
Abstract
Neuromuscular disorders encompass a wide category of illnesses with a significant burden on the patient, family, and society. Telehome monitoring presents an alternative for closer follow-up, by ensuring timely transmission of data and prompting medical support before deterioration occurs. We used telehome monitoring devices for amyotrophic lateral sclerosis patients with respiratory failure in a clinic. This instrument directly acts as a digital recorder of parameters received from an external instrument, such as the bi-level ventilator, and contains an internal modem for direct connection to the Internet, thereby allowing bidirectional flexibility in collecting data and parameter changes whenever needed. The use and acceptance of the system was investigated with patients and all therapists involved. The instrument was found to be user-friendly and effective by the researchers, being practical for both patients and therapists. Therefore, it can be integrated into a routine home care application based on a large respiratory rehabilitation center. The device was extensively tested, and in an ongoing randomized controlled study it is being investigated whether this management strategy is able to hasten the ventilator adaptation process and to diminish the overall utilization of health services, with concurrent economic viability. We conclude that home telemonitoring represents a positive contribution to the management of chronic patients and raised awareness of it should be considered in a near future. This portable telemonitoring device provides an opportune approach to better understand and recognize a ventilatory pattern through long-term ventilation monitoring in the home environment.
Introduction
In recent years, there is an emerging literature about the convenient telemedicine solutions to monitor remotely a patient's medical condition at his or her own home. Telemedicine empowers patients and clinicians to share decision making and clinical outcomes, improving continuity of care and efficiency by remote sensing at a distance, especially for the chronically ill. 1 –3 Rapidly evolving telecommunications and information technologies have provided a solid groundwork for telemedicine as a feasible, reliable, and user-friendly tool in medicine. 4 –9 Moreover, the European community considers the use of home telemanagement for chronic disease surveillance to be of main concern and, the “vision for Europe 2020” calls for the implementation of telemedicine collaborative arrangements. 10
In the particular setting of respiratory medicine, there is an enormous potential for such monitoring technology to assist in the provision of better care for those with chronic lung diseases and associated increased incidence and healthcare burden. However, due to the critical nature of long-term conditions, the importance of telemonitoring is usually underrated. There remains a need for robust studies before such monitoring can be recommended for widespread implementation. 11 –17 On the other hand, there is a trend toward noninvasive ventilation (NIV) due to the advent of technological progress, with novel respiratory support devices being developed by manufacturers and made commercially available for the patients themselves in their own familiar environment. 18 This application aims at enhancing handling of patient/device matching and at keeping track of possible ventilation asynchronies, especially in cases of unsupervised NIV.
Amyotrophic lateral sclerosis (ALS) is a good example of a neurodegenerative disease where respiratory failure is the most common terminal event, the reason why NIV plays a crucial role in prolonging survival. 19,20 Adversely, it requires a process of adaptation not always achieved by a significant set of patients, mostly those with rapidly progressive neurological symptoms and those with marked bulbar weakness. In fact, the advantages of new remote/wireless technologies have scarcely been evaluated in neuromuscular patients. 21
We have implemented a telemonitoring instrument in our ALS clinics, which is able to act as a digital recorder of parameters exported from the pulmonary ventilator device. At prescribed time intervals, all collected data are transmitted to a Web server, which connects directly to the Internet via an internal modem. Our portable medical instrument technically gives the possibility of remotely monitoring home-ventilated ALS patients, by using embedded memory in the device, thereby facilitating posterior online analysis of ventilator parameters and remotely tuning the sets of the ventilator according to the patient's needs and comfort.
