
Abstract
Background:
BRAF and MEK inhibitors are cornerstones of the redifferentiation strategy in metastatic radioactive iodine (RAI)-resistant mutant thyroid cancers. We explored the exposure–toxicity relationship for dose-limiting toxicity (DLT) onset in patients treated with dabrafenib and/or trametinib and investigated whether plasma exposure was associated with RAI reuptake.
Methods:
We conducted a retrospective monocentric study in which we reviewed the electronic medical records of patients treated in our institution with a tumor redifferentiation strategy, for whom plasma concentration of dabrafenib, its active metabolite hydroxy-dabrafenib, and trametinib was measured. Trough concentrations (Cminpred) and total plasma drug exposure (area under the curve, AUC) of dabrafenib (AUCDAB), hydroxy-dabrafenib (AUCOHD), and trametinib (AUCTRA) were estimated.
Results:
Of the 22 patients treated in a redifferentiation strategy between March 2014 and December 2021, 15 were included in this study. A dabrafenib- or trametinib-related DLT was experienced by 8 (62%) and 9 (64%) patients, respectively. Patients who experienced a trametinib-related DLT exhibited a significantly higher last AUCTRA than the average AUCTRA of patients who had no DLT (390, IQR: 67 vs. 215, IQR: 91 ng/mL·h−1, respectively; p = 0.008). Patients who experienced a dabrafenib-related DLT had a higher AUCDAB than observed in other patients (9265 ng/mL·h−1 vs. 6953 ng/mL·h−1, respectively; p = 0.09). No clinical and demographical characteristic was associated with the DLT onset. Overall, 9 of 15 (60%) patients demonstrated tumor redifferentiation. Patients in whom RAI reuptake was achieved had significant lower AUCDAB (6990 ng/mL·h−1 vs. 9764 ng/mL·h−1, p = 0.014; respectively) compared with patients who did not. Moreover, the relative exposure ratio of AUCOHD/DAB was significantly higher in patients who achieved RAI reuptake (1.11 vs. 0.71, respectively; p = 0.0047).
Conclusions:
Our data suggest a relationship between DLT onset and trametinib plasma exposure, as well as an association between achievement of RAI reuptake and dabrafenib plasma exposure (AUC and ratio of AUCOHD/DAB). These data imply that the use of plasma drug monitoring could be helpful in guiding clinical practice in redifferentiation treatment.
Introduction
Thyroid cancer (TC) is the most frequent endocrine cancer with 43,720 new estimated cases and 2120 estimated death in the United States in 2023. 1 The prognosis of differentiated thyroid cancer (DTC) is generally good with treatments combining surgery and radioactive iodine (RAI). 2,3 Despite this overall good prognosis, distant metastases occur in 4–23% of cases and one-third of patients with metastatic disease have no RAI uptake, limiting therapeutic possibilities and thereby contributing to worse prognosis and to the majority of deaths. 4,5 These RAI-resistant (RAIR) cancers represent ∼5% of all TCs. 6 Currently, lenvatinib and sorafenib, two multitargeted receptor tyrosine kinase inhibitors (TKIs) with predominant antiangiogenic activity, are considered the standard of care in the first-line metastatic RAIR setting, with a median progressive-free survival of 18.3 and 10.8 months, respectively. 7,8
In recent years, BRAF and RAS mutations, and RET, NTRK, ALK gene rearrangements have been, respectively, identified in 60%, 15%, and 12% of papillary thyroid cancers. 9 These molecular alterations activate the mitogen-activated protein kinase pathway involved in DTC oncogenesis by different mechanisms, 10 –12 promoting uncontrolled proliferation and tumor dedifferentiation 13 with a consequent decrease in the ability of tumor cells to uptake RAI. One of the challenges in the management of such tumors is to induce a significant reuptake of RAI. This is referred to as a mechanism of tumor redifferentiation. 14 Several studies focused on the redifferentiation of RAIR DTC with molecular alteration, with promising results with BRAF inhibitors (vemurafenib, dabrafenib) and/or MEK1/2 inhibitors (selumetinib, trametinib), 15,16 but to date this strategy remains investigational and the precise therapeutic consequences and clinical benefits are yet to be established.
Nevertheless, severe toxicities leading to dose reduction or discontinuation are frequently associated with these treatments in patients with molecularly altered TC. Large phase III studies of dabrafenib alone or combined with trametinib in melanoma patients show that almost all patients experience an adverse event and up to 58% of patients require a dose reduction and up to 18% require permanent discontinuation of the treatment. 17 –19 Known MEK inhibitor-associated toxic effects, including peripheral edema, hypertension, decreased cardiac ejection fraction, and ocular events, occurred more frequently in the combination-therapy groups than in the monotherapy group. Conversely, known BRAF inhibitor-induced hyperproliferative skin lesions, such as cutaneous squamous-cell carcinoma, papilloma, and hyperkeratosis, were observed less frequently in the combination-therapy groups than in the monotherapy group. 18
In these studies, the most common events that led to permanent discontinuation were pyrexia, decreased left ventricular ejection fraction, and an increased alanine aminotransferase level. In the setting of TC, the most common treatment-related adverse events reported in one study were skin and subcutaneous tissue disorders, fever, hyperglycemia with dabrafenib alone, and fever, nausea, chills, and fatigue with dabrafenib+trametinib. 20 In other studies, grade 3 or 4 adverse events have included pyrexia and rash. 15,16
Kinase inhibitors such as antiangiogenic drugs (lenvatinib, sorafenib) and BRAF inhibitors (vemurafenib) are known to exhibit a large interindividual variability in their pharmacokinetics (PK), as well as a narrow therapeutic index. 21 –23 Dabrafenib and trametinib present mild-to-large interindividual variability in their PK. 22,24,25 Moreover, several PK/pharmacodynamic (PD) studies have identified an increased plasma exposure of drug (dabrafenib or trametinib) as a risk factor of toxicity onset in metastatic BRAF-mutated melanoma patients. 24,26 –28 However, other studies did not confirm these results. 24,25,29 30 In patients with BRAF-mutated TC, the exposure–toxicity relationship could be different since their toxicity profile and comorbidities such as sarcopenia can differ from those observed in metastatic BRAF-mutated melanoma patients. To the best of our knowledge, no PK/PD data (toxicity, efficacy) for dabrafenib and trametinib are currently published in patients treated for BRAF-mutated TC, especially in the context of redifferentiation of RAIR DTC with molecular alteration.
