
Abstract
Introduction
After a limb is amputated, many patients continue to experience sensation in the absent limb. This phenomenon has been termed “phantom limb” sensation. 1,2 Studies show that 50–80% of patients experience pain in their phantom limb following amputation, and many experience pain that persists long after amputation. 3 The etiology of phantom limb pain (PLP) is unknown, but neuroplasticity, a mismatch in neuronal signals, and proprioceptive memory have been theorized as possible sources of pain, and all have some supporting evidence. 3,4 The neuroplasticity theory has the greatest preponderance of experimental evidence. This theory states that neurons that previously controlled the amputated limb become idle and form new connections with neighboring neurons, and this expanded cortical representation of the missing limb causes PLP. 3,5 The second theory is that there is a mismatch in signals that the brain receives from the residual limb, peripheral nerves, and visual feedback, and this mismatch in signaling leads to PLP. 3,4 The third theory suggests that a memory of the last position and sensation of the limb prior to amputation, termed proprioceptive memory, is recalled in the experience of PLP. 3
Mirror therapy was first reported by Ramachandran and Rogers-Ramachandran 5,6 as a successful treatment for PLP in 6 of 10 (60%) upper limb amputees. Patients were instructed to view the reflected movement of their intact limb in a mirror placed along the body midline while simultaneously moving the amputated or “phantom” limb. This gives the visual illusion that the phantom limb has been resurrected. 2,3,5 When the intact limb was moved, the phantom limb was felt to move by the patient as well, relieving discomfort and pain associated with phantom limb immobility. 1,2 In other words, mirror therapy has the ability to alleviate PLP by restoring visual feedback of phantom movement.
Chan et al. 7 conducted a randomized, controlled study of mirror therapy with lower extremity amputees randomly assigned to one of three groups: mirror therapy, covered mirror therapy, and mental visualization therapy. Patients in the mirror group were asked to perform movements with the phantom leg/foot while viewing movements of the intact leg/foot in the mirror. Patients in the covered mirror group were asked to perform the same movements with the intact and the phantom leg/foot while the mirror was covered with an opaque sheet. Patients in the mental visualization group were instructed to simply close their eyes and to attempt to perform movements with their amputated leg/foot. Patients performed their assigned therapy daily for 15 min under direct study investigator observation and recorded the number, duration, and intensity of pain episodes. After 4 weeks of treatment, six of six (100%) amputees in the mirror group reported a decrease in pain, whereas only one amputee (17%) reported a decrease in pain and three (56%) amputees reported an increase in pain in the covered mirror group. 7 Only two (33%) amputees in the mental visualization group reported a decrease in pain, whereas four (67%) amputees reported an increase in pain. 7 Amputees in the covered mirror and mental visualization groups who crossed over to mirror therapy subsequently reported decreased PLP. 7 These findings indicate that visual feedback forms the basis of the efficacy of mirror therapy.
Given the simplicity of mirror therapy, we examined whether it would be feasible to use telemedicine to instruct amputees to self-administer this treatment for PLP. Two patients with major limb amputations self-administered mirror therapy under the remote supervision of a trained physician. Both patients experienced successful reduction and elimination of PLP as a result.
Mirror Therapy
Mirror therapy consists of a mirror placed between the intact and phantom limbs, as demonstrated in Figures 1 and 2. The patients were instructed to place the residual/phantom limb on one side of the mirror and the intact limb on the other side and to start with the intact limb in the same position that the phantom limb was felt to be positioned. Patients were then instructed to move the intact limb very slowly while viewing the reflected image in the mirror and simultaneously moving the phantom limb, to mimic the movements seen in the mirror. Plantar flexion and extension, foot rotation at the ankle, and knee flexion and extension were the easiest lower limb movements, whereas opening and closing the hand into the shape of a fist, wrist flexion and extension, and forearm flexion and extension were the easiest upper limb movements. Movement speed of the intact limb was increased once the patient reported sensation of movement of the phantom, and phantom movements kept time with the reflection that the patient viewed in the mirror. Prior to daily therapy, the patients indicated the level of pain experienced over the past 24 h on a 4-inch visual analog scale (VAS), along with the number and duration of pain episodes, which were used to track the progress of mirror therapy over a 4-week treatment regimen. The patients were advised through e-mail to perform mirror therapy treatment for 15 min, 5 days a week for 4 weeks initially and continuing as needed for up to 8 weeks. The patients purchased their own mirrors and were instructed to completed self-report assessments of pain daily for the duration of the therapy.