Materials and Methods
Setting
In our reference ALS clinics, a collaborative multidisciplinary team is responsible for the treatment for roughly 170 ALS patients of whom about 100 are home ventilated with the Goodknight 425ST® Bi-level device (Tyco Healthcare Group LP). The workgroup encompasses two consulting physiatrists, two consulting neurologists, a physiotherapist, an occupational therapist, a speech trainer, a social worker, and a psychologist. The aim is to provide the best quality of life in all phases of the disease by providing the best of care as close as possible to the patient's own environment, coupled with support for caregivers and community care suppliers. In-house visits by the cardiopulmonology technician play a crucial role in the implementation and management of telemonitoring. These visits average once per 1–3 weeks per patient, and the frequency rises for patients with end-stage disease.
Indeed, the geographical area covered by the ALS clinics is sometimes significantly large and sparsely populated, with consequent higher overhead financial constraints due to traveling time. No support can be given to patients' caregivers during travel, and therefore this time cannot be reimbursed by the healthcare service. In view of the excessive costs in healthcare utilization along with the scenario of struggling compliance these patients must burden, the application of tele-treatment has been regarded by us as a convenient approach in addition to the standard mode of care.
Our medical instrument firmware encompasses a motherboard, a main CPU (microprocessor), and additional electronic units used for the input/output functionalities. The main board is composed of different slots in which electronic boards for parameter measurements are inserted, thereby allowing appropriate flexibility of use. In our specific scenario, a slot is used to interface to the external pulmonary ventilator that the patient is connected to.
The instrument contains an internal modem matching all the necessary requirements for electromagnetic compatibility and safety. It permits wireless access to the Internet via an integrated transmission control protocol/Internet protocol (TCP/IP) and the storage of data in the instrument (data memory embedded) outside of the hospital environment, that is, wherever the patient uses the ventilator. Through the interface boards, especially the ventilation board, the device acts as a digital recorder of data measured by the ventilator connected. It is also noting that in case there is an abnormal electronic event, the architecture of the instrument circuitry prevents its propagation, allowing both device and patients safety.
The communication between server and instrument is designed to be bi-directional, so that it is possible to send a new file setup or a new firmware version. Therefore, this bi-directionality in the system allowed not only registering compliance data but also to introduce modifications in parameters settings, hence signifying a real-time evaluation of its impact on ventilator mechanics. Also, patients themselves are supposed to activate the system from time to time and warn the physician in charge whenever they feel uncomfortably symptomatic and/or notice any kind of device breakdown. The telemonitoring instrument provided herein by the Bi-level equipment Goodknight 425ST device, which is the smallest, lightest bi-level device on the market. It includes backup rate/assist control as well as a patented flow sensor technology that allow the physician to customize the inspiratory and expiratory settings for better patient ease and synchronicity.
Goodknight 425 ST Bilevel Machine
The GoodKnight 425ST BiLevel machine is comprehensive to monitor therapy effectiveness and comes with new FlowSens Technology. The system is designed for daily use or travel. The 425ST has a Backup Rate that helps manage breathing. The FlowSens technology, Backup Rate, and software are the most complete solution on the market for treating sleep apnea. The unit is manufactured by Puritan Bennett (
An air flow sensor is inserted into the patient's tube circuit that brings air from the ventilator, providing a resistance to the airflow due to lumen narrowing. This flow sensor connects to the ventilation board where a differential pressure sensor measures the pressure difference at both ends of the flow sensor. Last, it provides an estimation of the inspiratory and expiratory flows and the respiratory cycle air volumes.
The telemedicine software was designed to be intuitive, fast, graphic, and user-friendly. It requires that all users have individual accounts to control access to the records and safeguard patient confidentiality. The consulting physician (equipped with same telemedicine software on a desktop personal computer [PC]) can either create new entries or search through the networked database for existing patient records. Patients' data are entered and/or updated as to name, age, sex, address, social security number, history of previous illness, family history, drugs or allergies, current clinical status, and so on. From the other end, the consulting physician downloads the record at agreed times and performs an evaluation in a store-and-forward mode; this sometimes may require more than one prior connection by the practitioner. When they are done; they establish a network connection (wireless connectivity) and upload the file to the central database, notifying the practitioner that the diagnosis/assessment is complete on a real-time mobile session. Figures 1 and 2 include illustrative screenshots of the program mode of telemedicine software that we have used.