In the present study, the main purpose was to explore the exposure–toxicity relationship for dose-limiting toxicity (DLT) onset in patients with RAS- or BRAF-mutated metastatic RAIR DTC and treated with dabrafenib and/or trametinib. Furthermore, the association between plasma drug exposure and RAI reuptake was assessed.
Methods
Patients
Consecutive patients treated with BRAF and/or MEK inhibitors for metastatic RAIR DTC between March 2014 and December 2021 at Cochin University Hospital (Paris, France) were included in this retrospective monocentric study. Patients with a BRAF-mutated cancer received dabrafenib and trametinib (except for the first patient of our cohort who received dabrafenib alone) and patients with RAS-mutated cancer received trametinib alone in the context of tumor redifferentiation strategy. After two to four weeks of treatment, the RAI reuptake was evaluated by 123I or 131I diagnostic whole-body scintigraphy. The assessment of RAI uptake was purely qualitative, and no dosimetry was used. In this cohort, redifferentiation was defined as RAI uptake in lesions that were shown to be previously non-RAI avid, and uptake in all metastases was not necessary.
For patients with low-volume disease and tumor redifferentiation, treatment was continued until an RAI therapy was performed and then interrupted. For patients with high-volume disease and tumor redifferentiation, treatment could be continued after RAI therapy if deemed necessary by the multidisciplinary tumor board. For patients with no tumor redifferentiation, treatment could be continued until disease progression or excessive toxicity as per the patient and physician discretion. The study inclusion criteria were as follows: patients older than 18 years, treatment with dabrafenib or trametinib for metastatic RAIR, BRAF- or RAS-mutated DTC, and at least one plasma concentration of dabrafenib or trametinib available performed as part of routine drug monitoring. All patients provided their written consent for the use of their data for research. The study was approved by the local ethics committee in oncology (No. CLEC 211218ACBB1). Ethical procedures were followed according to the Declaration of Helsinki and relevant local rules.
Data collection
Clinical (including adverse events), biological, and radiological data were collected from each patient's electronic medical records over the treatment course. The evaluation and scoring of treatment-related adverse events were reported according to the Common Terminology Criteria for Adverse Effects version 5.0. Ion AmpliSeq® (Thermo Fisher Scientific, Waltham, MA) was used to examine various hotspots, including in genes of interest for thyroid cancer BRAF, NRAS, KRAS, and HRAS.
Sarcopenia assessment
Baseline computed tomography scans just before treatment initiation were studied for skeletal muscle mass measurement. Images were analyzed using ImageJ software, v1.48q (National Institutes of Health). The axial slice centered on the L3 vertebra was chosen to measure muscle mass, 31,32 and muscles were identified anatomically and then quantified using Hounsfield unit bounds (−29; +150) of skeletal muscle density. 33 The cross-sectional areas of the sum of all muscles were computed for each image, and the mean values for two consecutive images were computed. For each patient, the cross-sectional areas of the sum of all muscles were determined by two physicians and the average area was recorded. The muscle area was then standardized by the height of the patient. 34,35 Patients were considered sarcopenic for index values less than 55.4 cm2/m2 in men and 38.9 cm2/m2 in women. 31
PK analysis
Drug monitoring was performed at the physician's discretion for routine practice. Blood samples were collected at any time over the dosing interval. Dabrafenib, its active metabolite hydroxy-dabrafenib, and trametinib plasma concentrations were assessed using a previously published high-performance liquid chromatography coupled with tandem mass spectrometry method (LC-MS/MS). 36 This method presents both sufficient precision (intra- and interassay coefficient of variation from 2.0% to 14.9%) and accuracy (inter- and intraday bias between 1.2% and 10.9%). Furthermore, the accuracy for dabrafenib and trametinib was ensured by participation in the TKI Proficiency Testing Scheme provided by the Group of Clinical Pharmacology in Oncology (Asqualab, Issy Les Moulineaux, France).
Trough concentrations (Cminpred) and total plasma drug exposure (area under the curve, AUC) of dabrafenib (AUCDAB), hydroxy-dabrafenib (AUCOHD), and trametinib (AUCTRA) were estimated using population PK models previously developed by our team with the nonlinear mixed-effects modeling program NONMEM v7.4.1 and the Perl-Speaks NONMEM (PsN) Toolkit v4.8.0 (22).
Efficacy and safety analyses
The primary endpoint for the exposure–toxicity relationship was the onset of DLT defined as any toxicity leading to dose reduction or treatment discontinuation (temporary or permanent). The secondary objective was to investigate whether dabrafenib, hydroxy-dabrafenib, and trametinib exposure (AUC and Cminpred) was associated with RAI reuptake.
Statistics
Results were described as number (percentage) for binary/categorical variables and median [range] for continuous variables. The association of age (<75 years vs. ≥75 years), sex, and sarcopenia with drug PK was explored using dose-normalized AUC as the PK parameter and nonparametric unpaired Wilcoxon test. Regarding the analysis of exposure–toxicity relationship, plasma drug (dabrafenib, hydroxy-dabrafenib, and/or trametinib) exposure (AUC, Cminpred) close to the DLT onset was analyzed in patients experiencing DLT. Conversely, average plasma exposure (AUC or Cminpred) over the treatment course was considered in patients who did not experience any DLT. The average plasma exposure was calculated by averaging all available AUC or Cminpred of dabrafenib, hydroxy-dabrafenib, and/or trametinib. The association between the DLT onset and continuous or binary variables was investigated using nonparametric unpaired Wilcoxon test and Fisher test, respectively.
