
Abstract
Background:
Few risk factors for the development of intracranial aneurysms (IAs) are known. We investigated the potential role of thyroid diseases in IA development using nationwide real-world data.
Methods:
A nested case–control study within the National Health Insurance Service—National Sample Cohort data from 2002 to 2019 was performed. A total of 5335 patients with unruptured IA were matched by age and sex with 80,025 controls at a ratio of 1:15. We estimated the odds ratios (ORs) and corresponding confidence intervals [CIs] between thyroid diseases and unruptured IA using a multivariable conditional logistic regression model.
Results:
Tobacco smoking, use of antihypertensive medication, and hypothyroidism were significantly associated with an elevated risk for unruptured IA in univariate analysis. In multivariable analysis, a history of hypothyroidism was associated with unruptured IA (adjusted OR: 1.46 [CI: 1.26–1.69]). Among patients with hypothyroidism, long-term use of thyroid hormone for >5 years was associated with a reduced risk for unruptured IA (adjusted OR: 0.69 [CI: 0.48–0.99]). A history of hyperthyroidism was associated with a reduced risk for unruptured IAs (adjusted OR: 0.71 [CI: 0.54–0.93]). In secondary analyses of the data according to sex, the respective observed associations between hypothyroidism and hyperthyroidism and the risk of IAs were found to be statistically significant in females but not in males.
Conclusions:
Hypothyroidism is associated with an increased risk of unruptured IAs, whereas hyperthyroidism is associated with a reduced risk. Overall, the findings suggest that thyroid hormones may play a protective role in the development of unruptured IAs. Further studies are needed to clarify potential direct causality and the biologic mechanisms relating thyroid dysfunction and unruptured IA.
Introduction
The prevalence of unruptured intracranial aneurysms (IAs) is ∼3% in adults. 1,2 Although most unruptured IAs are asymptomatic, they may lead to catastrophic sequelae if they rupture. 3 Therefore, preemptive recognition and management of relevant risk factors are very important. Age, sex, ethnicity, family history, and genetic diseases are unmodifiable risk factors for unruptured IAs, whereas smoking and hypertension are well-known modifiable risk factors. 2,4 –9 However, many cases of IA are identified without known risk factors.
Thyroid function disorders, such as hypothyroidism and hyperthyroidism, are common endocrine disorders. Epidemiological studies have suggested that hypothyroidism and hyperthyroidism are associated with cardiovascular diseases. Hypothyroidism is associated with atherosclerosis and related risk factors, such as hypertension, hyperlipidemia, and endothelial dysfunction. 10 –12 Hyperthyroidism is associated with atrial fibrillation, cardiovascular thromboembolic events, and related mortality. 13,14 A nationwide study demonstrated that hyperthyroidism and hypothyroidism were associated with an increased risk of cerebrovascular disease, such as ischemic stroke. 15 However, there are few reports on the relationship between thyroid diseases and IA, with limited sample sizes. 16,17 This study investigated the relationship between thyroid diseases (hypothyroidism and hyperthyroidism) and development of IA, utilizing nationwide population-based cohort data from Korea.
Materials and Methods
Data sources
We conducted a nested case–control study using the Korean National Health Insurance Service—National Sample Cohort (NHIS-NSC). The NHIS covers ∼97% of the Korean population. 18 The NSC represents a randomly selected sample of 2.2% of all Korean citizens eligible for inclusion in the NHIS-NSC. The NHIS-NSC contains information on demographic factors, claims for inpatient and outpatient visits, medical check-ups, and medical prescriptions from 2002 to 2019. 18,19
Case identification and control selection
From the NHIS-NSC (n = 1,137,861), we selected 5869 subjects who were diagnosed with unruptured IA at least twice as a main or sub-disease in claim data (the 10th International Classification of Disease [ICD-10] code I671) (Fig. 1). 20 Subjects who were younger than 20 years of age at the time of diagnosis (n = 10), subjects who were diagnosed before January 2003 (n = 42), and subjects who did not have medical check-up records (n = 482) were excluded. A total of 5335 patients diagnosed with unruptured IA from 2003 to 2019 were selected as the case group. Figure 2 illustrates the study design. The index date was defined as the initial date of unruptured IA diagnosis in inpatient or outpatient claims. The exposure periods of tobacco, alcohol, antihypertensive drug usage, and medical history of thyroid disease or cancers were defined from 2002 to the index date.
