
Abstract
Introduction
Neonatal hearing screening and tracking enjoy international and interdisciplinary support and have been a mandatory service in Germany since 2009. 1 Screening all newborn babies in the first few days of life for the presence of a hearing disorder significantly reduces the age of diagnosis and care requirements of the children concerned. 2 The success of a screening program depends on successful tracking and follow-up to ensure that babies referred from the clinic receive appropriate and timely diagnostic and intervention services. 3 The management of information relating to findings, quality control of measurements, and timely coordination of all those involved in the diagnostic process is both challenging and time consuming.
In small locally based projects, it is possible to coordinate the exchange of information between clinics, parents, follow-up centers, and tracking centers using paper-based solutions or phone and e-mail. However, as the size of the project increases, such communication methods become inefficient. 4
Different information management concepts, which have a varying degree of effectiveness, have emerged from various countries. In The Netherlands, where identical screening devices are used throughout the country, the data are transmitted directly from the devices to the central tracking database by means of an analogue modem. 5 In England, the transmission of screening results is done using the national information system eScreener Plus (eSP). 6 In the United States, the Centers for Disease Control and Prevention have defined national goals, program objectives, and performance measures for early hearing and intervention and tracking programs according to the recommendations of the Joint Committee on Infant Hearing. 7,8 Young, Keogh, and Glennon showed in their review how different the information management in nine international newborn hearing screening and tracking projects is and how much manual work must be done. 9
In 2008, the German legislature missed the chance to make national requirements for information management and tracking systems as an addition to the quality and target parameters, which were defined. 1 This is unfortunate because, according to Downing et al. and Houston et al., the easy and timely availability of the necessary data through a suitable infrastructure for the tracking, diagnosis, and care of children concerned is a major challenge for the successful development of the newborn hearing screening. 10,11
The Clinic for Phoniatrics and Pedaudiology, University Hospital of Muenster, Germany, runs a screening and tracking center for Westphalia-Lippe—part of the state of North Rhine-Westphalia—with responsibility for more than 55,000 babies every year. In this program, 58 maternity clinics and 37 follow-up centers exchange hearing screening data with the tracking center.
The following data transmission problems resulted in our tracking center requiring a significant level of on-site support.
In our project, only trained and certified staff from the maternity clinic are permitted to send screening data. In view of the considerable levels of staff turnover and the need to offer additional training for individual staff, we offer off-site training sessions. In such instances, one of our technicians must visit the clinics to enter personal data into the screening device.
Data transfer connections between screening devices and the tracking center always depend on cooperation between the IT department and the data protection department of the hospital concerned. In this study, again, on-site support from the tracking center is needed. Increasingly, we are encountering problems in modern hospitals when installing analogue modem technology for data transfer, owing to a lack of suitable connection points.
Regular maintenance activities (annual inspections) often result in incorrect or incomplete configurations of replacement devices in the clinics.
The screening devices used in our project permit the transmission of additional comments relating to the measurements. The preset comments stored in the device are particularly important for statistical analysis according to the guidelines set out by the German Federal Joint Committee. Changes can normally be made by the instrument manufacturers as part of annual inspections, although the resulting time delay is unsatisfactory in practice.
One solution to the problems described above can be found in a so-called “out-of-the-box” data transmission solution for screening devices, which is configured by the hearing screening center before delivery to the clinic and operates independent of the clinic infrastructure. This provides the option of two-way data transfer between the screening device and the tracking center, which makes on-site support for updates of login permissions, the comment list, and other configuration data unnecessary.
In a research project funded by the state of North Rhine-Westphalia and the European Union, a system for the automated transmission of hearing screening data based on mobile communication technology for the screening devices Natus Echo-Screen® and MADSEN AccuScreen® (that was first launched at the newborn hearing screening conference in Cernobbio, 2010) was developed and used in a field study to overcome the issues above.
This study aims to investigate the speed, reliability, and frequency of use of a radio modem solution for screening devices in newborn hearing screening compared with a conventional analogue solution.
