
Abstract
Introduction
Incidence and prevalence of heart failure have increased steadily in recent decades in Germany as well as in other Western industrialized countries and are continuing to rise. 1 Studies suggest that currently about 1.8 million people in Germany suffer from chronic heart failure, and 200,000–300,000 new patients are added each year. 2 Despite the implementation of new therapy strategies with an impact on the patients' prognosis—such as the use of beta-blockers, angiotensin converting enzyme inhibitors, angiotensin II AT1 receptor blockers, and aldosterone receptor antagonists—life expectancy of heart failure patients continues to be significantly reduced. For patients with higher stages of heart failure, the 1-year lethality is up to 50%, similar to that of patients with a malignancy. 3 Heart failure is associated with a progressive decrease in quality of life and physical performance. Frequent hospitalizations, long periods of sick leave, and a high rate of illness-associated disability have significant health and macroeconomic consequences. The costs of treatment for chronic heart failure patients in Germany have been estimated to amount to 2.7 billion Euro per year. 4 The bulk of these costs (70%) cannot be attributed to drug therapy or expensive interventions such as pacemakers/defibrillators and heart transplants, but to costs associated with the frequent and lengthy hospitalizations of patient with chronic heart failure. Hospital reports show that the average length of stay for patients with heart failure continues to be longer than 14 days. 4 Projections predict a rise of 30% of hospitalizations due to heart failure, particularly in the patient group of 65 years and older. 5
The positive influence of adherence to medical guidelines for the drug treatment of patients with systolic heart failure is undisputed. It reduces hospitalizations and can quantitatively improve the prognosis of patients with heart failure significantly. 6 –9 However, it has been shown that with three different drugs per day, patient compliance is only about 70%. 10 Several studies have demonstrated that a majority of cardiac decompensations and rehospitalizations due to heart failure can be contributed to a lack of knowledge about the disease as well as a lack of medical compliance. 11 –15 In addition, a shorter length of stay in acute care clinics/hospitals makes it more difficult to complete the implementation of drug therapy regimens conforming to medical guidelines. In addition, there is little time for individual education and training of the patients. Considering these facts, it is not surprising that no more than one-fourth of the heart failure patients follow the recommendation of daily weighing. 11 Although various meta-analysis demonstrated the significant clinical (number needed to treat=34) and health economic benefit of multidisciplinary heart failure programs, only a minority of patients receive this kind of care. 14
For these reasons, the German Foundation for the Chronically Ill in cooperation with the Techniker Krankenkasse (TK) established the care and education program “Telemedicine for the Heart” for patients with chronic heart failure (for a detailed overview of the "Telemedicine for Heart" program, see
Subjects and Methods
Study Design
Program participants for “Telemedicine for the Heart” in Germany were recruited from patients insured by the TK. To evaluate the program, a retrospective matched-pairs analysis was performed. Program participants (n=281) with demographics and morbidity status (e.g., age, sex, and New York Heart Association [NYHA] status [the established classification for heart failure defined by the NYHA]) (Table 1) comparable to those of regularly insured patients (n=843) were evaluated and compared according to their use of resources.
Characteristics of Study and Control Groups
New York Heart Association (NYHA) II represents mild symptoms and slight limitation; NYHA III/IV represents marked to severe symptoms and limitation.
SD, standard deviation.
Inclusion and Exclusion Criteria
Inclusion criteria for participation in the telemedical care program were symptomatic heart failure (≥NYHA classification II [persons with mild symptoms and slight limitation]) and an inpatient hospital stay due to heart failure up to 6 months prior to the start of the telemedical care program. Eleven patients were excluded from matching because they dropped out of the program before or during the first training unit owing to cancellation of program participance or death within the first month after the program started. This exclusion was performed as at least one single nurse-call was considered necessary for assuming any impact of the program on the patients' health and behavior. For each member of the study group three patients with a similar health status were included in the control group. Comparability was ensured by matching the following parameters: age, sex, NYHA status, and number and kind of prior hospital admissions. Participants in the control group were selected randomly and retrospectively with these criteria from the health insurance database (>6 million insured) of the participants of the program.
