
Abstract
Background:
Sorafenib and lenvatinib are multikinase inhibitors (MKIs) approved for patients with radioactive iodine-refractory (RAI-R) differentiated thyroid cancer (DTC). There is no consensus on when to initiate MKI treatment. The objective of this study was to evaluate time to symptomatic progression (TTSP) in patients with RAI-R DTC for whom the decision to treat with an MKI was made at study entry.
Methods:
International, prospective, open-label, noninterventional cohort study (NCT02303444). Eligible patients had asymptomatic progressive RAI-R DTC, with ≥1 lesion ≥1 cm in diameter and life expectancy ≥6 months. The decision to treat with an MKI was at the treating physician's discretion. Primary endpoint was TTSP from study entry. Two cohorts were evaluated: patients for whom a decision to initiate an MKI was made at study entry (Cohort 1) and patients for whom there was a decision not to initiate an MKI at study entry (Cohort 2). Cohorts were compared descriptively.
Results:
The full analysis set (FAS) comprised 647 patients. The median duration of observation was 35.5 months (range <1–59.4). Of 344 MKI-treated patients, 209 received sorafenib, 191 received lenvatinib, and 19 received another MKI at some point. Median TTSP was 55.4 months (interquartile range [IQR] 18.6–not estimable [NE]) overall, 55.4 months (IQR 15.2–NE) in Cohort 1 (n = 169), and 51.4 months (IQR 20.0–NE) in Cohort 2 (n = 478). TTSP ≥36 months was achieved in 64.5% of patients overall, 59.5% of patients in Cohort 1, and 66.4% of patients in Cohort 2. Median overall survival from classification as RAI-R was 167 months and median progression-free survival from start of MKI therapy was 19.2 months and from start of sorafenib therapy 16.7 months. Among sorafenib-treated patients, 70% had dose modifications, 35% had a dose reduction, 89% experienced ≥1 treatment-emergent adverse event (TEAE), and 82% experienced ≥1 drug-related TEAE.
Conclusions:
This real-world study provides valuable insight into outcomes in patients with asymptomatic, progressive RAI-R DTC under observation or receiving MKI treatment. TTSP in the FAS provides insight into the current prognosis for patients with RAI-R DTC in the era of MKIs.
Registration:
NCT02303444.
Introduction
The mainstay of treatment for differentiated thyroid cancer (DTC) is surgical resection followed by treatment with radioactive iodine (RAI), depending on the level of risk for disease recurrence. 1,2 The prognosis of patients with DTC is generally favorable; however, some patients (5–10%) develop metastatic disease, two-thirds of whom become refractory to RAI therapy. 3 –5 Lack of response to RAI treatment is the strongest predictor of morbidity and mortality in patients with DTC. 6 Such patients, who have clinically significant structural disease progression during the last 6–12 months of RAI therapy, are candidates for systemic therapy. 1,5,7
Sorafenib and lenvatinib are oral multikinase inhibitors (MKIs) that target the vascular endothelial growth factor receptor, have activity against RAI-refractory (RAI-R) DTC, 1 and are approved to treat patients with RAI-R DTC. Sorafenib significantly improved median progression-free survival (PFS) in patients with locally advanced RAI-R DTC in the phase 3 DECISION trial. 8 Improved PFS was observed with sorafenib independent of age, sex, geographic region, histological subtype, site of metastasis, or tumor burden. 8 Lenvatinib also significantly extended PFS in the phase 3 SELECT trial in patients with RAI-R DTC. 9 Lenvatinib was associated with improved PFS in patients who had or had not previously received an MKI, and in patients with all histological types. Moreover, the presence of BRAF or RAS mutations did not modify the PFS benefit conferred by sorafenib in DECISION 8 or by lenvatinib in SELECT. 9
There is no consensus to when MKIs should be started in patients with RAI-R DTC. 1 In 2012, a panel of experts recommended that systemic therapy be considered when tumor burden is substantial (multiple lesions >1–2 cm) and tumor progression within <12 months is documented. 7 The American Thyroid Association (ATA) subsequently recommended consideration of MKI therapy in patients with RAI-R DTC with metastatic, rapidly progressive, symptomatic, and/or imminently threatening disease not amenable to other therapies. 1 More recently, the European Thyroid Association recommended that MKIs be considered in patients with progressive disease when refraining from treatment would lead to harm or clinical complications. 5 As symptomatic progression is associated with poor prognosis, it is critical to prolong time to progression in patients with RAI-R DTC.