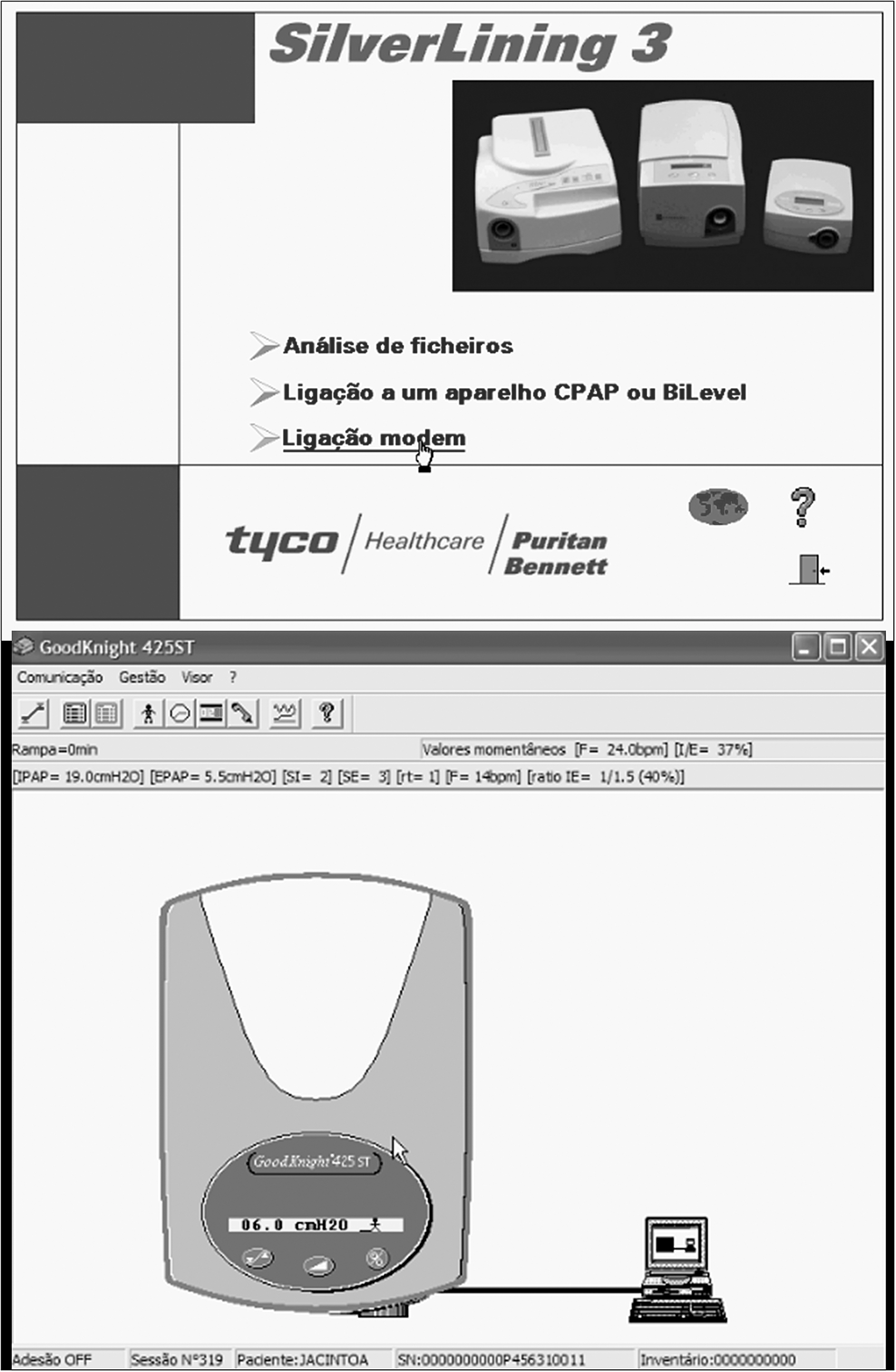
Screenshots of our software package to log patient/ventilator interaction and change parameter settings online or remotely.
