
Abstract
Introduction
Three prevalent trends in the healthcare industry have led to the need for new care-delivery tools. The most important of these is payment reform, which has new payment structures encouraging population management as opposed to per-visit payments. 1 The second is a growing shortage of primary care clinicians available to provide primary and preventive care and management of chronic illness. 2 Last of these is the increasing prevalence of chronic diseases among a longer-lived patient population. 3 These trends are well documented and have been cited as the momentum builders behind the concept of a “medical home,” which is rooted in the concept of care being accessible, contiguous, comprehensive, and coordinated. 4 Increasingly available broadband service provides a significant opportunity for providers to increase the value that they bring to the patient/care team interaction, through proven channels for online healthcare delivery such as (a) Web and asynchronous messaging and (b) real-time text and video consults.
These channels are especially cogent in a time of focus on patient self-management and population management. The vision of continuous and coordinated care, both preventative and curative, may be realized with a reduced cost structure by leveraging online healthcare delivery technologies. 5 However, it is important to consider clinician work flow in the design of these technologies to encourage long-term adoption. 6 With such an approach, healthcare systems that have significant primary care referral networks can leverage such channels for online healthcare delivery to facilitate value-oriented transformation while extending the reach of their tertiary-care centers.
This study examined the adoption of, usage of, and satisfaction with using an online healthcare delivery tool to conduct scripted asynchronous virtual visits for the follow-up of chronic illnesses in a primary care setting. The objective of this study was to examine the efficiency and satisfaction with an initiative to conduct virtual patient follow-up visits using asynchronous online exchange between a patient and the physician, as well as the synchronous communication via phone/video between a patient and physician. Specific aims include (1) to examine the adoption and usage of the virtual follow-up Web site and (2) to examine patient and physician satisfaction with conducting follow-up visits virtually over the Web.
Materials and Methods
Study Design
Case study design was used: once patients were consented and enrolled, they completed an asynchronous virtual visit with their doctor via a Web site questionnaire (Fig. 1). After receiving a response to the virtual visit from their physician, both patients and physicians completed an evaluation survey of their experience. Ten providers at one Massachusetts General Hospital (MGH) ambulatory internal medicine practice site MGH–Beacon Hill Practice) were recruited into the study. In total, nine physicians and one nurse practitioner participated in the study. The study was approved by the MGH Institutional Review Board, and written consents were used for patients and providers.
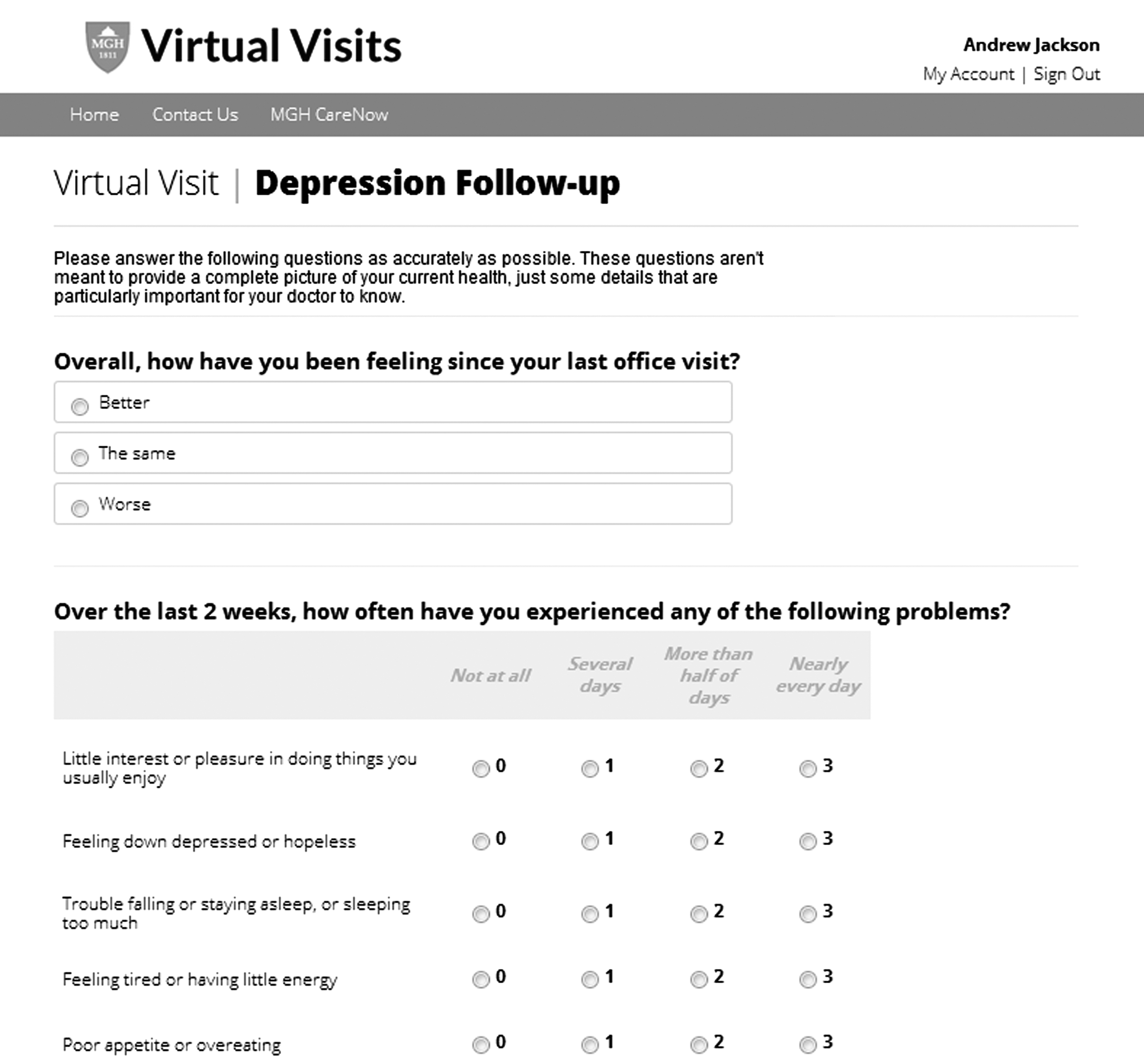
Example (partial) of the virtual visit questionnaire.