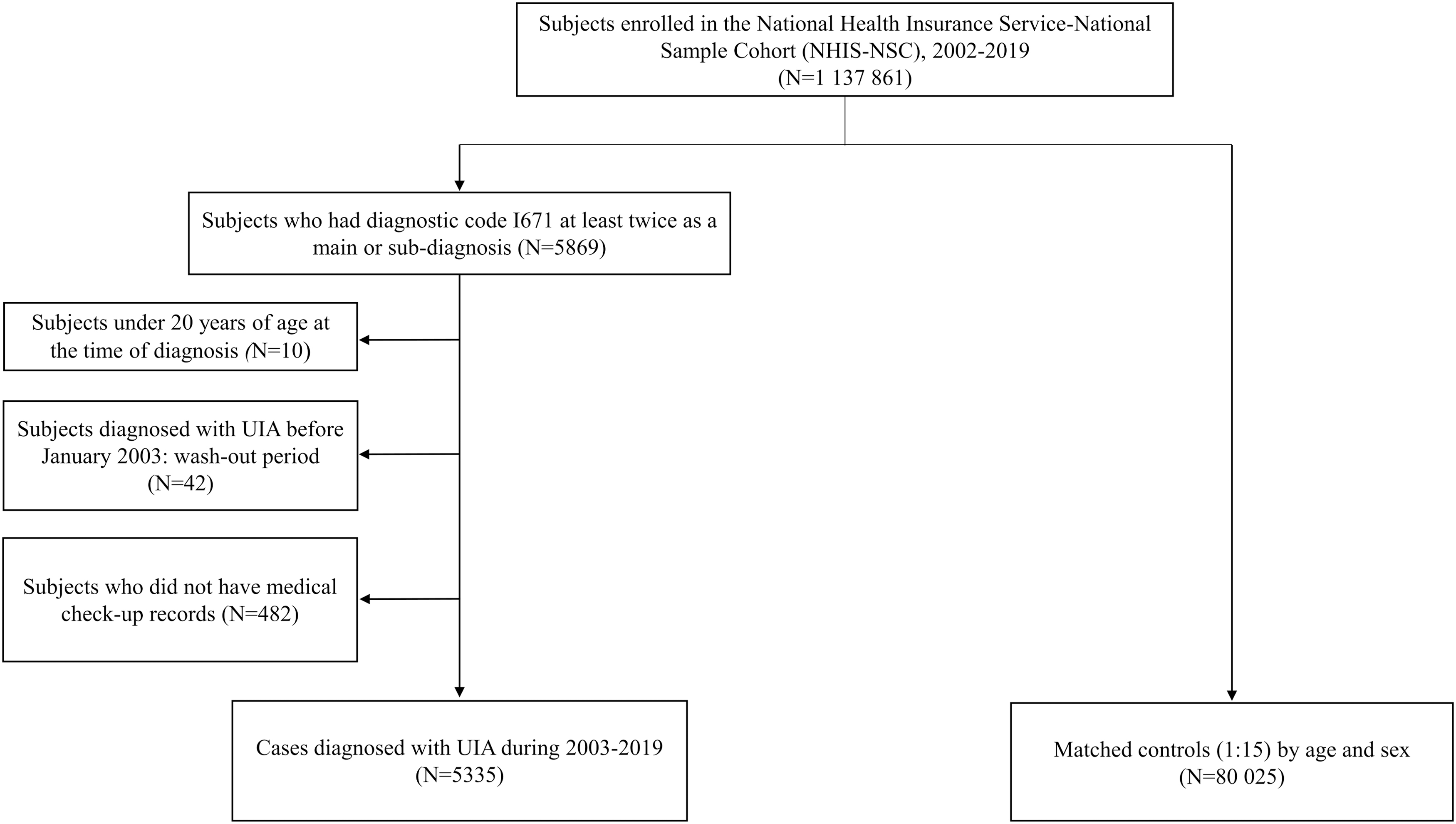
Flowchart of case–control dataset selection. UIA, unruptured intracranial aneurysm.