The following baseline patients' characteristics were evaluated for their association with DLT onset: age, sex, Eastern Cooperative Oncology Group Performance Status, body weight, body mass index, C-reactive protein, albumin, average muscle area, muscle index, sarcopenia, and plasma drug exposure (dabrafenib, hydroxy-dabrafenib, and trametinib). The potential associations of AUC and Cminpred for each drug and RAI reuptake were evaluated using the nonparametric unpaired Wilcoxon test. The closest plasma drug exposure to RAI reuptake evaluation was analyzed. Statistical significance was defined by p < 0.05. Statistical analyses were performed by R program v3.6.1 with RStudio v1.1.383.
Results
Patients' characteristics
Twenty-two patients were treated with BRAF and/or MEK inhibitors for RAIR DTC from March 2014 to December 2021. Among them, four were excluded because plasma drug monitoring was not performed, or insufficient clinical information was available. Three patients treated by vemurafenib and/or cobimetinib were also excluded. Overall, 15 patients were included in the study cohort: 12 (80%) treated concomitantly with dabrafenib and trametinib, 1 (7%) treated with dabrafenib monotherapy, and 2 (13%) treated with trametinib monotherapy (Fig. 1). Patients' characteristics are summarized in Table 1. BRAFV600E mutation was present in 80% regardless of the tumor type. No patient presented impaired hepatic or renal function, while 47% of patients were sarcopenic. Finally, one patient started at a reduced dose for dabrafenib and trametinib because of advanced age and altered general condition.
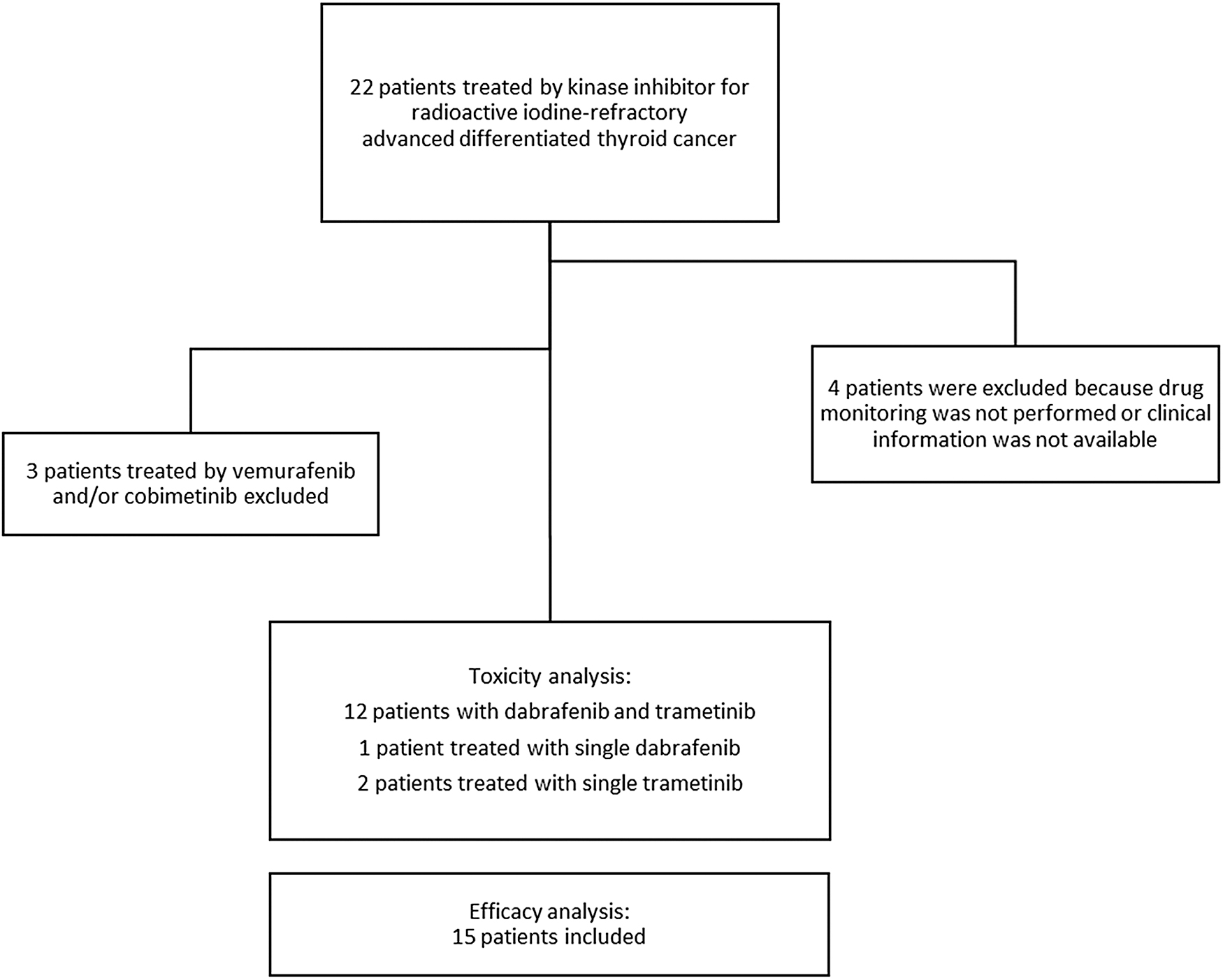
Study flowchart.
Patients' Characteristics
Results are expressed as median [range] or number (percent).
