
Abstract
Introduction:
The prognosis of phenylketonuria (PKU) in terms of neurocognitive outcome is directly related to lifelong phenylalanine (Phe) levels and adherence to treatment. Monitoring and treatment of PKU patients can be complicated in challenging circumstances as pandemics. This study aims to evaluate the impact of telemedicine for monitoring and treatment of PKU patients on metabolic outcome during coronavirus disease-19 (COVID-19) outbreak.
Materials and Methods:
Patients who were diagnosed as PKU and treated with low Phe diet, tetrahydrobiopterin (BH4), or BH4 adjunct with low Phe diet were enrolled. Study period was divided into two periods: prepandemic period wherein patients were followed up in outpatients' clinic and during pandemic wherein telemedicine was used. Demographic findings, laboratory results, and therapy responses were reviewed retrospectively and compared between the two periods. All procedures were in accordance with the ethical standards of the local ethical committee of Cerrahpasa Medical Faculty (17/11/2020-151640) and with the Helsinki Declaration of 1975, as revised in 2013.
Results:
Ninety-three (n = 93) patients were enrolled to this study. The ratio of the samples with Phe levels in the recommended ranges was found to be statistically higher during the pandemic wherein an online monitoring system was used in all treatment modalities (p< 0.05). The decrease in Phe washout frequency was statistically significant during the pandemic in the low Phe diet group (p < 0.05). Considering the relationship between Phe tolerance before and during the pandemic, a significant increase in Phe tolerance was noted during the pandemic in the low Phe diet group (p< 0.05).
Conclusions:
Telemedicine can be an appropriate and effective monitoring option for PKU patients during the COVID-19 pandemic.
Introduction
Phenylketonuria (PKU) is an autosomal recessively inherited metabolic disorder caused by defective enzyme activity of phenylalanine hydroxylase (PAH). The impaired enzyme activity results in disrupted conversion of phenylalanine (Phe) to tyrosine and causes accumulation of Phe in plasma and cerebrospinal fluid. 1 Neurocognitive impairment and psychological disturbances are the main clinical characteristics of untreated PKU. As early diagnosis and initiation of therapy play a crucial role in preventing intellectual disability, PKU became one of the most prominent disorders that benefits from newborn screening (NBS). 2 To date, different classification schemes have been used to identify clinical severity of PKU depending on blood Phe levels. Although there is still not a consensus regarding PKU classification, patients with a blood Phe level >120 μmol/L are described as hyperphenylalaninemia and can be classified as either not requiring treatment or requiring diet and/or tetrahydrobiopterin (BH4). 3,4 Dietary PHE restriction still remains the main treatment strategy; however, BH4 (alone or with low Phe diet) and phenylalanine ammonia lyase enzyme therapy are other treatment options. Regardless of the modality of treatment, maintaining the blood Phe levels in targeted ranges is the goal of therapy and can prevent neurocognitive impairment. 5
The coronavirus disease-19 (COVID-19), caused by SARS-CoV-2, was announced as a pandemic worldwide by the World Health Organization (WHO) in March 2020. According to the WHO, COVID-19 database, 47,930,397 confirmed cases, including 1,221,781 deaths, were reported till November 2020. 6 In Turkey, the first COVID-19 case was reported on March 11, 2020, and pandemic measures were implemented as in all over the world. As a consequence of the restrictions and reorganization of the health care system, patients with chronic diseases had to face major challenges. Inborn errors of metabolism (IEM) are rare, chronic, and generally progressive multisystem disorders that require multidisciplinary and close approach for diagnosis, management, and follow-up. Partly due to the high prevalence of consanguinity marriages, IEM are more frequent and a great health issue in Turkey. Literature concerning impact of COVID-19 on patients with IEM mainly included patients with lysosomal storage disorders (LSDs). 7 –9 However, only limited data are available about the problems experienced and their solutions in the follow-up of other IEM in the COVID-19 period. 10 –12
PKU is the most frequent IEM in Turkey with a prevalence of 1:4,200. 13 Treatment and follow-up of PKU is lifelong and should be managed in specialized centers to prevent neurocognitive disability. Both blood Phe monitorization and assessment of nutritional treatment according to blood Phe levels require frequent outpatient clinic admission. 3,4 Dietary adherence and management of both patients and their caregivers are complex; thus, treatment incompatibility and loss of follow-up are common problems especially in late diagnosed and/or adult patients. 14,15 In addition, during the pandemic, most of the hospitals were designed for serving to COVID-19 patients, which led to diminution in both number of the outpatient clinics and the number of patients admitted. Also patients and their families tried to avoid the hospitals due to the real risk or fear and anxiety of contagion. These changes in the standard health care system caused a major difficulty in PKU patients who need close monitoring and personalized treatment both before and during the COVID-19 pandemic. To date, any study that specifically evaluates the impact of the COVID-19 pandemic on metabolic control and treatment adherence of PKU patients has not been reported.