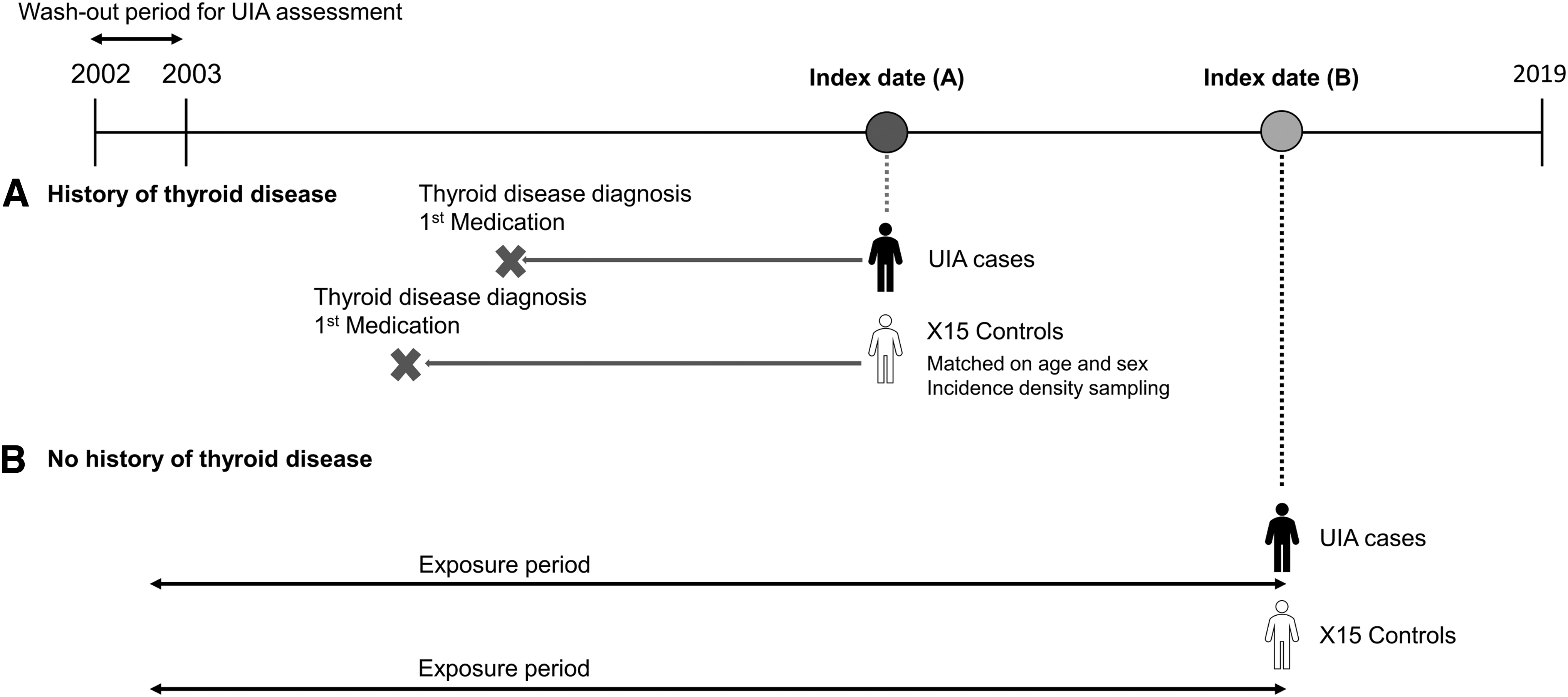
Design of the study. The index date was defined as the initial date of UIA diagnosis in inpatient or outpatient claims.
Incidence density sampling was used to match cases to age- and sex-matched controls in a 1:15 ratio, which resulted in 80,025 controls. For subjects with a history of thyroid disease, the periods of medication exposure for thyroid disease were defined from the initial date of thyroid disease diagnosis to the index date (Fig. 2A).
