
Abstract
Objectives:
Thyroid autoimmunity is common in pregnant women and associated with thyroid dysfunction and adverse obstetric outcomes. Most studies focus on thyroid peroxidase antibodies (TPOAbs) assessed by a negative–positive dichotomy and rarely take into account thyroglobulin antibodies (TgAbs). This study aimed at determining the association of TPOAbs and TgAbs, respectively, and interdependently, with maternal thyroid function.
Methods:
This was a meta-analysis of individual participant cross-sectional data from 20 cohorts in the Consortium on Thyroid and Pregnancy. Women with multiple pregnancy, pregnancy by assisted reproductive technology, history of thyroid disease, or use of thyroid interfering medication were excluded. Associations of (log2) TPOAbs and TgAbs (with/without mutual adjustment) with cohort-specific z-scores of (log2) thyrotropin (TSH), free triiodothyronine (fT3), total triiodothyronine (TT3), free thyroxine (fT4), total thyroxine (TT4), or triiodothyronine:thyroxine (T3:T4) ratio were evaluated in a linear mixed model.
Results:
In total, 51,138 women participated (51,094 had TPOAb-data and 27,874 had TgAb-data). Isolated TPOAb positivity was present in 4.1% [95% confidence interval, CI: 3.0 to 5.2], isolated TgAb positivity in 4.8% [CI: 2.9 to 6.6], and positivity for both antibodies in 4.7% [CI: 3.1 to 6.3]. Compared with antibody-negative women, TSH was higher in women with isolated TPOAb positivity (z-score increment 0.40, CI: 0.16 to 0.64) and TgAb positivity (0.21, CI: 0.10 to 0.32), but highest in those positive for both antibodies (0.54, CI: 0.36 to 0.71). There was a dose–response effect of higher TPOAb and TgAb concentrations with higher TSH (TSH z-score increment for TPOAbs 0.12, CI: 0.09 to 0.15, TgAbs 0.08, CI: 0.02 to 0.15). When adjusting analyses for the other antibody, only the association of TPOAbs remained statistically significant. A higher TPOAb concentration was associated with lower fT4 (p < 0.001) and higher T3:T4 ratio (0.09, CI: 0.03 to 0.14), however, the association with fT4 was not significant when adjusting for TgAbs (p = 0.16).
Conclusions:
This individual participant data meta-analysis demonstrated an increase in TSH with isolated TPOAb positivity and TgAb positivity, respectively, which was amplified for individuals positive for both antibodies. There was a dose-dependent association of TPOAbs, but not TgAbs, with TSH when adjusting for the other antibody. This supports current practice of using TPOAbs in initial laboratory testing of pregnant women suspected of autoimmune thyroid disease. However, studies on the differences between TPOAb- and TgAb-positive women are needed to fully understand the spectrum of phenotypes.
Introduction
Thyroid autoimmunity in pregnant women is associated with altered thyroid function and adverse obstetric outcomes (1 –5). Whether the latter arises from a general immune dysregulation or insufficient thyroid hormone production, or both, is uncertain. Because thyroid hormones regulate fetal development (1,6), maternal thyroid hormone physiology and metabolism change during pregnancy (7). This includes the pregnancy hormone human chorionic gonadotropin stimulating the thyrotropin (TSH) receptor to increase thyroid hormone production. Also, estrogen-induced increase in thyroxine (T4) binding globulin increases circulating total thyroxine (TT4) to 150% of prepregnancy levels by midgestation (7). Women with thyroid autoimmunity are less likely to meet the increased demands for thyroid hormone production during pregnancy (8).
Thyroid autoimmunity is the most common autoimmune aberration in women of reproductive age, with a prevalence up to 17% depending on population and cutoff for positivity (2,9). A distinction between thyroid peroxidase antibodies (TPOAbs) and thyroglobulin antibodies (TgAbs) is rarely applied and most studies focus on TPOAbs. Up to 95% of patients with Hashimoto's thyroiditis have circulating TPOAbs, making this the preferred laboratory marker for autoimmune hypothyroidism (10 –12). Thus, the American Thyroid Association' guidelines on thyroid and pregnancy recommend measurement of TPOAbs to assess thyroid autoimmunity (9). However, in some populations, TgAbs may be highly prevalent and could be an equally sensitive marker of thyroid dysfunction. Unuane et al. (13) found TgAbs associated with lower thyroid function in infertile women, with isolated TgAbs in 5% of the women. In a cohort of Danish pregnant women, the presence of either antibody was associated with higher TSH concentrations, however, only TgAb positivity was significantly associated with lower free thyroxine (fT4) concentrations (14,15). Positivity for both antibodies had the highest association with thyroid dysfunction (15). This was also the case in the First and Second Trimester Assessment of Aneuploidy Risk (FaSTER) trial of 9562 healthy pregnant women, finding higher TSH concentrations in TgAb-positive women than antibody-negative women, even higher in TPOAb-positive women, and highest in women positive for both (16).
Studies investigating the role of thyroid autoimmunity often focus on TPOAbs assessed by a dichotomous negative–positive distinction, which may be too simplistic. Korevaar et al. demonstrated a dose–response relationship of higher TPOAb concentrations with higher TSH in healthy pregnant women (17). Similarly, Ashoor et al. (18) found a higher proportion of healthy pregnant women with TSH above the 97.5th percentile among those positive for TPOAbs and TgAbs, respectively; this proportion increased with higher concentrations of either antibody (18).
Measurement of TPOAbs has been the preferred screening tool in the past decades and TgAb effects have remained understudied (9). Identifying a relevant role of TgAbs in pregnant women would lead to reconsideration of study designs, guidelines, and clinical practice.
We aimed to determine and quantify the effect of TPOAbs and TgAbs, respectively, and interdependently, on maternal thyroid function.
Materials and Methods
Participants
This study was a meta-analysis of individual participant cross-sectional data within the Consortium on Thyroid and Pregnancy, an international collaboration between cohorts with data on thyroid function in pregnant women (19). The Consortium cohorts were identified by a systematic literature search, invitations to participate through international peer-reviewed journals, and individual contacts (4). Cohorts with thyroid antibody measurements that participated in a study on birth weight (5) were invited as were three cohorts that subsequently joined the Consortium. All cohorts consented to this study. Briefly, studies of thyroid function and autoimmunity during pregnancy in the general population, or in cohorts without selection based upon patient subgroups, were included and individual participant data collected with a standardized codebook (5).