As our university hospital was also selected as a pandemic hospital and regular outpatient's clinic services were interrupted, we created an online communication platform for the follow-up of the PKU patients during the COVID-19 pandemic. In this study, we aimed to evaluate the impact of this online and personalized follow-up system on the metabolic outcome of PKU patients.
Materials and Methods
This retrospective study was conducted between November 2019 and June 2020 with PKU patients in Istanbul University-Cerrahpasa, Cerrahpasa Medical Faculty, Pediatric Nutrition and Metabolic Department. Patients who were diagnosed as PKU and treated with low Phe diet, BH4, or BH4 adjunct with low Phe diet were included if
PKU was diagnosed by NBS,
patient and family education was given concerning the issues of taking blood samples at home for dried blood spot (DBS) analysis, Phe, and protein contents of foods, main principles of low Phe diet, sick day diet, and avoiding of medication/nutrition consisting of aspartame and bovin gelatin, and
patients were under regular follow-up and DBS sampling was obtained appropriate with age recommended frequency (Table 1). 3
Recommended Target Phenylalanine Levels and Frequency of Blood Phenylalanine Measurement for the Follow-Up of Phenylketonuria Patients 3
Phe, phenylalanine.
Patients who were not under regular follow-up, with missing data, and receiving unrestricted breastfeeding due to the difficulty of accurate Phe content calculation were excluded from the study.
As our hospital became a pandemic hospital according to government's COVID-19 measures, the study period was divided into two periods: period 1 (prepandemic): from November 2019 to March 2020; period 2 (during pandemic): from March 2020 to June 2020. In the prepandemic period, the parents of the patients were visiting the outpatient clinic at 08:00 a.m. for DBS sampling. After blood Phe levels were determined by the laboratory at nearly 14:00 p.m., the results were evaluated along with a detailed food record of the patient given by the parents. Dietary or drug dosage modifications were made according to the Phe level, patient's body weight, and food records. During the COVID-19 pandemic, an online communication platform was created and patients were requested to join this telemedicine system.
DETAILS OF THE TELEMEDICINE INTERVENTION
With the beginning of COVID-19 restrictions, caregivers of the patients who were diagnosed with PKU were reached by phone calls and they were informed that their monitoring is now planned to be continued on an online follow-up platform. In these phone calls, an online face-to-face meeting was scheduled through WhatsApp, Facetime, Skype, or Zoom according to their preferences. Caregivers were requested to get an e-mail account if they did not already have one until this online meeting schedule.
At the time of the online face-to-face meeting, “ctf.metabolizma@gmail.com” was given as the main address of telemedicine intervention. Caregivers were requested to send an e-mail to this address from their e-mail accounts and checked whether there was any problem at that moment. During the meeting, several examples including getting a screen shot, writing an e-mail, and attaching a file were practiced and the questions of the caregivers were responded to. A phone number was given, with which they could get support at any time in case they had a problem with the telemedicine process. All patients and/or caregivers who were included in the study were educated concerning the issues of taking blood samples at home for DBS analysis, timing of taking the samples, and main principles of low Phe diet at the time of diagnosis. However, all these issues were discussed again and the problems were reviewed in the meeting. After obtaining family consent for the continuation of the follow-up with the telemedicine platform, the details of the process were determined as follows.