The objective of this study was to evaluate the outcomes (primary outcome measure: time to symptomatic progression [TTSP]) in asymptomatic patients with progressive RAI-R DTC for whom the decision to treat or not to treat with an MKI at study entry was made in a real-life setting.
Methods
Study design and patients
RIFTOS MKI (Radioactive Iodine reFractory Asymptomatic Patients in Differentiated Thyroid Cancer - an Observational Study to Assess the Use of Multikinase Inhibitors; NCT02303444) was an international, prospective, open-label, noninterventional study of patients with RAI-R DTC.
Eligible patients had histologically/cytologically documented DTC with radiological progression preferably defined according to response evaluation criteria in solid tumors (RECIST) version 1.1. Patients were required to have no DTC symptoms, ≥1 lesion ≥1 cm in diameter (i.e., measurable disease), and a life expectancy of ≥6 months. The definition of RAI-R included patients who had (1) a lesion with no RAI uptake on a diagnostic or therapeutic whole-body post-RAI scan; (2) progression of lesions after ≥1 RAI treatments with ≥3.7 GBq (≥100 mCi) ≤16 months before enrollment despite iodine uptake on a post-RAI scan; or (3) received previous RAI treatments with a cumulative activity >22.2 GBq (≥600 mCi). Details of inclusion and exclusion criteria have been published previously. 10
The study was conducted in accordance with guidelines and regulations of the European Medicines Agency, the U.S. Food and Drug Administration, and local laws and regulations. The protocol was reviewed and approved by local independent ethics committees or institutional review boards where required. All patients provided informed written consent before enrollment.
Outcomes and assessments
Primary endpoint
The primary endpoint was to compare TTSP in patients for whom there was a decision to initiate MKIs at study entry (Cohort 1) with those for whom there was a decision not to initiate MKIs at study entry (Cohort 2) (Fig. 1). TTSP was defined as the time from initial visit to symptomatic progression. The initial visit was the point when progression was confirmed and the physician made the decision to treat (or not) with an MKI. Some physicians initiated MKI treatment at a subsequent visit; thus, the time of MKI initiation is not reflected in the TTSP calculation.

Treatment schema. aDefined as the date of study entry to the date of first symptomatic progression. DTC, differentiated thyroid cancer; MKI, multikinase inhibitor; RAI-R, radioactive iodine-refractory.
Patients who did not have symptomatic progression at the time of analysis were censored at the date of their last evaluable assessment. Symptomatic disease progression was defined as any sign, symptom, or outcome caused by DTC, including symptoms due to bone metastasis, respiratory symptoms, central nervous system events due to brain metastasis, bleeding due to a DTC lesion, local pain or discomfort due to a metastatic lesion, deterioration of general condition due to DTC, reduced mobility due to a metastatic lesion, or coincident death. 10
Secondary endpoints
Secondary endpoints included overall survival (OS) and PFS from various time points in the overall population, OS and PFS from the start of sorafenib treatment in the safety analysis set, and post-progression survival (time from the date of symptomatic progression to death from any cause). Disease progression was defined as radiological or clinical progression. Additional secondary endpoints included MKI treatment exposure (overall population), sorafenib treatment exposure in the safety analysis set, and safety, as assessed by treatment-emergent adverse events (TEAEs) in the safety analysis set (sorafenib-treated patients).
Statistical analysis
The full analysis set (FAS) comprised all patients who met all inclusion and exclusion criteria and had a decision to start or not to start MKI therapy. The MKI-treated population included all patients who received ≥1 MKI dose during the study. The safety analysis set included patients who received ≥1 dose of sorafenib during the study.
A propensity score approach was originally planned to minimize potential confounders and balance covariate patterns between the two cohorts. However, the number of events and the overlapping rate after propensity score matching at a second interim analysis were lower than anticipated; therefore, adequately addressing the primary study endpoint was deemed unlikely and propensity score modeling was not performed. No formal statistical tests or comparisons were performed. All variables were analyzed descriptively. Time to event data were described by Kaplan–Meier estimates.
