
Abstract
Introduction:
The University of Virginia's (UVA's) adult cystic fibrosis (CF) program implemented a rapid and successful transition to telemedicine care mid-March of 2020 in response to the coronavirus disease 2019 (COVID-19) pandemic. In May 2020, the adult UVA CF program redesigned the care model to adjust to the reopening of ambulatory operations and introduced hybrid clinics. The goal remained to minimize person-to-person contacts for patients and care team members (CTMs) while ensuring patient access to quarterly, coproduced, synchronous, multidisciplinary CF care, similar to pre-COVID-19 era regular CF care.
Methods:
Using quality improvement tools, the UVA adult CF program created a standardized hybrid model of care for in-clinic visits, which included combined components of in-person and synchronous virtual interactions with members of the multidisciplinary team.
Results:
A total of 16 hybrid visits occurred between May 14 and June 11, 2020. All hybrid visits were multidisciplinary and fulfilled patient requests to see CTMs. All patients seen by hybrid encounter participated in coproduced agenda setting, underwent spirometry, and obtained blood work; 75% provided sputum for surveillance culture. Each hybrid visit type was attended by an average of four CTMs and amounted to 63 separate interactions. Of these interactions, 28 were completed virtually, reducing in-person contacts and personal protection equipment utilization by 44% compared with a fully in-person model of care.
Conclusions:
Combining in-person and telehealth components in a multidisciplinary CF care model reduces patient and staff interactions and personal protective equipment utilization. The hybrid model of in-person/remote combined care enables reliable access to biological data to support medical decision making while mitigating the risks of person-to-person contact for patients and staff.
Background
Cystic fibrosis (CF) is a systemic genetic disorder that affects ∼30,000 people in the United States. 1 It affects multiple organs and systems and primarily causes increased morbidity and mortality through its effects on the respiratory system, and more specifically bronchiectasis. 2,3 The respiratory involvement places people with CF at higher risk of complications with any respiratory infections, especially respiratory viruses. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic emerged as a major world health problem at the beginning of 2020. As of June 2020, the rapid spread of the virus throughout the world has resulted in more than seven million infections and >400,000 deaths worldwide; in the United States alone, >100,000 people have died. 4 The University of Virginia's (UVA's) adult CF program made a rapid and successful transition to virtual care visits in mid-March 2020 in response to coronavirus disease 2019 (COVID-19). 