobectomy hypothyroidism and 21.2% of patients (7/33) requiring long-term LT4 replacement therapy. Thus, autonomous thyroid nodules associated with suppressed preoperative TSH appear to be a clinically significant risk factor for patients developing postlobectomy hypothyroidism who ultimately require LT4 therapy.
This observation is likely due to suppression of the contralateral lobe from the autonomous nodule associated with impaired recovery of the remaining thyroid lobe after lobectomy (3). Based on the results from our study, it is recommended that patients with suppressed preoperative TSH pursuing definitive surgical treatment for autonomous nodules be counseled on the increased risk for developing postlobectomy hypothyroidism.
When thyroid hormone replacement is initiated promptly after the presentation of hypothyroidism, the opportunity for the gland to spontaneously recover thyroid function may be confounded. Hypothyroidism after thyroid lobectomy if left untreated, however, may impair linear growth and neurocognitive development in children and adolescents (12,20 –23). With this in mind, while the minority of pediatric patients will develop permanent hypothyroidism after lobectomy, 7.8% for patients with a normal TSH before surgery and 21.2% for patients with an autonomous nodule in our study, to ensure early diagnosis we recommend a laboratory assessment of thyroid function (TSH and T4) four to six weeks after thyroid lobectomy for pediatric patients (2).
To minimize the potential for unnecessary LT4 administration, patients with serum TSH concentrations above the upper limit of normal range are recommended to continue thyroid function monitoring every two to three months to determine whether TSH remains elevated or normalizes. LT4 replacement therapy should be considered for patients with a TSH above the upper limit of normal range 6 to 12 months after lobectomy, especially for patients with a TSH >10 mIU/L. LT4 therapy to target the TSH in the low normal range (≤1.0 mIU/L) should also be considered for patients who undergo lobectomy for resection of a thyroid nodule with surgical pathology revealing a thyroid cancer with low-invasive potential (i.e., minimally invasive follicular thyroid cancer and encapsulated follicular variant papillary thyroid cancer) (4,24,25).
Our study is limited by its retrospective design, the variable information in medical records, and in the variation in approach to thyroid hormone monitoring and LT4 replacement inherent to clinical practice. In addition, in our cohort, the incidence of postoperative hypothyroidism may be underestimated secondary to early initiation of thyroid hormone replacement (n = 14) due to concerns for potential negative impact on growth and development as well as the relatively short duration of follow-up (range 1–62 months, median 12 months).
Consequently, because of limited data, we did not analyze preoperative antithyroid antibody concentrations or lymphocytic-infiltration grade in the thyroid surgical specimen, features that have been previously resolved to predict postlobectomy hypothyroidism (26,27). While TFTs were evaluated at CLIA-certified laboratories, assay methods used throughout the study period varied and may possess differing coefficients of variation and functional sensitivities.
Nevertheless, this comprehensive review describes the largest cohort of pediatric patients postlobectomy from a single institution and presents important data that should lead to improved presurgical counseling as well as postsurgical monitoring and management of pediatric patients who undergo thyroid lobectomy. Variance in health care delivery has improved with the deployment of our electronic health records to include access to partnering institutes (Epic Care Everywhere) as well as the formation of an organized Thyroid Center at our institute since 2010.
In conclusion, the majority of pediatric patients (81.6%; 84/103) who undergo lobectomy will achieve euthyroidism within 12 months after surgery. Patients with suppressed TSH from autonomous nodules are at an increased risk of developing postlobectomy hypothyroidism that would benefit from LT4 replacement therapy. Thyroid function should be assessed 4–6 weeks after lobectomy and then every 2–3 months up to 12 months after surgery for patients with a TSH concentration in the subclinical range (>4.5 and <10.0 mIU/L).
If TSH remains in the subclinical range at 12 months or displays an increasing trend, LT4 therapy should be considered. A shorter length of observation with initiation of LT4 should be pursued for patients with a TSH in the overt range (>10.0 mIU/L) after lobectomy.
Footnotes
Authors' Contributions
K.K. and A.J.B. devised the project. J.A.B. collected the data and wrote the article with support and critical review by A.J.B., K.K., S.M.M., N.S.A., and S.H. S.H. and J.A.B. performed the analysis and created the tables and figures. All authors discussed the results and provided an editorial review of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported in part by the consortium grant from NIH R01CA21451 (Aime T. Franco) and The Children's Hospital of Philadelphia Frontier Program's Grant.