Extent of the Telemedicine Intervention
Throughout the program patients received a decreasing intensity of nurse-supervised telephone calls. In the training phase nurse-calls were conducted at 14-day intervals. During these calls patients were motivated to perform regular self-measurements with either devices provided by the program or devices existent in the patient's household. All measurements (blood pressure, pulse, weight) were recorded by the patients in their heart failure diaries. The diaries were then used as the basis of discussion with the telemedicine center as well as the treating physician. As part of the nurse-calls, the results were transferred into the electronic patient record. In addition, medical compliance was monitored, and education about signs of decompensating heart failure was provided. During the first phase of the program, patients classified as NYHA III and IV were supplied with and instructed on the use of a telemetric scale and blood pressure cuff. Measured values were automatically transmitted to the telemedicine center. In the case of measurements outside of set limits, calls could be placed to the patients to increase their awareness and to treating physicians in order to induce therapy adjustment where applicable.
The telemedicine-enabled devices set (Fig. 1) contained a scale (TC100® portable; IEM, Stolberg, Germany), an upper arm blood pressure monitoring cuff (Stabil-O-Graph® mobil; IEM, Stolberg, Germany), and a modern, commercially available mobile phone.

Preset, telemedicine-enabled device set with scales, blood pressure measuring device, and mobile phone that patients in the program “Telemedicine for the Heart” receive.
Data Analysis and Statistics
For all patients in the intervention and control group, the data from the health insurance database of the TK were anonymized prior to collection. The period considered for the study started 6 weeks after inclusion in the program and ended March 31, 2008. The total costs included were projected, normalized, and analyzed over 1 year. The primary outcome measures were monetary aspects (sectoral costs [e.g., cost for medication, for hospitalizations, or for therapeutic aids] and costs of total treatment), number of hospitalizations, and mortality rates.
The health-related quality of life was monitored at the program start and in a follow-up survey at the end of the observation period of the study in Spring 2008 by means of a self-administered questionnaire on quality of life (SF-36). In addition, an individual semi-poll on patient satisfaction was carried out with the program participants. For this purpose, 331 participants (most of them included in the health economic evaluation) were asked by the TK in Autumn 2007 to rate their experiences with the program.
Basic figures were processed using descriptive statistics and then presented. During the cost analysis, the direct medical costs, from the perspective of the statutory health insurance, for each participant were analyzed individually. Approximated costs for the program itself were considered in a supplemental sensitivity analysis. The t test and chi-squared test were used for the comparison of costs, hospitalizations, and mortality rates between the two groups. Because of the skewness of cost data additional resampling bootstrap techniques were used to check the robustness of the t test. 16 The mortality trends within the two groups were examined using Kaplan–Meier plots. For statistical analysis SPSS version 15 software was used.
Results
Composition of Program and Control Groups
Table 1 shows the matching between patients in the intervention and control groups. The differences in the observation periods between the groups (as a whole and regarding the NYHA status) result from the higher mortality in the control group and should not bias the following results. Also, the ratio of occupational disability insurance differed between the groups. A sensitivity analysis indicated that, because of the small group size of occupationally disabled, only marginal differences around 0.2% in relation to the total costs of the two main comparative groups could occur.
Mortality and Survival
During a mean observation period of 582±134 days participants of the “Telemedicine for the Heart” group exhibited significantly higher survival than participants of the control group. In the study group 24 of 281 participants died, whereas in the control group 111 deaths occurred in 843 patients (8.5% versus 13.2%, p<0.05, chi-squared test). In a sensitivity analysis concerning the occupational disability the difference between the groups is still significant at the 0.05 level.
The cumulative survival rate over time was shown by the Kaplan–Meier curve (p<0.05) in Figure 2. It illustrates the higher death rate in the heart disease comparison group during the observation period. The number needed to treat was 22 patients during the observation period (i.e., 22 patients would need to participate in the program to prevent one death).