Materials and Methods
Technical Background
Together with partner companies Path medical, Telekom Germany, and the Institute for IT and Biomathematics of the University Hospital of Muenster, we developed an alternative solution to the existing analogue modem used with the Natus Echo-Screen.
The device contains a terminal module with a radio modem that has technical approval in nearly all countries.
As the functional protocols of the Natus Echo-Screen with its analogue modem have previously been published, it has been possible to develop an alternative solution on them without the need to make changes to the Echo-Screen firmware. The wireless modem interacts with the Echo-Screen in the same way as an analogue modem, which is an option for the device. There is no difference from analogue technology in the way in which data transfer is initialized. Data transfer is made using the Secure Sockets Layer (SSL) Protocol, which ensures secure data transmission through the Internet. At the tracking center, the new program receives the connection request. Identification is verified using standard public key certificates (X509). Each radio modem can also be identified from its International Mobile Station Equipment Identity (IMEI).
We used general packet radio service (GPRS), which is the packet-switched standard for data transfer of the Global System for Mobile Communication (GSM). It has sufficient bandwidth for the transmission and has complete coverage in Germany and in many other parts of the world. 12
The transmission route is part of the data protection plan implemented by the tracking center and is approved by the data protection official. Subsequent data flows within the tracking center take place in the same way as before, through analogue modem or encrypted e-mail attachments.