Patient Recruitment
Two hundred ninety-three adult subjects presenting with one of the 10 chronic illness diagnoses included in the study were recruited from an adult primary care practice. Subjects were recruited at the discretion of the primary care provider if they met the following inclusion criteria: the patient has established primary care at MGH–Beacon Hill Practice (i.e., the patient was previously seen at the practice), the patient has Internet access, and one of the following as the chief complaint—asthma, anxiety disorders, back pain, depression, diabetes, gastroesophageal reflux disease, headaches, hypertension, obesity, or osteoarthritis.
Exclusion criteria were that the patient (1) was acutely ill (i.e., requiring urgent/emergent therapeutic intervention within the same day as the office visit), (2) was new to the practice (i.e., not an established patient), or (3) had a chief complaint different from those in the inclusion criteria.
Enrolled patients were consented to participate in the study and given log-in instructions immediately after the patient's clinic visit.
Intervention
Enrolled patients received an e-mail initiating a virtual follow-up visit scheduled 7–28 days after the office visit, based on the physician's discretion. Patients followed a link in the e-mail to the virtual visit Web site, a Health Insurance Portability and Accountability Act–compliant Web site hosted on the MGH server, meeting MGH's Web site security policies. Once logged into the Web site, the patient was directed to complete a script of questions to collect follow-up data based on his or her initial diagnosis. These scripts were developed by the research team based on evidence-based guidelines and standard medical practices. 7,8 Content was then revised based on feedback from physician subject matter experts and mock patients prior to the start of the study. The patient's responses to the scripts were forwarded to the patient's primary care physician. This platform differs significantly from the typical patient portal in that the scripts provide the clinical content and documentation by which concrete medical decision-making is made.
Patients who did not respond to the initial virtual visit e-mail received automated reminder e-mails 1, 3, and 5 days after the date of the appointment. Patients who did not complete their virtual visit 5 days after the scheduled virtual visit date were contacted via telephone by clinic staff to schedule a traditional office appointment.
Study physicians had time set aside in their schedule to review patient responses to the virtual visit questionnaire and make recommendations for next steps. Physicians were expected to follow up on virtual visit responses within 1 business day. Following review of the patient's responses, the physician could recommend that the patient continue with current treatment, schedule a follow-up phone call or video chat, or call the clinic to set up a face-to-face appointment. Additionally, the physician could add other specific instructions in note form. The responses to the virtual visit questionnaire along with the physician's note and recommendations were cut and pasted from the virtual visit Web site to the electronic medical record.