DBS samples were taken at home at 08.00 a.m. and delivered to the same laboratory of our hospital by one of their family members for blood Phe analysis.
Results of the blood Phe analysis were tracked online and the results were learned on the same day from the online results address of the laboratory belonging to the hospital.
A detailed e-mail including the information of current body weight of the patient, the most recent low Phe diet, and/or BH4 treatment they have received, detailed food record of the past 2 days, and the screen shot of the blood Phe analysis was sent to “ctf.metabolizma@gmail.com” by the caregivers from their personal accounts.
After evaluating each e-mail, dietary or drug dosage modifications were made according to the Phe level, patient's body weight, and food records and posted as a reply to each patient. In these reply mails, questions of the patients and caregivers regarding medication and diet were also answered. The patients were informed about their next blood sampling dates.
In conclusion, the whole process already mentioned except the collection and delivery of the DBS samples was executed by using this online platform. There were no changes in the principles of follow-up including implementation of low Phe diet, targeted blood Phe levels, and recommended DBS sampling frequency between the two periods.
In this study, clinical and biochemical features of the patients were reviewed in detail and the following items were recorded for both periods: age at the time of diagnosis and pandemic (in months), gender, educational level of patients' caregivers in pediatric cases and patients in adult cases, blood Phe levels, prescribed low Phe diets, detailed dietary recalls, and dose of BH4 treatment. Phe tolerance was calculated for each DBS sampling by using the 25 mg Phe exchange system. Frequency of DBS sampling, mean blood Phe levels, frequency of Phe washout (administration of only normocaloric Phe-free formulas in the diet until normalization of blood Phe), and percentage of achieving of good metabolic control according to the targeted ranges of Phe in the PKU guideline were compared between the two periods.
All procedures followed were in accordance with the ethical standards of the local ethical committee of Cerrahpasa Medical Faculty (17/11/2020-151640) and with the Helsinki Declaration of 1975, as revised in 2013. All parents of the patients included in this study gave informed consent.
STATISTICAL ANALYSIS
Statistical analyses were performed using Statistical Package for Social Sciences version 26.0 (SPSS, Inc., Chicago, IL, USA) and R programming language. The mean, standard deviation (SD), frequency, and ratio values were used as descriptive statistics. Qualitative variables were examined by using the chi-square test and one-way analysis of variance (ANOVA) test. The one-way ANOVA test was used to investigate the variations in more than three groups if the related variable was normal. Normal distribution of data was evaluated with a Kolmogorov–Smirnov test. If the significance obtained from Kolmogorov–Smirnov test related to each variable is more than 0.05, the related variable is considered to be normally distributed. Categorical variables are expressed as numbers and percentages. Continuous variables are expressed as mean ± SD. A value of p < 0.05 was considered statistically significant. For longitudinal data analysis, we performed the linear mixed-effect modelling using R software, nlme package at the level of 0.05 is considered.
Results
During the study period, data of 116 PKU patients were evaluated, 23 patients were excluded from the study due to different reasons, and a total of 93 PKU patients were enrolled to this study (Fig. 1). Forty-one patients (44%) were female and 52 patients (55.9%) were male. Patients were divided into three subgroups according to the treatment modality: 38 (40.8%) patients were receiving BH4 treatment, 39 (41.9%) patients were receiving low Phe diet, 16 (19.3%) patients were receiving both BH4 and low Phe diet. Table 2 gives the demographic data of the patients belonging to each subgroup.
