
Abstract
Background:
Despite being less costly than prolonged hospitalization, home parenteral nutrition (HPN) is associated with high rates of post-discharge complications, including frequent readmissions and central line-associated bloodstream infections (CLABSIs). Telemedicine has been associated with improved outcomes and reduced healthcare utilization in other high-risk populations, but no studies to date have supported effectiveness of telemedicine in pediatric HPN.
Methods:
We prospectively collected data on pediatric patients managed at a single HPN program who participated in postdischarge telemedicine visits from March 1, 2014 to March 30, 2016. We excluded patients with a history of HPN and strictly palliative care goals. Univariate analysis was performed for primary outcomes: Community-acquired CLABSI and 30-day readmission rate.
Results:
Twenty-six families participated in the pilot initiative with median (interquartile range) patient age 1.5 (5.7) years old, diagnosis of short bowel syndrome in 16 (62%), and in-state residence in 17 (55%). Ishikawa (fishbone) diagram identified causes of post-discharge HPN complications. Areas of focus during telemedicine visit included central venous catheter care methods, materials, clinical concerns, and equipment. Compared to historical comparison group, the telemedicine group experienced CLABSI rates of 1.0 versus 2.7 per 1,000 line days and readmission rates of 38% versus 17% (p = 0.03, 0.02, respectively).
Conclusions:
Telemedicine visits identified opportunities for improvement for families newly discharged on HPN. In a small cohort of patients who experienced telemedicine visits, we found lower CLABSI rates alongside higher readmission rates compared with a historical comparison group. Further studies are needed to optimize telemedicine in delivering care to this high-risk population.
Introduction
Home parenteral nutrition (HPN) is a complex therapy offered to children and adults suffering with a variety of severe digestive diseases, such as short bowel syndrome, motility disorders, and malignant bowel obstruction. 1 Patients require close monitoring as HPN provides individualized provision of intravenous hydration, electrolytes, protein, sugar, fat, vitamins, and minerals. In the United States ∼40,000 patients receive HPN, which offers improved quality of life and reduced medical expenses to the healthcare system over prolonged hospitalizations. 2,3 Despite improving survival and other outcomes, HPN remains associated with high morbidity and expense. 3,4 Patients are at particularly high-risk for complications such as readmissions and central line-associated bloodstream infections (CLABSIs) within the first 30-days post-discharge. 5,6 The average annual estimated cost per patient of HPN care is $296,808, with ∼60% of those costs attributable to ancillary inpatient care. 7
In March 1, 2014, the HPN program at Boston Children's Hospital started offering scheduled telemedicine visits on a limited basis upon initial hospital discharge. Telemedicine visits were not a substitute for face-to-face outpatient visits. The number of telemedicine visits was limited to one per parent based upon program resources, as neither the patient nor insurance was charged for this service. The standard HPN telemedicine visit includes a gastroenterologist, nurse practitioner, pediatric nurse, program coordinator, a parent, the patient, and any homecare providers.
In adult HPN programs and pediatric feeding disorders programs, telemedicine offers reduced costs of travel to patients, higher patient satisfaction with their care plan, and effective recommendations enabling treatment in their home community. 8,9 In selected patient populations, telemedicine can improve outcomes and reduce healthcare utilization such as frequency of ambulatory visits, emergency department visits, and hospitalizations. 10 –12 Management of chronic healthcare conditions is a valuable target for telemedicine, because medical teams are responsible for supporting families with complex self-care in the home setting. 4,13 To our knowledge, there have been no studies describing telemedicine outcomes in pediatric HPN patients.
We therefore investigated whether early post-discharge telemedicine visits might support particular elements of clinical decision-making and affect patient outcomes for our pediatric HPN program.
Methods
Study Subjects
We collected data on all post-discharge telemedicine visits conducted from March 1, 2014 to March 30, 2016. Inclusion criteria for telemedicine cases were enrollment in our HPN program, ages <18 years at initial discharge on HPN, at least 30 days post-discharge follow-up, and all possible diagnoses leading to HPN dependence. We excluded patients with short-term HPN use defined as <30 days of follow-up (unless readmission occurred within 30 days). We identified historical comparison cases from a nested cohort of patients initially discharged on HPN matched on age within 5 years and sex (1:1) from years 2000 to 2017. In both groups, we excluded patients with strictly palliative goals of care. This work met our institution's definition of quality improvement and therefore Institutional Review Board review was not required.
