
Abstract
Background:
The impact of thyroid dysfunction (TD) on the female reproductive system has been extensively documented. While there is evidence suggesting that alteration in female reproductive status may affect thyroid function, conflicting results have prevented definitive conclusions. This study aimed to investigate the associations of parity, spontaneous abortion (mentioned as abortion throughout this study), and menopause status with the prevalence and incidence of TD.
Methods:
From the Tehran thyroid study population, 2711 participants were included in the cross-sectional analysis to explore associations between female reproductive status and TD. Overall, 2191 participants with euthyroid were included in the survival study and followed up in 3-year intervals. Multinomial logistic regression was adopted in cross-sectional analysis and multivariable Cox proportional hazard model was used to determine associations between the incidence of TD with parity, abortion, and menopause status, adjusting for age, smoking, body mass index, and thyroid peroxidase antibodies positivity.
Results:
At the baseline, multiple parities (≥4) were significantly associated with overt hypothyroidism (odds ratio [OR] = 1.12; confidence interval [CI] 1.0–1.26) and subclinical hyperthyroidism (OR = 1.11 [CI 1.03–1.21]). Furthermore, multiple abortions were associated with overt hyperthyroidism (OR = 2.09 [CI 1.02–4.26]). Over the course of the study, multiple parities were significantly associated with the incident subclinical and clinical hypothyroidism. Conversely, a history of abortion was associated with a reduced risk of incident overt hypothyroidism. We found no significant association between menopause status and the prevalence or incidence of either hypothyroidism or hyperthyroidism.
Conclusions:
Our results suggest that the female reproductive system may be associated with thyroid function. Parity and abortion are associated with the occurrence of TD. A deeper understanding of the underlying mechanisms of the cellular and molecular alterations in signaling cascades during pregnancy is necessary to fully elucidate these associations.
Introduction
The association of thyroid dysfunction (TD) with reproductive disorders in females is well-studied. 1,2 The female reproductive system may also influence thyroid function since TD such as hypothyroidism and hyperthyroidism are more common in women. 3 Although studies on reciprocal interactions between reproductive system and endocrine system exist, the influence of female reproductive system condition on TD is still obscure. 4 –6 The controversies in literature regarding the effect of female reproductive system can be attributed to limitations of cross-sectional studies. A decisive conclusion regarding the association of female reproductive system with thyroid function requires long-term studies with proper sample size. However, many cohort studies have not paid adequate attention to the reproductive system’s associations with thyroid function.
Female reproductive system goes through several alterations during life, resulting in changes in hormonal homeostasis. 7 Physiological fluctuations in female reproductive hormones in menstruation cycles can impact other endocrine glands’ functions. Some females experience physiological cycles of pregnancy and lactation during their lifetime that could significantly alter immune system responses and endocrine signaling permanently. Many reports suggest that parity may be associated with breast cancer incidence and endocrine dysfunction such as incidence of diabetes. 8,9 Some observations propose that cycles of pregnancy and lactation can be associated with TD. For instance, higher levels of circulating autoantibodies are detected in the female population. 10 Also, high human gonadotropin hormone levels at early pregnancy can stimulate thyroid activity and lower thyrotropin (TSH). 11 Furthermore, there are constructive hypotheses on the potential mechanisms of how changes in female reproductive system cycles during pregnancies can affect thyroid function, including microchimerism during pregnancy, the effect on thyroid hormone-binding proteins, and the shortening of telomeres. 12,13
Menopause may lead to physiological changes, including the possibility of autoimmune antibodies developing in some women. 14 Although TD can be more common in older female population and although the possible association of TD with postmenopausal period has been discussed, the independent effect of menopause physiological alteration on thyroid function is unknown. 3,15 However, the occurrence of TD due to autoimmunity is a complex phenomenon, and the effect of alterations in cycles of female reproductive system is still obscure. 16
Our previous study investigated the relation of female reproductive status and the incidence of thyroid autoimmunity within the Tehran thyroid study (TTS). It was observed that parity, abortion, and menopause had no significant association with the incidence of positive conversion of thyroid peroxidase antibodies (TPOAb). 17 To extend our previous study, here we investigate the associations between parity, spontaneous abortion (mentioned as abortion throughout this study), and menopause status with the prevalence and incidence of TPOAb-dependent and -independent TD in a similar population of TTS. The result of this study can be a steppingstone for broadening our knowledge regarding the independent effects of female reproductive system on thyroid functions.