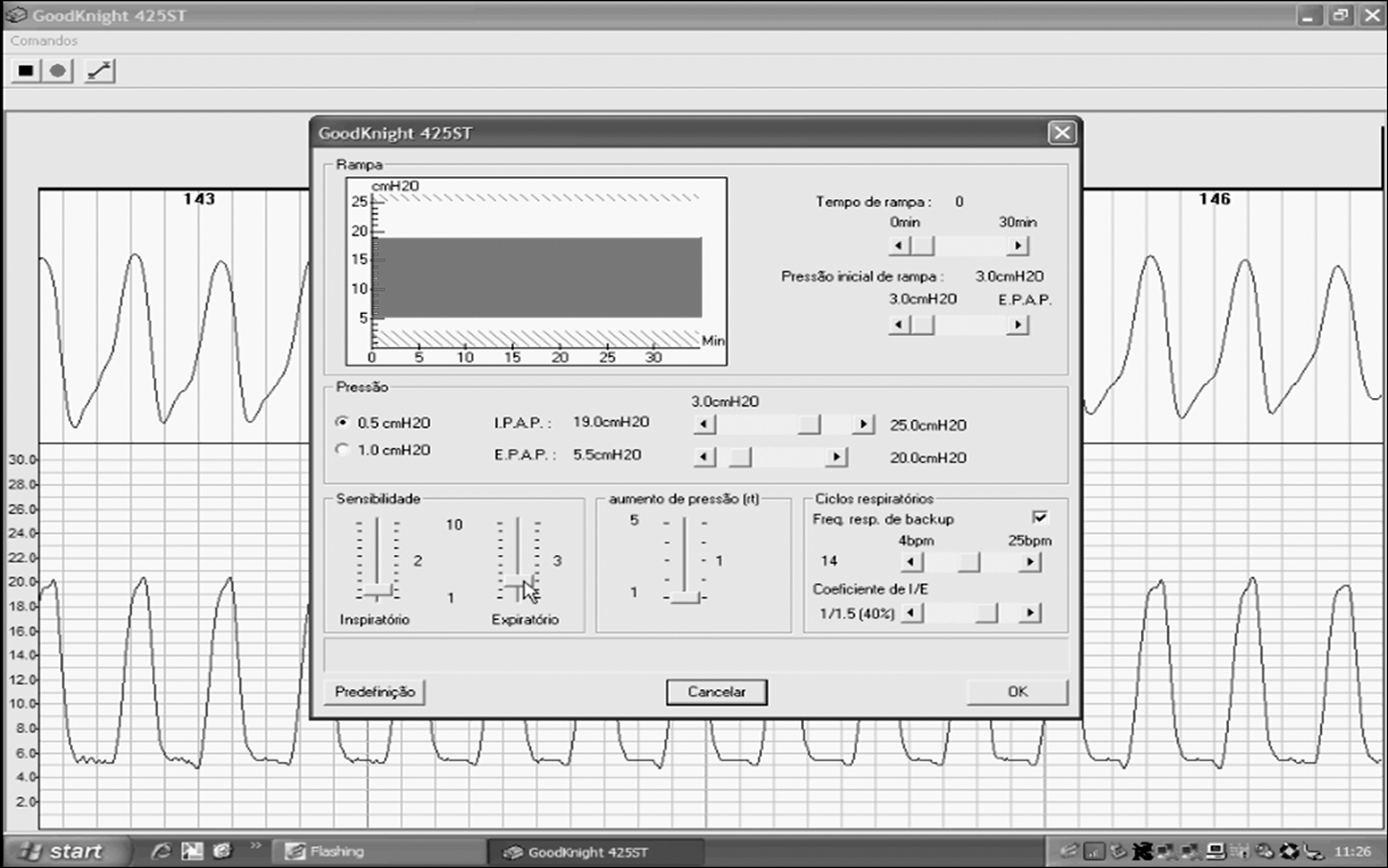
Portion of the Web page in the instrument Web application displaying the amplitude of the ventilatory profile and measurement of the corresponding inspiratory and expiratory air pressures in a specific amyotrophic lateral sclerosis patient who was ventilated at the moment. These parameters can be directly changed according to the patient needs and respiratory comfort.