5 By May 2020, the program needed to redesign the care model yet again to adjust to the reopening of ambulatory clinics for nonurgent care (Fig. 1). The reopening coincided with health system-wide staff reductions, furloughs, and stay-at-home orders and required strategic decisions by care team members (CTMs) to minimize physical presence in the clinic space for the safety of patients and CTMs.
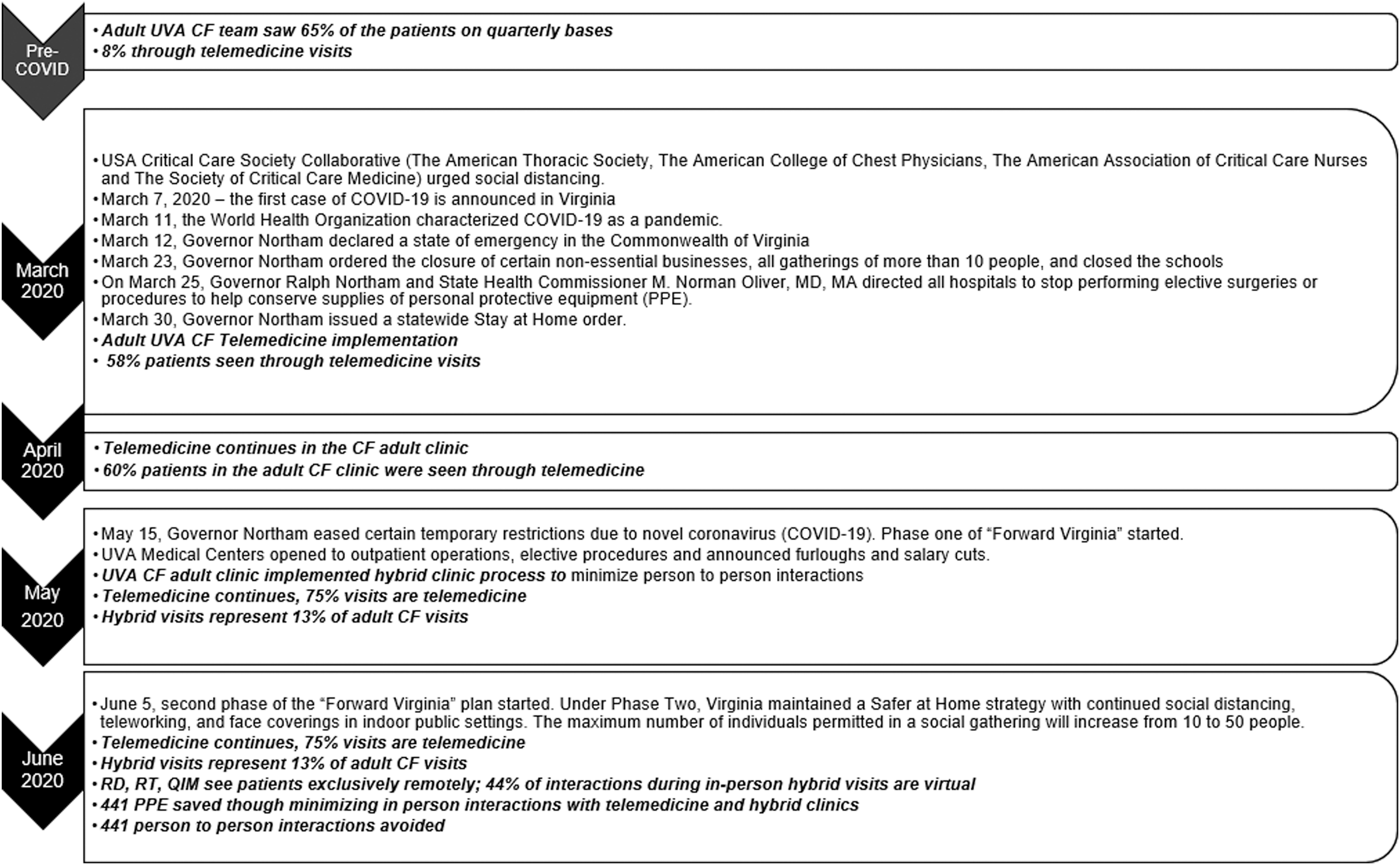
Timeline of changes in recommendations related to social distancing in Virginia and implications to changes in clinic type at UVA adult CF clinic. 6 CF, cystic fibrosis; QIM, quality improvement manager; RD, registered dietitian; RT, respiratory therapist; UVA, University of Virginia, USA.
AIM
In the context of increased economic pressure to open the health care system to outpatient clinic visits, the UVA CF team has developed a standardized process for hybrid multidisciplinary CF adult visits that include in-person and virtual interactions in a single clinic experience. The adult program goal was to minimize person-to-person contacts for patients and CTMs while ensuring patients would have continued access to coproduced and multidisciplinary care during every CF clinic visit. (Coproduced visits are visits in which agenda for the visit is produced in collaboration with the patient.)
Methods
Using quality improvement (QI) tools, the UVA adult CF program created a standardized hybrid model of care for in-clinic visits to include a few in-person interactions combined with up to four virtual interactions with members of the multidisciplinary team. From the CF team, two physicians, the nurse coordinator, and social worker (SW) attend clinic in person while the registered dietitian (RD), respiratory therapist (RT), psychologist, and QI coordinator attend clinic remotely through a Cisco WebEx telehealth platform (Cisco, San Francisco, CA). All CTM interactions occur within the patient's clinic examination room, and are synchronous and private; hybrid visit types are limited to maximum three per half-day clinic. In addition, the patients undergo spirometry, sputum culture, and blood work. The hybrid process required at least one other CTM to be physically present in the clinic space to facilitate team and ancillary staff communication and technology connection between patients and remote CTMs. A virtual clinic tracking sheet and WebEx (Health Insurance Portability and Accountability Act [HIPAA] compliant, virtual platform provided by the organization) work room were used to facilitate handoffs between team members, record patient or CTM needs/requests, and to ensure that all aspects of the coproduced visit plan were carried out.