Materials and Methods
Study population
This study is conducted in the context of TTS, aimed to assess the natural course, incidence, and long-term impacts of thyroid disorders on metabolic diseases. TTS is a subdivision of the Tehran lipid and glucose study, a prospective population-based cohort study on noncommunicable diseases and their risk factors. 18,19 Participants were volunteers aged ≥20 from Tehran’s District 13, an urban area with almost similar economic status and no recorded iodine deficiency cases. 18
This study was conducted with the approval and under the observation of the ethical committee of the Research Institute for Endocrine Sciences of Shahid Beheshti University of Medical Sciences and in line with policies on research ethics of the institute. A written informed consent has been obtained from each patient after full explanation of the purpose and nature of all procedures used. This study complied with the Declaration of Helsinki and its subsequent amendments.
Participants were surveyed for a period of 12 years with scheduled follow-ups of every three years, over phase 1 to phase 4. The clinical data of participants including the thyroid function and reproductive system status were assessed separately at each four phases. From 3406 women who participated in the TTS, 695 individuals were excluded from this study at baseline due to misreported parity data at the time of examinations (n = 370), pregnancy at the time of interview (n = 46), history of thyroid surgery (n = 43), incomplete data (n = 232), and unreasonable and unreliable TSH and/or free thyroxine (fT4) laboratory values (n = 4). Therefore, 2711 participants were included in the cross-sectional analysis, regardless of their thyroid function status, to explore associations between female reproductive status and TD. To perform survival analysis, of 2711 individuals who underwent cross-sectional analysis at baseline, 520 were excluded during follow-up as 449 had thyroid disorders, 57 were pregnant during at least one follow-up visit, and 14 underwent thyroid surgery. Eventually, 2191 participants were included in the longitudinal analysis (Fig. 1).
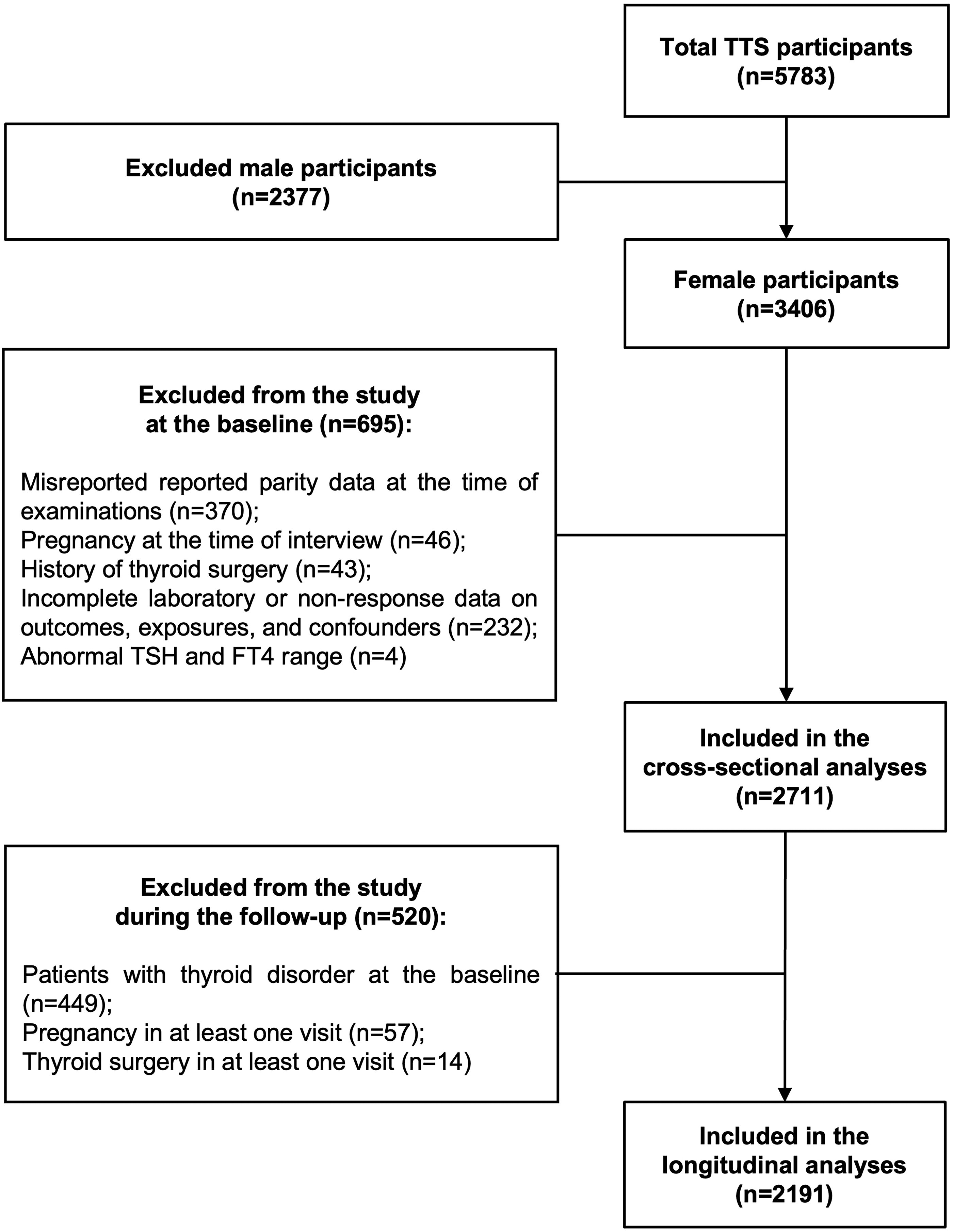
Flow diagram of the study participants.
Laboratory analysis