Results
Assessment of Performance And Reliability
The telemedicine instrument and software were extensively tested in different configurations. We established several test procedures with the ventilation board, where the instrument measured and recorded various parameters from the commercial ventilator connected. A cardiopulmonology technician was present from the beginning of all sessions and checked the entire procedure on the display, to track unexpected respiratory rates or volumes. At the end of each session, the instrument was connected to a desktop PC in the consulting doctor's office, and data were downloaded and displayed, and then compared to the standard mode of assessment (based on similar acceptance criteria). Only errors below 5% were accepted.
A crucial element of this telemedicine instrument functionality is the remote transmission of data. The integrated protocol of wireless connectivity permits a direct connection to a server over the Internet, and the data stored can be easily accessible through a Web application. The consulting physician can access transmitted data either automatically, that is, recorded at prescribed intervals with no attention required from the patient, or manually, by starting a new session in a desktop PC with telemedicine software. The communication sessions run correctly, proving to be robust enough for data transmission and parameter settings modifications.
The instrument is compliant with the Council Directive 93/42/EEC as of June 14, 1993, concerning medical devices. It was allocated in Class IIa since it serves for diagnostic and follow-up purposes through noninvasive measurements and/or parameters changes of physiological parameters, for short time intervals.
Preliminary Trials On Als Patients
We ran an exploratory phase to test safety, acceptance, and accuracy. Some preliminary tests have been performed on volunteer patients with amyotrophic lateral sclerosis followed-up in our outpatient clinics, after giving informed consent. All patients were informed about the rationale of the test, and very positive comments on the easiness of settings arrangements were expressed throughout the study phase. The system was suitable, worked well, and served our investigational purposes. Main limitations were related to the need of a fixed telephone line and the speed of data extraction.
For the follow-up of compliance to NIV and parameters settings, all participants received a helpline to clarify any doubts or to look for medical advice whenever necessary. Anticipating difficulties and constraints imposed by continuously monitoring and data storing, patients were further instructed to activate the system once a week or whenever they felt uncomfortable with the device. They should proceed to call the physician in charge and to be in touch with the helpline in case of any technological issue or a worsening clinical condition.
In addition to this first exploratory trial, an intermediate level of care was set up to detect and flag alarm signs requiring an immediate revision of ventilation parameters settings. This monitoring was performed by the cardiopulmonology technician who, after reviewing the synthesis report or night calendar, would send a message to the physician who then decided the next step: tuning specific parameters settings, scheduling an office visit, a phone call, or a real-time interaction. Since there are no published or established alert signs for home ventilation, in rapidly progressive neuromuscular disorders, we established alert signs based on our clinical experience. All data that were ± 1 standard deviation of the mean values of the following ventilatory parameters were arbitrarily chosen by us as the most convenient flags: inspiratory positive air pressure (IPAP), expiratory positive air pressure (EPAP), inspiratory/expiratory ratio, imposed breath frequency (back-up rate [BR]), inspiratory sensitivity (IS), expiratory sensitivity, and rise time. Also, we considered as alert signs all data conflicting with the preceding ventilation profile of the patient, previously measured by the office-based standard mode of care.
An example of data display is shown in Figure 3.