Results
Patients
Between April 2015 and March 2020, 699 patients were screened for eligibility and 671 enrolled, 24 of whom were subsequently excluded from the FAS because they did not meet the necessary criteria (Fig. 2). Data from 647 patients from North America, South America, Europe, Asia, and the Middle East were included in the FAS at the cut-off date (July 24, 2020). This includes 169 patients (26%) who were recommended to initiate MKI treatment at study entry (Cohort 1) and 478 (74%) who were recommended not to start MKI therapy at study entry (Cohort 2) (Fig. 2).
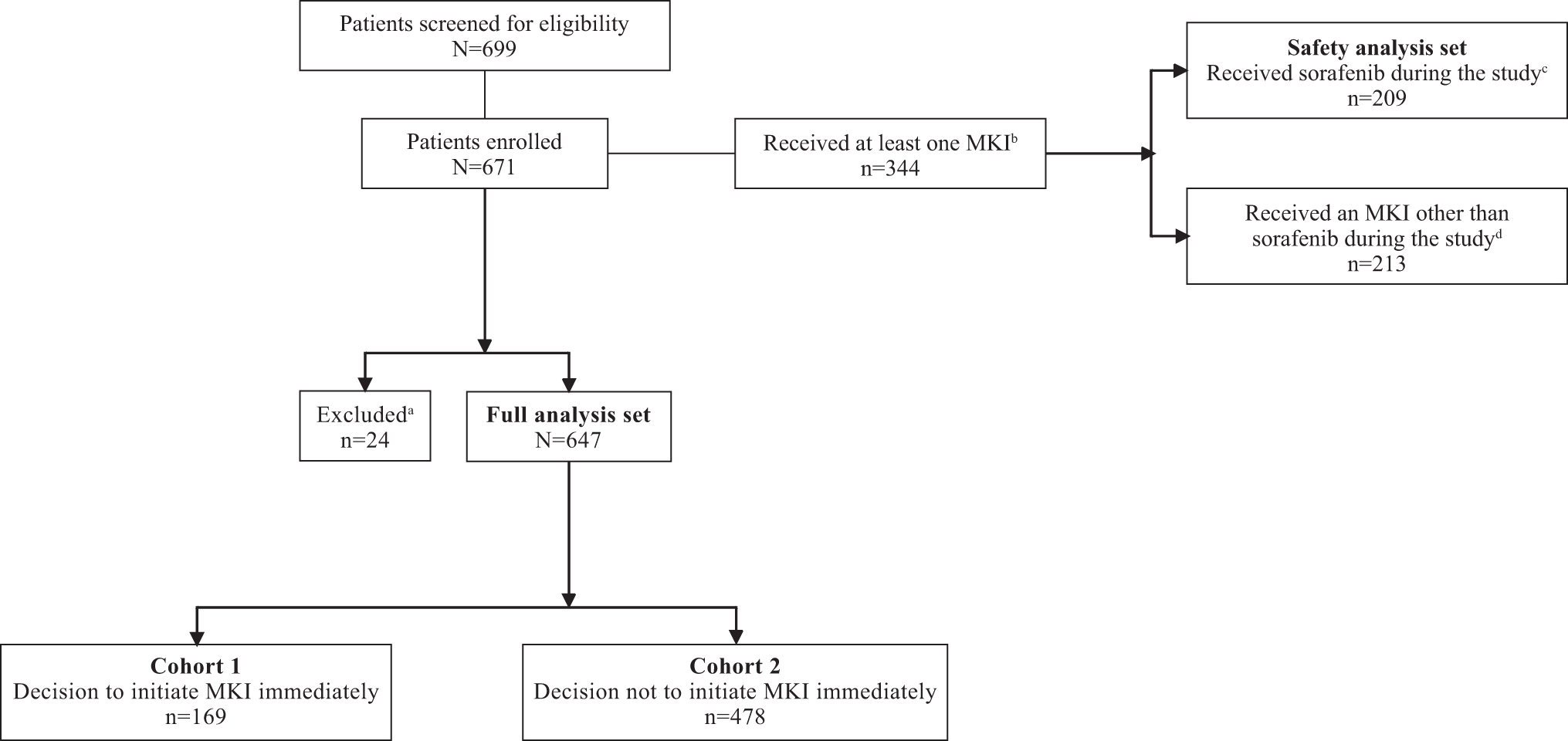
Patient disposition. aExcluded from the FAS based on final data checks. Twenty-four patients were excluded because during data review they were found to either meet exclusion criteria or did not meet the specified inclusion criteria. bSome patients received more than one MKI. cSeven patients were excluded from the FAS. dThree patients were excluded from the FAS. Eighty-one patients of 647 included in the FAS were lost to follow-up. FAS, full analysis set; MKI, multikinase inhibitor.
