
Abstract
Background:
International guidelines recommend that the indication to perform thyroid function testing during pregnancy is based on the presence of risk factors for thyroid function test abnormalities. However, the discriminative ability of currently recommended risk factors is questionable. To inform on an update of the American Thyroid Association Guidelines for the Diagnosis and Management of Thyroid Disease in Preconception, Pregnancy, and the Postpartum, we aimed to systematically review the literature to evaluate evidence for current risk factors and potential novel ones for thyroid function test abnormalities in pregnancy.
Methods:
A systematic literature search was performed on Embase, Medline Ovid, and the Cochrane Library from inception to October 17, 2024, to identify articles on the associations of any candidate variables with thyroid function test abnormalities, thyroid antibody positivity, or results of continuous thyroid function tests in pregnancy. Additional records were identified through citation searching. Study quality was assessed using the Newcastle-Ottawa Scale. We summarized the results using a narrative synthesis.
Results:
A total of 81 articles were included, describing 36 candidate variables. Thyroid antibody positivity was associated with a higher risk of overt or subclinical hypothyroidism compared with antibody negativity (absolute risks: 2.4–7.0% vs. 0.1–0.2% for overt hypothyroidism and 1.9–29.0% vs. 2.0–5.7% for subclinical hypothyroidism). In cases of iodine deficiency, sufficiency, and intake above pregnancy requirements or excess, the absolute risks for subclinical hypothyroidism were 2.2–42.6%, 1.42–16.0%, and 3.8–24.3%, respectively. A limited number of studies were available for history of autoimmune diseases, family history of thyroid disease, symptoms of hypothyroidism, and history of pregnancy loss, preterm delivery, or infertility. There was little or no association of current risk factors with isolated hypothyroxinemia or (subclinical) hyperthyroidism. We did not identify novel risk factors for thyroid function test abnormalities.
Conclusions:
Evidence for most currently recommended risk factors remains limited and heterogeneous, and no novel risk factor was identified. While risk factors can help guide thyroid function testing in pregnancy, a clinical risk assessment cannot be replaced. Future studies are needed to detect novel risk factors that can improve the accuracy and efficiency of identifying pregnant women at high risk of thyroid function test abnormalities, in particular, overt hypothyroidism.
Introduction
Adequate thyroid hormone availability is important for a healthy pregnancy and optimal fetal growth and development. 1 Overt and subclinical hypothyroidism are present in about 0.4% and 3.2% of pregnancies, and overt and subclinical hyperthyroidism in about 0.9% and 1.4% of pregnancies. 2 When left untreated, especially overt but also subclinical hypothyroidism are associated with adverse pregnancy and child outcomes, including pregnancy loss, abnormal fetal growth, preterm delivery, gestational diabetes mellitus, pre-eclampsia, and suboptimal offspring neurodevelopment. 3 –11 To mitigate these risks, levothyroxine therapy is recommended for pregnancies complicated by overt hypothyroidism and most cases of subclinical hypothyroidism. 12 To help identify pregnant women at high risk of thyroid function test abnormalities, the 2017 guidelines of the American Thyroid Association (ATA) recommend using a set of risk factors to guide thyroid function testing. 12 However, accurately identifying high-risk women remains a challenge.
The vast majority of women presenting with a thyroid function test abnormality during pregnancy are asymptomatic, and not all current risk factors for identifying high-risk populations have a good discriminative ability. 2,13,14 With the use of the risk factors recommended in the 2017 ATA guidelines, 55–78% of pregnant women would be considered high-risk and could undergo thyroid testing, while the detection rates were only 75–85% and 54–59% for overt and subclinical hypothyroidism, respectively. 12,15 –18 Moreover, in multiple studies, there was no difference in the prevalence of overt and/or subclinical hypothyroidism between the high- and low-risk groups, further verifying a lack of discriminative ability. 15 –17 In a recent individual participant data (IPD) meta-analysis, it was shown that various current risk factors with a high prevalence (e.g., maternal age >30 years, parity ≥2, and body mass index [BMI] >40 kg/m2) are poor screening factors for thyroid function test abnormalities, indicating their limited effectiveness in guiding indications for thyroid function testing. 2 The identification of pregnant women at high risk of thyroid function test abnormalities could be improved with an evidence-based reevaluation of currently recommended risk factors and the addition of novel risk factors with a potentially better discriminative ability and differential absolute risks of clinical significance for thyroid function test abnormalities. However, there is currently no up-to-date overview of relevant risk factors.
As initiated by the ATA Task Force for the Guidelines for the Diagnosis and Management of Thyroid Disease in Preconception, Pregnancy, and the Postpartum, this study was performed to systematically review the literature to summarize evidence on the risk factors currently recommended in the 2017 ATA guidelines and to identify potential novel risk factors for thyroid function test abnormalities in pregnancy.