PRECLINIC
The preclinic CF triage process has previously been reported in the journal of Telemedicine and e-Health. 5 Patients are triaged by the CF team 1 week in advance of the clinic visit. If there are concerns for COVID-19, they are directed to a COVID specialized clinic for testing before their visit in the UVA pulmonary clinic. All patients are screened for symptoms suggestive of SARS-CoV-2 at the medical center ground entry point on the day of visit, and temperature is verified.
DAY OF CLINIC
The hybrid schedule consists of one to three CF patients in-person and three to five patients through telemedicine out of six patients scheduled per half-day clinic. There are two to three examination rooms available for CF visits and two are negative pressure rooms. All in-person providers wear gowns, gloves, surgical masks, and goggles. The gowns and gloves are changed between patients, goggles are wiped down, and surgical masks are reused throughout the clinic day (Fig. 2).
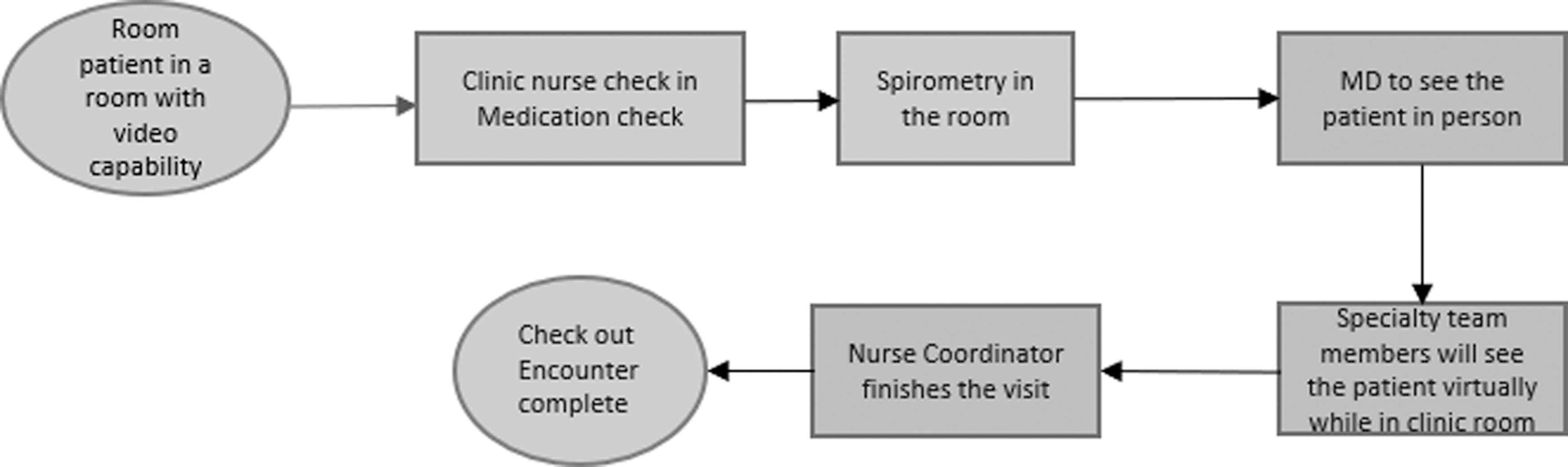
UVA CF adult hybrid clinic process map starts with patient intake in pulmonary clinic and ends with completion of patient encounter.
The team members huddle in a virtual WebEx workroom and complete a clinic flow sheet (maintained in a Google spreadsheet) with subspecialty members requests to see the patients (RT, RD, SW, registered nurse [RN] coordinator, and psychology doctor [PsyD] in addition to the medical doctor [MD]), very similar to the process created at UVA for a regular face-to-face clinic day.
The CTMs all have access to view and edit the tracking sheet simultaneously so they are aware of who else requests to see patient and are able to coordinate the order of their interactions. Every CTM records the times they enter and exit a patient encounter to provide real-time data for patient visit progress.
Upon arrival to the pulmonary clinic, each patient is escorted to a negative pressure examination room by the clinic RN. The RN obtains vital signs, provides clinical questionnaires pertinent to the visit, and reviews the CF team patient itinerary as per standard of care.
The RN notifies clinic RT staff when intake is complete and the RTs assist patients to perform spirometry in the examination room or in a dedicated PFT laboratory located adjacent to the pulmonary clinic examination rooms.
The RN coordinator and MD are informed of patient readiness for CF team after spirometry and intake is complete.