All laboratory data were gathered from fasting blood samples of participants at the end of every follow-up visit. After the visit, plasma of drawn blood samples was immediately stored at −70°C following a 30–45 minutes centrifuge. FT4 and TSH values were calculated using electrochemiluminescence immunoassay (GmbH). For validating the accuracy of the tests, quality control material (Bio-Rad Laboratories) was used. The inter- and intra-assay coefficients of variability (CVs) were 3.7% and 1.3% for fT4 and 4.5% and 1.5% for TSH assessments, respectively. TPOAb concentrations were determined using an immune-enzymometric assay (Monobind) and the Sunrise ELISA reader (Tecan Co.) by inter- and intra-assay CVs of 4.7% and 3.9%, respectively. All the above stages were performed in the same laboratory.
Definition of terms
Parity was defined as the number of pregnancies that survived >20 weeks after gestation. Abortion was defined as miscarriage before 20 weeks of pregnancy. 20 Menopause was defined as the physiological absence of menstrual cycles for at least 12 months. TPOAb positivity was defined as TPOAb levels ≥35 IU/mL.
Euthyroidism was defined as 0.32≤ TSH ≤5.06 and normal reference limits of fT4, without thyroid medication or other interfering agents. Subclinical hypothyroidism and overt hypothyroidism were defined as TSH >5.06 IU/mL and 0.91≤ fT4 ≤ 1.55, and TSH > 5.06 IU/mL and fT4 < 0.91 ng/dL, respectively. Subclinical hyperthyroidism and overt hyperthyroidism were defined as TSH < 0.32 mIU/L and 0.91 ≤ fT4 ≤ 1.55 ng/dL, and TSH < 0.32 IU/mL and fT4 > 1.55 ng/dL, respectively. 21
Statistical analysis
Parities and abortions were analyzed using the number of pregnancies and abortions as binary variables (0, ≥1) as well as continuous variables. Quantitative and categorical data are expressed as mean ± standard deviation and number (%), respectively. Reproductive and demographic characteristics are presented at baseline. Chi-square or Fisher’s exact test is used for comparing categorical data, while independent Student’s t-test is used for continuous quantitative variables.
In cross-sectional analysis, to determine the associations of parities, abortions, and menopause status as independent variables with TD (subclinical hypothyroidism, overt hypothyroidism, subclinical hyperthyroidism, and overt hyperthyroidism) at baseline, we adopted multinomial logistic regression analysis in different models. In these analyses, after obtaining odds ratios (ORs) and confidence intervals (CIs) in the crude model, adjustments were made for age, smoking status, body mass index (BMI), and TPOAb positivity.