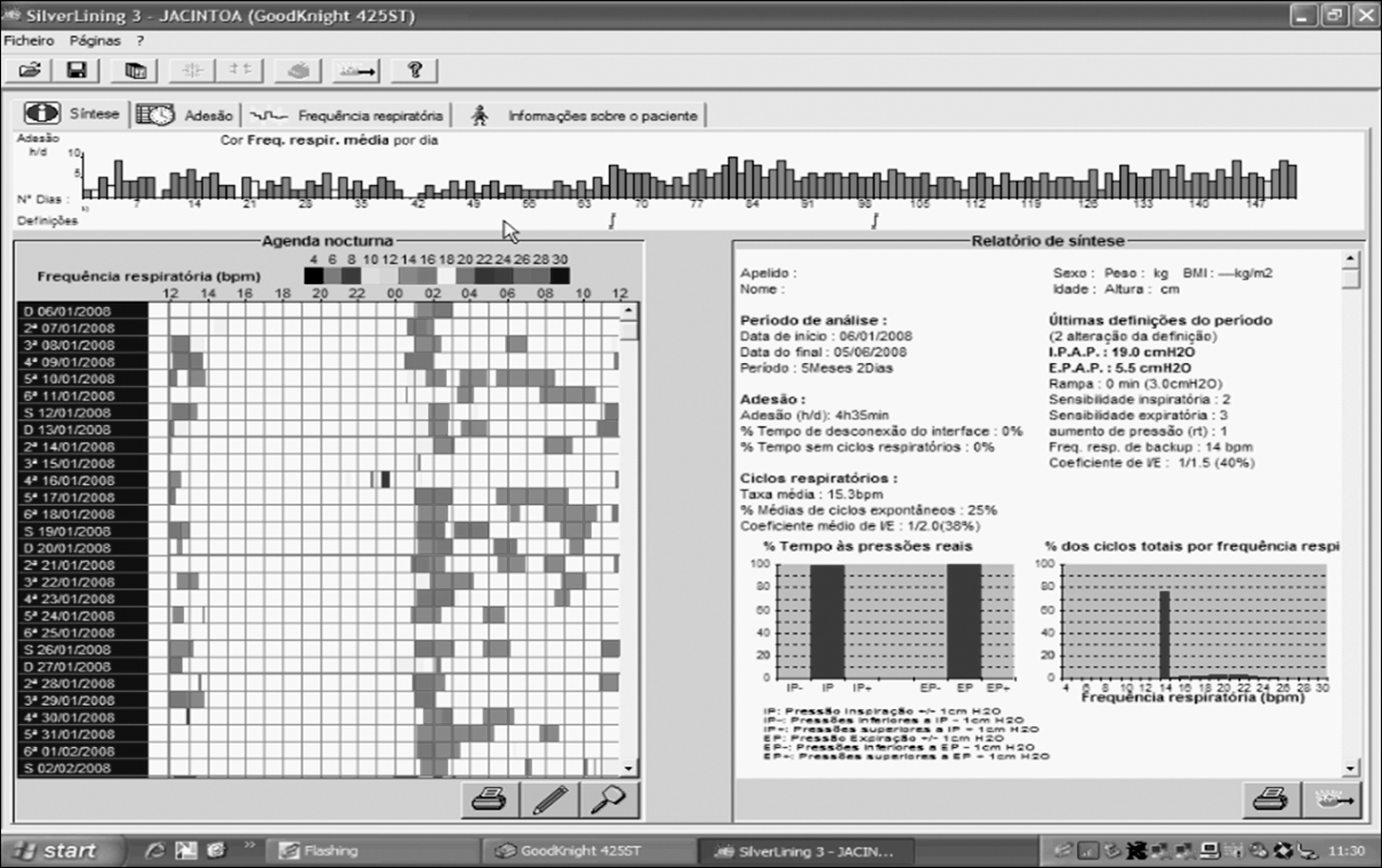
Screenshot of the remote site database, displaying data from the number of hours of ventilator usage per day, along the illustrated months, as well as average data values of the ventilation parameters (pressures and others) and compliance to noninvasive ventilation (>6 h/day) throughout that period. This is very useful given that one can access and analyze these data by choosing a specific period of the year and then proceed to comparisons among months or even longer.