Definition of thyroid diseases
Patients with hyperthyroidism were defined as individuals who were diagnosed with the ICD-10 codes E050–E059 at least twice as a main or sub-disease and prescribed one of the antithyroid medications at least twice for no less than 60 days. 21 The antithyroid medications are given in Supplementary Table S1. Based on in vivo efficacy, the dose of antithyroid medication was adjusted at the following ratio: methimazole (MMI) 5 mg as 1T (reference), propylthiouracil 50 mg as 1T, MMI 2.5 mg as 0.5T, carbimazole 5 mg as 0.6T, and carbimazole 10 mg as 1.2T. 22
Patients with hypothyroidism were defined as individuals (1) who were diagnosed with one of the following ICD-10 codes at least twice as a main or sub-disease (E01, E010–E012, E018, E02, E03, E030–E035, E038–E039, E04, E06, E060–E065, E069, E07, E071, E078, E079, O905) and (2) who were prescribed thyroid hormone medications at least twice for no less than 60 days. 21 Patients with thyroid cancer were defined as individuals who were diagnosed with C73 at least twice as a main or sub-disease. A list of procedures and treatments related to the treatment of hypothyroidism and thyroid cancer are provided in Supplementary Table S1.
Assessment of medications related to thyroid diseases
We collected all the prescription data regarding antithyroid and thyroid hormone medication before the index date and calculated the daily medication dose using the PROC SQL function. We estimated the duration of thyroid medication use and categorized it into four groups: over 60 days and <1, 1–3, 3–5, and ≥5 years. The mean daily dose of thyroid medication for each patient was categorized as follows: antithyroid medication: <10, 10–20, and 20–100 mg/day; and thyroid hormone medication: <50, 50–100, and ≥100 μg/day. We also estimated the time interval between the initiation of prescription and IA diagnosis and categorized the duration into four groups: <1, 1–2, 2–4, and ≥4 years.
Covariate information
History of thyroid disease and cancer diagnosis were extracted from the NHIS-NSC. Smoking and drinking status were extracted from data from the health check-up performed on the date closest to the index date.
To identify medication adherence levels for thyroid and antihypertensive medications, we used the proportion of days covered (PDC), which is one of the most common methods used to assess medication adherence, in the case and control groups. The list of antihypertensive medications is provided in Supplementary Table S1. The PDC was calculated as the number of days with drug on hand divided by the number of days in the specified time interval, and only information before the index date was used. 23 We categorized medication adherence into two groups, <80% and ≥80%, for comparison.
Statistical analysis
Conditional logistic regression analysis was used to estimate the odds ratios (ORs) and corresponding 95% confidence intervals [CIs] for the association between each variable and unruptured IA. An unadjusted model and model adjusted for antihypertensive medication adherence and ever use of tobacco were generated. All analyses were performed using SAS 9 · 4 software (SAS Institute, Cary, NC). 24
Ethics approval
The Institutional Review Board of Seoul National University College of Medicine/Seoul National University Hospital granted an exemption for this study (approval no.: 2105-044-1218) as all analyses were performed on publicly accessible data that did not contain any personally identifiable information.
Results
Baseline characteristics
Table 1 provides the general characteristics of 5335 patients with unruptured IA and 80,025 controls. The mean age of patients in both groups was 60.4 ± 11.9 years, and 31.5% were males (case: 1682, control: 25,230). Univariate regression analysis showed that ever use of tobacco was associated with a higher risk for unruptured IA (OR: 1.31 [CI: 1.20–1.43]), and alcohol consumption was not associated with the risk of unruptured IA (OR: 1.04 [CI: 0.97–1.11]). The use of antihypertensive medication was associated with unruptured IA (OR: 2.09 [CI: 1.96–2.23]). The diagnosis of hypothyroidism was associated with unruptured IA (OR: 1.55 [CI: 1.34–1.79]), and the diagnosis of hyperthyroidism or thyroid cancer showed no association with unruptured IA.