Creatinine clearance was estimated according to Cockcroft–Gault formula.
Thirteen patients received dabrafenib.
Fourteen patients received trametinib.
BMI, body mass index; CRP, C-reactive protein; ECOG PS, Eastern Cooperative Oncology Group Performance Status.
PK analysis and prediction
Overall, 46 and 45 PK samples for dabrafenib (including hydroxy-dabrafenib) trametinib were, respectively, examined, and then analyzed with population pharmacokinetic (popPK) models. These data were well-fitted by the models and observed concentrations of dabrafenib, hydroxy-dabrafenib, and trametinib were well predicted. The mean absolute prediction error was 33.5%, 37.5%, and 22.9% for dabrafenib, hydroxy-dabrafenib, and trametinib, respectively. Additional validation results are presented in Supplementary Figures S1 and S2. On average, each patient had 5 [1–11] PK samples for trametinib and 3 [1–11] PK samples for dabrafenib. According to the popPK model, the median [range] AUC per patient was 7920 [6680–12,121], 7187 [5634–8390], and 311 [148–542] ng/mL·h−1 for dabrafenib, hydroxy-dabrafenib, and trametinib, respectively. The median [range] relative exposure ratio of AUCOHD/AUCDAB (AUCOHD/DAB) was 0.83 [0.58–1.23].
Finally, the average median [range] Cminpred per patient were 97.2 [37.0–549.0] ng/mL, 130.2 [81.0–344.0] ng/mL, and 10.7 [5.0–20.0] ng/mL for dabrafenib, hydroxy-dabrafenib, and trametinib, respectively. Figure 2 presents the variabilities on AUCs according to the daily dose.
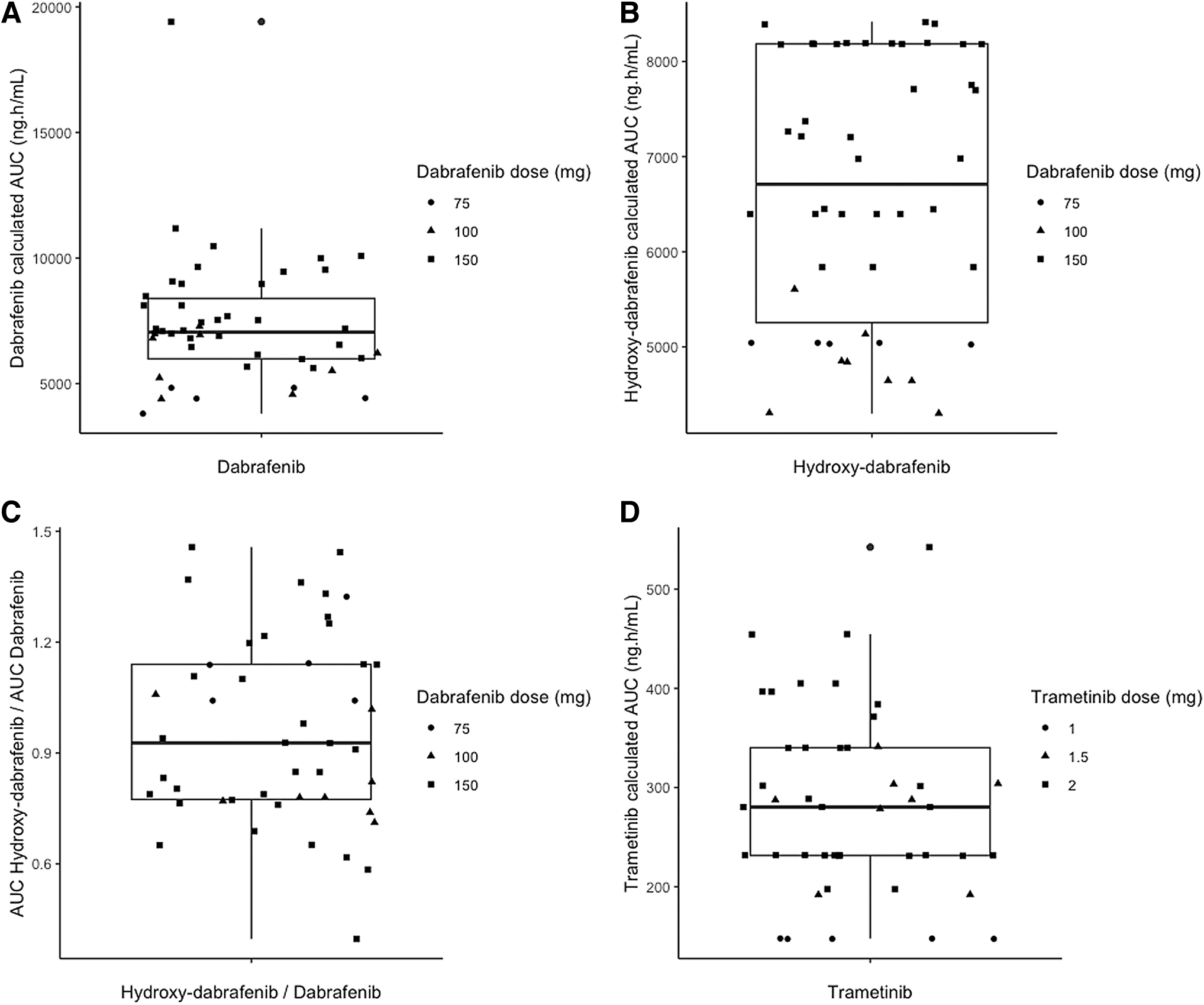
Pharmacokinetic variability according to daily dose. (
PK variability factors
Females exhibited higher dose-normalized AUCDAB [9841 (IQR: 695) vs. 7019 (IQR: 1369) ng/mL·h−1, respectively; p = 0.0082] and dose-normalized AUCTRA [378 (IQR: 81) vs. 272 (IQR: 56) ng/mL·h−1, respectively; p = 0.043] compared with males (Fig. 3). The dose-normalized relative exposure ratio of AUCOHD/DAB was 1.51-fold higher in males compared with females [1.11 (IQR: 0.25) vs. 0.73 (IQR: 0.16), respectively; p = 0.0082]. Neither sarcopenia (Fig. 3) nor age (data not shown) was associated with any PK biomarkers (AUCDAB, AUCOHD, ratio of AUCOHD/DAB, and AUCTRA).