The median duration from the initial visit to the end of observation was 35.5 months (range <1–59.4). The median age of patients in the overall population was 67 years and 44% of patients were male (Table 1). Five hundred and five patients (78%) presented with concomitant diseases, with hypertension (45%), dyslipidemia (17%), and diabetes mellitus (16%) most frequently reported. The majority of patients (86%) had undergone total thyroidectomy before study entry.
Baseline Demographic and Disease Characteristics (Full Analysis Set)
Percentages may not total 100 due to rounding.
Multiple responses possible.
Location was specified for 646 patients.
ATA, American Thyroid Association; DTC, differentiated thyroid cancer; ECOG PS, Eastern Cooperative Oncology Group performance status; IQR, interquartile range; RAI, radioactive iodine; RAI-R, RAI-refractory.
At the time of initial diagnosis, 74% of patients had papillary histology; after surgery, 72% of patients had been classified as having intermediate or high risk of recurrence according to ATA criteria; at the initial study visit, 89% of patients had distant metastases (Table 1). The most common reason for being classified as RAI-R was no uptake of RAI (65%). The median number of prior RAI treatments was two, the median RAI activity was 4.72 GBq (127.6 mCi), and the median cumulative activity of RAI administered before the initial visit was 9.25 GBq (250.0 mCi) (Table 2). Of the 647 patients in the FAS, 157 (24%) died during the trial, 96 of whom were receiving an MKI. The most frequent primary reason for death was progressive disease (n = 96 [15%]; 71 were receiving an MKI) (Supplementary Table S1).
Prior Radioactive Iodine Treatment (Full Analysis Set)
IQR, interquartile range; RAI, radioactive iodine.
MKI treatment
Of 671 patients enrolled, 344 received ≥1 MKI during the study (Fig. 2): 209 received sorafenib and 210 received an MKI other than sorafenib (Table 3). Among patients treated with sorafenib, median duration of therapy was 475 days (range 1–1778) (15.6 months), the most common initial dose was 800 mg/day (66%), and the median of the average daily dose was 618 mg/day (range 176–800 mg/day) (Table 3). Sorafenib dose modifications were reported for 146 patients (70%). The most frequent reason for dose modifications was adverse events (AEs; n = 118, 56%). Seventy four patients (35%) had a dose reduction, with the majority (33%) due to AEs. One hundred and twenty patients discontinued sorafenib, reasons for which included disease progression (n = 52), AEs (n = 33), switch to other therapy (n = 14), withdrawal by subject (n = 9), death (n = 6), physician's decision (n = 3), hospice care (n = 2), and cost/reimbursement issues (n = 1).
Drug Exposure During the Study
All enrolled patients (N = 671). Seven patients who received sorafenib were excluded from the FAS.
FAS (N = 647).
FAS, full analysis set; MKI, multikinase inhibitor; SD, standard deviation.
Among lenvatinib-treated patients (n = 191), the median duration of therapy was 451 days (range 1–1739) (14.8 months) (Table 3). Of 191 patients, lenvatinib dose modifications were reported for 122 patients (64%) and could be attributed to more than one reason; the most frequent were toxicity (n = 101, 52.9%) and AEs (n = 28, 14.7%). Forty-one patients discontinued treatment with lenvatinib. Reasons for discontinuing lenvatinib included disease progression (n = 15), AEs (n = 16), switch to other treatment (n = 4), death (n = 3), and patient's decision (n = 3). For reasons for dose modification and discontinuation, toxicity was a predefined answer, while AE was derived from free-text entries if “other” was chosen.