Patients received an e-mail notifying them that their physician had reviewed their responses and made recommendations. Patients followed the link in the e-mail back to the virtual visit Web site to see their physician's recommendations. Those patients who did not open the link received automated reminder e-mails 1, 3, and 5 days after the response was posted to the virtual visit Web site. Patients who did not respond after 5 days were contacted by clinic staff to make an in-person appointment.
Once the asynchronous virtual visit was completed, both the physician and the patients followed links to an anonymous evaluation questionnaire using the Redcap survey tool. In addition to the survey questions, data on age, sex, and diagnosis were collected and tabulated for each patient. Data on Web site usage and visit time were also collected.
Results
Two hundred ninety-three patients were recruited for this study. Of the total, 175 consented and completed a virtual visit for a usage rate of 60%. The mean age of users was 50 (range, 24–90) years; of those who completed the virtual visit, 53% were male, and 27% were 55–64 years of age. The most frequent diagnosis among those who completed the virtual visit was hypertension (31%), followed by weight control (14%) (Fig. 2). No significant differences in age, gender, or diagnosis were found between those who completed the virtual visit and those who did not. The clinician sample had a mean age of 51.8 (range, 33–80) years and mean years of practice of 21.4 (range, 5–53).
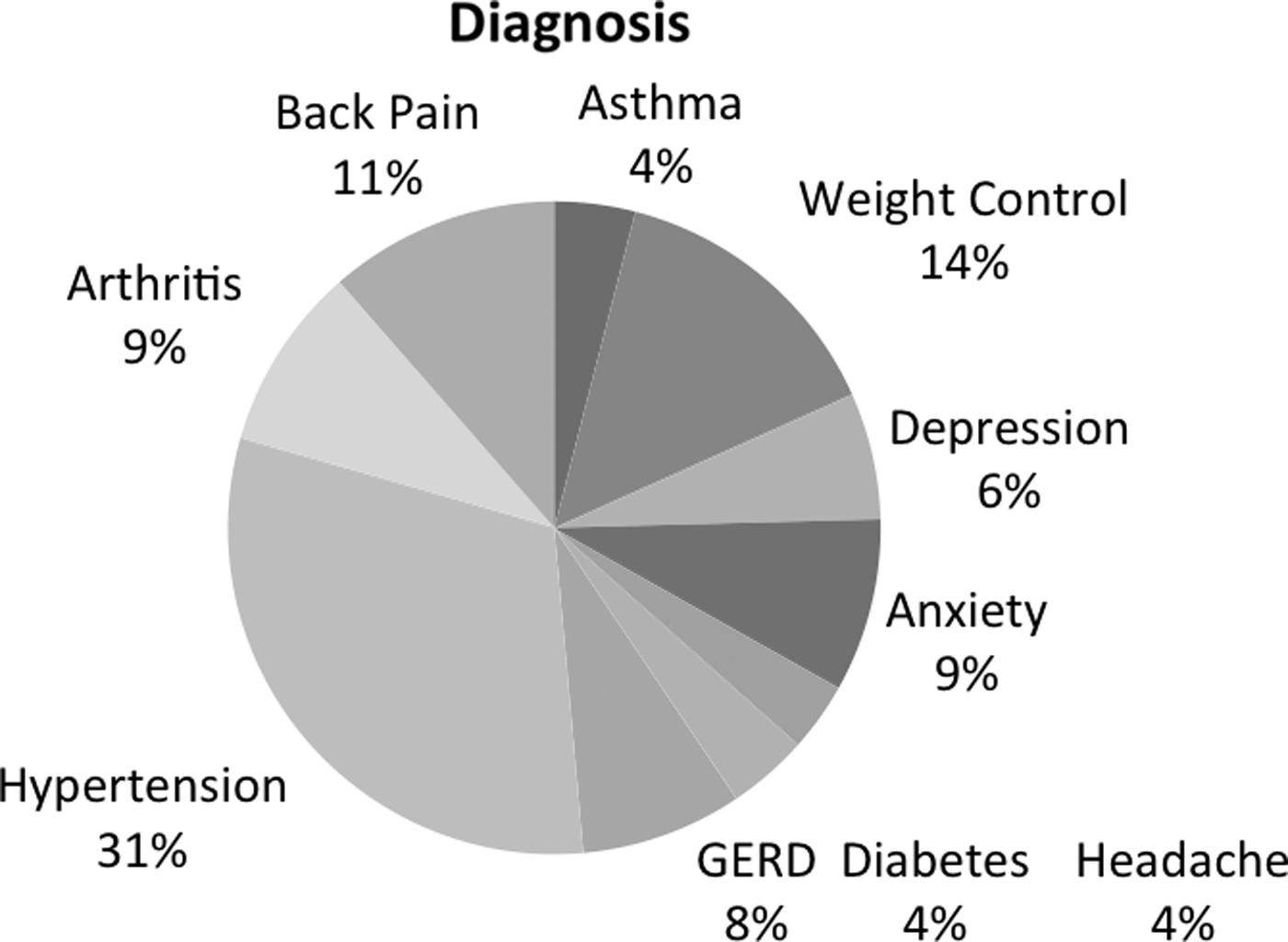
Distribution of diagnoses (n=175). GERD, gastroesophageal reflux disease.