It is possible to transmit data from the tracking center to the screening devices this way. This has been achieved through the implementation of a method, by which files can be sent. When the correct commands are entered into the command files for the modem, updates for user lists or comments will be downloaded the next time screening data are exchanged.
The second stage involves the development and testing of an integrated wireless solution based on the same technology and offered as an option with MADSEN AccuScreen. Ten prototypes of the MADSEN AccuScreen with an integrated solution for the docking station were developed. It is also possible to connect an external modem to the device without needing to make any changes to the docking station.
Figure 1 shows the possibilities for data transfer between the screening device and the tracking center using two-way connection.
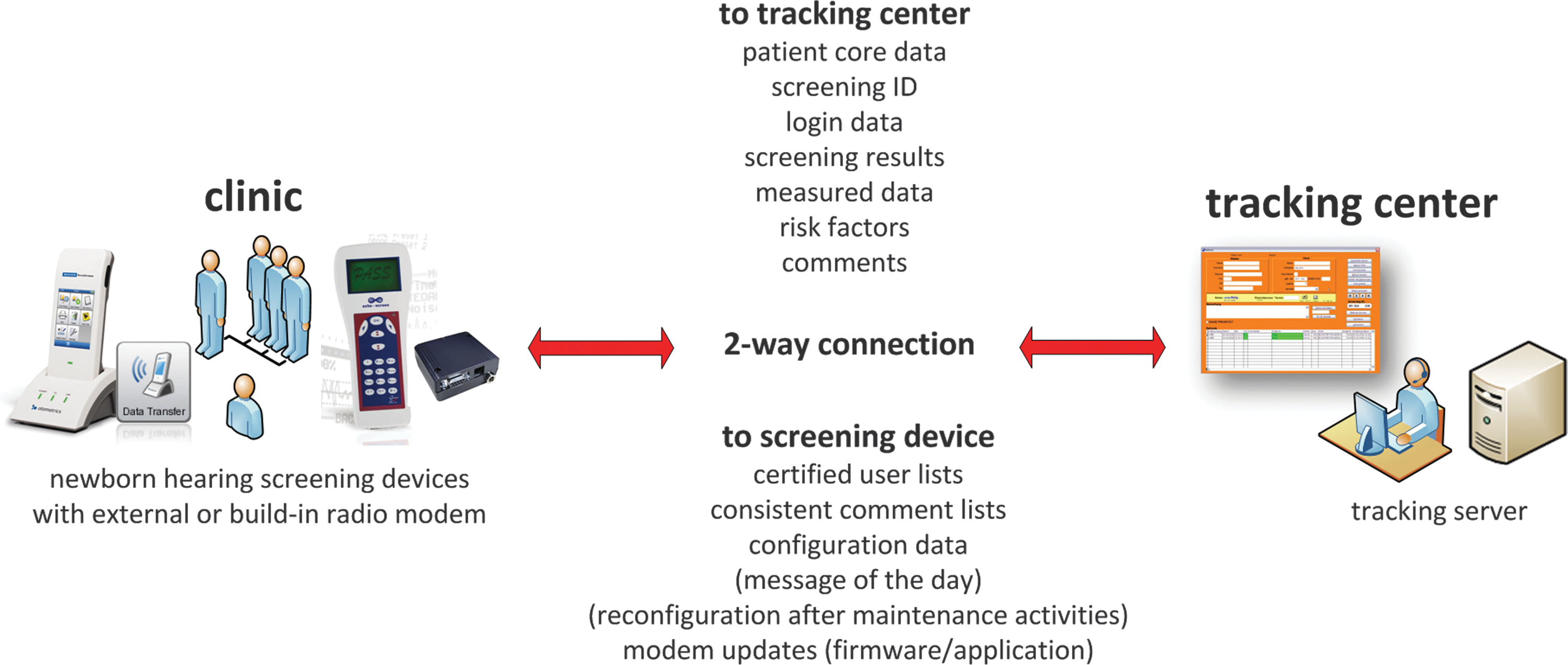
Data transferred to and from tracking centers using screening devices with two-way connections.
The radio modem solution is integrated into our data flow in Westphalia-Lippe as shown in Figure 2.
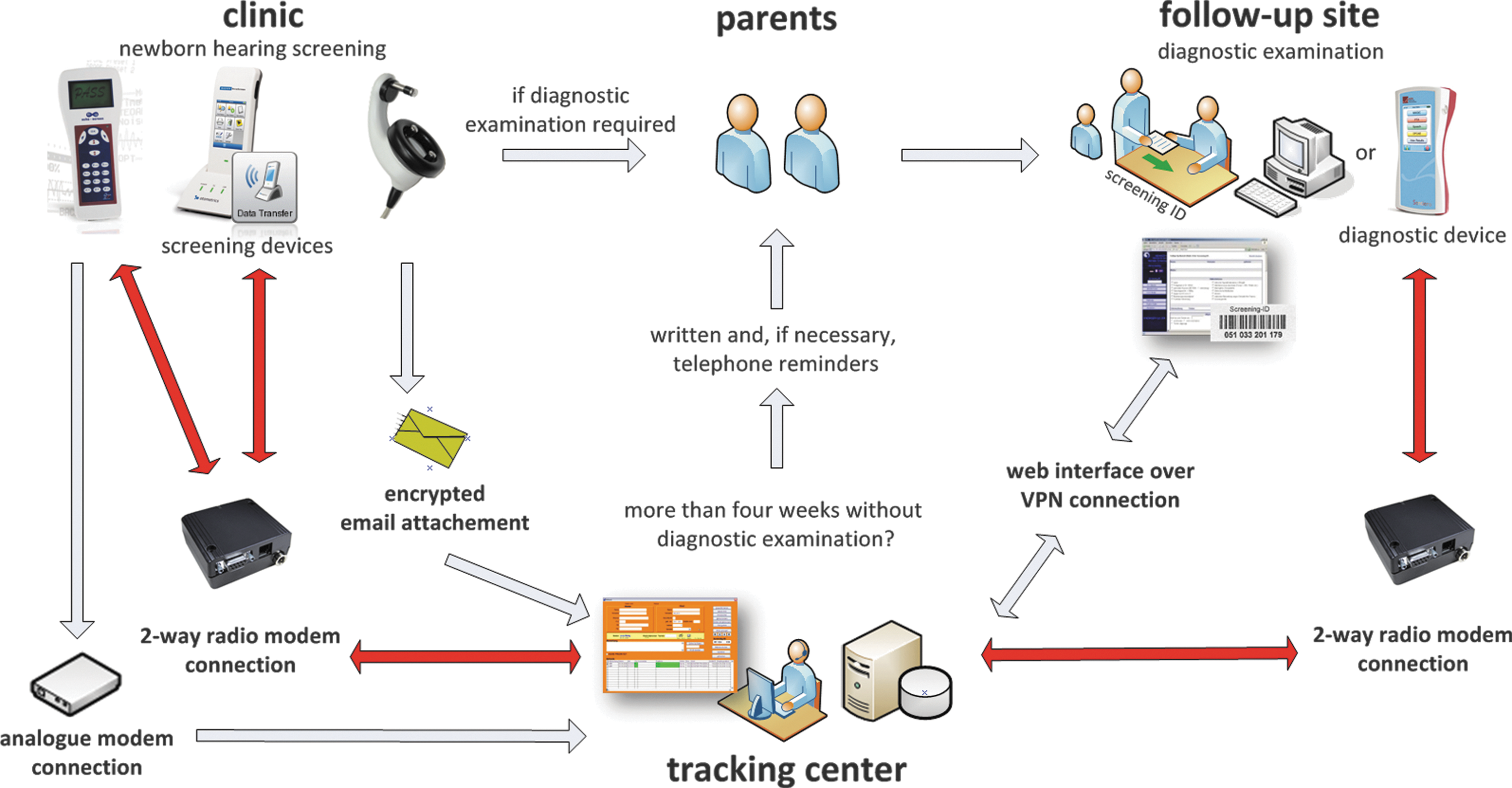
Integration of the radio modem solution (red arrows) in the data flow of the hearing screening program.
Field Study
We conducted a field test in 12 maternity clinics in our project. We started with the external radio modem solution in six hospitals, which used a Natus Echo-Screen for screening. Six other clinics were supplied with the internal radio modem solution for the MADSEN AccuScreen (built-in docking station).
The log files of 687 (463 with the Natus Echo-Screen and 224 with the MADSEN AccuScreen) instances of information transfer of the two radio modem groups were compared with 7,809 log files of analogue transmissions from Natus Echo-Screen devices on the basis of session duration, volume of data, transmission rate, number of lost connections, and frequency of data transmission. The null hypothesis was that the use of radio modem technology had no effect on session duration, volume of data, transmission rate, number of lost connections, and frequency of data transmission.