The median time to MKI initiation was 7.0 days (interquartile range [IQR] 2.0–17.0) for Cohort 1 and 330.0 days (148.0–685.0) for Cohort 2. In Cohorts 1 and 2, 65% and 85% of patients received only one line of MKI treatment, respectively (Supplementary Table S2).
Efficacy
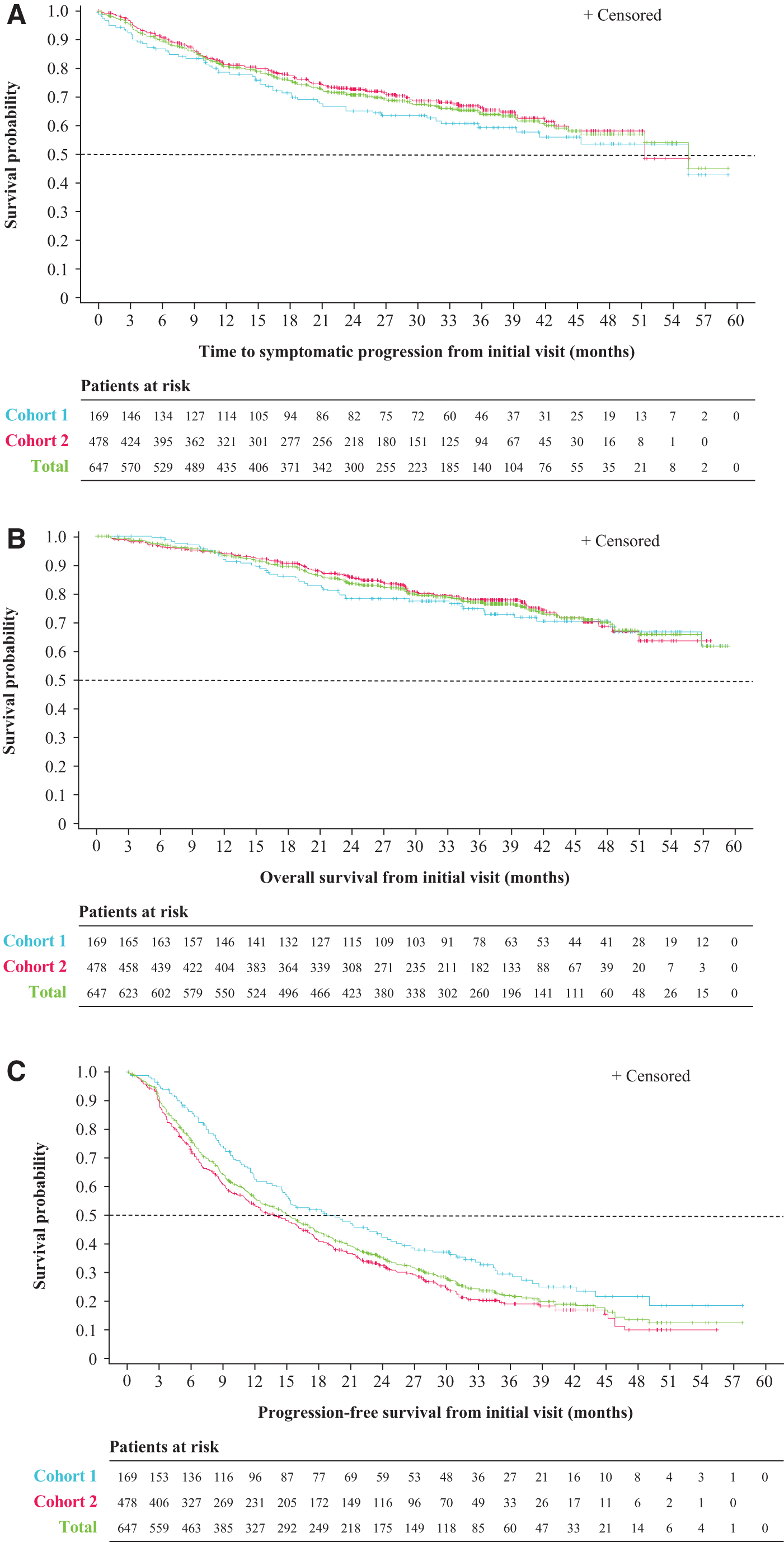
In the FAS (N = 647), approximately one-third of patients experienced symptomatic progression (n = 193); median TTSP from initial visit was 55.4 months (IQR 18.6–not estimable [NE]) and 64.5% of patients had a TTSP of 36 months or longer (Fig. 3A).