Methods
This systematic review was reported following the procedures of Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 19
To identify studies for inclusion, we conducted a systematic literature search for articles on the associations of any candidate variables with thyroid function test abnormalities, thyroid antibody positivity, or results of continuous thyroid function tests in pregnancy, published from database inception to September 26, 2022, without language restrictions, using Embase, Medline Ovid, and the Cochrane Library. The primary outcomes of this review were thyroid function test abnormalities, including overt hypothyroidism, subclinical hypothyroidism, isolated hypothyroxinemia, subclinical hyperthyroidism, and overt hyperthyroidism. Secondary outcomes included thyroid antibody positivity and continuous thyroid function tests. A candidate variable was considered as a potential risk factor if there were both statistically significant relative measures of the association and differential absolute risks for the primary outcomes. 20 An update of the literature search was performed on October 17, 2024, and relevant data were retrieved and added to the review. A detailed search strategy can be found in Supplementary Tables S1 and S2. There were also additional relevant studies added through citation searching. Possible studies for inclusion were divided among specific working group members of the Guideline Task Force (T.I.M.K., A.M.L., S.B., C.D., E.K.A., S.M.), and titles and abstracts were independently assessed for suitability in duplicate. Full-text screening was independently performed by two reviewers (Y.L. and T.I.M.K.), and any disagreement was resolved by discussion with a third reviewer (A.M.L.).
We included both observational studies and randomized controlled trials. Studies were excluded if the full text was unavailable, there was a lack of information on thyroid hormone measurements, or they were not written in English. Studies whose populations overlapped with those of another study that had a larger sample size (including meta-analyses) were excluded unless they contributed distinct candidate variables not examined by the larger study, in which case they were retained for those specific variables only. Studies using a fixed upper limit of 2.5 or 3.0 mU/L for TSH or retrieving data only based on diagnosis code (e.g., International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10]) to define overt or subclinical hypothyroidism were excluded from the main study, but were outlined in Supplementary Tables S3 and S4 for specific candidate variables in case of sparse data availability for a risk factor and as a benchmark utility for future studies.
Data extraction was performed by Y.L., and extracted data were organized into frequency tables for different types of thyroid function test abnormalities, thyroid antibody positivity, and continuous thyroid function tests. If a composite outcome was reported, such as elevated or suppressed TSH without regard to FT4, which therefore included both overt and subclinical thyroid dysfunction, it was assigned to the largest category (subclinical hypothyroidism or subclinical hyperthyroidism) to ensure optimal data availability. Data on effect estimates (e.g., odds ratio [OR], relative risk [RR], regression coefficient) as well as absolute risks were extracted if these were reported in the articles. If not provided, and if data permitted, relative risks were manually calculated using MedCalc Software, and absolute risks were estimated based on the frequency or percentage. 21
Quality assessment of included studies was performed by Y.L. using the Newcastle-Ottawa Scale, a risk of bias assessment tool for cohort and case-control studies and in a modified version for cross-sectional studies. 22 –24 Cohort or case-control studies were scored out of a maximum of 9 points across three main categories (selection, comparability, and ascertainment of exposure/outcome) with a total score of ≥7, 4–6, or ≤3 indicative of a high, medium, or low quality of evidence, respectively. 23 Cross-sectional studies were scored out of a maximum of 10 points across three main categories (selection, comparability, and ascertainment of outcome) with a total score of ≥8, 4–7, or ≤3 indicative of a high, medium, or low quality of evidence, respectively. 24