Participants with TPOAb or TgAb measurements, and TSH or fT4, measurements were eligible. Women with multiple pregnancy, pregnancy by assisted reproductive technology, history of thyroid disease, or use of thyroid interfering medication were excluded.
Laboratory analyses
All cohorts analyzed thyroid function and autoantibodies by immunoassays (Supplementary Table S1 provides assay specifications). To account for interlaboratory variation, all thyroid function measurements were standardized to cohort-specific z-scores (20 –23). The manufacturer cutoffs defined TPOAb and TgAb positivity (Supplementary Table S1). One exception was made in the Northern Finland Birth Cohort Study where the manufacturer cutoff was questioned why previous studies had used the 95th percentile of the cohort as cutoff (24,25).
Statistical analyses
Pooled prevalence estimates for thyroid antibody positivity were based on meta-analyses (R metafor package version 3.0-2 using a random effects model with the function rma.glmm).
For dichotomous analyses of antibody positivity versus antibody negativity, associations with TSH and fT4, respectively, were investigated for the following: (i) Women positive for both TPOAbs and TgAbs, (ii) women with isolated TPOAb positivity, and (iii) women with isolated TgAb positivity, compared with women negative for both antibodies. Differences were estimated by linear models with z-score of log-transformed thyroid variables as outcome within each cohort and estimates integrated in a meta-analysis.
The associations between continuous TPOAb and TgAb concentrations and cohort-specific z-scores of TSH, free triiodothyronine (fT3), total triiodothyronine (TT3), fT4, total thyroxine (TT4), and triiodothyronine (T3):T4 ratio were investigated in linear dose–response models with z-score as outcome and log2 antibody concentration as predictor. Because some women lacked information about exact concentrations below the cutoff, antibody concentrations below the cutoff were included as a binary predictor (Supplementary Fig. S1). The reported effect estimate was an increase in mean z-score per doubling of antibody concentration above the manufacturer's cutoff. The models were developed for each cohort and integrated in a final meta-analysis where cohort differences were accounted for by including random effects for all regression parameters in a linear mixed model.
Associations with TPOAbs and TgAbs were evaluated with and without mutual adjustment and with and without adjustment for potential confounders. To reduce model complexity and isolate the effect of the antibodies, we accounted for potential confounding factors by transforming outcomes to cohort-specific adjusted z-scores. Adjusted z-scores were derived from a linear model for the log-transformed outcome and included potential confounders: gestational age (linear), age (linear), body mass index (linear), fetal sex (0/1), smoking (0/1), and parity (0, 1, 2, 3+) if available. The model was based on data from antibody-negative pregnancies. Subsequently, z-scores were computed as “(observed-predicted)/residual_sd” where “observed” was the outcome on log scale and “predicted” was the predicted value from the linear model.
In the primary analyses, missing data for potential confounders were imputed by multilevel multiple imputation, creating five data sets for pooled analyses as previously described (4,26). Sensitivity analyses were as follows: complete case analyses, excluding outliers more than three standard deviations from the mean on log-scale, excluding the Northern Finland Birth Cohort, using the manufacturer's cutoff for the Northern Finland Birth cohort, excluding cohorts without TgAb-data, and using cohort-specific 95th-percentiles of antibody concentration as cutoff for antibody positivity.
To correct for multiple comparisons, p-values from primary analyses were Bonferroni adjusted, while the remaining p-values were adjusted according to Benjamini and Hochberg (27), which controls for false discovery rate. Adjusted p/q-value <0.05 was considered statistically significant. All statistical analyses and figures were made in R-version 3.6.3 (28).
Ethics
All cohorts adhered to the legal requirements of the participating countries, were approved by the local review boards, and acquired participants' informed consent unless exemption was granted by ethics committees. Data were treated according to the national data protection legislation.
Results
The final study population comprised 51,138 women, of whom 51,094 had data on TPOAbs and 27,874 on TgAbs (Fig. 1). Pooled prevalence estimates for antibody positivity were 9.1% for TPOAbs (95% confidence interval, CI: 7.9 to 10.3, range across cohorts: 5.0–13.8%) and 9.5% for TgAbs (CI: 6.2 to 12.8, range across cohorts: 4.3–16.6%). In the nine cohorts with measurements of both antibodies (n = 27,874), the pooled prevalence estimates for isolated TPOAb positivity were 4.1% [CI: 3.0 to 5.2], for isolated TgAb positivity were 4.8% [CI: 2.9 to 6.6], and positivity for both antibodies 4.7% [CI: 3.1 to 6.3]. Supplementary Figure S2 illustrates the correlation between TPOAbs and TgAbs, with correlations ranging from 0.25 to 0.46.