Kaplan–Meier curves for time to symptomatic progression (
Median TTSP from the initial visit was 55.4 months (IQR 15.2–NE) in Cohort 1 (n = 169) and 51.4 months (IQR 20.0–NE) in Cohort 2 (n = 478). A TTSP of 36 months or longer was achieved in 59.5% of patients in Cohort 1 and in 66.4% of patients in Cohort 2.
In patients with papillary histology (n = 476), median TTSP from initial visit was 55.4 months and 67.5% of patients had a TTSP of 36 months or longer, regardless of treatment with an MKI. In patients with follicular histology at initial diagnosis (n = 86), median TTSP from initial visit was 37.7 months and 59.6% of patients had a TTSP of 36 months or longer. Median TTSP by patient characteristics are presented for Cohorts 1 and 2 in Supplementary Table S3.
Median OS from the initial visit could not be estimated (Fig. 3B); however, the proportion of patients with an OS of 36 months or more from the initial visit was 77.1% (95% confidence interval [CI] 73.2–80.5%) in the FAS, 74.9% (CI 67.1–81.1%) in Cohort 1, and 77.8% (CI 73.1–81.8%) in Cohort 2.
Median PFS was 15.2 months (CI 12.6–17.1) in the FAS, 19.5 months (14.6–24.4) in Cohort 1, and 13.8 months (11.4–16.3) in Cohort 2 (Fig. 3C). A PFS of 36 months or longer was achieved in 22.1% of patients in the FAS, 29.7% of patients in Cohort 1 and in 19.2% of patients in Cohort 2. Median PFS is presented by patient characteristics for the FAS in Table 4 and for Cohorts 1 and 2 in Supplementary Table S4. Median interval from symptomatic progression to death from any cause was 28.4 months. In the FAS (N = 647), median OS from classification as RAI-R was 167 months (Supplementary Table S5).
Efficacy. Kaplan–Meier Estimates of Progression-Free Survival from Initial Visit in Selected Subgroups
CI, confidence interval; DTC, differentiated thyroid cancer; ECOG PS, Eastern Cooperative Oncology Group performance status; RAI, radioactive iodine; RAI-R, RAI-refractory; ROW, rest of world.
Kaplan–Meier estimates of other endpoints in the FAS are provided in Supplementary Table S5.
TEAEs: Safety analysis set (sorafenib-treated patients)
Among patients treated with sorafenib (n = 209), 89% experienced ≥1 TEAE and 82% experienced ≥1 drug-related TEAE (Supplementary Table S6). The most common TEAEs of any grade included diarrhea (44%), hand–foot skin reaction (HFSR, 41%), hypertension (26%), fatigue (25%), and alopecia (20%). Most drug-related TEAEs were judged to be Grades 1–3 in severity (Supplementary Table S6). There were 66 (32%) Grade 3 drug-related TEAEs and 4 (2%) Grade 4 drug-related TEAEs.
The most common Grades 3–5 drug-related TEAEs were hypertension (8.6%), HFSR (8.1%), fatigue (3.8%), anorexia (2.4%), and diarrhea (2.4%). Grade 5 AEs experienced by 19 patients (9%) included dyspnea (n = 2), hypoxia (n = 2), pleural effusion (n = 2), respiratory failure (n = 2), sepsis (n = 2), adult respiratory distress syndrome (n = 1), colonic hemorrhage (n = 1), conduction disorder (n = 1), multiorgan failure (n = 1), neoplasms (benign, malignant, and unspecified; n = 1), other gastrointestinal disorder (n = 1), sudden death not specified (n = 1), and other (not coded; n = 3).
TEAEs were not collected for patients treated with other MKIs.