In longitudinal analysis, incidence rates per 1000 person-years for subclinical and overt hypothyroidism and hyperthyroidism were estimated from 1999 to 2012. In all analyses, TD is considered as the outcome. A multivariable Cox proportional hazard model was used to estimate hazard ratios (HRs) and CIs for the association between each definition of thyroid disease with each measure of parity, abortion, and menopause status. Statistical analyses were performed using STATA Statistical Software (Release 14). Significance was set at p-value <0.05, or an OR/HR with CI not including 1.0 was regarded as statistically significant.
Results
Table 1 summarizes thyroid function status and thyroid-related characteristics at the baseline. The average age of participants was 40.7 ± 13.5 years. At the initial phase of the study, 29% of participants were postmenopausal. Furthermore, 2477 participants had at least one successful pregnancy (91.3%) and 775 women (28.5%) experienced at least one abortion. At the baseline, women with at least one successful pregnancy had significantly lower fT4 concentrations (1.25 ± 0.26 vs. 1.16 ± 0.26). Although not significant, the number of parities was associated with higher positive TPOAb levels. Likewise, the postmenopausal period was accompanied by a significant increase in TPOAb positivity.
Sociodemographic and Thyroid-Related Characteristics, According to the Number of Parities, Abortions, and Menopause Status, N = 2711
Data are presented as mean ± standard deviation or number (percentage).
BMI, body mass index; fT4, free thyroxine; N, number; SD, standard deviation; TSH, thyrotropin; TPOAb, thyroid peroxidase antibody.
Independent student’s t-test.
Chi-square test.
Fisher’s exact test.
Prevalence of TD and related ORs with regards to the reproductive system status at the baseline are demonstrated in Table 2. Multiple parities were significantly associated with overt hypothyroidism (OR, CI: 1.12, 1.0–1.26) and subclinical hyperthyroidism (OR, CI: 1.11, 1.03–1.21). In additio, it was observed that women with >5 parities (≥6) are associated with a higher occurrence of subclinical hyperthyroidism (OR, CI: 3.75, 1.46–9.66), and women in the category of 4–5 parities were significantly associated with overt hyperthyroidism (OR, CI: 5.0, 1.11–22.39). Likewise, multiple abortions were associated with overt hyperthyroidism (OR, CI: 2.1, 1.02–4.26). Furthermore, menopausal status was not associated with TD.
Odds Ratios (Confidence Intervals) for the Prevalence of Thyroid Dysfunction by the Number of Parities, Abortions, and Menopause Status: Tehran Thyroid Study (1999–2012), N = 2711
All data are presented as odds ratio [CI], multinomial logistic regression for each reproductive characteristic, separately were adjusted for age, smoking status, BMI, and TPOAb positivity.
CI, 95% confidence interval; OR, odds ratio.
Table 3 presents the incidence rates of TD by the age, parity, abortion, and menopause status throughout the study period. The incidence rates per 1000 persons-years of subclinical and overt hypothyroidism were 15.2 (CI: 13.5–17.2) and 3.3 (CI: 2.5–4.3), respectively; corresponding values for subclinical and overt hyperthyroidism were 3.27 (CI: 2.51–4.27) and 1.55 (CI: 1.05–2.27), respectively. No subclinical hyperthyroidism was identified among the participants during 12 years of follow-up. Fig. 2 shows cumulative incidence rate of the hypo and hyperthyroidism and subclinical hypo and hyperthyroidism as a function time in years.