The MD sees the patient first to evaluate and discuss symptoms, spirometry, and blood monitoring. MD notifies CTMs through secure text that the MD interaction has ended and patient is available.
The physician writes the note, bills for the visit, closes the note, and communicates through epic with the nurse coordinator regarding follow-up laboratory tests and follow-up visit.
Either the SW or RN coordinator sees the patient next and performs steps pertinent to their subspecialty and then initiates a secure WebEx meeting on a computer equipped with a camera and microphone in the clinic examination room. This CTM orients the patient to the platform features and controls for remote subspecialty team member interactions, leaves the examination room, and sends secure text to the CF team to signal that the patient is connected and ready for virtual interactions.
Subsequently, other team members (RT, RD, PsyD, and QI coordinator) join the patient one at a time in the WebEx virtual room and repeat the process until all subspecialty team members on the patient itinerary have completed their interaction.
The RN coordinator sees the patient last to provide a link to review the after-visit summary, address any outstanding needs/concerns, provide a postclinic patient experience of care survey, and assist with check out and follow-up scheduling.
A sputum specimen and blood work are obtained as necessary.
MEASURES
Data are collected with each visit, in real time, in a secure health system HIPAA-compliant server. Process measures collected include the number of providers (interactions) who saw the patient remotely versus in-person, percentage encounters with coproduced shared agenda setting, percentage encounters that were multidisciplinary, percentage visits through telemedicine, percentage hybrid visits, average encounter length, and patient satisfaction.
Results
Between March 17 and June 15, 2020, the UVA multidisciplinary team had 120 encounters in the CF adult clinic out of which 16 (13%) encounters were hybrid visits (in-person with a remote component), 90 (75%) were telemedicine encounters, 5 (4%) encounters were conducted by phone visits, and 9 (8%) visits were acute illness visits with MD only (Fig. 3a). The 120 encounters allowed 105 independent patients to be seen in clinic during this period of time. Combined hybrid, telemedicine, phone, and acute patient visits provided by MD alone counted for a total of 492 multidisciplinary team interactions. Only 51 interactions were in-person (Fig. 3b). Four CTMs (RD, RT, PsyD, and QI manager) have worked exclusively remotely during this period of time and two MD providers, the SW and RN, have been present in clinic. This process reduced personal protective equipment (PPE) utilization by 90% (saved 441 gowns and gloves, and additional surgical masks and goggles).
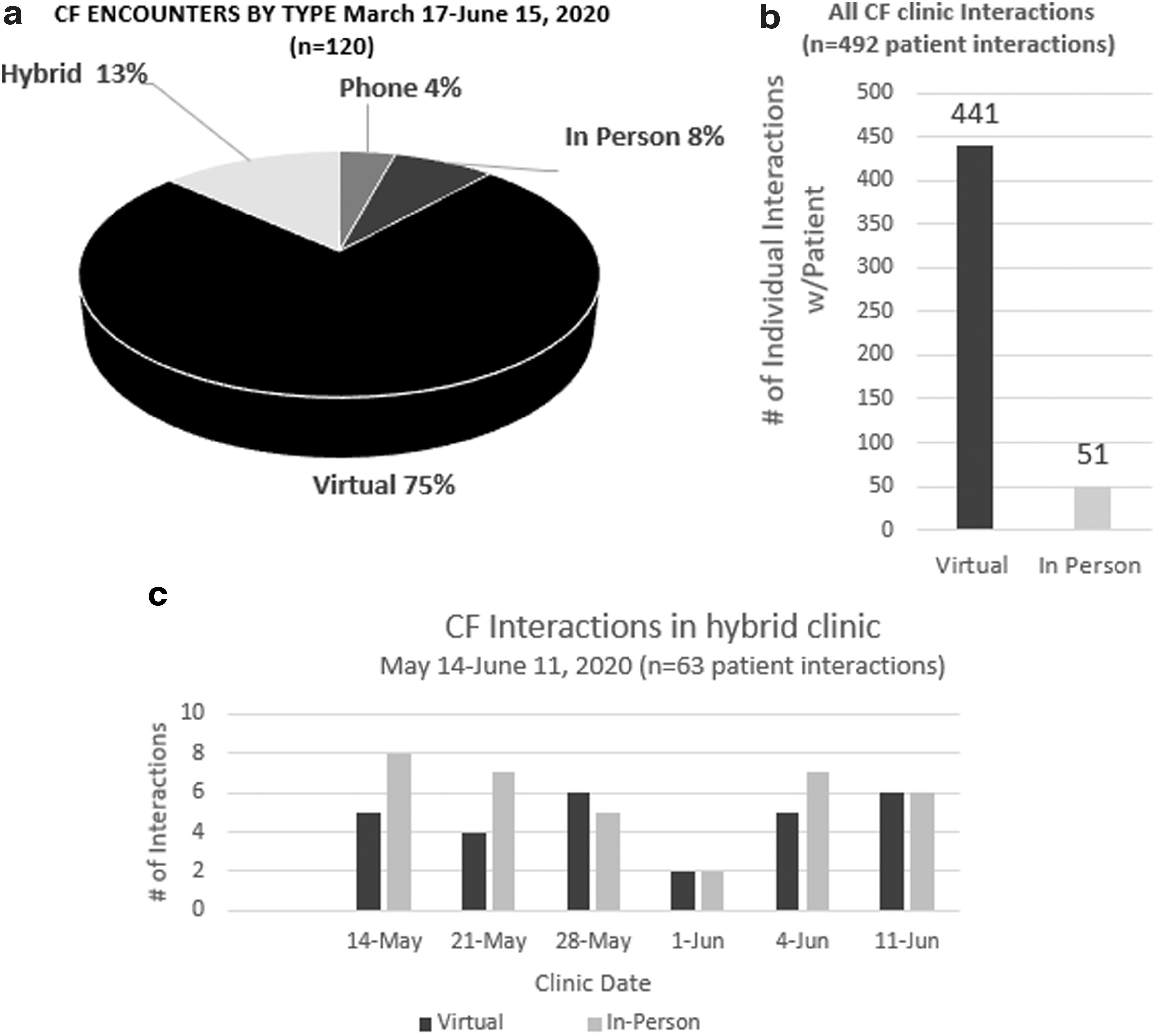