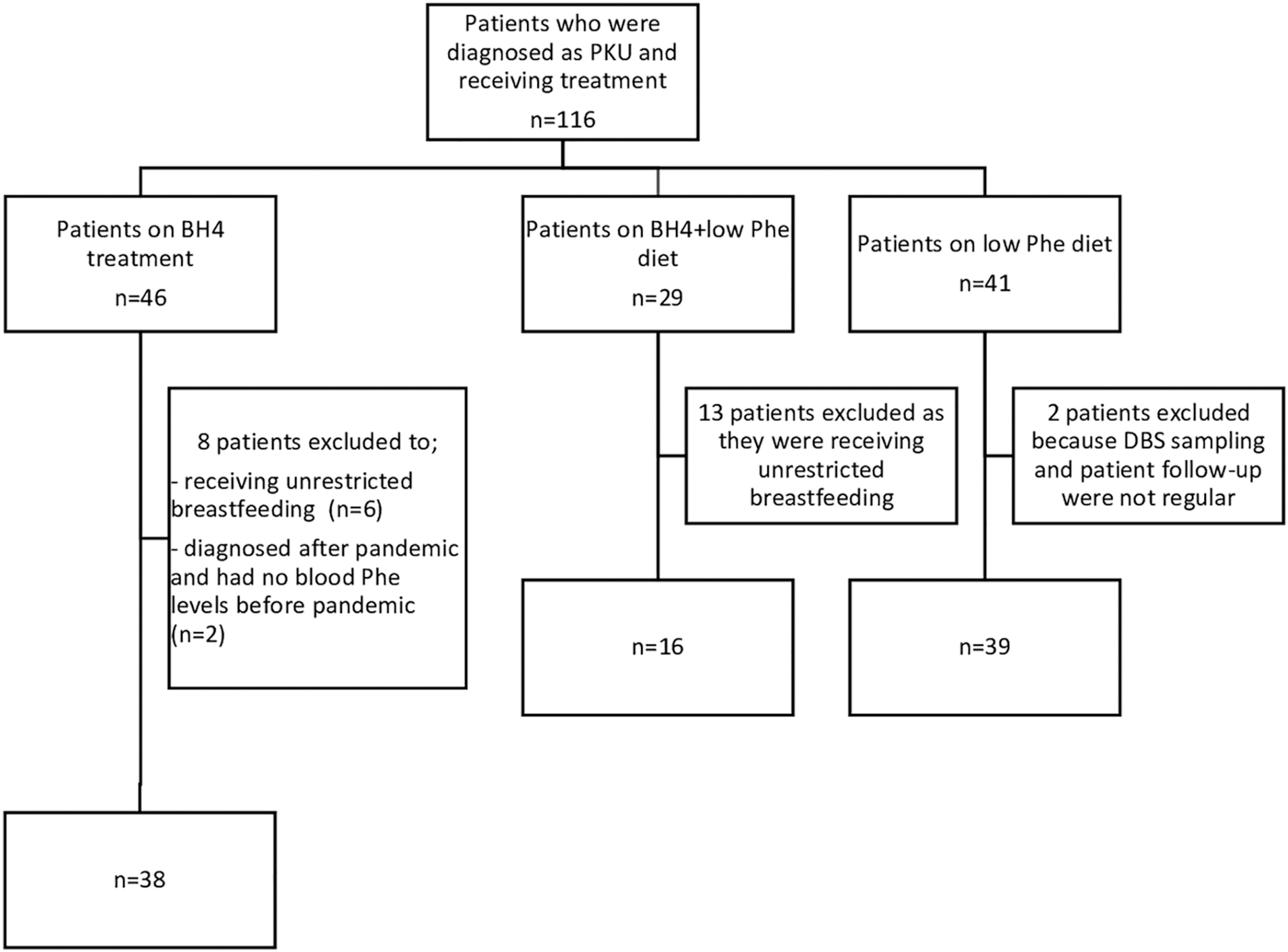
Flow chart of inclusion and exclusion criteria of the study.
Demographic Data of the Phenylketonuria Patients According to the Treatment Modalities
BH4, tetrahydrobiopterin.
