
Abstract
Introduction:
Wearable devices, including smart wristbands and watches, are often used with e-health applications (apps). The users' characteristics of wrist wearable devices currently lack description, and the cardiovascular disease (CVD) high-risk rate of users remains unknown.
Purpose:
This study aimed to (1) describe the basic characteristics and habits of users of the “Amazfit Health” app and Huami wrist wearable devices and (2) analyze the proportion and define the population characteristics of users with a high risk of developing CVD.
Subjects and Methods:
This study included users >18 years of age, residing in mainland China, using the “Amazfit Health” app and Huami wearable devices. Devices data and users' self-reported information were collected in the app. The risk stratification was based on WHO/ISH cardiovascular risk prediction charts for the Western Pacific Region. Subjects with CVD history, total cholesterol ≥8 mmol/L, or ≥10% predicted CVD risk and those with <10% predicted CVD risk were considered to be at high and low risk of developing CVD, respectively.
Results:
Data were obtained from 80,098 (total users) and 10,866 users (subjects) for risk stratification. The age of the total users and subjects were 45.6 ± 15.4 and 50.7 ± 14.0 years, respectively. The number of male and female users was 50,024, and 30,074 in total users, and 7,284, and 3,582 in subjects, respectively. The body mass index of total users and subjects was 24.0 ± 4.6 kg/m2 and 24.6 ± 3.8 kg/m2, respectively. By classifying users' residences into first-tier cities, municipalities and provincial capitals, and other areas, the numbers of total users were 20,179, 28,213, and 31,137, and subjects were 2,587, 3,966, and 4,269, respectively. The number of subjects with high CVD risk was 1,161, accounting for 10.7% of all subjects.
Conclusions:
Users with high CVD risk only accounted for a small proportion of the population of wearable devices users.
Introduction
Wrist wearable devices, including smart wristbands and smartwatches, are currently being utilized by many people who are conscious of their health. Wearable devices can record exercise, photoplethysmographic (PPG), electrocardiogram (ECG), and other data over a long time. There have been some large-scale clinical studies evaluating the role of wrist wearable devices in screening for arrhythmias. 1,2 However, the characteristics of wrist wearable device users currently lack description and are still changing rapidly. We speculate that most of the users of the devices are relatively healthy young people. The risk stratification of users of wrist wearable devices and screening them for high risk of cardiovascular disease (CVD) may help focus attention on and establish interventions for such people.
There are several tools available for 10-year risk stratification of CVD, including Framingham Risk Scores (FRS), 3 Pooled Cohort atherosclerotic cardiovascular disease Risk Equations (PCE), 4 Systematic COronary Risk Evaluation (SCORE) system, 5 WHO/ISH cardiovascular risk prediction charts for the Western Pacific Region, 6 and China-PAR model. 7 The last two models are suitable for the mainland Chinese population. Both China-PAR and FRS-stratified models require several laboratory results, and these results are usually difficult to obtain from the general population, especially in areas with insufficient medical resources. Since the WHO/ISH stratified model is easy to use and does not require laboratory results, it is more suitable for risk assessment in such situations.
The use of wrist wearable devices and corresponding application (app) provides a good platform to conduct various evaluations for this group of people. Therefore, we aimed to use the WHO/ISH cardiovascular risk prediction charts to understand the feasibility of using wrist wearable devices and corresponding app for risk assessment and the CVD risk characteristics of users of these devices.
Smartphone Application
The “Amazfit Health” app (Huami [Beijing] Information Technology Co. Ltd., Beijing, China) is a e-health smartphone app for Huami wearable device users (screenshots of “Amazfit Health” app are shown in Supplementary Material S1). The devices that can be connected to the app include smartwatches, smart wristbands, smart scales, and Bluetooth sphygmomanometers. The connected device can automatically transmit data to this app. The user can also self-report the past medical history, blood cholesterol level, and other health information in the app. For these self-reported data, the upper and lower limits are set in the app to prevent unrealistic data from being incorrectly reported.
All four models of wrist wearable devices in this study were capable of both PPG and ECG recording. The atrial fibrillation-recognizing artificial intelligence algorithms of PPG and ECG have been verified under specific circumstances in a previous study. 8 The users can send their ECG recordings through the internet to a doctor for a diagnosis. The symptom label for the recorded ECG and the health information stored in the server can be used as additional information for remote ECG diagnosis.