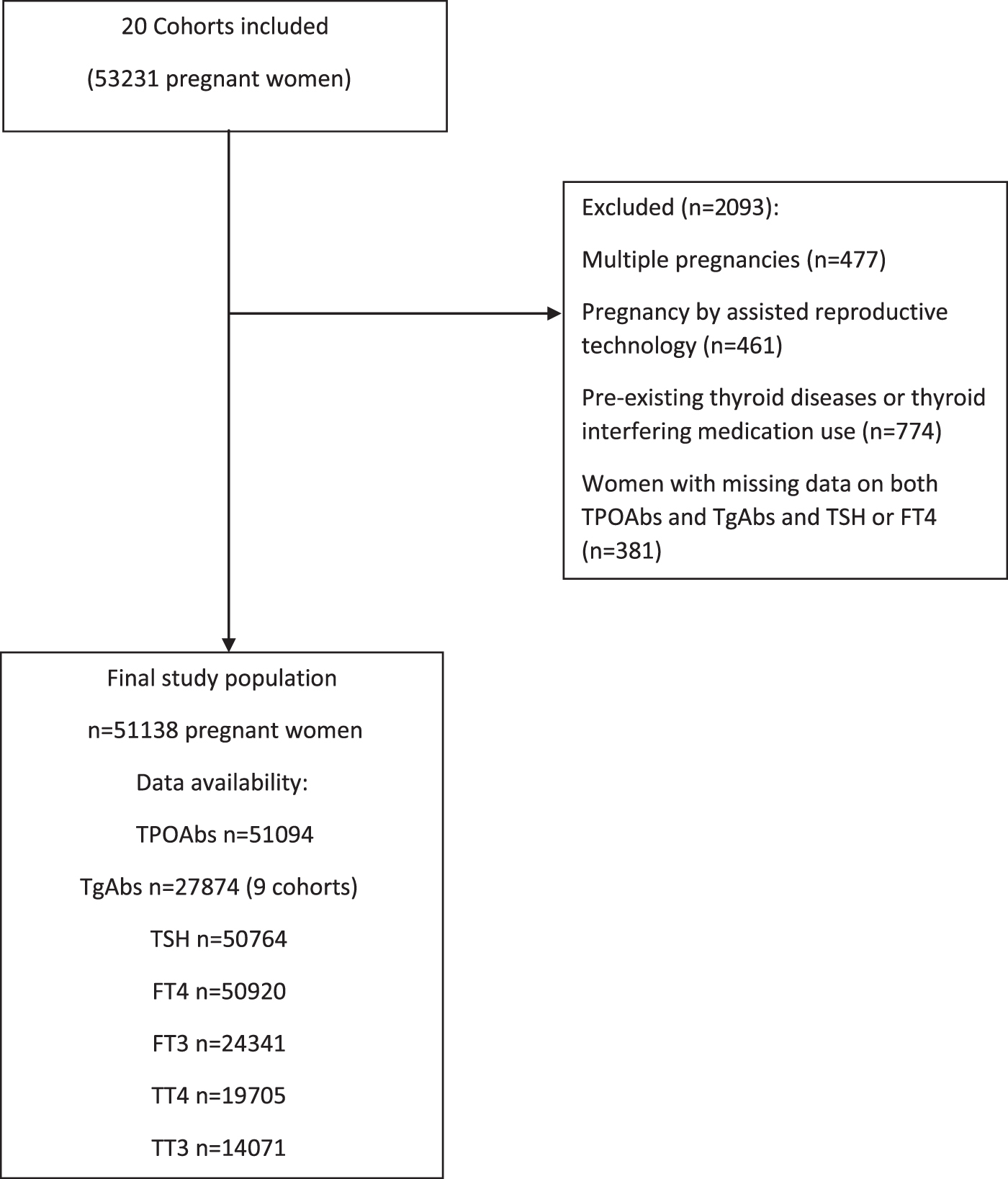
Flowchart. Based on 20 cohorts participating in the Consortium on Thyroid and Pregnancy, we excluded all women with known thyroid disease or use of thyroid interfering medication, with multiple pregnancies, with pregnancies achieved with assisted reproductive technology (in vitro fertilization or intracytoplasmic sperm injection), and women who lacked data on both thyroid antibody measurements (TPOAbs and TgAbs) and both TSH and fT4. fT4, free thyroxine; TgAbs, thyroglobulin antibodies; TPOAbs, thyroid peroxidase antibodies; TSH, thyrotropin.
Most cohorts originated from iodine-sufficient countries, but the proportion of antibody-positive women ranged both between the highest and lowest in iodine-sufficient and iodine-deficient regions, respectively (Supplementary Table S2). Demographic characteristics are summarized in Table 1. Supplementary Tables S3 and S4 depict missing data by cohort, and cohort-specific characteristics are provided in Supplementary Table S5 (demographics) and Supplementary Table S6 (thyroid function).
Demographic Characteristics of Included Women
In total, 51,138 women were included, of whom 51,094 had data on TPOAbs and 27,874 on TgAbs. Not all women had data on both antibodies and thus not all numbers add up to the total number of included women.
Continuous data are presented as median (2.5 and 97.5 percentiles) and categorical data as number (%).
BMI, body mass index; TgAbs, thyroglobulin antibodies; TgAb+, thyroglobulin antibody positive; TPOAbs, thyroid peroxidase antibodies; TPOAb+, thyroid peroxidase antibody positive.
Thyroid antibody positivity
TPOAb and TgAb positivity, respectively, was associated with higher TSH concentrations (z-score increment with TPOAb positivity 0.49 [CI: 0.38 to 0.60] and with TgAb positivity 0.34 [CI: 0.22 to 0.47]).
In cohorts with data on both antibodies, distinguishing between women with isolated TPOAbs (Fig. 2A), isolated TgAbs (Fig. 2B), and those being positive for both (Fig. 2C), the TSH concentration was higher in all subgroups compared with women who were negative for both antibodies, with the largest increment in women positive for both antibodies. These findings remained consistent when TSH z-scores were adjusted for potential confounders (isolated TPOAbs 0.39 [CI: 0.16 to 0.62], isolated TgAbs 0.26 [CI: 0.19 to 0.34], and positivity for both 0.58 [CI: 0.43 to 0.74]). In women with dual antibody positivity, fT4 concentration was lower compared with antibody-negative women (−0.17, CI: −0.29 to −0.05). While TPOAb-positive women had lower fT4 concentration than TPOAb-negative women (−0.19, CI: −0.26 to −0.12), this was not the case in TgAb-positive women compared with TgAb-negative women (−0.06, CI: −0.18 to 0.06).