Study Design
The videoconferencing software (Vidyo Corporation, Hackensack, NJ; version 3.5.2) allowed encrypted communications. It was provided free for families via e-mail to download. Videoconferences were not recorded, but were documented in the patient's medical record. The program coordinator scheduled telemedicine visits and sent an e-mail confirmation to the family. Table 1 summarizes rapid cycle improvements incorporated into post-discharge telemedicine visits process. Based upon feedback, we invited others to participate in the telemedicine visits and enabled our coordinator to help families troubleshoot. Families advised that we schedule telemedicine visits at 48–72 h after initial discharge. Certified medical interpreters facilitated telemedicine visits for non-English speaking families.
Rapid Cycle Improvements Incorporated Into Post-Discharge Telemedicine Visits
At time of post-discharge telemedicine visits, HPN staff completed a standardized case report form in research electronic data capture (REDCap). 14 As part of the HPN program's ongoing quality improvement activities, we collected data prospectively via a combination of automated database algorithms, medical chart review, and clinic interview on the following: Patient demographics, central line placement and removal, hospitalizations, as well as CLABSI, which was defined according to Center for Disease Control definition. 15
Analysis Approach
We summarized continuous variables using median (interquartile range) and categorical variables using frequency (%). We compared all cause 30-day readmission rates, including non-HPN-related and HPN-related hospitalizations. We compared proportions or categorical variables using the chi-squared test or Fisher's exact test in case of small cell counts; we used the Wilcoxon rank-sum test to compare continuous variables. We performed conditional logistic regression to compare odds of 30-day readmission and CLABSI. Based upon individual visit case report forms, a separate member of the HPN nursing staff itemized responses into themes (e.g., environment, materials, methods, and people), which formed the basis for our Pareto chart (Fig. 2). We analyzed all data using R (R Foundation, v3.1.0) and SAS (SAS Institute, v9.3), using two-sided hypothesis tests with 0.05 significance level unless otherwise noted.
Results
During the study period, 26/67 (39%) families participated in the telemedicine quality improvement initiative. Table 2 summarizes demographic characteristics of study participants. The HPN program delivered telemedicine visits within 48 h for 20/26 patients (77%), and HPN physicians spent median time of 32 min (15–63) during the 18 visits where physician time was collected.
Demographic Characteristics in 205 Home Parenteral Nutrition Patients
GI, gastrointestinal; MA, Massachusetts.
To help understand causes of post-discharge complications, our HPN team created an Ishikawa (fishbone) diagram (Fig. 1). Telemedicine visits could conceivably address the following causes of complications: inspection for quality, support documentation, adequate supply, barriers to following up, caregiver technique, caregiver training, access to communicate with medical providers, distance to medical facility, financial resources, stress, social supports, family perceptions, unhealthy perceptions, nursing availability, comorbid disease, medical literacy, nutrition/hydration status, and cultural barriers to care. The clinical management areas requiring attention during actual HPN post-discharge visits are summarized in the Pareto chart on Figure 2. Commonly reported problems related to “Methods” included education/training; trouble using the central line; and safe and proper care technique. The most commonly reported problems related to “Materials” included supply delivery problems, insufficient materials, and wrong supply type. The most commonly reported problems related to “Clinical complaints” included vomiting, changes in bowel habits, and edema.