Discussion
The results of this international, noninterventional, real-world study provide important insights into the real-world characteristics and rates of disease progression of patients with RAI-R DTC with measurable disease as defined as ≥1 lesion ≥1 cm in diameter. The population included in this study was representative of patients with RAI-R DTC and generally consistent with a prior analysis of 444 patients with metastatic DTC. 3
The profile of patients with RAI-R DTC in this study was generally similar to that in phase 3 studies of MKI therapies (i.e., age, histology, and metastases location) 8,9 ; however, patients with comorbidities were not excluded from RIFTOS MKI so it is likely that, as with all real-world studies, some would not have been eligible for the phase 3 studies. This is likely reflected in the incidence of death in this study (24% overall).
The original intention was to directly compare outcomes in two cohorts of patients (immediately and not immediately treated with an MKI); however, an interim analysis showed that it was unlikely that the comparison could be performed adequately because the accrual of events was slower than expected; therefore, no formal statistical comparisons were made. It is worth noting that of the 671 patients enrolled on the study meeting the eligibility criteria, only 344 (51%) received an MKI, indicating that there was a large proportion of patients for whom observation was still deemed an acceptable approach on the part of the treating physicians and their patients. This is due to several factors, including the fact that before use of MKIs, patients with RAI-R DTC were primarily referred for additional treatments on the basis of the presence of symptoms, which is unlikely for the majority of patients with measurable disease per RECIST, but overall low tumor burden.
Among patients for whom a decision to initiate MKI treatment at study entry was made, a TTSP and PFS of 36 months or longer was achieved in 59.5% and 29.7% of patients, respectively; among patients for whom a decision not to initiate MKI treatment at study entry was made, TTSP and PFS of 36 months or longer was reported in 66.4% and 19.2% of patients, respectively. The higher proportion of patients achieving a TTSP of 36 months or longer (with a longer median TTSP) than PFS in this study suggests that a subset of patients do not experience symptomatic progression.
Median OS from MKI start was not reached; the wide range in duration of OS from RAI-R classification and the inability to calculate median OS from MKI start indicate that RAI-R is a heterogeneous condition. Little data have been published on survival in patients with RAI-R DTC with or without treatment, and the limited data that are available are heterogeneous. The long-term study by Durante et al, which was conducted before the advent of MKI therapy, reported a 10-year survival rate in patients with metastatic DTC of 29% in patients with RAI uptake who did not achieve remission and 10% in patients who were RAI-R, defined as no RAI uptake. 3
PFS in this study compares well with the PFS obtained with MKI therapy in two large, randomized, phase 3 clinical trials. In the DECISION trial, median PFS was 10.8 months in patients treated with sorafenib 400 mg twice daily (n = 207) and 5.8 months with placebo (n = 210) (hazard ratio [HR] = 0.59 [CI 0.45–0.76]) after a median follow-up of 16 months. 8 In the SELECT trial, median PFS was 18.3 months in patients treated with lenvatinib 24 mg daily (n = 261) and 3.6 months with placebo (n = 131) (HR = 0.21 [99% CI 0.14–0.31]) after a median follow-up of 17 months. 9 In SELECT, median PFS was 15.1 months in lenvatinib-treated patients who had previously received an MKI (n = 66).
The safety and tolerability of sorafenib in this study were consistent with the known safety profile of sorafenib. The most common drug-related TEAEs were diarrhea, HFSR, and hypertension. HFSR was reported less frequently in this real-world study than it was in the phase 3 DECISION trial. In this study, HFSR (any grade) was reported in 41% of patients (Grade 3, 9%), whereas in DECISION, HFSR (any grade) was reported in 76% of sorafenib recipients (Grade 3, 20%), 8 which likely reflects improvements over time in the prevention and management of this AE. In the DECISION trial, the most common AEs were HFSR, diarrhea, alopecia, and rash/desquamation. 8
In this study, two-thirds of patients treated with sorafenib received an initial daily dose of 800 mg/day, which is the dose used in the phase 3 trials 8,11 –13 and the approved dosage for this indication. 14 Sorafenib dose reductions (33%) and withdrawals due to AEs (16%) were less frequent than in the phase 3 DECISION trial (64% and 19%, respectively). 8 A non-negligible rate of fatal AEs was reported (9%); this highlights how, given the long OS since RAI-R classification observed (roughly 14 years), the decision to start an MKI treatment should be carefully evaluated.