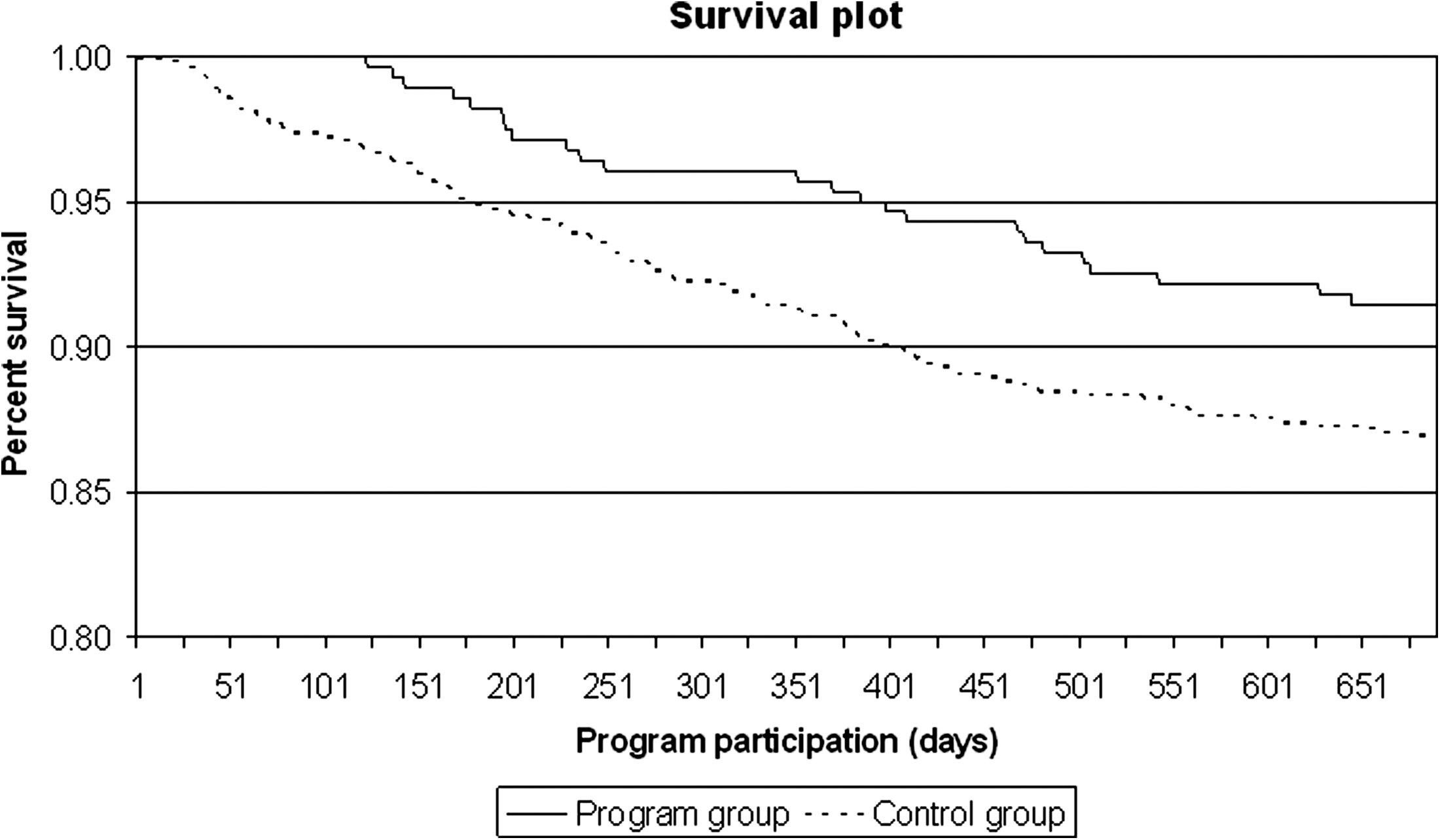
Cumulative survival probabilities as a Kaplan–Meier curve.