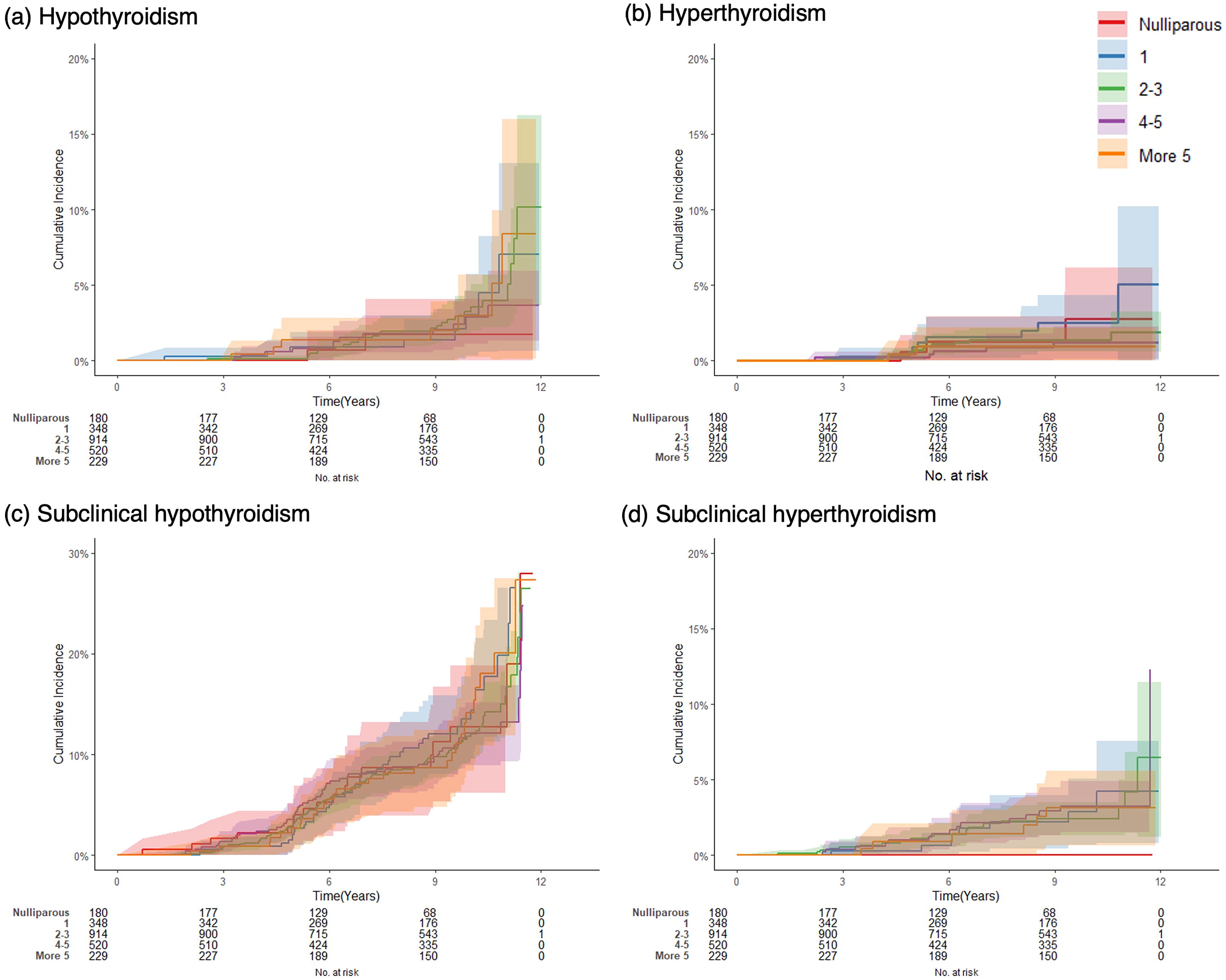
Cumulative incidence rate for
Incidence of Thyroid Dysfunction by the Number of Parities, Abortions, and the Menopause Status: Tehran Thyroid Study (1999–2012), N = 2191
Incidence rates per 1000 person-years for subclinical hypothyroidism, overt hypothyroidism, subclinical hyperthyroidism, and overt hyperthyroidism.
HRs for the incidence of TD by the number of parities, abortion, and the menopausal status during the follow-up are shown in Table 4 and the cumulative HR for various TD is visualized in Fig. 3. Adjusted HRs of each parity for subclinical hypothyroidism and overt hypothyroidism were 1.1 (CI: 0.99–1.19) and 1.2 (CI: 0.99–1.45), respectively. Multiple parities (≥4) significantly increased the risk of subclinical and overt hypothyroidism. An unexpected finding in our study was the significant association between abortion and a lower risk of overt hypothyroidism. The adjusted HR of every abortion for overt hypothyroidism was 0.52 (CI: 0.27–1.0). Regarding the menopausal status, no significant difference was found between premenopausal and postmenopausal women.