Due to the small number of eligible studies per risk factor and heterogeneous definitions of exposures/outcomes, we were not able to perform a meta-analysis. Instead, we have provided a narrative synthesis of the extracted data. We placed greater emphasis on overt and subclinical hypothyroidism, as there are established treatment recommendations for both conditions during pregnancy, whereas there is no therapeutic indication for either isolated hypothyroxinemia or non-Graves’ hyperthyroidism. 12
Results
After excluding duplicates, the literature search yielded 1686 records. Following title and abstract screening, 130 full-text articles were assessed, 79 of which were included. Two additional articles were retrieved as a result of citation searching. In total, 81 articles were included in the systematic review (Fig. 1). 2,13,18,25 –102 We identified 36 candidate variables, of which 11 are currently recommended in the 2017 ATA guidelines, and 25 are not addressed by the 2017 ATA guidelines but were explored for the associations with thyroid function test abnormalities in our literature search (Table 1). For other currently recommended risk factors, including presence of a goiter, history of head or neck radiation, prior thyroid surgery, the use of amiodarone or lithium, and recent administration of iodinated radiological contrast, we did not identify any study assessing them. 12
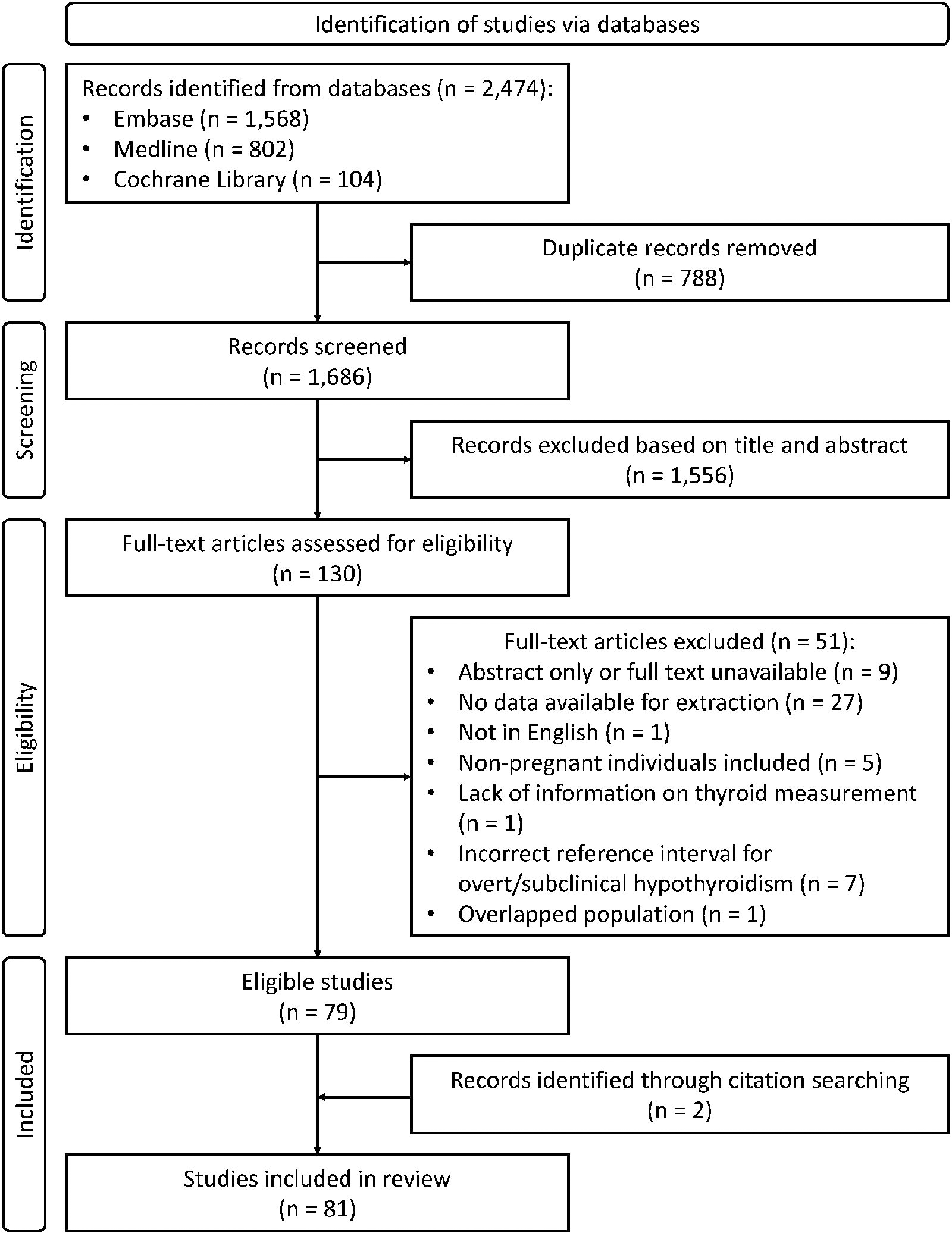
PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Number of Articles Assessing Potential Risk Factors for Thyroid Function Test Abnormalities, Results of Thyroid Function Tests, and Thyroid Antibody Positivity in Pregnancy
BMI, body mass index; EDC, endocrine disrupting chemical; hCG, human chorionic gonadotropin; IVF, in vitro fertilization; PAPP-A, pregnancy associated plasma protein A; PlGF, placental growth factor; sFlt1, soluble FMS-like tyrosine kinase-1; Tg, thyroglobulin.
The details of the 13 studies assessing overt hypothyroidism are described in Table 2, 2,13,36,44,51,54,57,63,81,83,85,92,97 37 studies assessing subclinical hypothyroidism in Table 3, 2,13,18,29,36,39,42,44 –46,51,54,57 –59,61,63,64,67,68,72 –74,76,78,80 –87,91,92,95,97 26 studies assessing isolated hypothyroxinemia in Supplementary Table S5, 2,26,28,35,36,42 –44,46,48,50,51,54,57 –59,63,65,67,69,74,81,83,86,92,97 14 studies assessing subclinical hyperthyroidism in Supplementary Table S6, 2,27 –29,36,42,44,57,76,78,81,84,87,97 9 studies assessing overt hyperthyroidism in Supplementary Table S7, 2,27,36,44,57,59,63,74,97 57 studies assessing results of thyroid function tests in Supplementary Table S8, 2,25,30,32,33,36 –43,45,47 –53,55,56,59 –64,66,68 –71,73 –75,77,79,80,83 –86,88 –90,92 –94,96 –102 and 31 studies assessing thyroid antibody positivity in Supplementary Table S9. 26,31,34,36,45 –51,54,55,58,60,62,63,66,69,73,74,78,83,84,88,89,92,93,96,98,99
Candidate Risk Factors for Overt Hypothyroidism
Gray background, manual calculation based on provided data.
Exposure group vs. comparator group.
Significant relative risk with p-value <0.05.
aOR, adjusted odds ratio; CI, confidence interval; FT4, free thyroxine; ISCED, International Standard Classification of Education; N/A, not applicable; OR, odds ratio; RR, rate ratio; SD, standard deviation; SF, serum ferritin; SIC, serum iodine concentration; sTfR, serum transferrin receptor; TBI, total body iron; TgAb, thyroglobulin antibodies; TPOAb, thyroid peroxidase antibody; TSH, thyroid stimulating hormone; UIC, urine iodine concentration.
Candidate Risk Factors for Subclinical Hypothyroidism
Gray background, manual calculation based on provided data.