Direct Costs
For the cost analysis, all available performance data over the period of the program for each insured person were used. Because of the different length of time each participant spent in the program, a direct comparison of the absolute costs would have led to distortions. This was prevented by normalization of the data to annual costs. Per-patient average daily cost rates were calculated and extrapolated to 1 year. This ensured the comparability of results. Results of the maximum period of this analysis are shown in Table 2.
Direct Medical Costs According to Survival
Costs (mean and SD) are in €.
Only cost differences in total and therapeutic aids were significant between groups: p<0.05, t test.
Analysis of the total costs over the maximum benefit period, regardless of survival status, shows that program participants contributed about €2,633 less costs than the average patient in the control group. That correspnds to a 25.0% cost reduction (p<0.05, t test). In particular, the reduction of costs for therapeutic aids and resources by 60.4% and a 19.6% reduction of acute inpatient hospital treatment of program participants contributed to this difference. The living program participants contributed 9.9% lower costs than their matches in the control group (a cost difference of approximately €669 per participant). The main contributing factor was the reduction of spending on therapeutic aids and resources by 65.3% in the program participant group. Similarly, differences of total costs over the maximum service period were found for patients who died during this period. Thus, patients in the program caused €8,100 (22.8%) lower costs until their time of death than those in the control group. These differences in costs were mainly contributed to a reduction in costs of drugs (30.9%), therapeutic aids (31.9%), and acute inpatient hospital treatment (18.3%). A sensitivity analysis on total costs of the whole program group including average program costs per participant shows almost a halving of the cost reduction of the program group against the control group.
Direct Costs by Severity
The cost comparison of the two groups revealed a considerable cost advantage for study participants, particularly in the group of patients in NYHA stage II (total costs, €5,037 versus €9,604; p<0.05, t test). Regardless of the survival status, significant differences (p<0.05, t test) in utilization of the most cost-intensive sectors—pharmaceutical sector (€1,473 versus €2,279), therapeutic aids (€423 versus €1,345), and hospital treatment (€2,836 versus €5,671)—were noted for the two groups.
In the more severe NYHA stages III/IV the cost intensity changed and showed a slight cost disadvantage of the program group (€12,211 versus €11,927; difference not significant). Here the costs arose primarily for hospital treatment (€8,596 versus €7,447; difference not significant) and were partially compensated for by higher costs for therapeutic aids (€961 versus €2,001; p<0.05, t test) in the control group. The differences in costs between the program and control group of patients with the higher stages of heart failure almost leveled off over the long observation period. The costs for hospital treatment of the program group were nearly compensated for by the costs for therapeutic aids in the control group.
Hospitalizations
Regardless of the survival status, there were fewer hospital admissions in the program group (1.02 vs. 1.30 per patient per year in the program and control groups, respectively). This is a decrease by 21.5% (p=0.03, t test). The average length of stay in hospital did not differ (8.10 versus 7.72 days).
Medication
The prescriptions of medications differed primarily in the average value of each prescription. The average value of each prescription in the study group was approximately 10% lower than that of the control group (€50.62 versus €57.40). The difference between the average number of prescriptions per patient per year was marginal (33.3 vs. 34.7). Noteworthy are the differences in supply of heart-specific drugs. The percentage supply of these drugs was considerably higher in the program group than in the control group: Loop diuretics (66% versus 47%), potassium-sparing diuretics (39% versus 21%), thiazide diuretics (14% versus 12%), angiotensin converting enzyme inhibitors (61% versus 52%), beta-blockers (85% versus 75%), and cardiac glycosides (28% versus 21%).
Quality of Life
The results of the SF-36 quality of life scales for physical and mental health are shown in Figures 3 and 4, respectively. The average values of the individual scales were, as expected, well below the standard values for the entire sample of the German population. 17 Compared with a population norm sample of German patients afflicted with heart disease, the physical sum scale showed an equal level, whereas the mental sum scale showed better quality of life of the program participants.