Study Objective
The objectives of this study were to (1) describe the basic characteristics and usage habits of the users of the “Amazfit Health” app wearing Huami wrist wearable devices and (2) analyze the proportion of users who were at high risk of CVD or had CVD, and evaluate the population characteristics of users with high CVD risk.
Subjects and Methods
Study Population
All data included for analysis were collected from the users residing in mainland China before July 31, 2020; all users included were ≥18 years of age and using the “Amazfit Health” app and the following Huami wearable devices: Amazfit Health Band, Amazfit Health Band 1S, Amazfit Health Band (Huangshan No. 1), and Amazfit Health Watch. The users' wristbands or watches were personally purchased, and no device was donated or borrowed for this study.
Retrieving Data
All data reported by users or transmitted automatically in the “Amazfit Health” app had been saved in an encrypted database on an online server located in China mainland. The users' data were purposely and anonymously retrieved according to the requirement of the study.
The following data were retrieved for risk stratification: age, gender, history of diabetes, history of smoking, systolic blood pressure level, and total cholesterol (TCHO) levels. In addition, to describe the population characteristics and utilization habits, the following data were collected from all users: height, weight, place of residence, monthly wearing time in the past 12 months, the monthly number of ECGs in the past 12 months, and history of CVD.
Place of residence was determined according to three categories, including “first-tier cities” (Beijing, Shanghai, Guangzhou, and Shenzhen), “other municipalities and capital cities” (Tianjin, Chongqing, Shijiazhuang, Shenyang, Harbin, Hangzhou, Fuzhou, Jinan, Wuhan, Chengdu, Kunming, Lanzhou, Nanning, Yinchuan, Taiyuan, Changchun, Nanjing, Hefei, Nanchang, Zhengzhou, Changsha, Haikou, Guiyang, Xi'an, Xining, Hohhot, Lhasa, and Urumqi), and “other cities, towns, and regions.” Although age and gender information were available for all users, the other data were incomplete for some, as they were not strictly requested in the app.
Risk Stratification of CVD
Risk stratification of CVD was based on the “Prevention of cardiovascular disease: pocket guidelines for assessment and management of cardiovascular risk: (WHO/ISH cardiovascular risk prediction charts for the Western Pacific Region).” 6 According to the guidelines, patients diagnosed with CVD or hypercholesterolemia with a TCHO level of ≥8 mmol/L should be excluded from the risk stratification analysis. As it was difficult to determine whether these criteria were met by the data obtained through the app, the users who were deemed unsuitable for this risk stratification based on other criteria were excluded from this study. Risk stratification was performed according to the method described in the guidelines. Age, gender, systolic blood pressure, history of diabetes, history of smoking, and cholesterol level (with or without) were used for risk stratification.
The WHO/ISH charts are a set of charts with different colors representing different risk stratifications, wherein the color green to crimson indicates a 10-year CVD (myocardial infarction or stroke) risk of <10% to ≥40%, respectively. Regardless of the availability of cholesterol values, different charts were used for risk stratification according to the guidelines. Users whose cholesterol values were reported as zero were regarded to have no cholesterol data.
Patients diagnosed with CVD or hypercholesterolemia with a TCHO level of ≥8 mmol/L were directly considered to be in the high-risk group. Similarly, subjects with ≥10% predicted CVD risk by the WHO/ISH risk prediction chart were considered to be in the high-risk group. Conversely, subjects with <10% predicted CVD risk, according to the WHO/ISH risk prediction chart, were considered to be in the low-risk group.
Data Analysis
The required data were directly derived from the database according to the setting's conditions. The user's age, height, weight, and body mass index (BMI) were represented by the mean and standard deviation. For all users and subjects undergoing risk stratification, basic characteristics were tested for consistency. Age, height, weight, and BMI were tested by a one-sample t-test, and age stratification, gender, and residence were tested by chi-square test. Statistical calculations were performed using SPSS25.0 software.
Since the duration of wearing and times of ECG recordings may be variedly distributed over time, we collected data for 12 months before the deadline separately. The monthly wearing time was counted by hours and days, whereas ECG times were represented by the median and the 25th and 75th percentiles. Among the subjects included for CVD risk stratification, the cholesterol level was expressed as the mean and standard deviation, and the number of subjects with CVD and diabetes was described.