Exposure group vs. comparator group.
Significant relative risk with p-value <0.05.
Prevalence = N subclinical hypothyroidism/(N subclinical hypothyroidism + N euthyroidism).
DBP, di-n-butyl phthalate; DEHP, di-(2-ethylhexyl) phthalate; LMWP, low molecular weight phthalate; MBP, monobutyl phthalate; MECPP, mono-(2-ethyl-5-carboxypentyl) phthalate; MEHP, mono-(2-ethylhexyl) phthalate; MEHHP, mono-(2-ethyl-5-hydroxyhexyl) phthalate; MEOHP, mono-(2-ethyl-5-oxohexyl) phthalate; MEP, monoethyl phthalate; MiBP, mono-isobutyl phthalate; MMP, monomethyl phthalate; NO2, nitrogen dioxide; NO x , nitrogen oxides; PAE, phthalate acid ester; PM, particulate matter.
In the quality assessment, 52/54 cohort studies, 3/3 case-control studies, and 16/23 cross-sectional studies were considered high quality (Supplementary Tables S10, S11 and S12). We also included one IPD meta-analysis. Since there is no specific quality assessment tool for IPD meta-analysis, we considered the included IPD meta-analysis high quality because it was conducted with a predefined protocol and registration, a comprehensive search strategy and study selection, a clear data acquisition, a homogeneous and standardized data analysis, a satisfactory technique for assessing risk of bias in individual studies, and a large sample size.
Overt hypothyroidism
Regarding the currently recommended risk factors, there was no association of maternal age, 2 parity, 2 or hypothyroid symptom scores 13 with overt hypothyroidism. TPOAb and/or thyroglobulin antibody (TgAb) positivity was associated with a higher risk of overt hypothyroidism as compared with thyroid antibody negativity. 2,85 The absolute risks for overt hypothyroidism were 2.4–7.0% and 0.1–0.2% for thyroid antibody positivity and negativity, respectively. Higher BMI was overall associated with a higher risk of overt hypothyroidism, while the absolute risk difference for overt hypothyroidism was relatively small according to an IPD meta-analysis (approximately 0.3% for BMI from 20 to 40 kg/m2). 2,51,81 There was only limited evidence to indicate an association of iodine status with the risk of overt hypothyroidism (1/4 studies; adjusted OR for 24-hour urinary iodine concentration [UIC], 0.98; 95% confidence interval [CI], 0.97, 1.00). 54,81,83,92
As for potential novel risk factors, there was no association of smoking, 2,81 in vitro fertilization (IVF), 2 twin pregnancy, 2,36 iron deficiency, 97 or human chorionic gonadotropin (hCG) level 57 with overt hypothyroidism. One cross-sectional study applying a smaller sample size and a TSH fixed upper limit of 4.0 mU/L indicated a positive association of gestational age at blood sampling and a negative association of maternal education levels with the risk of overt hypothyroidism. 81 However, an IPD meta-analysis using trimester-specific reference intervals for thyroid function indicated a negative association of gestational age at blood sampling and no association of maternal education levels with the risk of overt hypothyroidism. 2
Subclinical hypothyroidism
Regarding the currently recommended risk factors, there was no association of history of infertility with subclinical hypothyroidism. 18 Pregnant women with TPOAb and/or TgAb positivity (7/10 studies), 2,29,39,44,45,73,84,85,87,91 iodine deficiency (2/5 studies), 72,80,83,91,92 or iodine intake above pregnancy requirements or excess (4/6 studies) 39,80,82,83,91,92 tended to have a higher risk of subclinical hypothyroidism. The absolute risks for subclinical hypothyroidism were 1.9–29.0% and 2.0–5.7% (60.7–65.6% and 34.8–36.1% in one outlying case-control study) in cases of thyroid antibody positivity and negativity, respectively. As for iodine deficiency, sufficiency, and intake above pregnancy requirements or excess, the absolute risks for subclinical hypothyroidism were 2.2–42.6%, 1.42–16.0%, and 3.8–24.3% (52.6–53.8%, 41.1%, and 73.7% in one outlying case-control study), respectively. We identified a positive association of personal history of type 1 diabetes and other autoimmune disorders with the risk of subclinical hypothyroidism (RR, 4.8; CI, 1.3, 18.2). 87 There was a negative association of hypothyroid symptom scores with the risk of subclinical hypothyroidism (RR, 0.36; CI, 0.13, 0.98), 13 while excessive weight gain was associated with a higher risk of subclinical hypothyroidism (OR, 7.86; CI, 2.99, 20.7). 18 There was only limited evidence to indicate an association of maternal age (2/7 studies), 2,39,42,44,76,78,87 BMI (1/3 studies), 2,51,81 parity (1/3 studies), 2,44,87 family history of thyroid disease (1/2 studies), 18,87 and history of pregnancy loss (1/3 studies) 18,58,87 with the risk of subclinical hypothyroidism, with the absolute risk differences <5.0% for subclinical hypothyroidism (except 5.7% and 5.3% in case of family history of thyroid disease and history of pregnancy loss, respectively) from a baseline absolute risk of 3–7%.