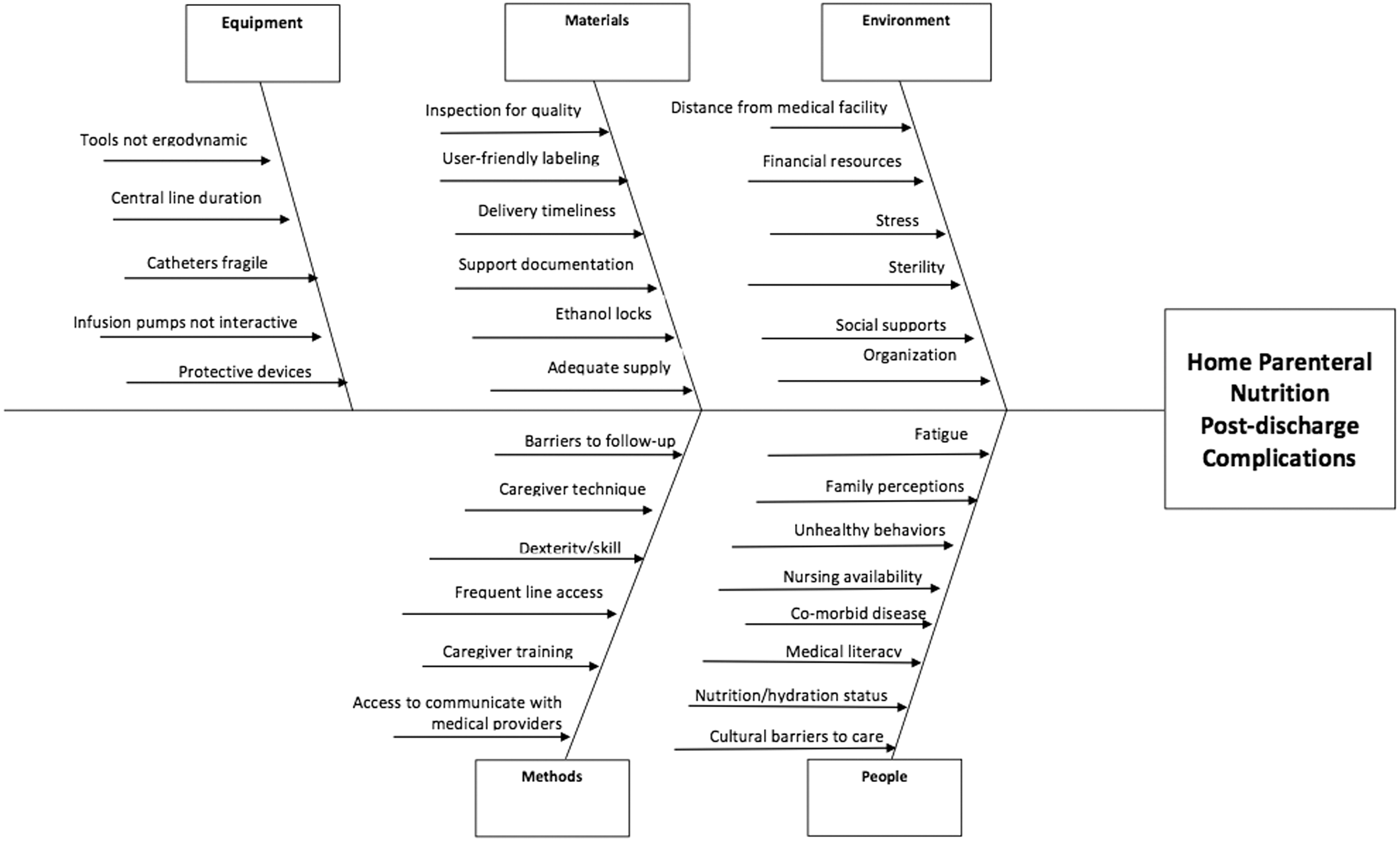
Ishikawa (fishbone) diagram of causes leading to post-discharge home parenteral nutrition complications.