Study Approval and Ethical Considerations
This study was approved by the Institutional Ethics Committee of Peking University First Hospital. Since this study is a retrospective analysis of existing data, the requirement of written informed consent was waived by the ethics committee. While registering on the “Amazfit Health” app, all users were required to read the privacy policy statement, which could be reviewed anytime on the app. Whenever the privacy policy statement was updated, a push notification was sent to inform the users. The privacy statement clearly informed that medical institutions or doctors cooperating with Anhui Huami Information Technology Co., Ltd. and its affiliates may access user-related data anonymously for medical research and analysis. This study has been registered in the China Clinical Trials Registry (chictr.org.cn, identifier: ChiCTR2000037523).
Results
As of July 31, 2020, the number of users (total users) who met the study criteria was 80,098. In the necessary data for risk stratification, age and gender data were complete in all users. The remaining information was optional for users. If any of the options, including diabetes history, smoking history, or systolic blood pressure, was not actively declared, the user was excluded from the risk stratification. Of the 80,098 “total users,” 39,365 and 30,229 reported whether they had a history of diabetes and smoking, respectively, and 19,589 of them reported their systolic blood pressure. Overall, 10,866 users had complete data for risk stratification (subjects). The mean age of total users was 45.6 ± 15.4 years, and the age of subjects was 50.7 ± 14.0 years.
The users were classified into three groups as follows: youth (18–44 years), middle aged (45–64 years), and elder (≥65 years); in these three groups, the number of total users was 42,641, 26,238, and 11,219 and the number of subjects was 3,983, 4,887, and 1,996, respectively. There was a significant difference between the total users and subjects regarding age and gender, respectively. Categorizing the entire study population in terms of gender showed that there were 50,024 males and 30,074 females in total users and 7,284 males and 3,582 females in subjects. There were 80,061 individuals with complete height and weight data in total users and 10,864 in subjects.