As for potential novel risk factors, there was no association of alcohol consumption, 95 physical activity, 95 IVF, 2 geographic area, 44 history of abnormal uterine bleeding, 18 hCG, 57 soluble FMS-like tyrosine kinase 1 (sFlt1), 59 placental growth factor (PlGF), 59 or air pollutants 46 with subclinical hypothyroidism. Pregnant women with pre-eclampsia tended to have an elevated predelivery TSH (absolute risk difference: 10%), and history of pre-eclampsia was associated with an elevated TSH measured years after pregnancy (absolute risk difference: 4.8%). 61 In two studies, smoking was associated with a lower risk of subclinical hypothyroidism, 2,87 while there were different associations in the other two studies with relatively small sample sizes. 39,81 There was only limited evidence to support a positive association of maternal education levels (1/3 studies) 2,81,95 or exposure to phthalates 95 with the risk of subclinical hypothyroidism, as well as a negative association of blood iron levels (1/2 studies) 64,97 with the risk of subclinical hypothyroidism. There was no convincing overall association of twin pregnancy 2,36 or gestational age at blood sampling 2,44,63,72,78,80,81,86 with subclinical hypothyroidism. The absolute risks for subclinical hypothyroidism varied from 4.1% to 14.2% across different ethnicities, but no clear, generalizable pattern could be extracted. 58,84,87
Isolated hypothyroxinemia
Regarding the currently recommended risk factors, there was no association of family history of thyroid disease or history of pregnancy loss with isolated hypothyroxinemia. 28,58 Pregnant women with higher maternal age (4/7 studies), 2,42,44,48,65,69,86 higher BMI (4/6 studies), 2,48,51,65,69,81 or higher parity (3/4 studies) 2,44,48,65 tended to have a higher risk of isolated hypothyroxinemia. In an IPD meta-analysis, the absolute risk differences for isolated hypothyroxinemia were approximately 1.6%, 3.1%, and <1.0% for maternal age from 20 to 40 years, BMI from 20 to 40 kg/m2, and parity, respectively. There was only limited evidence to indicate a positive association of TPOAb and/or TgAb positivity (1/4 studies, absolute risk difference 0.9–6.9%), 2,26,28,44 iodine intake above pregnancy requirements or excess (1/3 studies, absolute risk difference 1.0–2.7%), 50,83,92 and iodine deficiency (2/5 studies, absolute risk difference 0.2–12.4%) 43,50,63,83,92 with the risk of isolated hypothyroxinemia.
As for potential novel risk factors, there was no association of IVF, 2 vitamin D, 65 perfluorinated acids, 35 or weekly seafood consumption 48 with isolated hypothyroxinemia. We identified that twin pregnancy 2,36 and iron deficiency or anemia 65,69,97 were associated with a higher risk of isolated hypothyroxinemia. The absolute risks for isolated hypothyroxinemia were 3.3–4.7% and 2.0–2.2% for twin and singleton pregnancy, respectively; 2.1–24% for iron deficiency or anemia, and 1.5–14% for adequate iron status. We also identified a negative association of maternal education levels with isolated hypothyroxinemia, and the absolute risks for isolated hypothyroxinemia were 1.4–8.1%, 1.4–6.4%, and 1.1–1.7% in cases of low, medium, and high education, respectively. 2,81 Two studies indicated that greater gestational age at blood sampling was associated with a higher risk with isolated hypothyroxinemia, 2,44 but there was no association in another two studies with relatively small sample sizes. 50,81 There was only limited evidence to support a positive association of smoking (1/2 studies), 2,81 gravidity, 65 sFlt1, 59 PlGF, 59 and PM2.5 46 with the risk of isolated hypothyroxinemia, as well as a negative association of thyroid volume, 48 hCG 57 with the risk of isolated hypothyroxinemia. There was a difference in the risks of isolated hypothyroxinemia across different ethnicities and different geographic areas, but no clear, generalizable pattern could be extracted. 44,50,58
Subclinical hyperthyroidism
Regarding the currently recommended risk factors, there was no association of maternal age, 2,42,76,87 family history of thyroid disease, 27,28,87 history of pregnancy loss, 87 or iodine status 28,81 with subclinical hyperthyroidism. We identified a positive association of parity with subclinical hyperthyroidism, whereas the absolute risk difference between multiparity and nulliparity for subclinical hyperthyroidism was <2.0%. 2,87 A cross-sectional study with a smaller sample size indicated that higher BMI was associated with a higher risk of subclinical hyperthyroidism. 81 However, an IPD meta-analysis indicated a negative association of BMI with subclinical hyperthyroidism (absolute risks for subclinical hyperthyroidism from approximately 1.3% to 0.8% for BMI from 20 to 40 kg/m2). 2 There was no convincing overall association of TPOAb and/or TgAb positivity with the risk of subclinical hyperthyroidism. 2,29,84,87
As for potential novel risk factors, there was no association of IVF, 2 maternal education levels, 2,81 or iron deficiency 97 with subclinical hyperthyroidism. We identified that twin pregnancy was associated with a higher risk of subclinical hyperthyroidism. 2,36 The absolute risks for subclinical hyperthyroidism were 3.0–7.2% and 1.2–2.2% in cases of twin pregnancy and singleton pregnancy, respectively. There was no convincing overall association of gestational age at blood sampling with the risk of subclinical hyperthyroidism. 2,27,44,78,81 There was only limited evidence to support a positive association of hCG with the risk of subclinical hyperthyroidism. 57 The absolute risks for subclinical hyperthyroidism varied from 1.7% to 11.9% across different ethnicities, but no clear, generalizable pattern could be extracted. 84,87
Overt hyperthyroidism
Regarding the currently recommended risk factors, there was no association of maternal age 2 or family history of thyroid disease 27 with overt hyperthyroidism. We identified that serum iodine concentration (but not UIC) was positively associated with the risk of overt hyperthyroidism. 63,74 There was only limited evidence to indicate an association of BMI, 2 parity, 2 and TPOAb and/or TgAb positivity 2 with the risk of overt hyperthyroidism, whereas the absolute risk differences for overt hyperthyroidism were <1.0% for these risk factors.