On average, patients spent 8.31 min completing the virtual visit questionnaire. Physicians spent an average of 3.62 min reviewing a single patient's response and making recommendations. Patients found the virtual visits to be satisfactory on all measures, including convenience, time spent, clinical skill, explanation of next steps, and overall satisfaction, with means ranging from 3.59 (standard error [SE]=0.09) for overall satisfaction to 4.47 (SE=0.06) for satisfaction with clinical skills of the physician (Fig. 3).
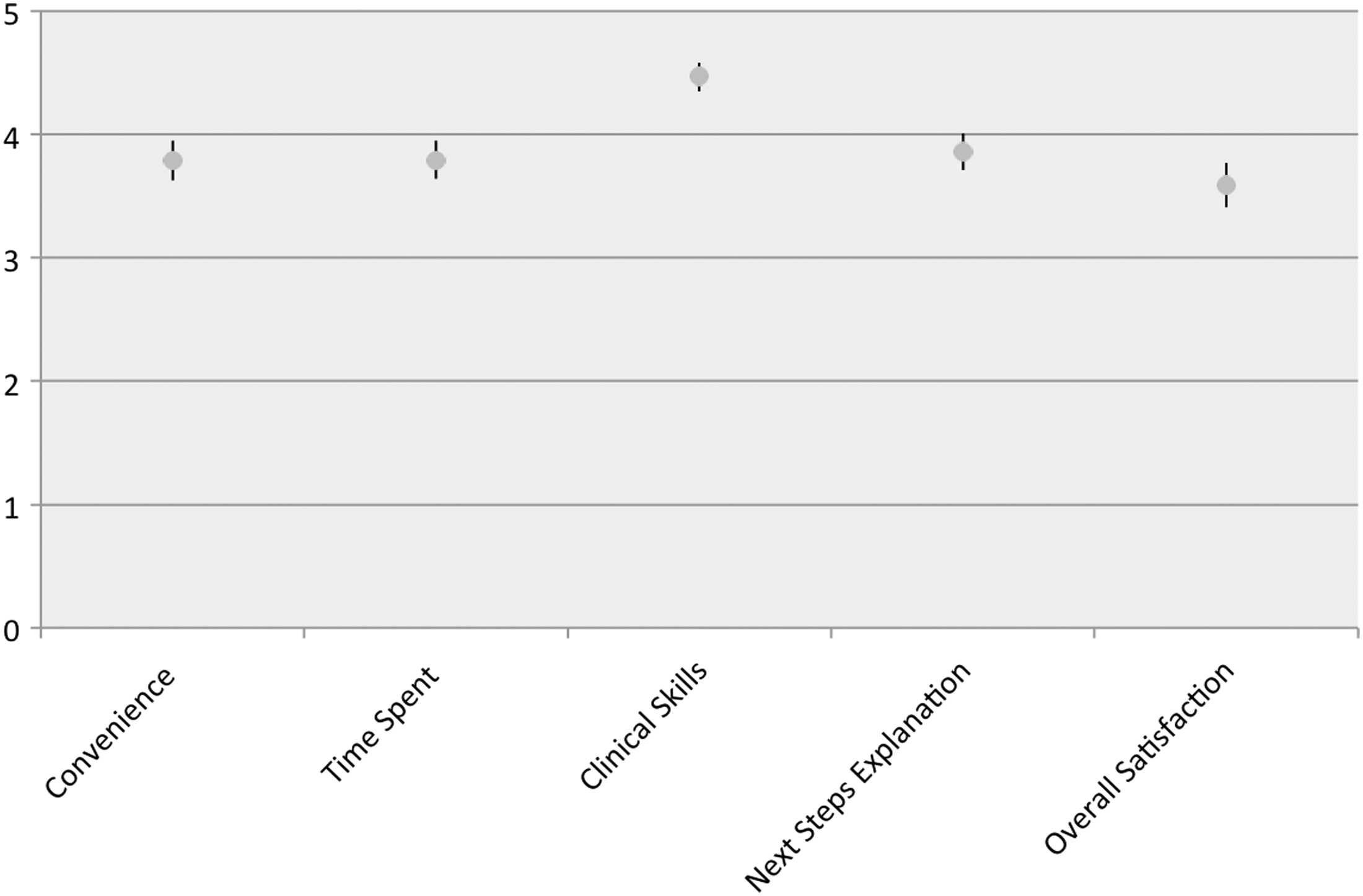
Patient satisfaction with the virtual visit experience (n=156). Responses were scored from 1=not at all satisfied to 5=extremely satisfied.