The raw data were taken from the different logs of transmissions with a program that was written for this purpose. The sample was then analyzed by IBM SPSS Statistics 20. 13
The homogeneity of the variance was tested with a Levene test and the distribution of the data with a Kolmogorov–Smirnov test. Since the homogeneity and the normal distribution for some parameters and groups were not given, we had to use nonparametric tests for testing the group differences.
The sample was calculated with a Kruskal–Wallis H test and a Mann–Whitney U test as a post hoc test with a Bonferroni correction.
Results
The average volumes of transmitted data and login and transfer of configuration data for the device in the mobile radio groups (10,141–36,738 bytes) were comparable with the volume of the conventional transmission group (19,725 bytes).
The groups differed significantly in session duration and transmission rate. The average session duration for the group with the analogue modem was 108 s, while the Echo-Screen and AccuScreen radio modem groups required only 12 and 15 s, respectively. The transmission rate was much higher in the radio modem groups, with 898 and 1,758 bytes per second, compared to the analogue modem transmission rate of 181 bytes per second. Both results are shown in Table 1.
Session Duration and Transmission Rate
Both radio modem groups had significantly lower rates of broken connections than the analogue modem group after an initial connection (Table 2).
Session Duration and Transmission Rate
Both connection breaks occurred after complete transmission of patient data.
We observed an increase in the frequency of data transmission from the maternity clinics (n = 48) in the mobile radio transmission groups, as shown in Table 3.