As for potential novel risk factors, there was no association of IVF, 2 sFlt1, 59 or PlGF 59 with overt hyperthyroidism. We identified that a twin pregnancy was associated with a higher risk of overt hyperthyroidism. 2,36 The absolute risks for overt hyperthyroidism were 5.7–8.5% and 0.5–1.3% in cases of twin pregnancy and singleton pregnancy, respectively. There was only limited evidence to support a positive association of maternal education levels 2 and hCG 57 with the risk of overt hyperthyroidism, as well as a negative association of smoking, 2 gestational age at blood sampling (1/2 studies), 2,44 and maternal education levels 2 with the risk of overt hyperthyroidism.
Thyroid function tests
Higher BMI (3/4 studies) 2,30,69,84 and TPOAb and/or TgAb positivity (5/5 studies) 2,53,56,75,84 were associated with a higher TSH, while higher parity (2/2 studies) 2,84 was associated with a lower TSH. Higher maternal age (3/5 studies), 2,42,69,84,97 higher BMI (5/6 studies), 2,30,48,53,69,84 and TPOAb and/or TgAb positivity (3/5 studies) 2,53,56,75,84 were associated with a lower FT4. There was no convincing overall association of maternal age 2,42,69,84 or UIC 56,60,69,80,84 with TSH concentrations. Similarly, there was no convincing overall association of UIC 33,56,60,69,75,84,86 or parity 2,84 with FT4 concentrations.
As for potential novel determinants, greater gestational age at blood sampling (2/2 studies) 2,84 was associated with a higher TSH, while smoking (3/4 studies), 2,30,41,69 a twin pregnancy (3/3 studies), 2,32,36 higher levels of blood iron measurements (serum ferritin [SF], total body iron stores [TBI], soluble transferrin receptor [sTfR], hemoglobin; 4/5 studies) 52,53,69,88,97 were associated with a lower TSH. A twin pregnancy (2/3 studies) 2,32,36 and higher levels of blood iron measurements (SF, TBI, hemoglobin; 4/5 studies) 52,53,69,86,97 were associated with a higher FT4, while smoking (3/4 studies) 2,30,41,69 and a greater gestational age at blood sampling (3/4 studies) 2,53,84,97 were associated with a lower FT4. There was only limited evidence to support that maternal education levels 2 and pregnancy associated plasma protein-A 66 were positively associated with TSH concentrations, or that vitamin D, 90 thyroglobulin (Tg), 70 and thyroid volume 48 were negatively associated with TSH concentrations; IVF, 2 vitamin D, 90 Tg, 70 and thyroid volume 48 were positively associated with FT4 concentrations. There was no convincing overall association of sFlt1 or PlGF with TSH and FT4 concentrations. 59,61,66
Thyroid antibody positivity
Pregnant women with a family history of thyroid disease (2/2 studies), 26,73 iodine deficiency (3/5 studies), 50,60,83,92,98 or iron deficiency (2/2 studies) 49,88 had a higher risk of TPOAb and/or TgAb positivity. The absolute risks for TPOAb and/or TgAb positivity were 18.5–22.8% and 8.1–16.5% for women with and without family history of thyroid diseases, respectively; 0.9–14.8% and 5.3–10.1% (19.3% and 20.6% in one outlying cross-sectional study) for iodine deficiency and sufficiency, respectively; and 3.1–6.0% and 10.0–22.1% for iron deficiency and sufficiency, respectively. We identified a negative association of gestational age at blood sampling with TPOAb positivity (4/5 studies). 47,50,58,69,78 There was only limited evidence to support a positive association of BMI (1/4 studies), 48,51,58,88 gravidity, 99 iodine intake above pregnancy requirements or excess (1/5 studies), 50,60,83,92,98 and thyroid volume 48 with the risk of TPOAb and/or TgAb positivity, as well as a negative association of parity (1/4 studies) 45,48,58,73 with the risk of TPOAb and/or TgAb positivity. We did not identify an association of alcohol consumption, 99 geographic area, 50 or symptoms of thyroid disease 26 with the risk of TPOAb positivity. There was no convincing overall association of smoking 58,99 or maternal age 48,58,78,88 with TPOAb positivity. The absolute risks for thyroid antibody positivity varied from 3% to 29.9% and from 10.3% to 12.3% across different ethnicities 31,58,84,89,99 and different seasons of enrollment, 99 respectively, but no clear, generalizable pattern could be extracted.