Physicians were on average extremely satisfied with the clinical decision-making capabilities of the virtual visit tool (Fig. 4). Physician satisfaction with receiving sufficient data to make a diagnosis, order tests, change medications, and make referrals ranged from 4.32 to 4.53/5 (SE=0.06–0.09). Satisfaction with the diagnostic capability was 4.60/5 (SE=0.07). Overall satisfaction was 4.47/5 (SE=0.08).
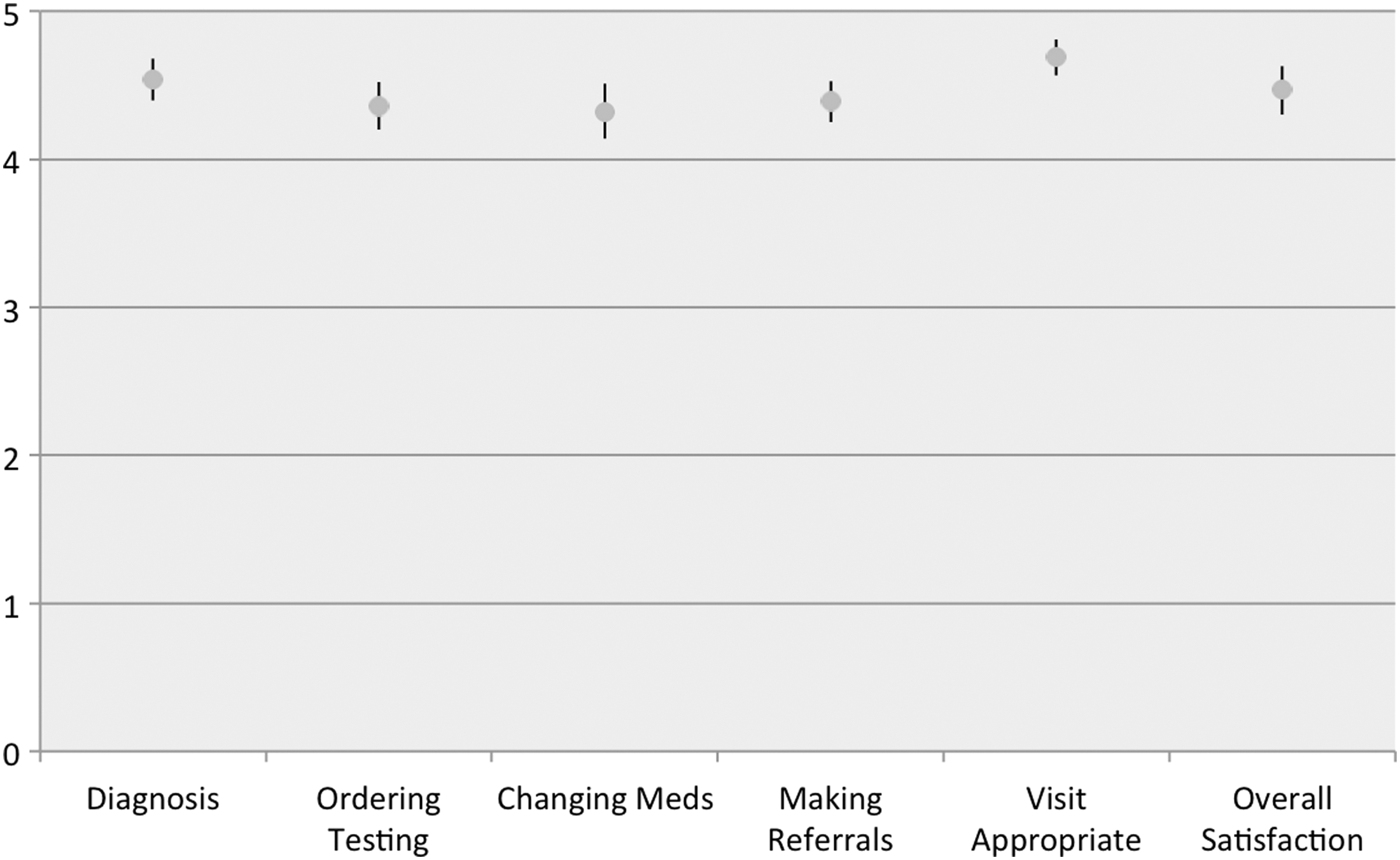
Physician satisfaction with the virtual visit experience (n=143). Responses were scored from 1=not at all satisfied to 5=extremely satisfied.