All hybrid encounters were multidisciplinary, included shared agenda setting, and fulfilled patient requests to see CTMs (Fig. 3c). (Four of five requests were honored on the same day with one requiring follow-up phone call due to team member absence.) In addition, 100% of patients who were seen for a hybrid encounter performed spirometry and obtained blood work on site and 75% had sputum cultures. Of the four patients who did not have sputum cultures, one was admitted from clinic for nonpulmonary related symptoms and one was a rapid return visit with a recent sputum culture still pending. Each hybrid visit type was attended by an average of four CTMs and amounted to 63 separate interactions. Of these interactions, 28 were completed virtually, reducing in-person contacts and PPE utilization by 44% compared with a fully in-person model of care (Fig. 3c). In addition, on any given half day of clinic, a maximum of three CF patients are seen in the hybrid clinic, out of six to seven scheduled. This allows patients to intake as soon as they arrive to clinic and minimizes patient wait time in the waiting room and potential patient–patient interactions.
Of all patients who had any component of telehealth between March and June of 2020, 81% felt they were able to get the same quality of care through telehealth as in-person (in the postclinic patient experience of care survey, 57.45% strongly agreed and 23.4% somewhat agreed to receiving same quality of care through telehealth as in-person) and 96% felt every effort was made to listen to the things that mattered most to them. The average length of hybrid encounters and telehealth encounters were similar: 97 and 102 min, respectively.
Discussion
At the beginning of the COVID-19 pandemic, while multiple organizations attempted transitioning from in-person clinics to telemedicine, the CF QI team at UVA found itself in a uniquely advantageous position due to previous expertise in QI and experience with providing telemedicine care, to design and implement rapidly a standardized process to deliver telemedicine visits. 5 Organizational pressures related to society opening in May 2020 created the need to rapidly adapt again to increase outpatient operations and face-to-face visits, so the UVA adult CF team implemented hybrid visits interspaced with telemedicine encounters in a regular clinic day (Fig. 1). The CF adult team at UVA had the training and experience necessary to undergo these process changes in a timely manner. In addition, the UVA organization provided the infrastructure, technology, and administrative support (scheduling and billing) necessary to develop this program. The CF clinic patient rooms at UVA are equipped with computers, video cameras, and microphones and high-speed internet access. The UVA CF providers receive free access to HIPAA compliant telemedicine platforms, and conditions are created for all subspecialty team members to work remotely. The multidisciplinary CTMs are provided protected time during CF adult multidisciplinary clinic to dedicate to synchronous CF visits. These factors allowed the adult CF team to innovate and adjust in the COVID-19 environment.