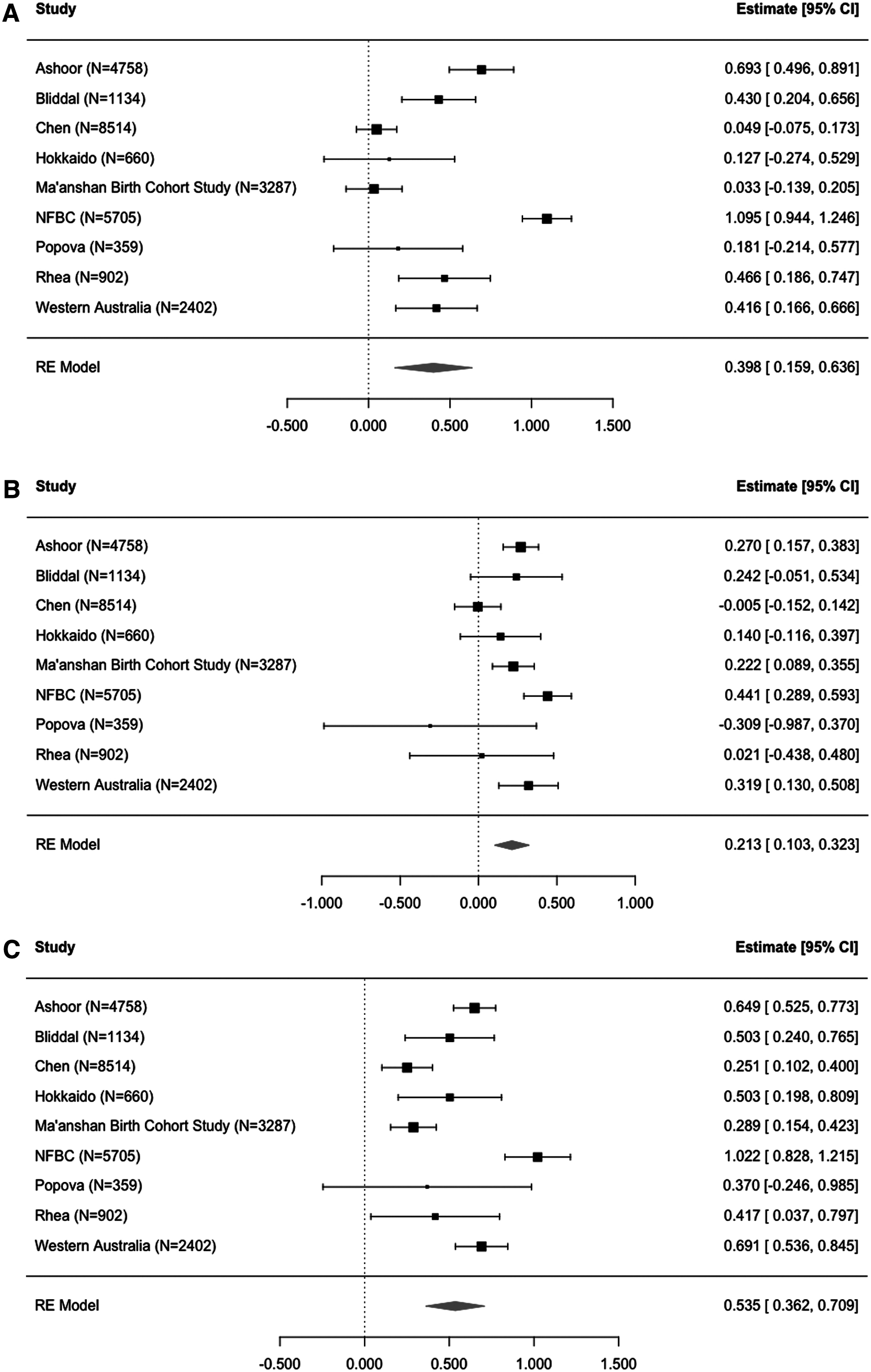
Difference in TSH z-score according to thyroid antibody positivity. Forest plots illustrating the result of the individual participant data meta-analysis of the increase in cohort-specific z-scores for TSH in women with isolated TPOAb positivity (
Thyroid antibody concentration
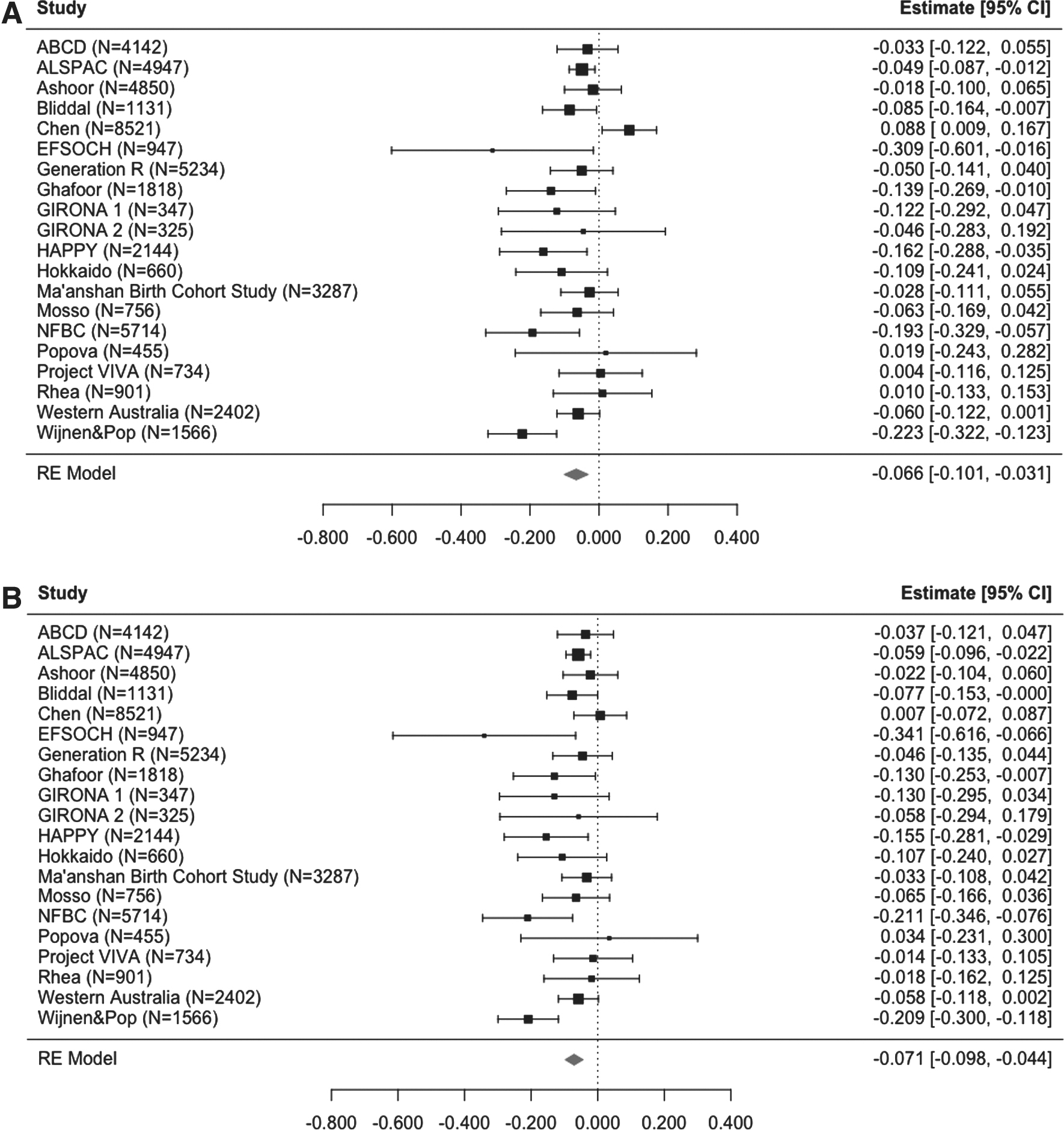
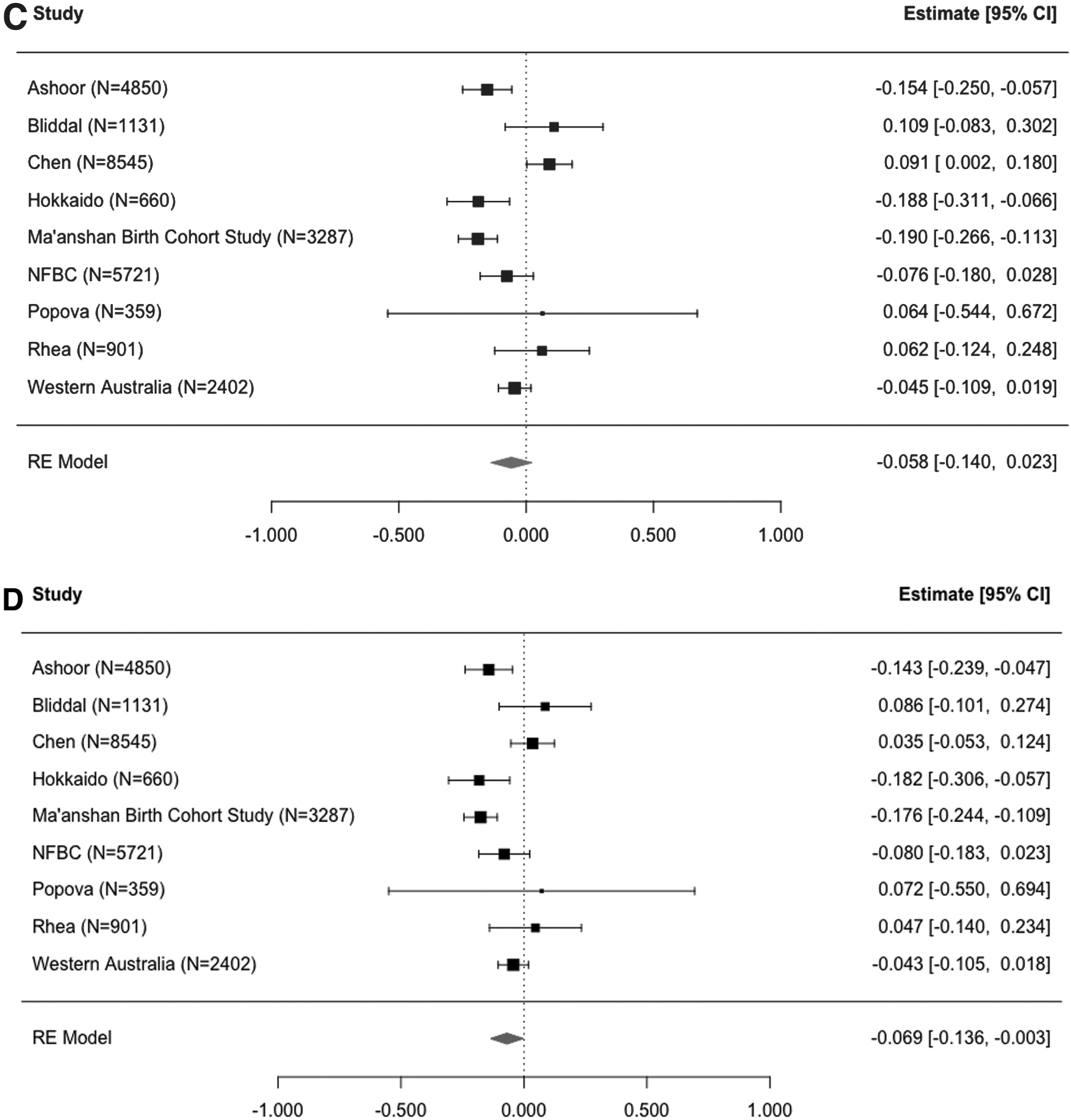
Among antibody-positive women, there was a significant dose–response effect, with higher TPOAb concentrations being associated with higher TSH concentrations—with and without adjustment for confounders (Fig. 3A, B). Also, higher TgAb concentrations were associated with higher TSH concentration (Fig. 3C, D). Higher TPOAb concentrations were associated with lower fT4 concentration both with and without adjustment for confounders (Fig. 4A, B). However, higher TgAb concentrations were significantly associated with slightly lower fT4 concentration only when adjusting for confounders (Fig. 4C, D).