Discussion
Physicians and patients found it feasible to conduct general medical visits via structured asynchronous visits, and both parties were satisfied with these visits. The results suggest that physicians and patients are comfortable with the clinical decisions that can be made via asynchronous technology, which is consistent with findings from other technology-based interventions. 9 It is interesting that patients were most satisfied with the clinical decision making that the physicians demonstrated through their responses to the virtual visits, whereas physicians were most satisfied with the ability to make care decisions. These results together suggest that both clinicians and patients find the clinical value of the tool extremely important to overall satisfaction.
The completion rate of 60% was influenced by a technical log-in issue that prevented many of the patients recruited in the first 2 weeks of the study from completing their virtual visit. Once this was detected and corrected, the completion rate increased to 84% for the remaining 6 weeks of the study. This remains slightly higher than the typical 5–8% no-show rate of the Beacon Hill office practice, which we attributed to the novelty of the tool and process. No difference in patient characteristics between these early recruits and the later recruits was detected.
Once again, the present study suggests that once patients and physicians are given the opportunity to use an alternative system of care, the experience can be a satisfying one. Making these systems adapt to the office work flow is very important to clinician satisfaction. Traditional physical examination was not performed as a part of these visits but was performed as a portion of the office visit that preceded the virtual follow-up visit. The clinical satisfaction with the virtual follow-up visit suggests that, for the conditions evaluated, a physical examination was not required for patient or clinician satisfaction. A randomized controlled study examining virtual visit satisfaction versus in-person follow-up satisfaction would be the best way to evaluate this.
Many telehealth studies focus on the downstream savings from the use of telehealth, such as decreased hospitalizations, emergency room use, or pharmacy costs. Although we may hypothesize that these downstream savings may exist if this technology were scaled, we can focus on immediate savings for physicians and patients with this technology. From a patient's perspective, the convenience/opportunity cost savings is obvious. Transportation costs, travel costs, and work absences are all valuable incentives for patients. The clinician savings equation is more powerful when compared with the traditional office visit. Imagine that the typical clinician spends 15 min on a follow-up visit for a chronic issue such as gastroesophageal reflux disease or hypertension, plus 2 min of documentation time. With an average “virtual” visit time across all conditions of 3.6 min including documentation, this represents a potential gain of 13 min per follow-up visit. This represents a tangible realized time gain to the primary care clinician, who increasingly operates with more time demands in a shrinking wage base.
The caveat to the above point is reimbursement. One of the main drivers for having patients come in for follow-up visits is that these straightforward visits are sources of relatively easy income for physicians. In a fee-for-service environment these virtual visits do not work, unless a supplemental fee is charged for these visits. In a population-based payment model such as an accountable care organization, this type of intervention has significantly more promise, as it may allow providers to offload many of their straightforward follow-up visits to a “virtual platform.” This could allow physicians to spend more time face to face with patients with more complex social or medical problems and positively affect medical expense trends over time. 10
The tool used in the pilot project here has been placed into practice with several incentives to encourage provider adoption, in the capitated environment of Massachusetts. More scripts for chronic disease follow-up have been developed and deployed. Adoption has been brisker than the typical personal health record implementation, which can induce clinician anxiety around interminable open-ended exchanges. The minimal clinician time investment—facilitated by careful scripting of questions, discrete chronic disease conditions, automated documentation, and reasonable compensation for performing these visits—has led to broader adoption. Outcomes that impact medical expense trends such as patient visit volume, specialty visit volume, and hospital/emergency room use are being measured and tracked. We look forward to further progress updates.
Footnotes
Acknowledgments
The authors thank John Schmucker for his editorial comments, Brett Thomas for technical contributions, and Lara Fraser for site administration. Thanks also to the physicians, staff, and patients of MGH–Beacon Hill Primary Care for their participation in this study.
Disclosure Statement
No competing financial interests exist.