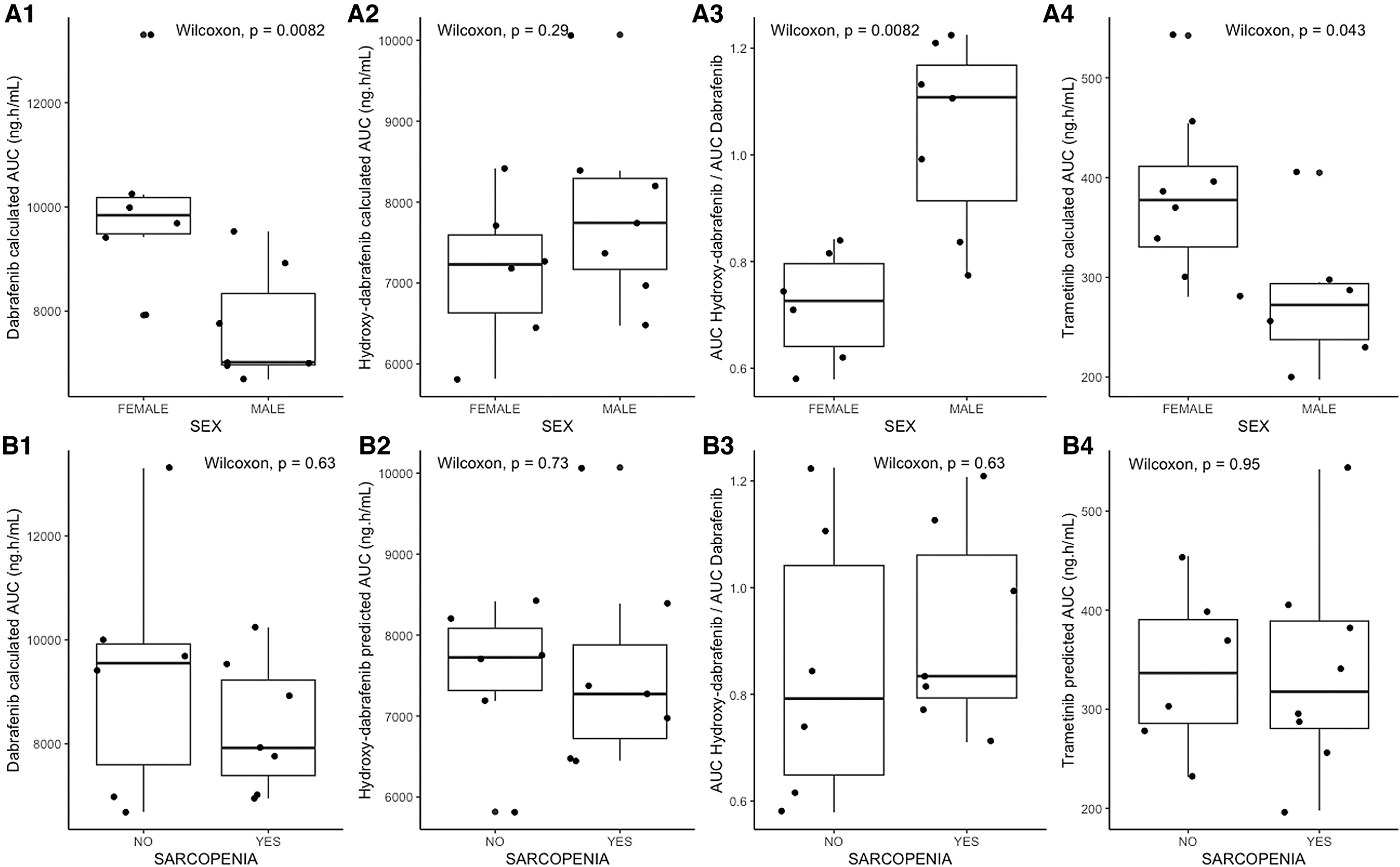
The respective associations between sex (
Analysis of exposure–toxicity relationship
Eight (62%) patients experienced a dabrafenib-related DLT with a median time to onset of 69 days [27–190] after treatment start. Dabrafenib was permanently discontinued in 2 patients (15%), paused in 2 patients (15%), and the dosing was reduced in 4 patients (31%). A trametinib-related DLT was observed in 9 (64%) patients with a median time to onset of 60 days [12–190] after treatment start. Trametinib was permanently discontinued for 3 patients (21%), paused for 2 patients (14%), and the dosing was reduced for 4 patients (28%).
The DLTs observed in the cohort study were as follows: asthenia (n = 5, 33%), cutaneous rash (n = 3, 20%), thrombocytopenia (n = 2, 13%), creatine phosphokinase elevation (n = 2, 13%), liver enzyme elevation (n = 2, 13%), pyrexia (n = 1, 7%), mucositis (n = 1, 7%), rhabdomyolysis (n = 1, 7%), muscle pain (n = 1, 7%), and lymphopenia (n = 1, 7%). The median time from last PK sample collection to DLT onset was 29 [range 0–138] and 9 days [range 0–138] for dabrafenib and trametinib, respectively. Patients who experienced a trametinib-related DLT exhibited a significantly higher last AUCTRA than the average AUCTRA of patients who had no DLT [390 (IQR: 67) vs. 215 (IQR: 91) ng/mL·h−1, respectively; p = 0.008] (Fig. 4).