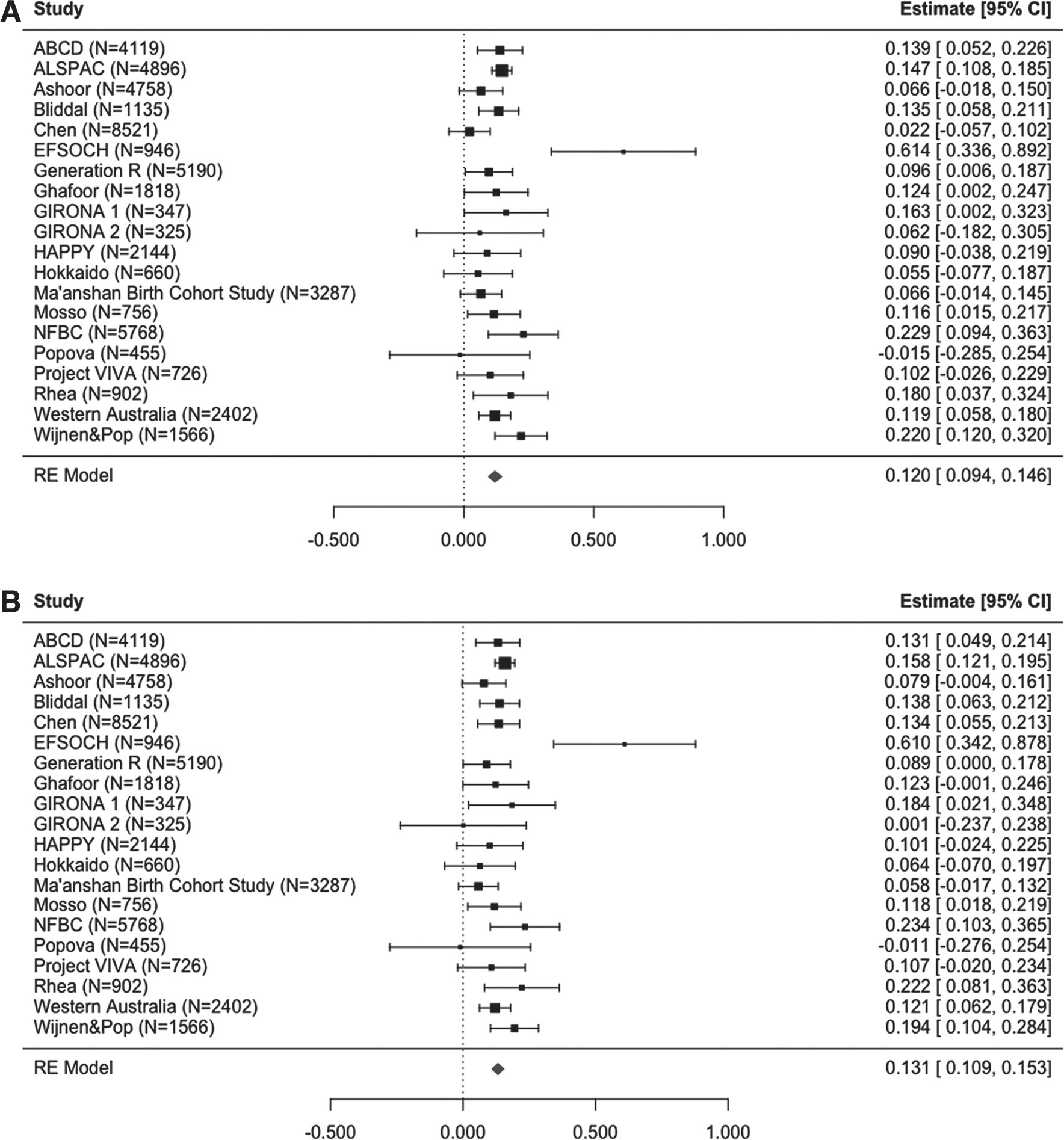
Change in TSH with increasing thyroid antibody concentration. Forest plots illustrating the result of the individual participant data meta-analysis of the change in cohort-specific z-scores for TSH with every doubling of thyroid antibody (log2) concentrations. (
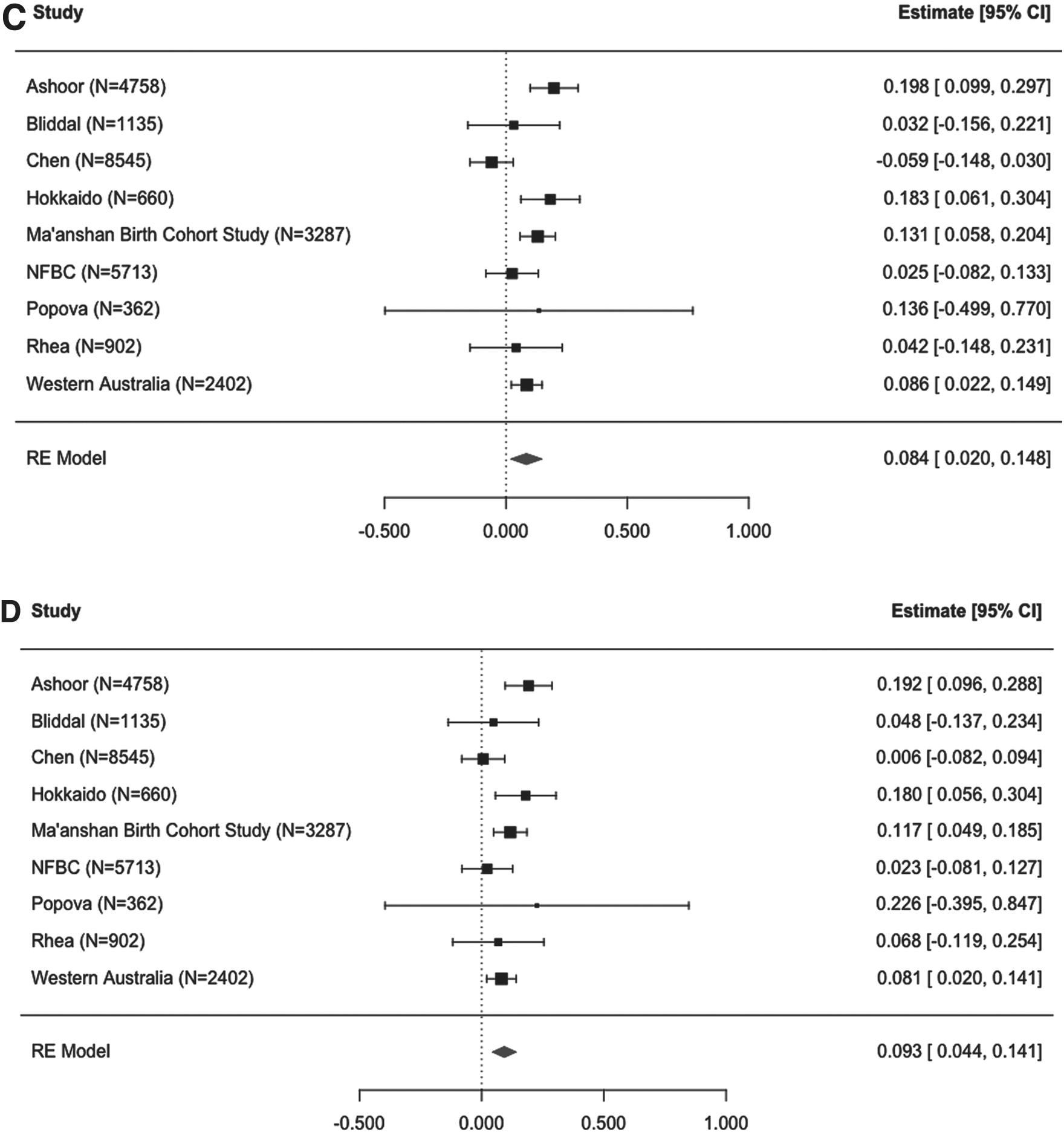
Change in fT4 with increasing thyroid antibody concentration. Forest plots illustrating the result of the individual participant data meta-analysis of the change in cohort-specific z-scores for fT4 with every doubling of thyroid antibody (log2) concentrations. (
When adjusting the linear mixed effect model analyses for the presence of the other antibody, only higher TPOAb concentrations remained significantly associated with higher TSH concentrations (Table 2). A higher TPOAb concentration was associated with lower fT4 concentration, but not significantly when adjusting for TgAbs (Table 2). Higher TgAb concentrations had no significant association with fT4 concentration (Table 2).