Data concerning the frequency of DBS sampling, mean blood Phe levels, and proportion of the samples with Phe levels over the recommended targets were compared between period 1 and period 2. Regarding the frequency of DBS sampling, the mean number of samplings was 7.52 ± 2.52, 7.76 ± 4.34, and 9.8 ± 3.1 in subgroups of BH4 treatment, low Phe diet, and BH4 adjunct with low Phe diet, respectively, in the prepandemic period. During the pandemic, number of DBS sampling was 4.63 ± 3.88 in the BH4 group, 6.05 ± 4.6 in the low Phe diet group, and 5.93 ± 3.21 in the BH4 adjunct with low Phe diet group. A statistically significant diminution was noted in the frequency of sampling in all groups during the pandemic (p < 0.05). However, considering the ratio of the samples with Phe levels to the recommended targets, it was seen that a better metabolic control can be achieved by using the online monitoring system during the pandemic. In the BH4 group, in the prepandemic period, blood Phe levels in 230 of 286 samples (80.5%) were within the target range for this age, whereas in 56 samples (19.5%), blood Phe levels were above the recommended ranges. During the pandemic, in only 9 of 176 samples (5%) blood Phe levels were above the recommended ranges, whereas in 167 samples (95%) blood Phe levels were in targeted ranges. In patients under low Phe diet, in the prepandemic period, blood Phe levels in 187 of 295 samples (56%) were within the target ranges for this age, whereas in 108 samples (36%) blood Phe levels were above the recommended ranges. During the pandemic, in 81 of 230 samples (35%) blood Phe levels were above the recommended ranges, whereas in 149 samples (65%) blood Phe levels were in targeted ranges. In patients who were receiving both BH4 and low Phe diet, in the prepandemic period, blood Phe levels were within the target ranges for this age in 125 of 157 samples (80%), whereas in 32 samples (20%) blood Phe levels were above the recommended ranges. During the pandemic, in 16 of 95 samples (8%) blood Phe levels were above the recommended ranges, whereas in 79 samples (92%) blood Phe levels were in targeted ranges. In brief, the ratio of the samples with Phe levels in the recommended ranges was found to be statistically higher during the pandemic where an online monitoring system was used for the follow-up in all three groups (p < 0.05).
In addition to these data, frequency of Phe washout and Phe tolerances were calculated for both periods in patients for whom a low Phe diet was a component of the treatment. In patients on low Phe diet, the mean number of Phe washouts was 1.5 ± 1.5 in the prepandemic period and was 0.5 ± 0.8 during the pandemic. However, in patients who were on both BH4 and low Phe diet, mean number of Phe washouts was 0.68 ± 1.25 in the prepandemic period and was 0.37 ± 0.62 during the pandemic. The decrease in Phe washout frequency was statistically significant during the pandemic in the low Phe diet group (p < 0.05), whereas no statistical difference was observed between the two periods in the BH4 adjunct with low Phe diet group (p = 0.3). Considering the relationship between Phe tolerance before and during the pandemic, a significant increase in Phe tolerance was noted during the pandemic in the low Phe diet group (p < 0.05), whereas the periods had no significant effect on Phe tolerance in the BH4 adjunct with low Phe diet group (p = 0.06). Table 3 gives the statistical analysis of the data concerning the mean frequency of DBS sampling, proportion of samples with blood Phe levels above the recommended ranges, and frequency of Phe washout between treatment modalities in the two periods. In Table 4, a linear mixed effects model evaluating the impact of the two periods—before and during the pandemic—on Phe tolerance in patients on low Phe diet and on BH4 adjunct with low Phe diet is given.
Wilcoxon Test Comparing the Mean Frequency of Dried Blood Spot Sampling, Proportion of Samples with Blood Phenylalanine Levels Above the Recommended Ranges, and Frequency of Phenylalanine Washout Between Treatment Modalities Before and After the Pandemic
DBS, dried blood spot; SD, standard deviation.