Understanding individual patient's social situation and personal preference as a player in the decision of participating to clinic is paramount. Patient confidence in safety and efficacy of virtual health care is very important and it is currently a limiting factor to utilizing telehealth. At UVA, 32% of CF patients initially preferred to reschedule to a future regular face-to-face visit rather than participate in virtual clinic. 5 In true coproduction of care, patient preference for telemedicine versus in-person visits needs to be respected. Having the ability to offer hybrid visits increases patient participation to clinic. As the pandemic progressed and telemedicine became standard of care for multiple specialties and disciplines, patients became more willing to participate in telemedicine visits. In addition, the UVA postvisit patient experience surveys results showed that the majority of patients seen through telemedicine felt that they received the same quality of care as in-person.
Any new health care delivery process needs to be implemented in a manner that would not increase social discrepancies in health care and would be equitably available to all patients. Offering hybrid visits in the CF clinic creates conditions for patients with technological barriers for telemedicine to continue to receive quarterly care while ensuring their safety. All patients seen in the hybrid clinic, independent of their socioeconomic status, performed spirometry and obtained blood work on site and most patients provided sputum samples for cultures. This process ensured monitoring according to Cystic Fibrosis Foundation (CFF) chronic care guidelines in this patient population. 2,3 The limitations of our data are a lack of absolute understanding of social circumstances related to the missing visits for the remaining 12% of our patient population.
We consider our current process of combined telemedicine and hybrid visits for CF care successful since we were able to see a total of 105 patients (88%) in quarterly follow-up in the context of COVID-19 pandemic, while the national average for quarterly adult visits in the pre-COVID era was ∼60%. 1
Across the country, ∼600 health care workers have died and thousands developed COVID-19 in the past several months. 7 In addition, multiple health care systems suffered tremendous financial losses due to decreased clinical operations in the context of social distancing. 8,9 Continuing to provide regular routine monitoring in the adult CF clinic maintained the necessary revenue to sustain clinical operations. At the same time, creating conditions for health care staff to work remotely maintained the CF adult team members employment during critical times when other teams and specialties were furloughed, redeployed, or even unemployed. 10 Also, providing team members with remote access to telehealth protected them from unnecessary interactions with potential SARS-CoV-2 patients and reduced the spread of the virus while ensuring staff safety. Staff safety is particularly important when health care workers are also vulnerable to increased morbidity and mortality from SARS-CoV-19, due to underlying chronic disease, pregnancy, or immunodeficiency. 11,12 Furthermore, decreasing PPE utilization contributed to the organizational goal to preserve scarce resources and decrease cost.
Having a limited number of patients and staff present in clinic at a certain time minimized patient–patient, patient–staff, and staff–staff interaction. Most health care systems have a limited number or patient rooms and staff work rooms. At UVA adult pulmonary clinic with current CF clinic system, all patients' intake happens immediately after patient arrival, minimizing patient–patient interactions. Providers also have the ability to maintain 1.82 meters distance to minimize provider–provider interactions. The remote visit component reduces patient–staff interactions by 50%.
It is difficult to estimate for the near future how many clinic visits will be conducted through telemedicine versus hybrid versus in-person only. However, having a standardized health care process in place for all these types of visits allows the CF adult multidisciplinary team to flex from one form of health care delivery to another as circumstances warrant (Fig. 4), while continuing to deliver care on a regular quarterly basis independent of the pandemic evolution and societal pressures. Through a standardized combined telemedicine and in-person clinic, chronic disease patients may continue to receive regular health monitoring during the COVID-19 era.