Characteristics of Cases with Unruptured Intracranial Aneurysms and Controls
Values are represented as n (%).
95% CI, 95% confidence interval; OR, odds ratio; PDC, proportion of days covered.
We examined the adherence level of patients relating to the use of levothyroxine or anti-thyroid drugs. In patients with hypothyroidism, the average percentage adherence with levothyroxine formulations was 81.2%, and 67.3% of these patients had a PDC of 80% or greater. In hyperthyroid patients, the average adherence rate for anti-thyroid medications was 79.2%. Of these patients, and 61.5% demonstrated a PDC of 80% or higher.
Association between hypothyroidism and unruptured IAs
Table 2 summarizes the association between hypothyroidism and the incidence of unruptured IA. The diagnosis of hypothyroidism was associated with unruptured IA (adjusted OR: 1.46 [CI: 1.26–1.69]). Stratified analysis of the mean daily dose or duration of thyroid hormone treatment showed no association between medication history and unruptured IA, except for the longest duration of medication (≥5 years). There was no association for the time interval between the diagnosis of hypothyroidism and aneurysm diagnosis, which showed no association with unruptured IA.
Hypothyroidism, Thyroid Hormone Medication and Incidence of Unruptured Intracranial Aneurysms
Adjusted to antihypertensive medication adherence and ever use of tobacco.
Given the predominant occurrence of thyroid disorders in females, 25 –27 we conducted subgroup analyses examining the association between hypothyroidism and incident IA according to sex. The adjusted OR for males was 1.26 [CI: 0.75–2.11], whereas it was 1.48 [CI: 1.27–1.73] for females. Therefore, the strength of association of hypothyroidism and incident unruptured IA was a greater in females (Supplementary Table S3) as compared with males (Supplementary Table S2).
Association between hyperthyroidism and unruptured IAs
We searched for any association between hyperthyroidism and the incidence of unruptured IA using univariate and multivariable logistic regression analyses (Table 3). A multivariable analysis adjusted for antihypertensive medication adherence and ever use of tobacco revealed that the diagnosis of hyperthyroidism was associated with a reduced incidence of unruptured IA (adjusted OR: 0.71 [CI: 0.54–0.93]). Furthermore, similar to the observations in hypothyroidism, there was no significant association in males (adjusted OR: 1.05 [CI: 0.61–1.83]) (Supplementary Table S4), but there was a statistically significant association observed in females (adjusted OR: 0.64 [CI: 0.47–0.87]) (Supplementary Table S5).
Hyperthyroidism, Anti-Thyroid Medication and Incidence of Unruptured Intracranial Aneurysms
Adjusted to anti-hypertensive medication adherence and ever use of tobacco.
Investigation of the dose and duration of antithyroid medication and the time interval between the prescription of these drugs and the diagnosis of unruptured IA did not reveal any significant associations. However, longer use of anti-thyroid drugs and a longer time interval from drug prescription to IA detection were associated with a lower OR for the risk of incident IA (duration of anti-thyroid medication ≥5 years; adjusted OR: 0.35 [CI: 0.13–0.92], time interval from drug prescription to IA detection ≥4 years; adjusted OR: 0.63 [CI: 0.22–1.85]).
Discussion
This nested case–control study examined the association between functional thyroid diseases and unruptured IA. The main findings of this study included that hypothyroidism was associated with a higher risk for unruptured IA, after adjusting for adherence to antihypertensive medication and tobacco use. Long-term thyroid hormone treatment for >5 years was associated with a reduced incidence of unruptured IA. A previous history of hyperthyroidism also appeared to be associated with a reduced risk of unruptured IA. 16,17 To the best of our knowledge, this study is the first nationwide study reporting the potential role of thyroid dysfunction in the development of IAs.