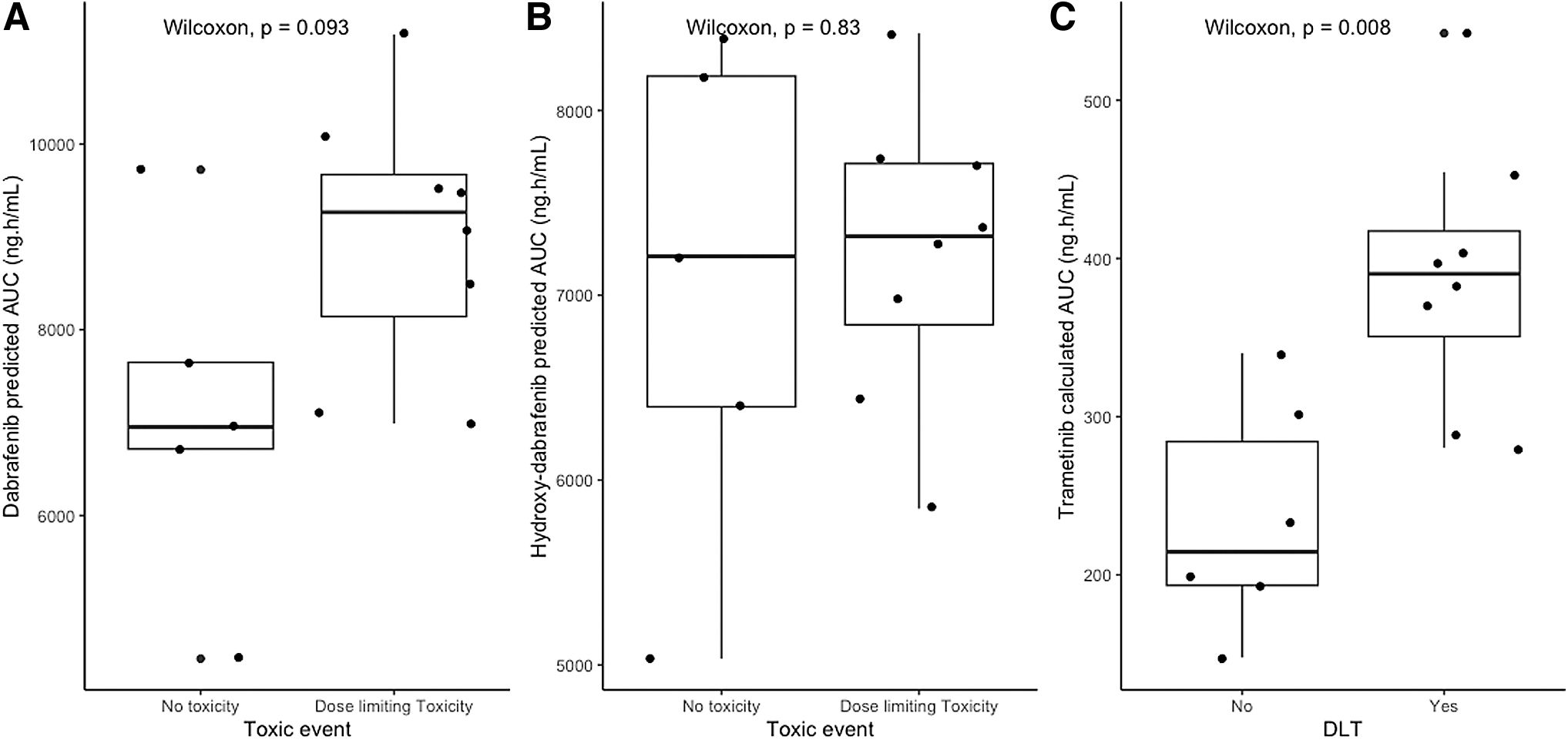
Plasma total exposure (AUC) according to the onset of dose-limiting toxicity of (
In the same way, AUCDAB in patients who experienced dabrafenib-related DLT tended to be higher than that in other patients [9265 (IQR: 1528) vs. 6953 (IQR: 933) ng/mL·h−1, respectively], although the statistical significance was not reached (p = 0.09). No clinical and demographical characteristic tested was associated with the onset of a DLT for dabrafenib and trametinib (Table 2).
Analysis of the Association of Variables with Dose-Limiting Toxicity Onset in Patients Treated with Dabrafenib and/or Trametinib
Results are expressed as median [range] or frequency (percent).
Pharmacokinetic analysis could not be performed for 1 patient who experienced a trametinib-related DLT in 2015 and this patient trametinib exposure was only evaluated after dose reduction, which did not lead to another DLT.
Patients were considered sarcopenic if <55.4 cm2·m−2 (men) or <38.9 cm2·m−2 (women).
AUC, area under the curve; Cminpred, trough concentrations; OHD, hydroxy-dabrafenib; DAB, dabrafenib; DLT, dose-limiting toxicity; TRA, trametinib.
Analysis of exposure-RAI reuptake relationship
Overall, 9 of 15 (60%) patients demonstrated tumor redifferentiation. The median delay between RAI reuptake evaluation and drug assay was 10 days [0–1277] for both dabrafenib and trametinib. Patients who achieved RAI reuptake had significant lower AUCDAB [6990 (IQR: 1577) vs. 9764 (IQR: 2418) ng/mL·h−1, p = 0.014; respectively] and Cminpred,DAB [51.6 (IQR: 24.4) ng/mL vs. 110.1 (IQR: 53.3) ng/mL, p = 0.014; respectively] compared with patients who did not (Table 3). Moreover, the relative exposure ratio of AUCOHD/DAB was also higher in patients who achieved RAI reuptake [1.11 (IQR: 0.26) vs. 0.71 (IQR: 0.18), respectively; p = 0.0047] (Fig. 5), while AUCOHD - and AUCTRA were not associated with RAI reuptake (p = 0.29 and p = 0.66; respectively).