Frequency of Data Transmissions
Outlier analysis to identify, for example, annual inspections and replacement devices.
Discussion, Perspectives, and Conclusions
It was not surprising, on technical grounds, to see significant improvements in terms of average session duration when using the mobile communication technology. This is the result of the significantly higher transmission speed of this technology than the low rate of the analogue modem. The differences between the two radio modem groups can be explained by the limitations of the modem interfaces and the overhead of the protocols used. Since we could not make any changes to the firmware of the Natus Echo-Screen, we were limited to the given interface speed, which is much lower than that possible using the radio modem. For the MADSEN AccuScreen, however, we could use the maximum serial transmission rate, both internally and externally.
We were surprised by the 5.5% of broken connections in the analogue group. The correlation of r = 0.63 indicates that there is a significant (p < 0.01) relationship between the size of the transmitted data and the number of broken connections within the analogue modem group. Mobile communication technology enables the use of connections, which are more stable. This saves time and prevents staff frustration.
The most important result of the field study was the increase in the frequency of data transmission in the mobile radio transmission groups. This was surprising to us, since there was no call for staff to transmit data more often. In our view, this is a result of a behavioral change in staff members and shows that simple-to-use technology can change behavior in a positive direction. Earlier feedback allows for timely questions and earlier tracking of the children. We think that the further reduction in the time interval between transmissions in the MADSEN AccuScreen groups with radio modem technology (group 3 in Table 3) is because data transmission can be carried out very simply directly from the main display menu. It seems to be a result of the seamless integration and user-friendliness of the mobile communication technology.
The amount of data transmitted per month and per clinic is very low, with each transmission consisting of only a few kilobytes. The cost of transmission varies according to the Internet service provider used and from country to country. In this project, we used a Machine-to-Machine Communication (M2M) service from Deutsche Telekom, which costs €1.93 per device per month (€1.19 basic price and €0.74 for 5 megabyte of data per month). 14
This solution seems to be optimal for use in countries without cable-based telecommunication infrastructures or where these infrastructures are unreliable. In this regard, the limitation of a terminal module with the relatively slow modem used in this project can be avoided, because other terminal modules with bandwidths of several hundred kilobits per second are available.
In comparison with the analogue system, the new technology has approximately the same acquisition costs and overhead (telephone and infrastructure costs compared with cost for the M2M service), is more reliable, has lower support costs, and has high additional value because of the two-way data transfer.
According to the European Medical Device Directive (Directive 93/42/EWG), annual inspections of the devices are regulated by the German Medical Devices Act (Medizinproduktegesetz, MPG) in conjunction with the Medical Devices Operator Ordinance (Medizinprodukte-Betreiberverordnung, MPBetreibV). 15 –17 Issues raised over unambiguous assignment of replacement devices are smoothly resolved using the two-way data flow.
The use of mobile communications technology is not limited just to the exchange of data between a clinic and the tracking center. Two-way transmission also has advantages for the exchange of data between the follow-up sites and the tracking center. In addition to the data shown in Figure 1, the following patient-related data, for example, can also be sent directly from the device to the tracking center: • audiological data • etiological data • diagnosis • scheduling
The following data from the tracking center can be retrieved or sent to the device: • patient core data • screening results • risk factors • configuration data
Previous findings are available and data need not be entered more than once. Our project partner, PATH medical, has recently developed just such a device for the special needs of follow-up sites. 18
The bidirectional aspect of this technology also allows for easy-to-use teleconsulting with the measured data. This could be the first step in changing the information management strategy of universal newborn hearing screening from a telematic solution to a telemedicine application.
Footnotes
Acknowledgments
This project, including the field study, was supported by the state of North Rhine-Westphalia and the European Union (Med.in NRW/GW01-090).
Disclosure Statement
The authors of the University Hospital of Muenster (UKM) and the Technical University of Munich (TUM) have no financial interest in this article. PATH medical coauthors report no financial or other conflict of interest relevant to the subject of this article.