Example of an individual with above-knee amputation.

An individual undergoing mirror therapy.
Case Reports
Two patients with major limb amputations were e-mailed instructions for mirror therapy after initiating contact with a trained physician through e-mail. The instructions consisted of PowerPoint® (Microsoft, Redmond, WA) slides directing the patients how to self-administer mirror therapy and a figure demonstrating mirror set-up. In accordance with Health Insurance Portability and Accountability Act guidelines, all e-mails related to the remote treatment of these 2 patients were exchanged through a secure messaging system and encrypted. The patients were instructed to follow up with the physician after completing 1 month of therapy and periodically with any questions or concerns.
Patient 01
An 86-year-old woman received an above-the-knee amputation as a result of infection following a femur fracture in the right leg. On a 4-inch VAS, with 0 indicating no pain and 4 indicating the worst pain imaginable, the patient reported an initial pain score of 4/4. The patient indicated that PLP episodes occurred an average of three times daily, with each episode lasting 1–2 h, and described the pain as a burning pain in the phantom leg accompanied by occasional spreading of pain to the intact leg. Multiple pain medications were ineffective in relieving the pain. The patient contacted the second author via e-mail 6 months after amputation requesting instructions for mirror therapy to be conducted at home. After 4 weeks of daily therapy, the patient's pain level had decreased to 0.25/4 (6% of total pain) and a frequency of at most one episode per day, with each episode lasting no more than 20 min. At that time, the patient did not have flexion or extension of the phantom limb but was able to rotate the phantom foot at the ankle. After a telephone conversation with the physician, the patient restarted mirror therapy 4 months after previously stopping therapy. By the end of the second 4-week course of therapy, PLP had completely resolved. The patient confirmed in a follow-up e-mail that PLP had not returned at the time of article revision.