Discussion
We implemented a medical instrument for home telemonitoring of ventilated patients from our ALS clinics. With the advent of powerful electronics, medical instruments in general and noninvasive respiratory devices in particular are now more available for patients in their home environment. In truth, the feasibility of telemedicine for home monitoring of patients with chronic respiratory failure has been documented to be a beneficial solution in the past. 12,22 –24 Literature further reports a trial of chronic obstructive pulmonary disease (COPD) patients in which telemedicine has been implemented and proved to be feasible and useful for titration of oxygen, mechanical ventilation setting, and stabilization of relapses. 25 Yet, to the best of our knowledge, the present feasibility study is the first implementation trial of NIV compliance evaluation with the new technical solution that enabled us to remotely monitor at distance the registered data in the telemedical software in ALS patients.
To evaluate efficacy and efficiency of this system, we are now running a controlled trial throughout which we intend to evaluate differences in compliance to NIV and healthcare utilization during the entire span of NIV use, as well as the number of parameter setting changes during the period needed to achieve full compliance. Also, from the ventilatory standpoint we are following up the type of parameter setting changes by the number of hours of usage a day; the percentage of spontaneous breathing; back-up respiratory rate; average, minimum, and maximal respiratory rates; and the percentage of attained predetermined pressures. Developments for improved physician's feedback on possible asynchronies and correct ventilatory adjustments are ongoing.
Despite there being a large number of studies of a variety of telemedical instruments, it remains difficult to ascertain the exact role and benefit they play as far as the health care system is concerned. On the one hand, although beneficial for the patient a major pitfall of today's telemedicine is the powerlessness to express the sense of touch. In ventilated patients, it is sometimes important to touch the patient to feel his respiratory pattern and track abnormal issues. Figure 4 illustrates one case of several ventilator parameters setting in an ALS patient. On the other hand, neuromuscular disorders are a major healthcare challenge from a respiratory outlook, thereby rendering the current, physician-centered models of management unsustainable in the critically ill and noncompliant patient, as happens in the clinical setting of our center.