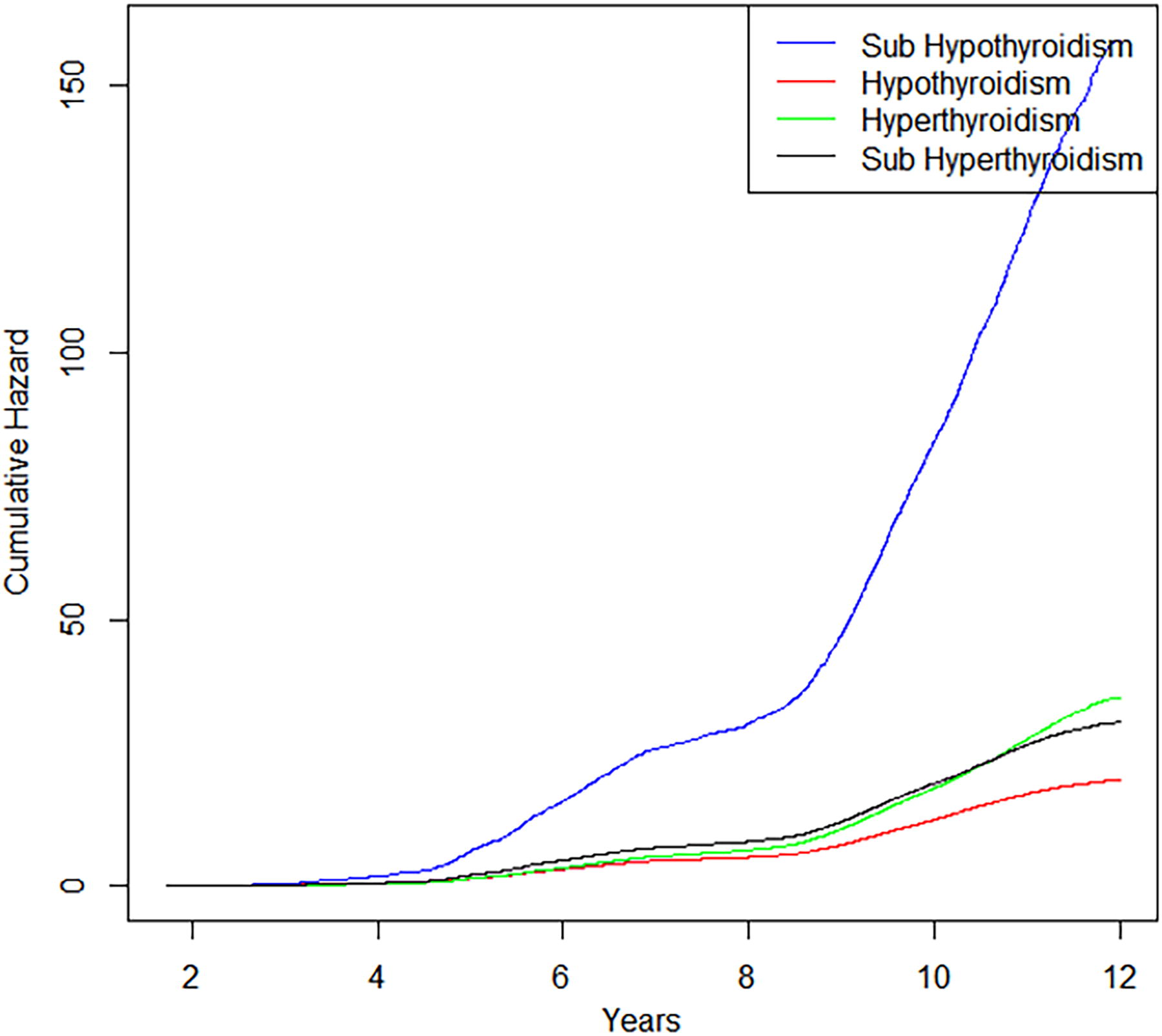
Cumulative hazard ratio for hyperthyroidism, hypothyroidism, subclinical hypothyroidism, and subclinical hyperthyroidism.
Hazard Ratios (Confidence Intervals) for the Incidence of Thyroid Dysfunction by the Number of Parities, Abortions, and Menopause Status: Tehran Thyroid Study (1999–2012), N = 2191
Based on multivariable Cox proportional hazard model adjusted for age, smoking status, BMI, and TPOAb positivity. All data are presented as HRs [CI].
HR, hazard ratio.