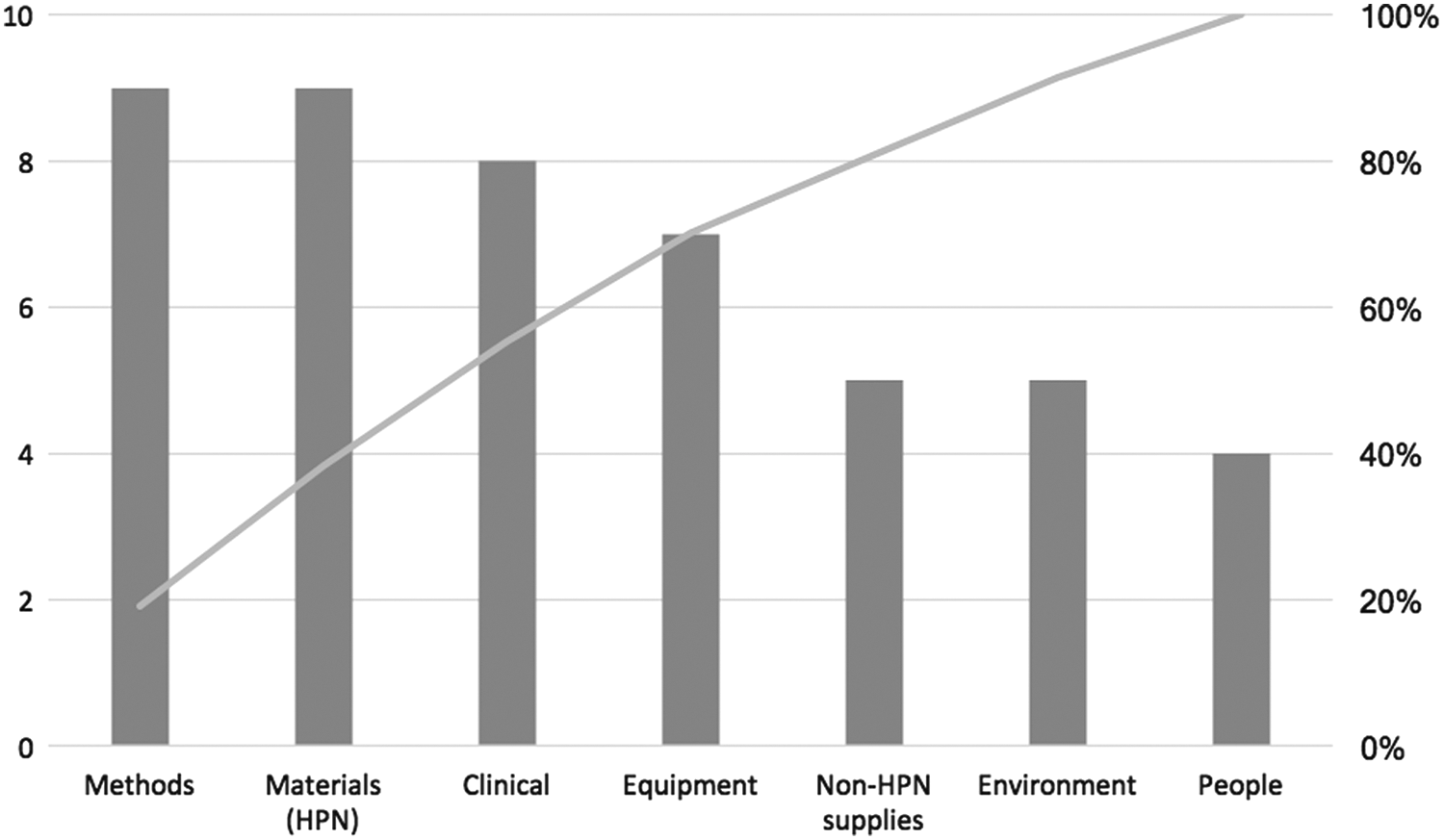
Pareto chart of issues requiring consideration during post-discharge HPN visits. HPN, home parenteral nutrition.
We observed higher readmission rates and lower CLABSI rates in patients who experienced telemedicine visits compared with historical comparison group. Ten of the 26 patients (38%) in the telemedicine group experienced readmission versus 36/208 (17%) among historical comparison group (odds ratio [OR] = 2.9, 95% confidence interval [CI]: 1.21–6.87, p = 0.02). A similar effect persists after adjusted analysis in a matched cohort (adjusted OR = 2.7, 95% CI: 0.70–10.1, p = 0.15). CLABSI rates in the telemedicine visit versus historical comparison group were 1.0 versus 2.7 per 1,000 line days, respectively (rate ratio [RR] = 0.38, 95% CI: 0.16–0.91, p = 0.03). Results are essentially unchanged when using the matched cohort (adjusted RR = 0.42, 95% CI: 0.17–1.05, p = 0.06).
Discussion
We conducted a quality improvement initiative of early post-discharge telemedicine visits involving 26 pediatric HPN patients. Our staff provided brief telemedicine visits that identified a variety of post-discharge HPN care issues. The patients experience a high rate of complications such as readmissions and CLABSI, and telemedicine visits may have the potential to reduce these complications.