Limitations of the trial are typical of real-world, observational studies. The results cannot confirm when it is best to initiate treatment with an MKI in patients with asymptomatic, progressive RAI-R DTC. Selection bias would have influenced the timing of physicians' decisions to offer treatment to patients. For example, physicians may have offered MKI treatment sooner to patients who appeared less well or who had more rapid disease progression. Conversely, a patient's decision to accept treatment with an MKI may have been influenced by unknown factors that were not captured in the database. Furthermore, the development of new selective kinase inhibitors (e.g., RET and TRK inhibitors) might influence a patient's or physician's decision to proceed with treatment due to different safety profiles. For this reason, we cannot comment on any differences between cohorts in terms of observed PFS. The relatively short duration of follow-up precluded estimation of OS in this patient population.
Conclusions
This real-world study is, to our knowledge, the largest noninterventional study yet completed in patients with RAI-R DTC. It was not possible to conduct the analysis as originally planned because of the slow accrual of events. The study reported a median TTSP of 55.4 months from the initial visit, and, importantly, provides insight into the current prognosis for patients with RAI-R DTC who have measurable disease in the era of MKIs and targeted therapies. Larger, longer-term studies are required to address the impact of MKI treatment on OS in a real-world setting.
Footnotes
Authors' Contributions
All authors contributed equally to the development of this article and agreed to submit this article for publication.
Acknowledgments
The authors thank the patients in the RIFTOS study, their families and the RIFTOS investigators, and participating study centers. The study was sponsored by Bayer HealthCare. Editorial assistance in the preparation of this article was provided by Victoria Jones of OPEN Health Communications (London, UK), with financial support from Bayer.
Author Disclosure Statement
S.B. is employed by Bayer. L.L. has received payment of honoraria from Eisai and has participated on a data safety monitoring or advisory board with Eisai and Bayer. R.P.P. has had an unpaid leadership of fiduciary role in the Executive Committee for the European Society for Endocrinology. S.T. has received support for this article from Bayer, royalties or licenses, payment or honoraria for lectures, presentations, speakers bureaus, article writing or educational events, support for attending meetings and/or travel, participated on a data safety monitoring board or advisory board, stock or stock options, and other financial or nonfinancial interests. F.W. has participated on a data safety monitoring board or advisory board with Eisai, Bayer, Merck, and Exelixis. H.-J.T. has nothing to disclose. K.O. is employed by Bayer. D.W.B. has received payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events from Blueprint Medicines and Exelixis. S.-M.H. has nothing to disclose. C.-C.L. has received consulting fees from AbbVie, Bayer, Blueprint Medicines, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Merck, and Novartis, payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events from Eli Lilly, Novartis, and Roche, and support for attending meetings and/or travel from BeiGene, Daiichi Sankyo, and Eli Lilly. F.P. has received consulting fees from Bayer, Roche, and Biotoscana, payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events from Bayer and Biotoscana. I.S. has received grants or contracts from Bayer, payment or honoraria for lectures, presentations, speakers bureaus, article writing, or educational events from Eisai and Medtronic, participated on a data safety monitoring board or advisory board from Eli Lilly, Ono Pharmaceutical, and Takeda. J.W.A.S. has received support for this article from Bayer. P.R. has nothing to disclose. R.G. is employed by Bayer and received support for this article. M.A. received support for this article from Bayer. D.H.-Y.S. has received consulting/advisory fees and payment of honorarium from Bayer Taiwan, Eisai Taiwan, Roche Taiwan, and Lilly Taiwan. M.S.B. has received support for this article from grant funding (support provided to institution), and consulting fees, honoraria, and support for advisory board participation from Bayer, Eisai, and Exelixis. M.T. has received support for this article from Bayer.
Funding Information
This study was sponsored by Bayer. The sponsor worked with the principal investigators to design the study. Data collection and interpretation, and preparation of this article were performed by the investigators and the sponsor. Statistical analyses were performed by the sponsor. All authors and the sponsor approved the decision to submit the article for publication. The sponsor funded writing assistance.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6