The height, weight, and BMI of the total users were 168.3 ± 8.1 cm, 68.4 ± 13.6 kg, and 24.0 ± 4.6 kg/m2, respectively. Conversely, the height, weight, and BMI of the subjects were 168.7 ± 7.8 cm, 70.2 ± 13.7 kg, and 24.6 ± 3.8 kg/m2, respectively. After classifying user's residences into first-tier cities, municipalities and provincial capitals (excluding first-tier cities), and other areas (including minor cities and rural areas), the number of total users in these three types of areas was 20,179, 28,213, and 31,137, respectively, and subjects were 2,587, 3,966, and 4,269, respectively. Overall, 569 total users and 44 subjects were not classified by residence as their IP addresses could not be obtained. The inclusion process and the number of users with complete data are shown in Figure 1. The characteristics and statistically determined differences between subjects and total users are described in Table 1.
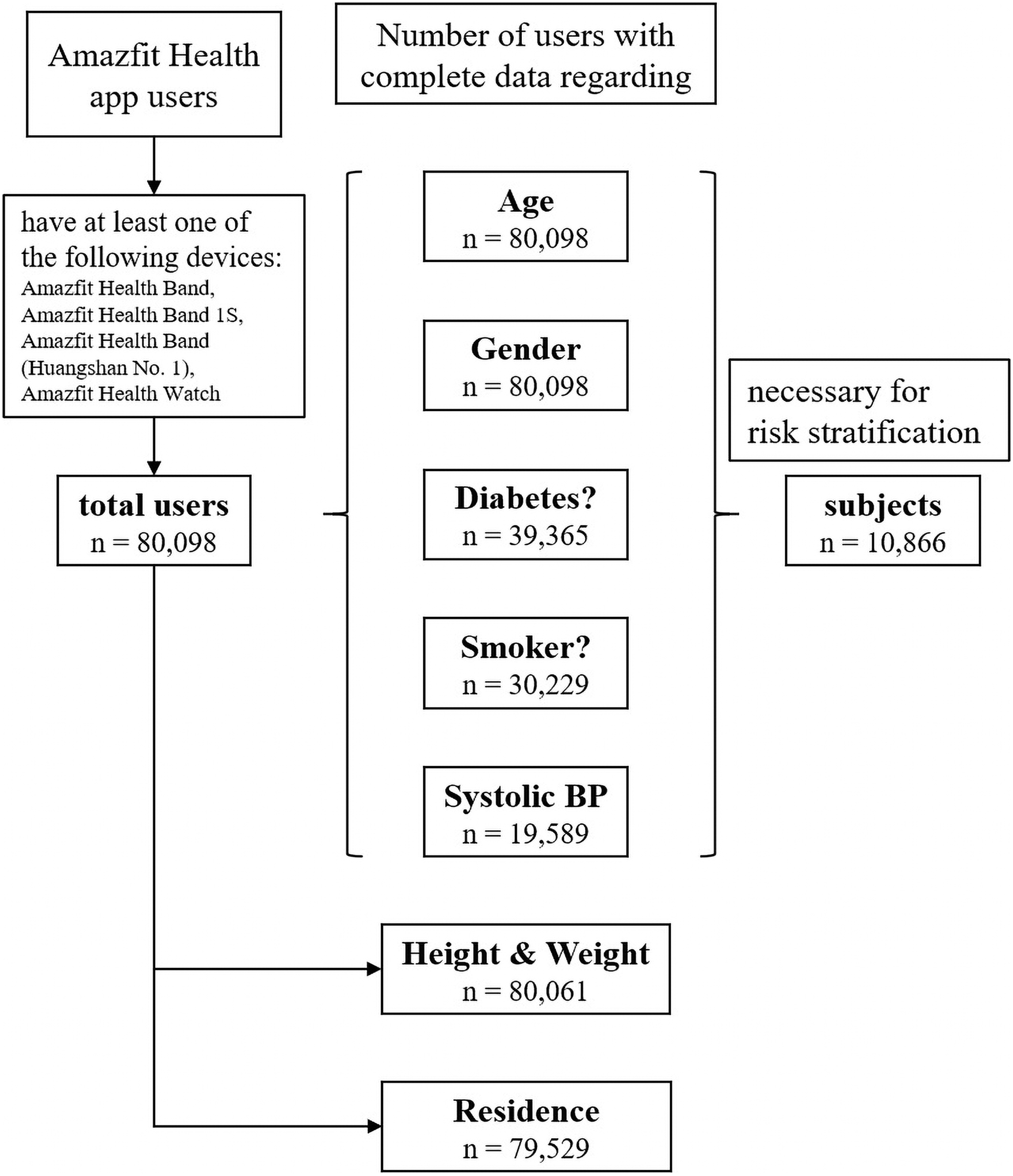
App users' inclusion process and the number of users with complete data. Age, gender, diabetes history, smoking history, and systolic blood pressure are necessary for risk stratification. App, application.
Characteristics of Total Users and Subjects
Age, height, weight, and BMI are shown in averages and standard deviations, using a single-sample t-test to compare the consistency of subjects with overall data. The remaining data are shown in a number of users (with percentages in parentheses), using the chi-square test to compare the consistency of subjects with the overall.
BMI, body mass index.
From August 2019 to July 2020, the monthly median time (in hours and days, respectively) when total users and subjects wore wristbands or watches and the median number of ECG recordings for total users and subjects are shown in Figure 2. The median and 25th and 75th percentiles of the abovementioned habit data are described in Supplementary Material S2. Since many users did not use wrist wearable devices continuously, this study only observed the habits of users who wore or used the ECG function each month. The number of users who wore or used the ECG function each month among “total users” and “subjects” is similarly described in detail in Supplementary Material S2.