Discussion
This study showed a significant association between parity and the prevalence of overt hypothyroidism and subclinical hyperthyroidism. After adjustment for age, smoking status, BMI, and TPOAb positivity, the prevalence of overt hyperthyroidism is associated with multiple abortions. Moreover, HRs showed a significant association of parity with higher incidences of subclinical and overt hypothyroidism. Conversely, history of abortion is significantly associated with a lower incidence of overt hypothyroidism. No significant association between menopause and TD was observed.
These observations underline the close interactions between the female reproductive system and thyroid function. This result suggests a significant increase in the HR for subclinical and hypothyroidism with each additional pregnancy. Similarly, a cross-sectional study found a nonstatistically significant increase in hypothyroidism odds with more pregnancies. 22 A study conducted in Greece found TSH levels significantly higher in mothers with one pregnancy compared with those with none or multiple pregnancies. 23 Our research indicated that >4 parities were significantly associated with higher rates of clinical and subclinical hypothyroidism incidence. This observation could not be reported in many previous studies due to the small sample size. Contrary to our findings, the Wickham survey showed no significant increase in incidence of TD after parity, and postpregnancy thyroiditis did not result in an increase in TD. 3
To accurately assess the impact of reproductive status on TD, we adjusted our results for TPOAb positivity, age, smoking status, and BMI, taking into account previous reports that suggested an association between autoimmune TD and the number of pregnancies. 24 We have also reported the incidence rates stratified by four age categories to provide a more specific understanding of the potential dilution effect due to varying ages of participants on the incidence of TD. Our previous study found that parity was not associated with the incidence of TPOAb positivity, consistent with other reports 6,17,25,26 but contradicting the report from Friedreich et al. 24 It was also observed that an increase in the incidence of hypothyroidism could not be necessarily aligned with an increase in autoimmune TD. 27 However, considering the complex signaling of autoimmune TD, herein, we adjusted solely for anti-TPO positivity. Although anti-TPO antibodies are the most common antithyroid antibodies in patients with Hashimoto thyroiditis or Graves disease, various other antibodies such as activating and blocking TSH receptor, anti-thyroglobulin, and anti-Na+/I− symporter antibodies have been detected in patients with autoimmune thyroiditis. Currently, many aspects of autoimmune TD remain unclear. Recent findings of thyroid peroxidase in the endometrium and placenta suggest a complex relationship between reproductive and thyroid function. 28 Many studies on pregnancy and thyroid function overlooked other immune autoantibodies, focusing mainly on anti-TPO antibodies. 28 Thus, this led to inconsistencies in the literature. However, our results can indicate that additional autoimmune mechanisms beyond anti-TPO may influence the long-term effects of reproductive cycles on pregnancies. In addition, factors such as iodine deficiency and socioeconomic status may influence hypothyroidism; however, the direct impact of socioeconomic status on TD remains to be established. 29 However, iodine deficiency is not a common finding in Tehran District 13 and participants have almost similar socioeconomic status, suggesting other unknown factors could contribute to these observations. Iron deficiency and silent anemia should also be considered, given that lower serum ferritin levels in early pregnancy can be associated with subsequent TD. 30
The relationship between pregnancy and the occurrence of hyperthyroidism, including transient hyperthyroidism episodes, remains debatable. 31 Earlier small-scale studies indicated a potential association between pregnancy and a higher incidence of Graves’ disease. 32 Furthermore, studies have shown higher rates of hyperthyroidism early in pregnancy and 7–9 months postpartum. 33 However, many other studies suggested that the association between Graves’ disease and pregnancy is weaker than previously reported. 34 Our findings demonstrate that parity is not associated with a higher risk of subclinical and overt hyperthyroidism incidence. Higher incidence rate of postpartum hyperthyroidism in previous studies can be attributed to the immunological and hormonal changes during pregnancy, which can temporarily influence the course of disorders. 35