Our Ishikawa (fishbone) diagram was helpful in identifying preventable causes of complications that telemedicine visits might target over face-to-face, phone, or e-mail interactions. Staff identified and addressed gaps in discharge training. Providers used screen sharing to review educational materials. Families found demonstrating home care products in real time is particularly helpful when troubleshooting supply and delivery issues. Using the far-end camera with the videoconferencing software, families were able to pan and zoom with good accuracy. Future work should evaluate how other videoconferencing software features provide value added services to telemedicine encounters.
During our pilot initiative, a HPN physician or nurse practitioner was present during of the entire telemedicine visit. The providers helped families recognize when early challenges represented common aspects of learning or warning of unsafe situations. HPN staff nurses were also present for the majority of the telemedicine visits. At 30 min, the visit time was similar to a typical outpatient follow-up encounter. However, not all areas of discussion were standard topics for providers to discuss with families, such as central line technique and home care supplies. Therefore, nursing staff alone might efficiently provide portions of the visit for greater value. Telemedicine visits could offer additional health services often missed in traditional office visits. One opportunity might be to incorporate pharmacy staff focusing on parenteral nutrition compounding issues, especially in light of the frequency we have recently reported these problems. 16 Telemedicine can address psychological as well as medical aspects of HPN, as early studies show promise for telehealth HPN group therapy sessions. 17
There are several challenges to offering telemedicine visits to HPN patients universally. Fragmented insurance coverage for telemedicine visits using a fee-for-service model has been a major barrier to telemedicine expansion. 18 Thirty-two states and the District of Columbia currently have reimbursement parity laws, mandating commercial payers reimburse providers equally for a telemedicine and in-person visits. 19 However, many of these states have stringent requirements where the patient can be located during the telemedicine encounter, such as another clinical site. 20 Other barriers to expanding telemedicine include the following: in-state medical licensure requirement; established in-person physician–patient relationship for all visits; attendance of a “attendance of” with the patient; and completion of telemedicine-specific informed consent forms. 21 Ultimately, consumer demand will allow families to access telemedicine, which offers more convenient, cost-effective, and accessible care when compared with traditional healthcare models. 22 Barriers such as reliable Internet and videoconferencing devices are expected to diminish over time. As of November 2016, 77% of Americans owned a smartphone, which include cameras, speakers, and audio sufficient for conducting telemedicine visits. 23 HIPAA compliant videoconferencing software is now easily accessible.
There are several limitations to this study. As the quality improvement intervention involved a relatively small number of subjects, it was not powered to evaluate endpoints of CLABSI and readmissions rates. Moreover, our study design was quasi-experimental, and therefore, not optimized for a planned evaluation. The project was offered to all families as part of a newly improved standard of clinical care model, so we did not randomize families to study the effect of telemedicine visits on their outcomes. Another limitation was that our team instituted multiple interventions over study time-period. Other than participation in telemedicine visits, multiple factors might contribute to our main outcomes of 30-day post-discharge CLABSI and all cause readmissions. Larger, multicenter studies might overcome these limitations.
One strength of this study is the study sample, which is broadly representative of the pediatric HPN population in general. 1 Another strength is that we studied telemedicine in a group who had much to gain: Over half of families were living out of state, so early ambulatory visits or home visits would carry heavy traveling burden. We did not limit our study population to those whose insurance offered reimbursement for telemedicine visits, mitigating selection bias. Future studies should evaluate safety and effectiveness of telemedicine in patients who face barriers to using telemedicine technology.
Conclusions
Hospitals, payers, accreditors, and families are increasingly looking to telemedicine to address post-discharge complications in high-risk populations, such as HPN. We found that telemedicine visits were brief, reasonably accessible, and successful at identifying important post-discharge care issues. More study will be needed to evaluate telemedicine interventions and post-discharge outcomes more rigorously.
Footnotes
Authors' Contributions
B.P.R., C.S., and A.O.: Substantial contributions to the conception, design, analysis, and interpretation of the work; drafting the article; and final approval of the work to be published. S.G.-G., J.M., C.R., C.T., M.G., M.T.-B., A.N.C., P.M., and C.D.: Substantial contributions to the analysis and interpretation of the work; and final approval of the work to be published.
Disclosure Statement
C.D. was supported, in part, by the National Institutes of Health (Grant Nos. K24DK104676 and 2P30 DK040561). For all other authors, no competing financial interests exist.