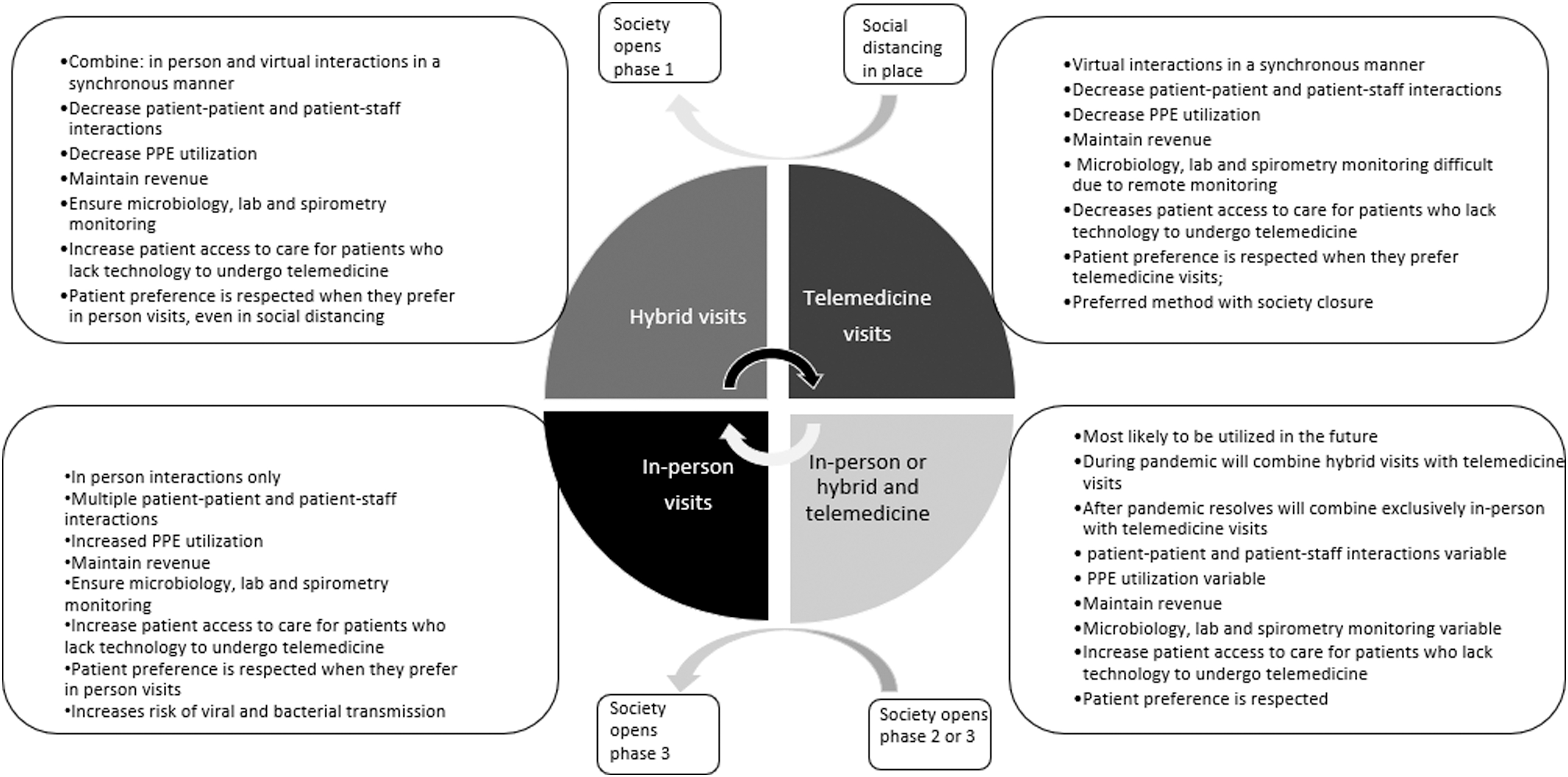
Types of multidisciplinary visits. The diagram shows the process of rapid changes from one type of multidisciplinary CF visit to another depending on societal pressures in the context of COVID-19 and differences and similarities between different models of care. COVID-19, coronavirus disease 2019.
Conclusions
The hybrid CF multidisciplinary model of telehealth enables reliable access to health care while taking under consideration patient preference and technological capabilities and enables access to clinical and biological data to support medical decisions while minimizing person-to-person contacts for patients and staff and PPE utilization.
A standardized health care delivery process that allows rapid changes from in-person to telemedicine visits and from telemedicine to in-person clinics or hybrid clinics will provide revenue for health care systems and decrease economic hardship for staff independent of future changes in society and potential reinstitution of social distancing while creating conditions for patients to continue to receive routine multidisciplinary coproduced care.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
We have received grant support from Cystic Fibrosis Foundation (CFF) (Grant No. 000447CC319).