Association of Thyroid Peroxidase Antibodies and Thyroglobulin Antibodies with Thyroid Function in Pregnant Women
CIL, confidence interval lower limit; CIU, confidence interval upper limit; fT4, free thyroxine; SE, standard error; TgAb, thyroglobulin antibodies; TPOAb, thyroid peroxidase antibodies; TSH, thyrotropin.
Furthermore, a higher TPOAb concentration was associated with lower TT4 concentration (−0.08, CI: −0.10 to −0.04) and higher T3:T4 ratio (0.09, CI: 0.03 to 0.14). However, the association with lower TT4 concentration lost significance when adjusting for TgAbs (−0.06, CI: −0.12 to 0.01). Supplementary Table S7 shows the remaining results of the linear mixed effect model analyses for fT3, TT3, TT4, and T3:T4 ratio, which showed no significant association with TPOAb or TgAb concentrations.
Sensitivity analyses (Supplementary Table S8) for the linear mixed effect model results were conducted but had little effect on the results and none on the conclusions.
Discussion
In this individual participant data meta-analysis of 51,138 pregnant women, TSH concentrations were significantly higher in women with isolated TPOAbs or TgAbs, which was amplified in those who tested positive for both antibodies. Among antibody-positive women, a higher TPOAb concentration was associated with a higher TSH concentration, which was independent of TgAb concentrations. In contrast, while higher TgAb concentrations were also associated with higher TSH, this was not significant when adjusting for TPOAb concentrations. Only TPOAbs were associated with lower fT4 in dichotomous and continuous analyses.
Importantly, this study adds new insights into the association of TgAbs with thyroid function variables in pregnant women. The findings confirm those of the FaSTER trial; TSH concentrations were increased among TgAb-positive women, more so in TPOAb-positive women, and the most in women with both antibodies (16). However, this study also explored the association on a continuous scale demonstrating that the dose–response effect of TgAb concentrations on TSH concentrations was no longer significant when adjusting for TPOAbs. This is in accordance with findings from the U.S. National Health and Nutrition Examination Survey (NHANES) III study (n = 13,344) investigating thyroid function and autoimmunity in the nonpregnant US population between 1988 and 1994. In NHANES III, both TPOAb positivity and TgAb positivity were associated with increased odds ratios of having a TSH >4.5 mIU/L, but more so in the TPOAb-positive participants (odds ratio 8.4 vs. 1.8), while the TSH concentration was not increased in TgAb-positive participants when adjusting for TPOAb positivity (29).
An important lesson learned from long-term follow-up studies of nonpregnant populations is that despite high prevalences of thyroid autoimmunity, only some individuals progress to overt thyroid disease, while others remain euthyroid and even turn antibody negative (30,31). Combined, these data indicate that women with a higher TPOAb concentration have a higher risk of thyroid function test abnormalities during pregnancy.
There may be several explanations for this study's findings. Numerous factors are involved in the development of thyroid autoimmunity. Thyroid autoimmunity is the result of a loss of tolerance toward self-antigens in the thyroid gland that elicit T and B cell responses. Although TPOAbs and TgAbs often co-occur in patients with autoimmune thyroid disease and fluctuate in parallel, they likely represent separate immunological mechanisms (32,33). The higher TSH concentration in individuals with TPOAbs is thought to reflect a reduced functional thyroid reserve due to ongoing or past autoimmune reactions toward the thyroid gland. Thus, TPOAbs fix complement and cause a cytotoxic reaction damaging the thyroid gland (33). During pregnancy, the thyroid gland would therefore not be able to accommodate the increased need of thyroid hormone production, resulting in increased TSH concentrations.
Conversely, TgAbs cannot directly affect the autoimmune pathogenic process, but some epitopes recognized by TgAbs (possibly driven by thyroglobulin iodination) are also recognized by TPOAbs (33 –35). Differences in the epitopes of such cross-reactive antibodies could explain why some TgAb-positive individuals develop overt thyroid disease, while others remain euthyroid (33,36). Thus, TgAbs may theoretically be able to trigger an immune reaction with TPOAb production and cytotoxicity toward the thyroid gland, and ultimately an increase in TSH. Nevertheless, TPOAb-mediated cytotoxic thyrocyte destruction is a likely explanation for this and other studies showing that TPOAb-positive women were more likely to have high TSH concentrations and that the higher TSH concentration found with higher TgAbs was no longer significant when corrected for TPOAbs. However, this does not explain why women with isolated TgAb positivity also had higher TSH concentrations, although to a smaller extent. Historical studies illustrated that hereditary dispositions determined differences in TgAb immunoglobulin subtypes with different complement fixing capabilities, but further mechanistic studies would be needed to clarify this.
Although a higher TSH among TPOAb-positive women was a consistent finding across cohorts, there was a markedly higher TSH among TPOAb-positive women in the Exeter Family Study of Childhood Health (EFSOCH) study. Because samples in EFSOCH were drawn at 28 weeks of gestation, this could reflect an inability of the thyroid gland to meet the pregnancy-related increased demands for thyroid hormone production, which could be more evident in late pregnancy (8). Also, pregnancy ameliorates thyroid antibody concentrations by physiological changes in the immune system needed to sustain pregnancy with the fetal semiallograft (37). Thus, thyroid antibody concentrations decrease during pregnancy (8,38,39) and in cohorts with samples drawn in late pregnancy, women who are (still) thyroid antibody positive may represent a more severe phenotype.