The prevalence of IA in the general adult population is ∼3%, but the reported prevalence rate may vary depending on the type of investigation, study design, and diagnostic modalities. 1,2 The annual incidence of IA has gradually increased owing to the increased routine medical check-ups and the technical development of imaging modalities. 1,2 Unruptured IAs are often detected during annual medical check-ups in Korea, and patients previously diagnosed with other medical conditions might undergo these check-ups more frequently, which could lead to a higher likelihood of IA diagnosis. 2 However, our study found that while hypothyroidism was associated with an increased risk of unruptured IA, hyperthyroidism was associated with a reduced risk. In a secondary analysis, these findings were robust in females but not in males. However, we believe that the frequent evaluations owing to a preexisting medical condition are unlikely to explain the observed association between thyroid dysfunction and IA.
To reduce the risk of severe morbidity and death resulting from IA rupture, it is essential to establish a management plan for unruptured IA based on patient- and IA-related risk factors. Currently known risk factors for IAs include being female and older than 50 years old, having Asian or Finnish ancestry, hypertension, smoking, and certain genetic diseases, such as autosomal dominant polycystic kidney disease, Marfan syndrome and Ehlers–Danlos syndrome. 2,4 –9 This study demonstrated that smoking and hypertension were associated with an increased risk of IA incidence by 1.3- and 2-fold, respectively. Previous studies including smaller study populations showed that hypothyroidism was independently associated with unruptured IA, 16,17 and this study confirms this finding using nationwide population-based cohort data. The OR of hypothyroidism was 1.5 ([CI: 1.3–1.8]), which is comparable with smoking (OR: 1.3 [CI: 1.2–1.4]), a well-known risk factor for IA.
Two previous studies were performed on tertiary hospital-based cohorts with relatively large-sized IAs and demonstrated hypothyroidism as a risk factor for unruptured IAs. 16,17 Atchaneeyasakul et al. performed a case–control study with 243 patients with IA and 243 age-matched controls, with a mean IA size of 9.6 ± 0.8 mm. 16 They reported that hypothyroidism was present in 16.5% of IA patients and 3.7% of controls, with an adjusted OR of 3.2 ([CI: 1.3–7.8]). Chien et al. studied the risk factors for predicting the growth of IA in a longitudinal cohort of 382 patients and demonstrated that hypothyroidism was observed in 17.8% of IA patients. 17 Smoking and hypothyroidism had significant effects on the growth rate of large-sized unruptured IA >7 mm. Although hypothyroidism was consistently associated with unruptured IA, these studies were performed on large IAs in hospital patients with small sample sizes, which makes it difficult to generalize to all IAs.
This study, which was based on a nationwide population-based nested cohort, showed that the prevalence of hypothyroidism in unruptured IA cases was 4%, and the OR of hypothyroidism for unruptured IA cases was 1.5. Of note, these prevalence rates and OR estimates were smaller than previous studies. 16,17 One possible explanation is that the unruptured IA cases from the population-based big data may have included more smaller IAs. Because there has been an increase in unruptured IA cases owing to the increase in health screening with high-resolution imaging modalities that predominantly detect relatively small-sized IA, 2,20 the results of this population-based study may be more applicable to the general population.
The possible biologic relationship between hypothyroidism and unruptured IAs may be explained in several ways. First, these conditions share a common pathophysiology, which is an outcome of hypothyroidism and a contributing factor to the development of unruptured IA. The formation, growth, and rupture of IA involve a combination of heterogeneous pathogenesis, such as proteolysis, apoptosis, inflammation, hemodynamic stress, dissection, atherosclerosis, and genetic backgrounds. 28 Because atherosclerosis, hypertension, endothelial dysfunction, and chronic vascular inflammation are established consequences of hypothyroidism, 10 –12 it plays a pivotal role in IA progression.
Second, thyroid hormone deficiency directly affects the trajectory of IA. Two findings of this study support this hypothesis. Among all hypothyroid patients, a duration of thyroid hormone medication of >5 years was associated with a lower risk of IA compared with patients who took the medication for <1 year, thereby suggesting that long-term replacement of thyroid hormone may play a role in reversing the pathogenic effects of hypothyroidism on IA. A history of hyperthyroidism was associated with a reduced risk of IA, with an adjusted OR of 0.71 [CI: 0.54–0.93]. This finding was unexpected because previous studies reported that a higher level of free thyroxine were associated with an increased cardiovascular risk and activity of angiotensin-converting enzyme. 14,29 –32 Further studies are needed to clarify potential direct causality and the biologic mechanisms relating thyroid dysfunction and unruptured IA.