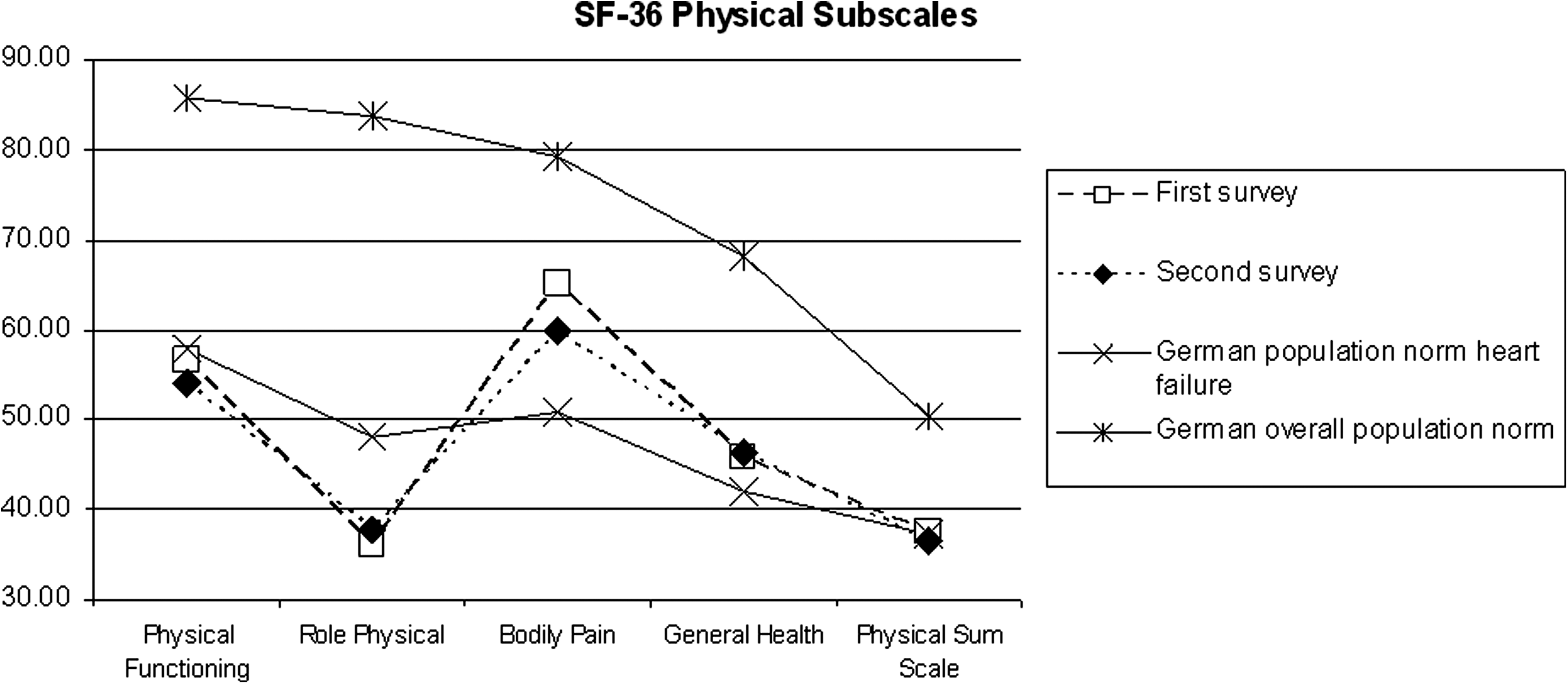
Physical health subscales in the first and second surveys compared with population norm values.