Linear Mixed Effects Model Evaluating the Impact of Two Periods—Before and After the Pandemic—on Phenylalanine Tolerance in Patients on Low Phenylalanine Diet and on Tetrahydrobiopterin Adjunct with Low Phenylalanine Diet
When the impact of education level of the caregivers on the frequency of DBS sampling, Phe washout, and proportion of samples with Phe level above the recommended ranges was examined, statistically significant differences were observed only in certain groups. Education level was significantly effective in the low Phe diet group in terms of frequency of DBS sampling and it was observed that patients whose caregivers graduated from college or university had more frequent DBS sampling in this group (p < 0.05). Among patients who were on a low Phe diet, those whose caregivers graduated from primary school had more frequent Phe washouts (p < 0.05). Education level of the caregivers had no significant effect on proportion of samples with Phe level above the recommended ranges in any of the groups. Table 5 gives the statistical relationship between education level of the caregivers and frequency of DBS sampling, frequency of Phe washout proportion of samples with blood Phe levels above the recommended ranges, respectively, in all treatment modalities.
Wilcoxon and One-Way Analysis of Variance Tests Evaluating the Impact of Education Level of the Parents on Frequency of Dried Blood Spot Sampling, Proportion of Samples with Blood Phenylalanine Above the Recommended Ranges, and Frequency of Phenylalanine Washout Between Treatment Modalities
One-way ANOVA.
ANOVA, analysis of variance.
Discussion
This study describes a telemedicine experience in the follow-up of patients with PKU during the COVID-19 pandemic. In our study, the ratio of the samples with Phe levels within the recommended ranges was found to be statistically higher in all groups during the pandemic in which the online monitoring system was used for follow-up in PKU patients. In addition, frequency of the Phe washout significantly decreased and a significant increase was noted in Phe tolerance in patients under low Phe diet during the pandemic. According to these results, it has been suggested that an online and personalized monitoring system can be effective in achieving metabolic control of PKU patients during the COVID-19 pandemic.
Telemedicine can be simply described as the use of information and communication technologies to provide continuity of health care services. It has been preferred by both clinicians and patients especially for the follow-up of chronic diseases and for patients living in rural areas or long distance from hospital. Besides the advantages of being low cost, widely available, and improving the adherence to treatment, lack of an optimal standardization for a complete examination and issues of patient privacy should be concerned carefully. 16 Telemedicine experience in IEM mainly includes dietary applications and precision medicine according to clinical and biochemical parameters of the patients. 17,18 During the COVID-19 pandemic, global measures were taken to control the spread of coronavirus. Health care services have also faced major challenges, and a digital transformation has taken place in many disease groups for patient monitoring and management. 16,19 Impact of COVID-19 on patients with IEM who require multidisciplinary and close approach for diagnosis, management and follow-up were reported limitedly in the medical literature. The main issues emphasized in the literature were the interruption of enzyme replacement therapy infusions in hospitals, modification of the treatments to home therapy, and the behavioral and emotional changes of LSD patients during the pandemic. 7 –9 In terms of other IEM, main topics mentioned in the literature were the number of newly diagnosed patients, number of emergency unit or outpatients' clinic admissions, factors affecting the frequency of admission, the level of awareness of the patients about pandemic, and questionnaire studies about the difficulties they experienced. Telemedicine platforms consisting of phone calls and online communication were recommended to ensure the continuity of follow-up and treatment of IEM patients. 10 –12 However, neither the clinical and biochemical findings of PKU patients during the COVID-19 pandemic nor the use of telemedicine to evaluate the metabolic control and treatment adherence was reported in the literature to date.