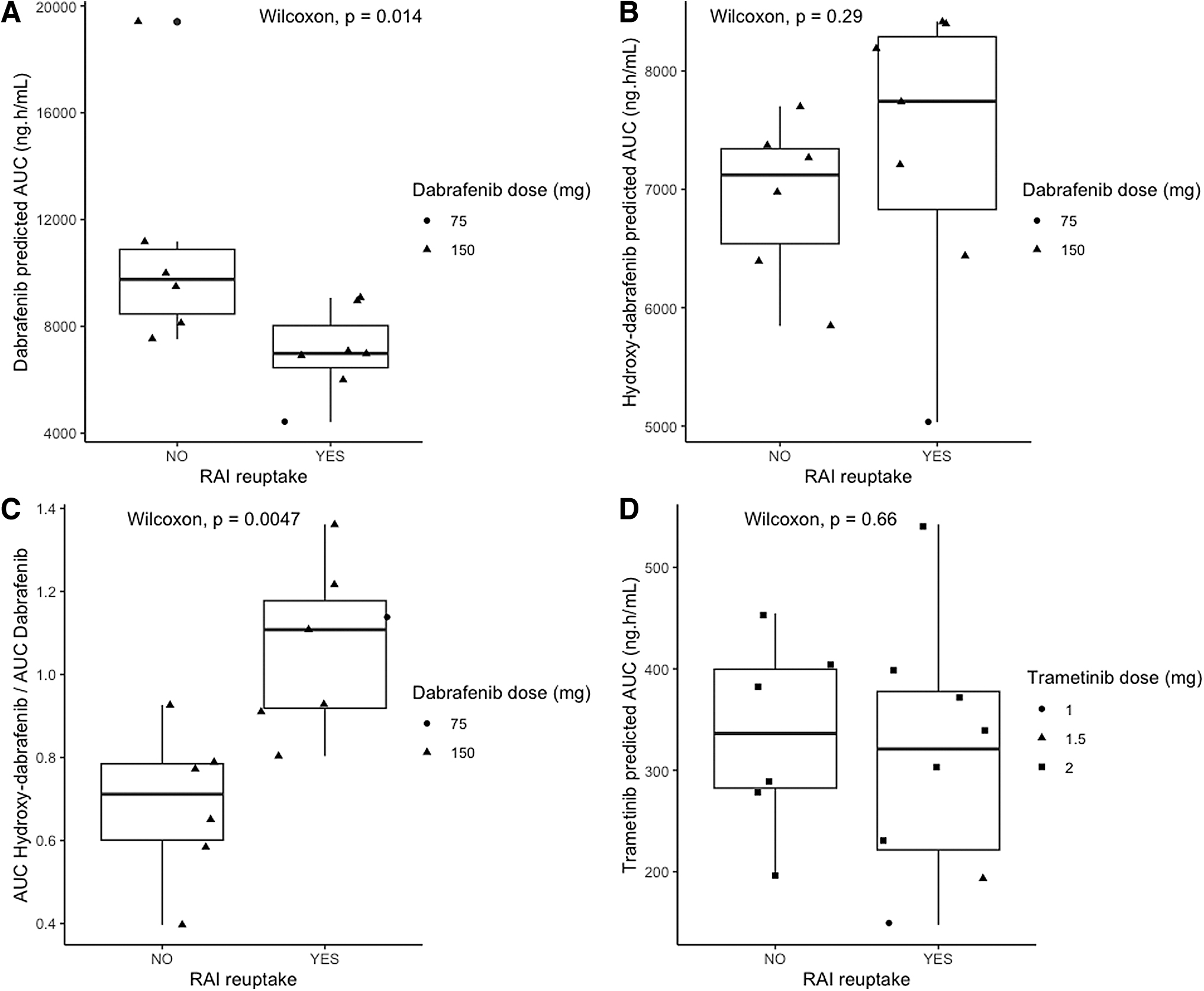
Levels of exposure for dabrafenib and trametinib according to the status of redifferentiation success.
Dabrafenib and Trametinib Exposure in Patients According to the Success of Redifferentiation
Results are expressed as median [range] or frequency (percent).
RAI, radioactive iodine.
Discussion
A better understanding of the relationship between the PK of dabrafenib and trametinib and clinical outcomes could enable optimization of redifferentiation strategies for advanced RAIR DTC. To our knowledge, this is the first study to report on the PK/PD relationship between plasma trametinib exposure and DLT onset, as well as the associations between dabrafenib AUC, AUCOHD/DAB, and RAI reuptake.
In the present study, the mean Cminpred of dabrafenib and hydroxy-dabrafenib were substantially higher than those reported in metastatic melanoma patients included in a phase III trial or a real-life cohort, 26,29,37 while mean Cminpred of trametinib were consistent with those reported in literature. 25,26,29 Finally, the median relative exposure ratio of AUCOHD/DAB was consistent with the expected ratio in metastatic melanoma patients, 24,38 which suggests similar metabolic capabilities in TC and melanoma patients.
In a recently published phase II trial on RAIR DTC patients, Busaidy et al. 20 reported mean AUCDAB and AUCTRA estimates that were close to ours, but the AUCOHD was lower. These authors conducted noncompartmental PK analysis to estimate AUCs, whereas we used a Bayesian approach. These different methodological approaches may explain the discrepancy in AUC values between these two studies. 20,24,38 In agreement with Busaidy et al., 20 we reported a high interindividual exposure variability for dabrafenib, hydroxy-dabrafenib, and trametinib. Sex was identified as a significant source of PK variability for both dabrafenib and trametinib. Females exhibited higher dose-normalized AUCDAB and AUCTRA, which confirms the findings of previous studies. 24,25,39 Neither age (less than or ≥75 years) nor sarcopenia was associated with the PK of dabrafenib and trametinib. However, the limited sample size of patients included in this study may be insufficient to identify a less impactful variability factor.