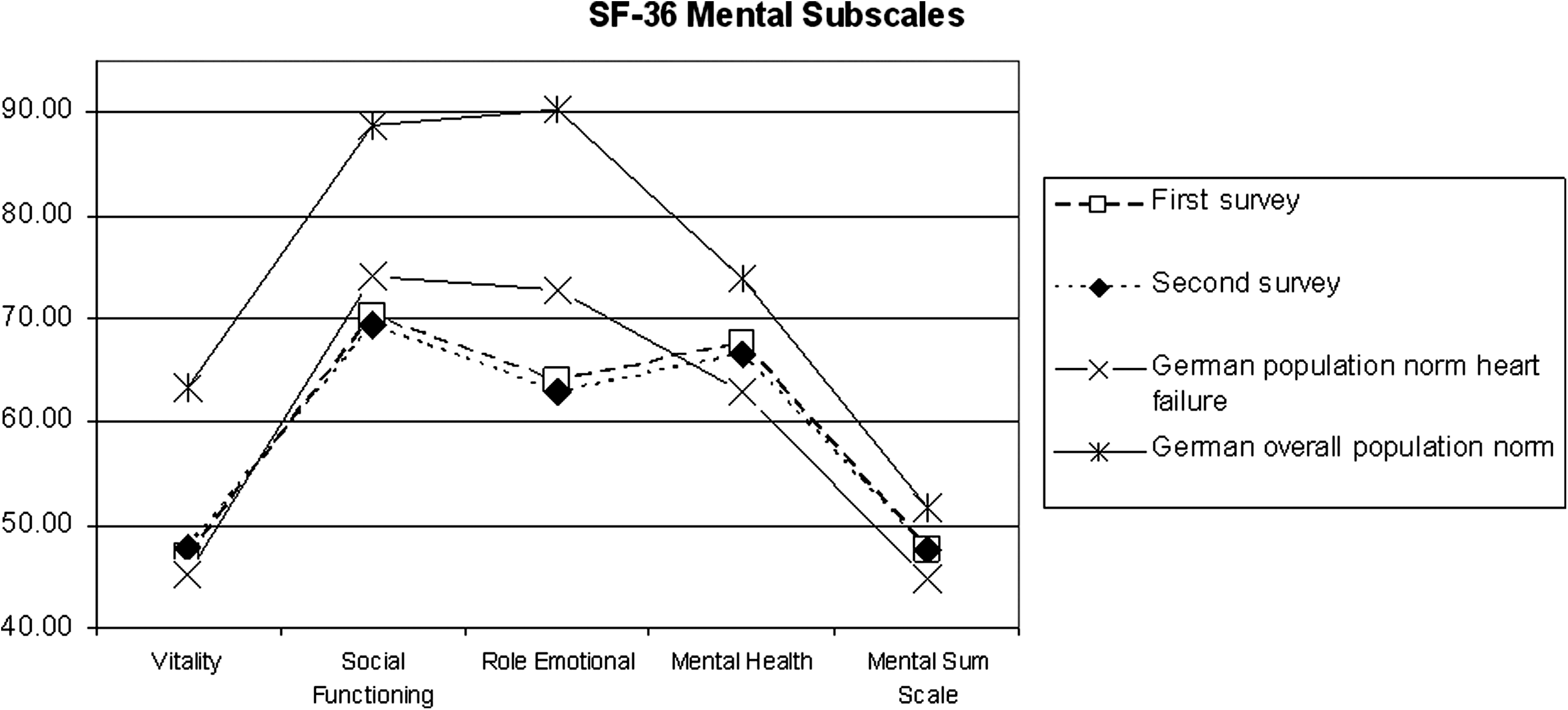
Mental health subscales in the first and second surveys compared with population norm values.
A comparison of the first and second surveys showed very small reductions in nearly all physical and mental subscales, except Vitality and Role Physical. Compensation effects of the individual subscales led in the the end to a nearly constant level of quality of life in the two sum scales over the course of the study.
Patient Satisfaction
Of the 331 selected patients, 238 provided an answer (response rate, 72%). The benefits of the program and the importance of clarity and appropriateness of the information conveyed were consistently rated as very high (>90% consent). More heterogeneous were the answers concerning the usefulness for preparation of visits to the physician and use of the information provided by the program during conversations with the treating physician (between 70% and 85% consent).
Discussion
The objective of this study was a health economic cost–cost analysis performing a ressource use comparison of the telemedicine program group and a matched control group.