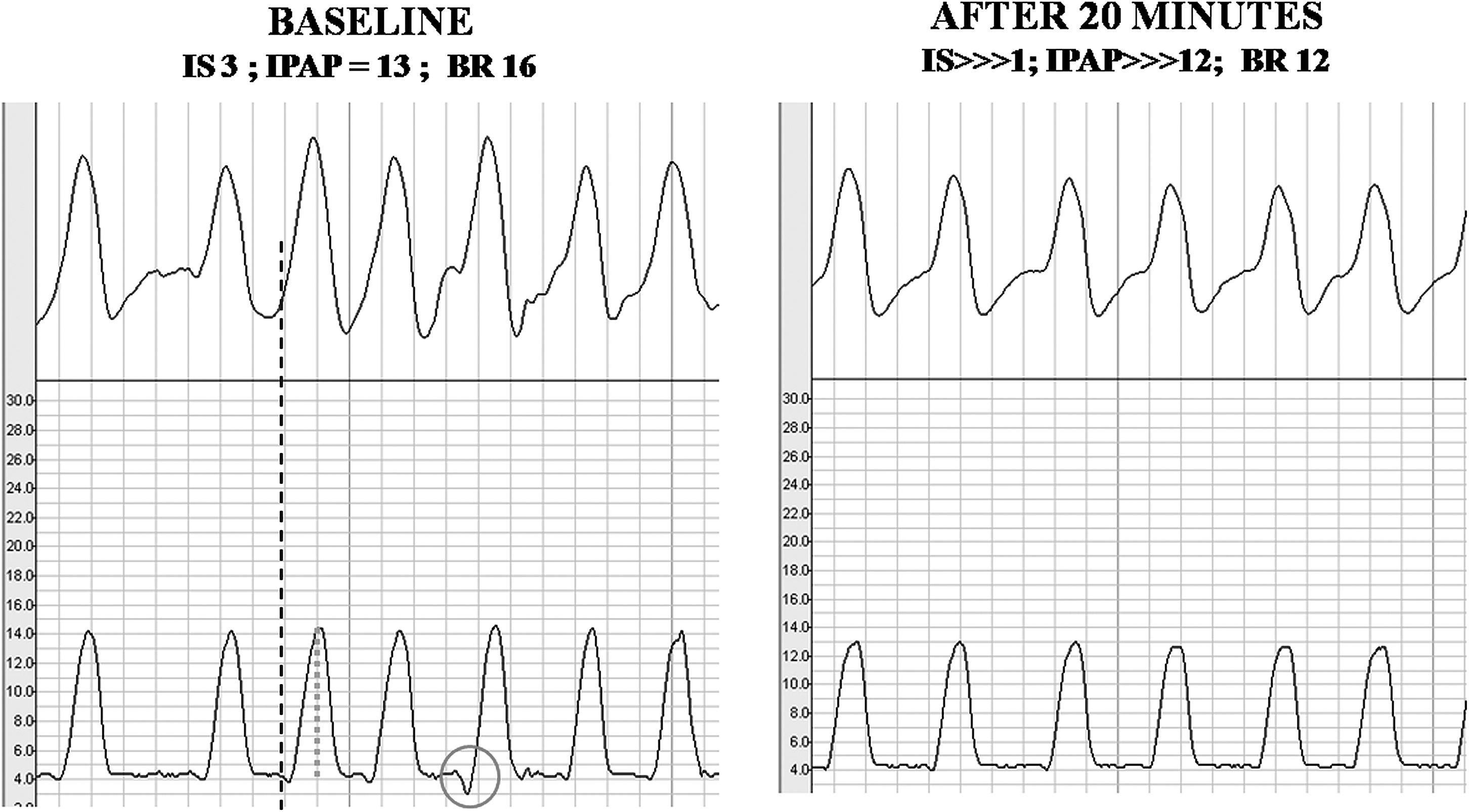
Screenshot of two pieces of the same recording of a patient during his initial trial of noninvasive ventilation where the pressure–flow curves at left show a delay of the inspiration time (long dashed line), an amplitude increase of the flow curve (short dotted line), and a negative deflection with a negative spike at initial inspiration, contributing to a general appearance of an asynchronous breathing. On the right side, after a reduction of the IPAP (12 cm H2O), and an increase of the inspiratory trigger sensitivity (IS > > > 1), it is clear that patient became comfortable with a normal respiratory frequency.
We therefore believe our telemonitoring instrument helps ease communication between the patient and the multidisciplinary team. It basically relies on a simple circuit of remote data transmission, first collected from the external ventilator, then downloaded to a desktop PC wirelessly, and next sent to a remote central database. The particularity of the included TCP/IP protocol and the availability of manual and automatic modes of data capture make it a singular instrument.
In the upcoming digital age, we may truly state that this kind of data transmission is still very poorly used in clinical scenarios. Yet, our feasibility study in struggling ALS disease shows that home telemonitoring is finding its way into the mainstream follow-up modes. To realize its full potential, we need to recognize further innovative applications of telemedicine and engender strong data on its cost effectiveness. Unresolved issues in telemedicine still include licensure, reimbursement issues, the development of standards, patient confidentiality, telecommunications infrastructure, and robust analysis on cost effectiveness. Health professionals first need to focus on enhancement of specific skills and then proceed to controlled trials on patients. Until we have universally applicable monitoring models, with proved user satisfaction and cost effectiveness, we need to look forward with aware optimism.
Footnotes
Acknowledgments
This work was supported by “Fundação para a Ciência e Tecnologia”—PIC/IC/82765/2007. The authors are grateful to Linde Sogas Co. for providing this research with the technical support.
Disclosure Statement
No competing financial interests exist.