As in other chronic diseases, the necessity of lifelong follow-up and management to ensure a good metabolic outcome in PKU patients brings many challenges. Frequent outpatient visits for diet maintenance, biochemical controls, and dietary evaluations make PKU difficult to manage for both patients and parents, resulting in loss of follow-up, especially in adult patients. Berry et al. estimated the ratio of PKU patients who discontinued the follow-up as 52% (7,808 of 14,988 patients) according to an incidence model based on clinical records. Although 19% of the patients who were lost to follow-up were between the ages of 0 and 4 years, this rate was 77% in patients between the ages of 25 and 45 years. The results showed a progressive increase in noncompliance with treatment and follow-up with age. 20 In another study, an online survey was conducted in 44 PKU clinics in the United States and it was estimated that 32% of all PKU patients (1,758 of 5,530 patients) were lost to follow-up. 21 Various factors that affect compliance with the follow-up and treatment of PKU patients have been identified to date. According to the literature, issues about the health care system, socioeconomic factors, education level of the patient and the parents, patient's neurocognitive impairment that complicates the treatment adherence, and complexity of the treatment regimens can be listed among the factors that make the compliance difficult. 20 Living at a distance from the metabolism clinic, difficulty in using public transportation systems, and not being able to get time off work have also been cited as challenging factors. 22 In studies on new strategies to increase the compliance of PKU patients, telemedicine was reported as one of the most beneficial approaches followed by educational events, satellite clinics, and adult clinic days/hours. 14
In our study, transition to a telemedicine platform resulted with a better metabolic outcome after the announcement of the COVID-19 pandemic. Data of the parameters indicating the metabolic control in PKU were compared between the two periods (prepandemic and during pandemic) in the same patients. Despite the challenging conditions of the pandemic, the rate of samples with Phe levels within the recommended ranges was found to be statistically higher, and in patients who were receiving low Phe diet, a decrease in the frequency of the Phe washout and a significant increase in Phe tolerance were observed. As no change was made regarding the treatment regimen or PKU follow-up principles, we think that improvement of the metabolic control in PKU during the pandemic was due to the telemedicine application. We believe that the main reason for this fact is related to the effect of telemedicine in facilitating the patients' life. Before the pandemic, DBS samplings were taken at 08:00 a.m. and patients had to wait until 14:00 p.m. for dietary and medical adjustments according to blood Phe levels. Difficulty in using public transportation systems and not being able to get time off work for the caregivers were challenging in PKU follow-up before the pandemic. In addition, although the fathers of the patients generally accompanied the patients in the outpatient clinic, the primary caregivers of most of the patients were their mothers. This situation caused problems in getting correct food records, evaluating the dietary compliance of the patients, and recognizing the difficulties experienced by the patient. The time spent by the patients and their caregivers in the hospital was shortened by transition of telemedicine. In addition, an online and personalized system has been achieved wherein patients' needs and dietary compliance problems can be better evaluated with telemedicine.
Conclusions
The main goal of treatment in PKU patients is to reach the appropriate intellectual and mental competence according to their age. The prognosis of PKU in terms of neurocognitive outcome is directly related to lifelong Phe levels and adherence to treatment. Telemedicine platforms can be effective to overcome the challenging circumstances in management of monitoring and treatment of PKU patients during pandemics. In addition, it can facilitate adaptation process and compliance of patients and families to treatment and follow-up in PKU after the pandemic. In conclusion, we strongly believe that telemedicine is an appropriate and effective monitoring option for PKU patients that can be used not only during pandemics but also during chronic follow-up after the pandemic.
Footnotes
Authors' Contributions
T.Z. serves as the guarantor for the article. She accepts full responsibility for the study, had access to the data, and controlled the decision to publish. She has been involved in conception, design, analysis, and interpretation of the data and also drafting the article. D.H., E.U., S.A., and E.O.-E. have been involved in conception, design, analysis, and interpretation of the data. E.I., M.S.C., and E.K. have been involved in analysis and interpretation of the data. C.A.-Z. has been involved in conception, design, and interpretation of the data and revising the article critically for important intellectual content. All the coauthors listed gave their final approval of this article version and agreed to conditions noted on the Authorship Agreement Form.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.