Our earlier study found no association between abortion and HR for TPOAb positivity. 17 However, other studies suggest that abortion may increase TPOAb positivity, supporting the hypothesis of microchimerism’s effect on autoimmune dysfunctions during pregnancy. Therefore, we adjusted the results for TPOAb positivity to achieve a more accurate view of the factors contributing to TD. Interestingly, we found that abortion is associated with a reduced risk of developing subclinical and overt hypothyroidism. This may be due to postabortion hormonal imbalances. Combined with other observations of our study, which indicated that parity is associated with a higher HR for subclinical and overt hypothyroidism, we hypothesize the changes at cellular and molecular levels during the third trimester could be responsible for these observations. Changes in endocrine and paracrine signaling in third trimester have been associated with alterations in protein production and the immune system that can potentially influence thyroid functions. 36,37 Furthermore, while TPO mRNA is expressed in breast, endometrium, and placenta, the function of ectopic TPO remains unclear. Anti-TPO positivity during pregnancy is associated with postpartum TD and has also been suggested to have an association with pregnancy course. However, further studies are needed to explore alterations in TPO gene expression throughout the course of pregnancy. Studies show that normal thyroid function is crucial for fetal survival in the first and second trimesters. Furthermore, the role of other antithyroid autoantibodies on placenta and endometrium is not investigated. 28 Spontaneous abortion may be associated with alterations in TPO expression or function in endometrium or other antithyroid targets, potentially contributing to modulation of long-term immune system responses before 20 weeks of pregnancy. Further evaluation of the local endometrial expression of TPO, endometrial targets of antithyroid antibodies, and effects of abortion on endometrium and immune system are crucial for devising proper hypotheses. From another perspective, variations in chorionic gonadotropin hormone and thyroxine-binding globulin during pregnancy have been discussed to be responsible for different reference values for TSH and fT4 across trimesters. 38
Our results demonstrated no significant association between menopause and the prevalence and incidence of TD. Previous observations of a positive association of autoimmune hypothyroidism with older ages suggest that this result may be related to menopausal status. 39,40 Our results after adjusting for TPOAb positivity and age, suggest that the positive association between age and TD can result from age-related TPOAb conversion and other autoimmune alterations, with minimal impact from changes in female reproductive hormones cycles.
This study has several limitations. One limitation is the absence of other thyroid autoimmunity biomarkers beyond TPO antibodies, such as the potential effect of TSH receptor antibodies, which are associated with Graves’ disease, on the incidence of hyperthyroidism. Furthermore, associations between other autoimmune diseases, such as rheumatoid arthritis, Sjögren’s syndrome, and systemic lupus erythematosus with TD have been suggested; however, they were not explored in this study. 41 –43 In addition, we did not specifically examine individuals for postpartum thyroiditis. These conditions could be relevant confounders due to their association with general autoimmunity, but they were not investigated in the context of this cohort. Although the population’s socioeconomic status was generally similar, certain behaviors and socioeconomic status, including diet, physical activity, and educational status, may be confounders for mothers with more pregnancies. These unassessed factors could affect the study’s results. In addition, the small number of participants with subclinical hyperthyroidism precluded decisive conclusions.
To further improve our knowledge of pregnancy and its association with TD, enhanced knowledge of paracrine and endocrine signaling during pregnancy is essential.
Conclusion
It was observed that every additional pregnancy was associated with an increased chance of developing subclinical or overt hypothyroidism, adjusting the results for age, smoking, BMI, and TPOAb positivity, while abortion was associated with a decreased chance of developing hypothyroidism. This result suggests that several unknown autoimmune mechanisms in the third trimester may be associated with increased vulnerability to developing hypothyroidism and subclinical hypothyroidism. Furthermore, menopause did not appear to affect the risk of hypothyroidism or hyperthyroidism. This suggests that alterations in thyroid function at older ages may be more influenced by TPOAb-related and other significant factors rather than changes in female reproductive hormones.
Footnotes
Acknowledgment
Authors’ Contributions
S.S. conceptualized the work, led the study design, drafted the article, and contributed to data analysis. H.H. contributed to the conceptualization, methodology, and article review. H.A. contributed to data acquisition and article editing. P.A. assisted in data interpretation and article review. S.S. substantially contributed to drafting the article, its revision, and data interpretation. M.T. substantially assisted in conceptualization, study design, data interpretation, and article review. F.A. contributed to data acquisition, interpretation, and article review for important intellectual content. A.A. conceptualized the work, designed the study, and critically reviewed the article. She takes the responsibility for or the acquisition, analysis, and interpretation of data. All authors approved the final version and agreed to be accountable for the accuracy and integrity of the work.
Author Disclosure Statement
The authors declare no potential conflict of interest.
Funding Information
The authors state no funding or external sponsors associated in the authorship and publication of this research.