Data for Months 1 and 2 of self-administered therapy are depicted in Figure 3, with a concomitant decrease in number and duration of episodes. Data for Days 1–8 during Month 1 were not recorded by the patient. Data trends across Months 1 and 2 demonstrate a marked improvement in pain, as well as decreased frequency and duration of PLP episodes. After the first day of Month 2 of therapy, the patient no longer experienced PLP episodes (Fig. 4). Episode duration decreased across Month 1, and the patient did not experience any PLP episodes after the first session of Month 2 therapy (Fig. 5).
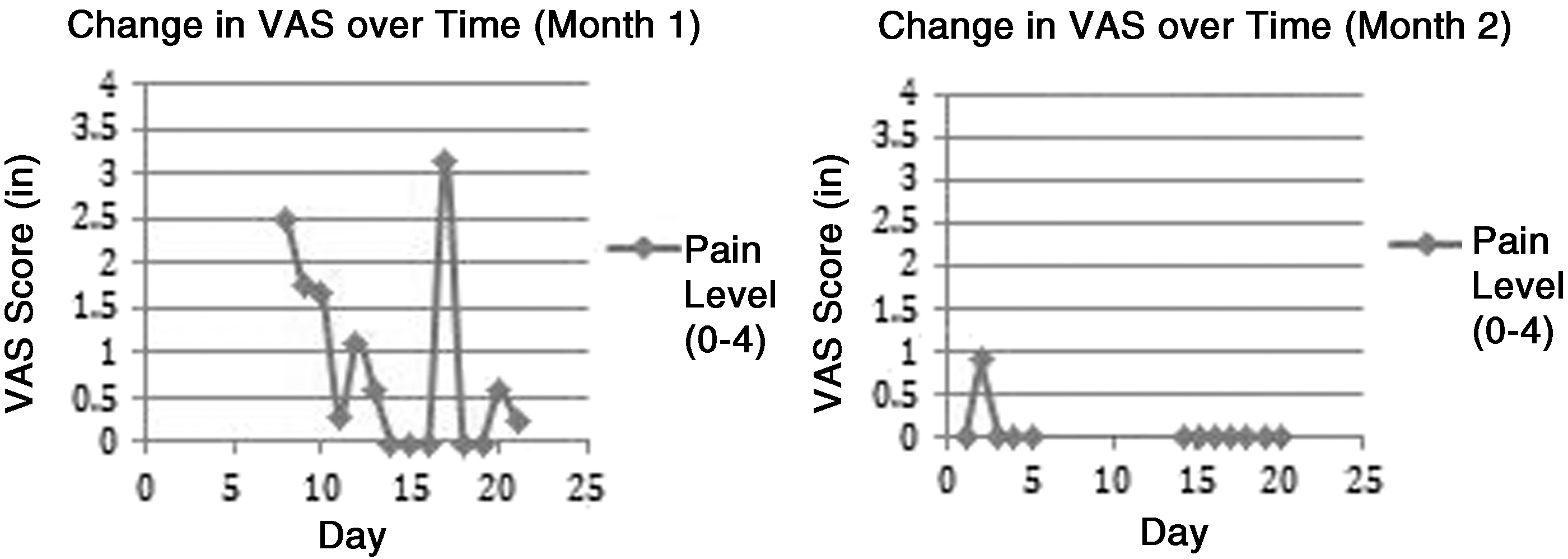
Change in visual analog scale (VAS) over time in
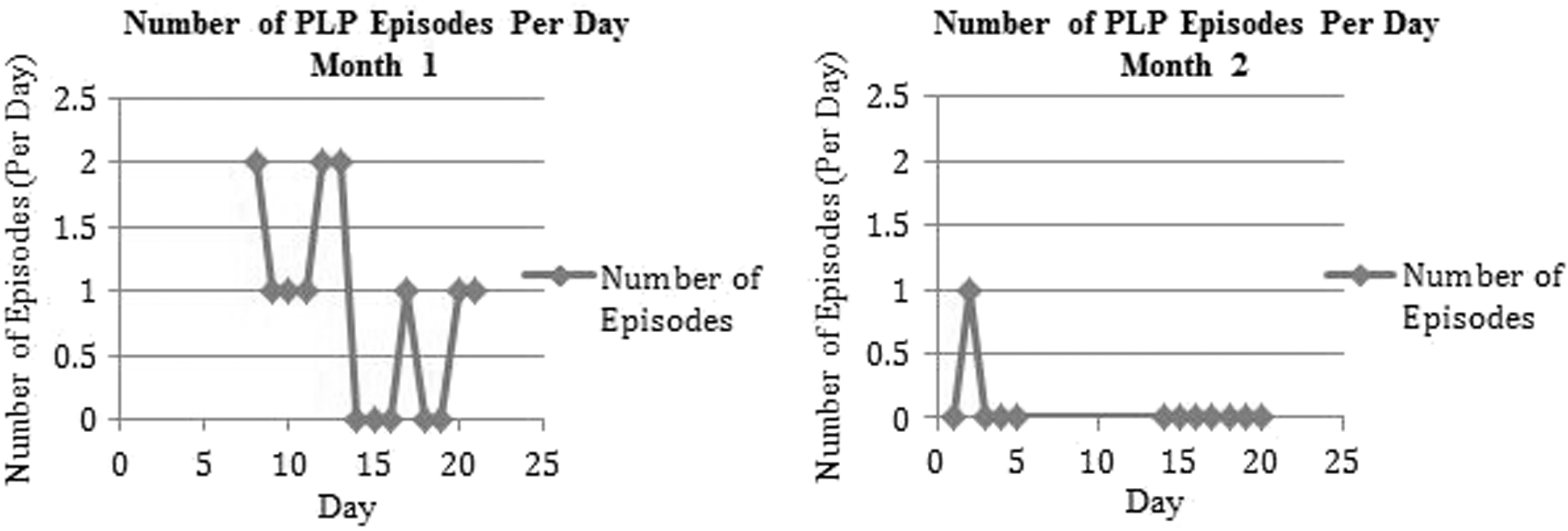
Phantom limb pain (PLP) episodes per day in
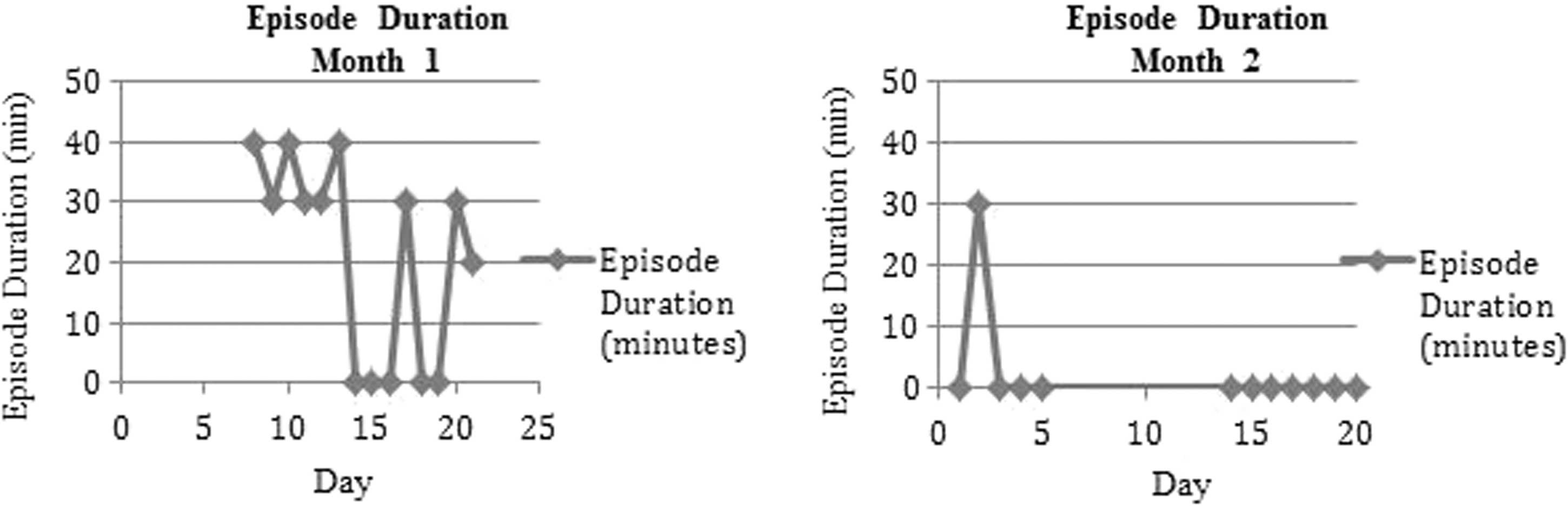
Phantom limb pain episode duration in
Patient 02
A 50-year-old man received a right upper extremity, above-elbow amputation. The patient was prescribed mirror therapy after having suffered from PLP for 2 years. He initially reported persistent PLP of 2.4–3.2/4 on a 4-inch VAS. The episodes occurred three to five times a week and lasted a few minutes. Medications were ineffective in relieving pain. The patient received instructions for mirror therapy to be conducted at-home through e-mail. After 4 weeks of self-administered therapy, the patient reported to the physician that his PLP had completely resolved. Individual data are not available for this patient.
Discussion
Mirror therapy is an efficacious treatment for PLP. The successful elimination of pain through self-administered mirror therapy presents important implications for the future of telepain management and telerehabilitation. The ability to self-administer mirror therapy will help to eliminate distance barriers and improve access to medical services for patients, with minimal disruption to a patient's daily life. Patients who live in remote regions without access