Significant cost differences in favor of the study group of up to 25% in relation to the total cost could be detected. This corresponds to an amount of about €1,500–2,500 total costs per patient per year. Similar cost savings were found in the literature for comparable programs. 18,19 The main differences occured in the sectors of therapeutic aids and hospital treatment costs. In particular, significant cost reductions were found in the group of NYHA II patients, suggesting that the program's impact was largest in the early stage of the disease. Further detailed evaluations demonstrate a higher prescription rate of heart-specific ATC codes in the program group. Compared with the literature, the prescription rates were slightly lower in case of angiotensin converting enzyme inhibitors but higher for beta-blockers. 8,20
The patients' quality of life measures examined were almost constant over the observation time. This may be considered as a success for this highly morbid group of patients over such a long observation period, as the quality of life of cardiac patients usually shows a tendency to decrease over time. 21 In addition, over 90% of the participants rated the benefits of the program as very high in the patient satisfaction survey.
We observed a lower mortality of patients in the study group than in the control group. Within the first observation year, the difference amounted to 52%, and over the entire observation period to 35%. These differences were statistically significant and correspond to the results in the TEN-HMS study 22 and other telemonitoring studies 23 but certainly need confirmation in larger, randomized intervention studies.
A look at the results in their entirety indicates differentiated benefits for the participating patients that were not altogether limited to chronic heart failure. The high rates of patient satisfaction show a striking degree of positive involvement in the program of these patients with an above average total burden of morbidity. A possible explanation of the considerable reductions in costs and mortality is that the support and care received during the program lead also to large reductions in the total costs and mortality for other diseases. The increased awareness and focus of patients on their health, combined with the positive effects of emotional support received, during the program could lead to positive effects in other areas as well, but this subject will need additional research in the future.
Further studies should also assess more clearly which program components constitute the largest effect. In particular, the question of which measure contributes to what part of the mortality and cost reductions (i.e., more adequate pharmacotherapy, telephone support, and self-management of the disease) needs to be adressed.
Limitations
The present study is based on a relatively small cohort of patients and is not a prospective randomized trial. The methodological approach of one-to-three matching was chosen in order to obtain the most comparable and widest possible database, which is usually not possible in simple one-to-one matchings because of dropouts. On the other hand, multiple matches lead to a wider distribution of characteristics that may not produce the exact image of the matching-master but provide for a better representation of the reality of care. Matching according to morbidity similarities had to be restricted to treatment-relevant diagnosis distribution, NYHA stage, age, and gender because other potentially important variables such as accompanying inpatient or outpatient diagnoses, smoking status, body mass index, clinical laboratory parameters, or socioeconomic parameters were not available. The patient population studied was characterized by a high degree of multimorbidity. Under these conditions, disease-related cost allocations are complex because of a high variety of secondary diagnoses that are partially induced by upcoding or gaming activities for billing optimization purposes. To better reflect this complexity, a follow-up project to improve the inclusion and evaluation of comorbidities is planned. Other limitations of the study arise from the fact that the data were obtained on a maximal observation period of 2 years or less. Long-term effects of telemedicine in cardiac patients may thus not be noted.
Despite these limitations, the current findings suggest that the “Telemedicine for the Heart” program leads to a reduction in the number of hospital stays in patients with chronic heart failure, improved medical therapy, reduced mortality, and better quality of life. They encourage the initiation of a randomized prospective trial.
Footnotes
Acknowledgments
The German Foundation for the Chronically Ill and the Chair of Health Care Management of the University Erlangen-Nuremberg want to acknowledge their gratitude for the willigness of the TK to convey this evaluation as to analyze the impact of additional telemedical care under realistic circumstances. The health economic evaluation of the program “Telemedicine for the Heart” was funded by the TK and the German Foundation for the Chronically Ill. The questionaire surveying the patients' satisfaction with the program and their usage of the given information in their everyday life was funded by the TK. The analysis was conducted at the Chair of Health Care Management, University of Erlangen-Nuremberg.
Disclosure Statement
S.S. and O.S. were funded for the conduct of the study by the German Foundation for the Chronically Ill and the TK. There are no other financial relations with the involved parties. T.M.H., J.T.P., and A.I.K. are employees of the German Foundation for the Chronically Ill. Apart from this there are no financial interests/arrangements or affiliations with any organization that could be perceived as a real or apparent conflict of interest in the context of the subject of the article. A.M. has no competing financial interests.