Discussion
In this study, we systematically searched the literature and reviewed 81 studies to assess the association of 36 candidate variables with thyroid function test abnormalities, thyroid antibody positivity, and the results of continuous thyroid function tests in pregnancy. Out of all risk factors currently recommended in the 2017 ATA guidelines, 12 we found that thyroid antibody positivity remains the most relevant risk factor for both overt and subclinical hypothyroidism. Additionally, we found iodine deficiency, personal history of type 1 diabetes or other autoimmune disorders, and family history of thyroid disease were associated with a higher risk of subclinical hypothyroidism during pregnancy, albeit limited to a few studies. There was a negligible or no convincing overall association of currently recommended risk factors with isolated hypothyroxinemia, subclinical hyperthyroidism, or overt hyperthyroidism. The differentiation capacity of other risk factors currently recommended for thyroid function testing in pregnancy was either absent or relatively small.
For the majority of characteristics that are currently considered risk factors for thyroid function test abnormalities during pregnancy, we identified not only large differences in data availability between risk factors, but also large differences in how that data altogether would support that these risk factors are associated with a significant risk of thyroid function test abnormalities during pregnancy. For example, there was ample data on maternal age, BMI, and parity from heterogeneous, small single-center studies. However, with a homogeneous method and a large sample size, results from a recent IPD meta-analysis suggest that while these characteristics may reach a statistically significant association, there is a relatively small difference in the absolute risks for either (subclinical) hypothyroidism or (subclinical) hyperthyroidism (<2.0%). 2 Consequently, their relevance in guiding thyroid function testing in pregnancy appears limited. For other currently recommended risk factors, evidence remains scant and/or inconsistent. For example, we identified only one study assessing personal history of autoimmune disease, which indicated a higher risk of subclinical hypothyroidism. 87 Similarly, there was only one study on the history of infertility indicating no association with subclinical hypothyroidism. 18 Moreover, results on subclinical hypothyroidism in relation to symptoms of thyroid disease, family history of thyroid disease, and history of pregnancy loss were inconsistent. 13,18,58,87 The inconsistent findings could be due to discrepancies in study populations and different methods of defining reference intervals for maternal thyroid function. Given the limited and/or inconsistent evidence, it is difficult to determine whether these risk factors would be efficient to indicate thyroid function testing. Utilizing risk factors without robust evidence may increase the likelihood of unnecessary thyroid function testing, overdiagnosis, and overtreatment. Therefore, more studies are needed to evaluate current and/or promising risk factors before they can be integrated into clinical guidelines for thyroid function testing in pregnancy.
TPOAb positivity is the most important risk factor for (subclinical) hypothyroidism during pregnancy and is currently used to guide the decision-making for thyroid function follow-up. 1,12 We purposefully added the data on this well-known risk factor as a benchmark of clinical significance, and the absolute risk difference for overt hypothyroidism (∼4.0%) was considerably higher than many of other characteristics except gestational age at blood sampling and maternal education levels studied in a cross-sectional study with a relatively small sample size. 2,81 On the other hand, TgAbs also reflect thyroid autoimmunity, and studies indicate higher TSH concentrations and a higher risk of (subclinical) hypothyroidism in women with isolated TgAb positivity. 2,103,104 While TPOAbs remain the preferred marker to identify thyroid autoimmunity and those at high risk of hypothyroidism, a TgAb measurement may be worth consideration in TPOAb negative women susceptible to autoimmune thyroiditis (e.g., women with a family history of thyroid disease and/or iodine deficiency) who also have a high-normal TSH concentration.
Iodine plays a critical role in thyroid physiology, and iodine deficiency is a known risk factor for gestational hypothyroidism. 105 Consistent with this, we observed in several studies that there was a higher risk of overt or subclinical hypothyroidism in women with iodine deficiency or who lacked iodine supplementation during pregnancy. 68,72,81,92 Interestingly, iodine intake above pregnancy requirements or excess was also associated with a higher risk of subclinical hypothyroidism, 39,82,83,91 possibly due to the Wolff–Chaikoff effect or due to increased thyroid autoimmunity. 106 While living in a severely iodine-deficient area is already recommended as an indication for thyroid function testing, living in an area with high iodine exposure or having been recently exposed to iodinated contrast or other sources of excessive iodine may also pose a reasonable indication for thyroid function testing. However, the evidence on iodine intake above pregnancy requirements or excess remains limited and more studies on pregnant women are required to better quantify the risks.