to pain specialists will especially benefit from the ability to self-administer mirror therapy at home. Remote patient monitoring through e-mail will enable patients to choose when and where to self-administer mirror therapy under the direction of a physician or therapist, reducing the need for outpatient visits and the overall cost of rehabilitative care. Self-administration of mirror therapy also has the potential to greatly benefit military service members and veterans with amputations, many of whom travel great distances to be treated at military or Veterans Affairs hospitals.
Although the use of e-mail provides a digital bridge between patients and their physicians, there are other applications of telemedicine through which patients might benefit from both cost and time savings as an alternative to visiting hospitals or clinics for rehabilitative care. YouTube videos that instruct patients how to self-administer therapy at home could prove greatly beneficial, as they provide visual and audio instruction for therapy. For example, one video of a U.S. Army soldier conducting mirror therapy has been viewed by more than 100,000 individuals. 8 Instructions could also be delivered through PowerPoint presentations, accessible through any laptop or desktop computer, through which patients could receive instruction for therapy to be completed in the place and time of their choosing, as was done for both patients described here. These digital alternatives may help relieve the social and economic burdens of in- and outpatient rehabilitative care.
Consistent with other published reports, mirror therapy provided relief from PLP to the amputees described above who had been unable to alleviate pain through other treatments. The ease with which the patients were able to self-administer mirror therapy afforded greater flexibility to choose the time and location of treatment. These cases demonstrate that mirror therapy can be performed successfully using telemedicine.
Footnotes
Disclosure Statement
No competing financial interests exist.