Our findings suggest that the thyroid hormone status, rather than the underlying pathophysiology such as autoimmunity, may have influenced the development of IA. It is plausible that patients undergoing long-term levothyroxine (LT4) treatment might have encountered phases during which their thyroid hormone levels exceeded the normal range, potentially yielding a protective effect. It is known that thyroid hormones play a positive role in stimulating endothelial cells to generate nitric oxide, culminating in vascular dilation. Although hypothyroidism impedes endothelium-dependent dilation, 12 hyperthyroidism augments the production of endothelial nitric oxide. 33 –35 Nonetheless, it is important to acknowledge that adverse cardiac events, including atrial fibrillation, are also recognized in patients with hyperthyroidism, underscoring the imperative for further research.
The main strength of this study is the use of nationwide population-based data analysis based on claims data, which includes information on disease diagnosis and medical prescriptions. This methodology allowed for a specific assessment of medication history, including the type, dose, and duration of medication, compared with self-reported data.
We recognize several limitations of this study. First, although we defined cases with unruptured IA using the same operational definition as the previous study, there could have been a misclassification bias owing to the use of claims data. This could have led to an underestimation of IA patients in the control group. However, the reported prevalence of unruptured IA in the adult population aged older than 50 years is low, at ∼3.2% [CI: 1.9–5.2]. 1 This potential bias may have been mitigated with the classification of subjects as controls, which resulted in an OR of IA toward the null. Therefore, the effect on the overall conclusion is likely insignificant. Second, the clinical information regarding the results of thyroid function studies such as thyrotropin level, size of aneurysms, or blood pressure levels were not available in the NHIS-NSC.
One of the frequently noted drawbacks in research that utilizes claims databases is the absence of assessments for potential confounding variables such as laboratory data, disease severity, and health behaviors. 36 Still, we believe that this study offers valuable insights into the potential role of thyroid dysfunction and IA using large-scale real-world data. These findings need to be further explored in well-designed clinical studies. Third, the assessment of tobacco and alcohol use was limited owing to the lack of information in some participants of the National Health Screening Program. The missing rate ranged from 11% to 14%, which may be considered high in some contexts. However, because the distribution of missing information was similar between the case and control groups, the impact on the results was likely minimal. Fourth, it is possible that adherence to prescriptions may be lower than our results indicate because we only analyzed medical prescriptions, not actual consumption.
However, there is unlikely to be a significant difference in compliance between the case and control groups. Finally, the NHIS-NSC does not contain information before 2002, which precludes the identification of IA or diagnosis of thyroid diseases before that year.
Conclusion
We found that hypothyroidism is independently associated with unruptured IA, alongside hypertension and tobacco use. Long-term utilization of thyroid hormone medication by hypothyroid patients was associated with a reduced incidence of unruptured IAs. Furthermore, a previous history of hyperthyroidism was associated with a reduced risk of unruptured IAs. Taken together, this study suggests a potential protective role of thyroid hormone on unruptured IA. Further well-designed prospective clinical studies on early IA screening and intervention in IA patients with or without hypothyroidism are needed.
Data Availability Statement
The data that support the findings of this study are available during a permitted period after the approval by the NHIS for a fee. The English site for requesting the Sample Research DB is as follows:
Footnotes
Authors' Contributions
H.P.: Conceptualization (equal); formal analysis (lead); writing—original draft (equal); writing—review and editing (equal); S.W.C.: Conceptualization (equal); writing—original draft (equal); writing—review and editing (equal); S.H.L.: Writing—review and editing (equal); K.K.: Writing—review and editing (equal); H.-S.K.: Writing—review and editing (equal); J.E.K.: Writing—review and editing (equal); A.S.: Conceptualization (equal); formal analysis (supporting); writing—original draft (equal); writing—review and editing (equal); W.-S.C.: Conceptualization (equal); writing—original draft (equal); writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
W.-S.C.: Seoul National University Hospital Research Fund (Grant No.: 0420203080).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5