Other potential risk factors, such as iron deficiency, twin pregnancy, ethnicity, and history of pre-eclampsia, are not included in the current ATA guidelines. 12 First, we identified a higher risk of isolated hypothyroxinemia in women with iron deficiency. 65,69,97 Additionally, in a recent systematic review there was a higher risk of TPOAb positivity in iron deficient women. 107 Neither of these biochemical abnormalities are an indication for levothyroxine treatment, suggesting that iron deficiency is not a relevant thyroid function testing indication during pregnancy. 12 Second, we identified that a twin pregnancy was associated with a higher risk of overt or subclinical hyperthyroidism and isolated hypothyroxinemia. 2,36 This could be explained by a higher concentration of hCG, which stimulates the production of thyroid hormones, and more overt physiological changes that may lower thyroid hormone availability in twin pregnancies (e.g., a greater increase in thyroxine binding globulin, placental type 3 deiodinase expression, and the consumption of thyroid hormone by the fetuses) as compared with singleton pregnancies. 108 –111 The association of twin pregnancy with overt or subclinical hyperthyroidism was more apparent during early pregnancy than late pregnancy, which is compatible with the hCG peak at the end of the first trimester, suggesting a biochemical but likely physiological hyperthyroidism related to the increase of hCG. 2,36,108,109 Accordingly, a transient gestational hCG-induced thyrotoxicosis does not warrant the use of antithyroid drugs, implicating limited value of twin pregnancy added to thyroid function testing indication. 12 Third, some studies reported relevant differences in the absolute risks (>10%) for subclinical hypothyroidism, subclinical hyperthyroidism, and thyroid antibody positivity according to national or ethnic background. 31,84 However, given the locality-specific diversity in national/ethnic backgrounds and the complexity in ethnic identities, it is difficult to draw distinct patterns which would support routine thyroid function testing. 112 Fourth, women with history of pre-eclampsia were found to have a higher risk of elevated TSH concentrations after pregnancy, and the onset of pre-eclampsia seemed to be associated with a higher predelivery TSH as well, which may be caused by antiangiogenic effects on the thyroid gland by placental factors. 59,61 These data suggest that further research is warranted to clarify the association between history of pre-eclampsia with the risk of thyroid function test abnormalities in subsequent pregnancies.
In addition, we could not identify any study in pregnant women on several risk factors known to increase the risk of thyroid dysfunction in non-pregnant populations such as prior thyroid surgery, history of head or neck radiation, and the use of specific medications (e.g., amiodarone, lithium, recent administration of iodinated radiological contrast). 12 Despite the lack of pregnancy-specific data, these risk factors should still be considered as indications for thyroid function testing given their intuitive and well-established risk patterns outside of pregnancy. Nonetheless, quantification of the associated risks could prove meaningful for future risk models and patient counseling.
In this systematic review, we provide an extensive overview of studies on potential risk factors for thyroid function test abnormalities during pregnancy. We initially assessed the potential of a candidate variable to be considered as a risk factor based on statistical significance and relative effect measures. However, our study remains subjective to some extent as the true relevance of any potential risk factor depends on the clinically significant increase in absolute risk and discriminative ability, which should be decided upon by following, for example, the Delphi method. 113 In addition, the heterogeneity in study populations, definitions of thyroid function test abnormalities, and iodine status across regions made it difficult to compare studies or draw consistent conclusions about most risk factors. Discrepancies in definitions of exposures/outcomes also precluded us from performing a meta-analysis. Furthermore, included studies which used alternative approaches to define reference intervals (e.g., a TSH fixed upper limit of 4.0 mU/L and nonpregnancy reference intervals), as compared with population-based trimester-specific reference intervals, were more likely to over- and under-diagnose thyroid function test abnormalities in pregnancy, limiting interpretability of the results. 114
Our study primarily focused on individual risk factors, whereas the co-occurrence and interaction of multiple risk factors may provide a more comprehensive understanding of the development and assessment of thyroid function test abnormalities. In an IPD meta-analysis, maternal age, BMI, smoking status, parity, and gestational age at blood sampling were used to construct receiver operator characteristic curves for overt and subclinical hypothyroidism. 2 With area under the curve values ranging from 0.58 to 0.63, the combined model offered only modest discriminative performance, suggesting that combining individual risk factors did not lead to satisfactory discriminative abilities and further studies to optimize risk factor models are needed.
This systematic review presents a comprehensive overview of risk factors for thyroid function test abnormalities during pregnancy. On the one hand, thyroid autoimmunity, particularly TPOAb positivity, and iodine deficiency were relevant risk factors for (subclinical) hypothyroidism. On the other hand, several currently recommended risk factors, including age, BMI, and parity, were associated with only small differences in the absolute risk for thyroid function test abnormalities, and should be reconsidered for guiding indications for thyroid function testing in pregnant women. Future studies are needed to focus research on key risk factors using consistent definitions. Given the need for improvement in current thyroid function test indications, clinical risk assessment remains essential in medical practice. Additionally, exploring novel risk factors is needed to improve the identification of pregnant women at high risk of thyroid function test abnormalities.
Footnotes
Acknowledgment
The authors would like to thank Ms. Reese S. Braam from Erasmus University Medical Center for her help in double-checking the quality of included studies and data extraction.
Authors’ Contributions
T.I.M.K. contributed to the conceptualization and design of the systematic review. T.I.M.K. designed the search strategy and supervised the study. T.I.M.K., A.M.L., S.B., C.D., E.K.A., S.M., and Y.L. screened and selected the articles. Y.L., J.A.J.O., and T.I.M.K. contributed to the data acquisition, analysis, and interpretation. Y.L. wrote the original draft, and all authors reviewed, revised, and approved the final version of the article. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
This study is funded by a Vidi grant (016.176.331) from the Netherlands Organization for Scientific Research (RPP), by a clinical fellowship from ZonMw, project number 90700412 (RPP) and by the ATHENA project, funded under the European Union’s Horizon 2020 Program for research, technological development and demonstration, grant agreement no. 825161. Y.L. received a scholarship from the China Scholarship Council. The funders had no role in study design, data collection, data analysis, data interpretation, writing of the report, or decision to submit the article for publication.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11
Supplementary Table S12