Also, differences in regional iodine intake could affect the findings. In the Chen cohort, samples were mainly drawn in late pregnancy, but TPOAb-positive women did not show the same high TSH as in the EFSOCH cohort. This likely reflects differences in iodine availability (EFSOCH being from an iodine-deficient and Chen from an iodine-sufficient region), where a lower iodine availability could exacerbate the inability to compensate the increased thyroid hormone production demands. Although the present study demonstrated an association between thyroid autoimmunity and higher TSH across cohorts, the extent of this association is likely to differ according to gestational age at blood sampling and varying regional iodine availability.
Strengths and limitations
This study provides important new insight into the associations between TPOAbs and TgAbs and thyroid function during pregnancy, which can guide clinical practice and studies of adverse pregnancy outcomes. To our knowledge, this is the largest to-date individual participant data-based study of thyroid function and autoimmunity in pregnant women. An advantage of the large number of individual participants' data was the opportunity to perform detailed analyses of the dose–response effect of increasing thyroid antibody concentrations, especially that of TgAbs, with statistical power to detect even small effects despite differences in cohort characteristics and analytical methods. The findings support the current practice of using TPOAbs in the initial laboratory testing of pregnant women suspected of autoimmune thyroid disease, but in cases of suspected autoimmune thyroiditis in women who are TPOAb negative, the measurement of TgAbs may still be of value.
Comparing data from multiple cohorts allowed us to investigate if the association of TPOAbs and TgAbs with thyroid function differed between populations (e.g., different laboratory methods, population iodine status) (40,41). Almost all included studies showed similar trends with higher TSH and lower fT4 among antibody-positive women. In the meta-analyses, we were able to overcome possible between-cohort differences by developing cohort-specific z-scores adjusted for confounders.
However, there are limitations to this study. First, the study was based on a data collection within the Consortium on Thyroid and Pregnancy and was not exhaustive in terms of pregnancy cohorts with thyroid antibody measurements, and not all cohorts had data on all exposures and/or outcomes. Only nine cohorts had TgAb measurements reducing the statistical power in analyses involving TgAbs. Second, the study was cross-sectional, not allowing for follow-up measurements of thyroid antibody concentration and monitoring of thyroid (dys)function as pregnancy progressed. Third, the study was based on established cohorts, and cross-laboratory validation of the antibody measurements was not possible, and neither was a detailed evaluation of the cohorts' laboratory quality control measures. Fourth, assays used for fT4 measurements are known to be prone to interference from anti-T4-antibodies, which occur more often in individuals with TPOAbs and TgAbs. This could affect the findings related to fT4.
Finally, the study results demonstrate associations between thyroid antibodies and thyroid function, but do not provide insight into the mechanisms causing these findings or whether TgAbs or TPOAbs were associated with adverse pregnancy outcomes.
Conclusions
In this individual participant data meta-analysis, both isolated TPOAb positivity and TgAb positivity were associated with higher TSH, and TSH was higher in women positive for both antibodies. Higher TPOAb concentrations were dose dependently associated with higher TSH, which was unaltered after adjustment for TgAbs. Although a similar effect was found for higher TgAb concentrations, this was not significant when controlling for TPOAbs. The findings likely reflect a greater extent of cytotoxic destruction of the thyroid gland by TPOAbs, whereas (isolated) TgAbs possibly indicate an early, less destructive, and potentially reversible phase of autoimmune thyroiditis. The findings support the current practice of using TPOAbs in the initial laboratory testing of pregnant women suspected of autoimmune thyroid disease. However, further studies into the differences between TPOAb-positive and TgAb-positive individuals, as well as mechanistic studies, are needed to fully understand the spectrum of phenotypes.
Footnotes
Authors' Contributions
S.B., U.F.-R., A.D., and T.I.M.K. designed the study. S.B., U.F.-R., J.L.F., and Y.X. developed the statistical analysis plan, which was discussed and adjusted in collaboration with T.I.M.K. and A.D. T.I.M.K. and A.D. were in charge of cohort identification and data collection for this study as part of the Consortium on Thyroid and Pregnancy. L.-M.C., T.M., G.A., F.T., S.J.B., M.V., S.I., E.N.G., P.T., F.G., B.V., A.H., L.M., E.O., R.K., E.K.A., S.M., K.H., L.C., J.B., A.P., A.L.-B., L.B., R.P.P., E.N.P., S.M.N., L.C., T.G.V., P.V.P., J.P.W., K.H.N., E.S., X.L., and V.J.M.P. contributed substantially to the establishment and data collection of the cohorts included in this study, or the supervision and critical appraisal of this study. S.B., J.L.F., Y.X., and U.F.-R. were responsible for the statistical analyses. S.B. drafted the first version of the article, which was critically discussed and approved by all the coauthors.
Acknowledgments
The authors acknowledge all the hard work put into the original gathering of the included cohorts and the contribution by the many pregnant women participating in the studies. They appreciate the debates about immunological mechanisms involved in thyroid autoimmunity with Prof. Claus Henrik Nielsen.
Author Disclosure Statement
The following authors have disclosures not related to or influencing this research project: S.B.'s research salary was funded by Rigshospitalet's Research Foundation and Sygesikring Danmark. U.F.-R.'s research salary was funded by Kirsten and Freddy Johansen's Foundation. E.K.A. is a consultant for Veracyte, Inc., and Roche Diagnostics. S.M. was supported by the Arkansas Biosciences Institute, the major research component of the Arkansas Tobacco Settlement Proceeds Act of 2000, and by the US Department of Veterans Affairs Health Services Research & Development Service of the VA Office of Research and Development, under Merit review award number 1I21HX003268-01A1 (the content of this study is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Veterans Affairs or the US Government).
S.M.N. has received support from Roche Diagnostics, Access Fertility, Modern Fertility, Ferring Pharmaceuticals, TFP, and Merck. P.V.P.'s work is supported by the Ministry of Health Care of Russian Federation: Governmental funding research number 121031100288-5. Part of S.J.B.'s salary was subsidized by Sonic Health (Douglass Hanly Moir Pathology in Sydney). All other authors have nothing to disclose.
Funding Information
The present study was kindly supported by Kirsten and Freddy Johansen's Foundation, Beckett's Foundation, and Rigshospitalet's Research Foundation, and the Netherlands Organization for Scientific Research (grant 401.16.020). Information on funding for the original cohort studies is included in Supplementary File S1. The funding sources had no influence on the study design, interpretation of the findings, or on the preparation of this article.
Supplementary Material
Supplementary File S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8