In the present study, DLTs were frequently observed; 8 (62%) patients experienced a dabrafenib-related DLT and 9 patients (64%) a trametinib-related DLT. Overall, 11 patients (73%) experienced a DLT under combination therapy. These results are in accordance with those reported in a recent phase II trial. 20 Of 27 patients treated with dabrafenib plus trametinib, dose reduction and permanent discontinuation were documented in 6 (22%) patients and 15 (56%), respectively. In another study conducted in 51 patients with metastatic BRAF-mutated DTC treated with continuous vemurafenib, 27 (53%) had dose reductions, 38 (75%) required a dose interruption, and 14 (27%) had to discontinue treatment due to adverse events. In addition, 34 patients (66%) experienced grade ≥3 adverse events. 40 Conversely, other studies investigating tumor redifferentiation in RAIR DTC with molecular alterations reported largely low-grade adverse events and few DLTs. 16,41 –43
Previous studies conducted in melanoma patients showed an association between increased dabrafenib plasma exposure and the onset of toxicities, 24,28,44 and one “real-life” study documented a relationship between trametinib trough concentration and adverse events. 26 However, other studies reported contradictory results. 24,26,29 30 Moreover, all these PK/PD studies were subject to differences in methodological approaches, which prevents the establishment of a threshold concentration (of dabrafenib or trametinib) for toxicity. In the present study, patients who experienced a trametinib-related DLT exhibited a significantly higher AUCTRA and Cminpred,TRA than patients who had no DLT. Furthermore, higher AUCDAB tended to be higher in patients who experienced dabrafenib-related DLT compared with other patients.
Taken together, these results suggest that plasma drug monitoring could potentially help in identifying patients who are at a higher risk of severe toxicity and require more close monitoring. No clinical and demographical characteristics were associated with the onset of a DLT. In particular, sarcopenia was not associated with an excess of toxicity contrary to our hypothesis based on previous data. 32,45
A deeper understanding of the PK of dabrafenib and trametinib could be valuable to enable optimizing the efficacy of redifferentiation strategies. Both trametinib and dabrafenib achieve PK steady state after 2 weeks of treatment for 2 distinct reasons: the long half-life for trametinib (about 90 hours) and the auto-induction of CYP3A4 metabolism for dabrafenib. 46,47 The duration of BRAF and MEK inhibitors before RAI therapy ranges from four to six weeks in most protocols. 15,48 In this study, we reported that DLTs commonly occur within the first two months of treatment, which suggests that the evaluation of redifferentiation and treatment with RAI should be performed as soon as possible, to limit the risk of toxicity. As previously described, the redifferentiation effect itself would be limited to the pharmacokinetic effect of the treatment, 49 with the clinical consequence that in case of treatment discontinuation during the redifferentiation phase, RAI therapy should be postponed.
Finally, we reported a 60% rate of redifferentiation, which is higher than the previously published study of Weber et al., which reported a 33% (2 of 6 patients) rate. 16 Interestingly, we observed both lower dabrafenib AUC and higher AUCOHDAB/DAB in patients with redifferentiation, which suggests an influence of dabrafenib PK on RAI reuptake. As hydroxy-dabrafenib is twofold pharmacologically active in clinical setting, 47 a high ratio of AUCOHDAB/DAB would be in favor of a greater pharmacodynamic activity on mutated BRAF kinase. However, AUCOHDAB was not significantly higher in patients with redifferentiation, which does not support our hypothesis.
These results should be interpreted with extreme caution because of the limited sample size of our cohort and sparse PK sampling over treatment course. Another limitation of our study is the retrospective nature, and the potential for selection bias as the pharmacokinetic assessments were subject to physician discretion.
In the era of precision medicine, it is appreciated that all patients do not necessarily benefit from fixed dosing strategies for oral targeted therapies since their PK frequently display significant interpatient variability. This later can lead to treatment failure or severe toxicity events. Pharmacokinetically guided dose optimization may therefore be a very interesting tool to be implemented in clinical practice. 50,51 The use of plasma drug monitoring is currently gaining popularity in the oncology field. From a single blood sample, total exposure (AUC) or trough concentration may be estimated using simple extrapolation or pharmacometric methods. 52,53 Furthermore, LC-MS/MS systems for drug-level assessment are more readily available in specialized centers. 50 Taken together, these factors contribute to better accessibility of plasma drug monitoring for physicians.
Conclusion
The present PK/PD study suggests a trametinib exposure–toxicity relationship and a dabrafenib exposure–response relationship for RAI uptake. Taken together, these PK/PD data suggest that plasma drug monitoring for dabrafenib and trametinib could potentially be helpful in optimizing redifferentiation treatment of DTC.
Footnotes
Authors' Contributions
D.B., R.S., L.G.-R., A.P., A.S.C., J.C., M.V., F.G., J.A., B.B., and O.H. have taken part in writing the article, reviewing it, and revising its intellectual and technical content.
Author Disclosure Statement
D.B., R.S., L.G., A.P., A.S.C., J.C., M.V., and J.A. have no relevant financial disclosures. F.G. reports grants and personal fees from BAXTER, personal fees from FRESENIUS KABI and NUTRICIA, outside the submitted work. B.B. reports personal fees from BMS, Pierre Fabre, PFIZER, EISAI, and PROMISE, outside the submitted work. O.H. reports personal fees from BAYER, SANOFI, MSD, BMS, IPSEN, PFIZER, EISAI, JANSSEN, and ASTRA ZENECA, outside the submitted work.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2