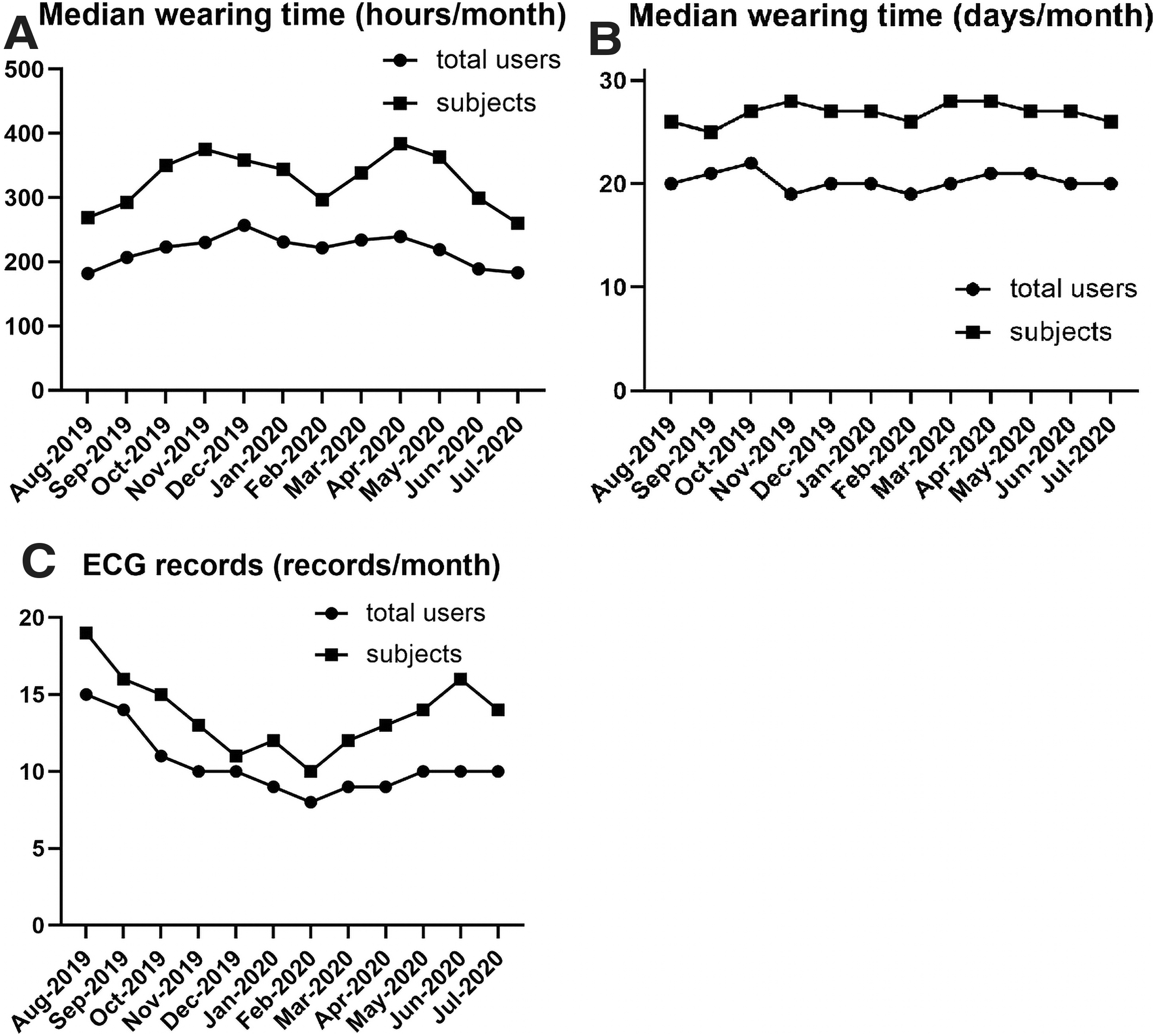
From August 2019 to July 2020, the median time for which total users and subjects wore wristbands or watches each month is shown in hours
Among the subjects, 79 had a past medical history of CVD, and 169 had a record of cholesterol value ≥8.0 mmol/L; the 246 subjects who had these two conditions were excluded from CVD risk stratification and directly counted as high-risk subjects. The numbers of excluded subjects, classified into groups according to gender, age groups, and residence, are described in Supplementary Material S3. The final CVD risk stratification subjects were 10,620 in number, of whom 2,180 had cholesterol data and 8,440 had no cholesterol data. In total, 1,152 individuals had a history of smoking, and 1,131 individuals had a history of diabetes mellitus. Among subjects with cholesterol data, the TCHO level was 4.60 ± 1.84 mmol/L, and subjects with CVD risk stratification (<8 mmol/L) had a TCHO level of 4.30 ± 1.20 mmol/L.
The results of calculated CVD risk stratification are shown in Table 2. The CVD high-risk groups, including subjects with a history of CVD, had TCHO values ≥8.0 mmol/L, and 10-year CVD risk ≥10%, totaled 1,161 and accounted for 10.7% of all subjects. After directly subtracting subjects stratified as high risk, the number of subjects with data classified into gender, age, and residence groups was 10,620, 10,620, and 10,580, respectively.
Results of Cardiovascular Disease Risk Stratification, Using WHO/ISH Cardiovascular Risk Prediction Charts for the Western Pacific Region
The proportion of number of subjects in each risk subgroup to the total number of subjects in the group is described as a percentage.
CVD, cardiovascular disease; TCHO, total cholesterol.
The numbers of subjects in the high- and low-risk groups, who were classified by risk factors, such as age, gender, systolic blood pressure, TCHO, diabetes history, smoking history, and basic characteristics, such as BMI, and places of residence, are described in Table 3. The comparative numbers of low-risk and high-risk subjects, grouped by gender, age groups, and residence, are shown in the histogram in Figure 3 and described in detail in Supplementary Material S3.
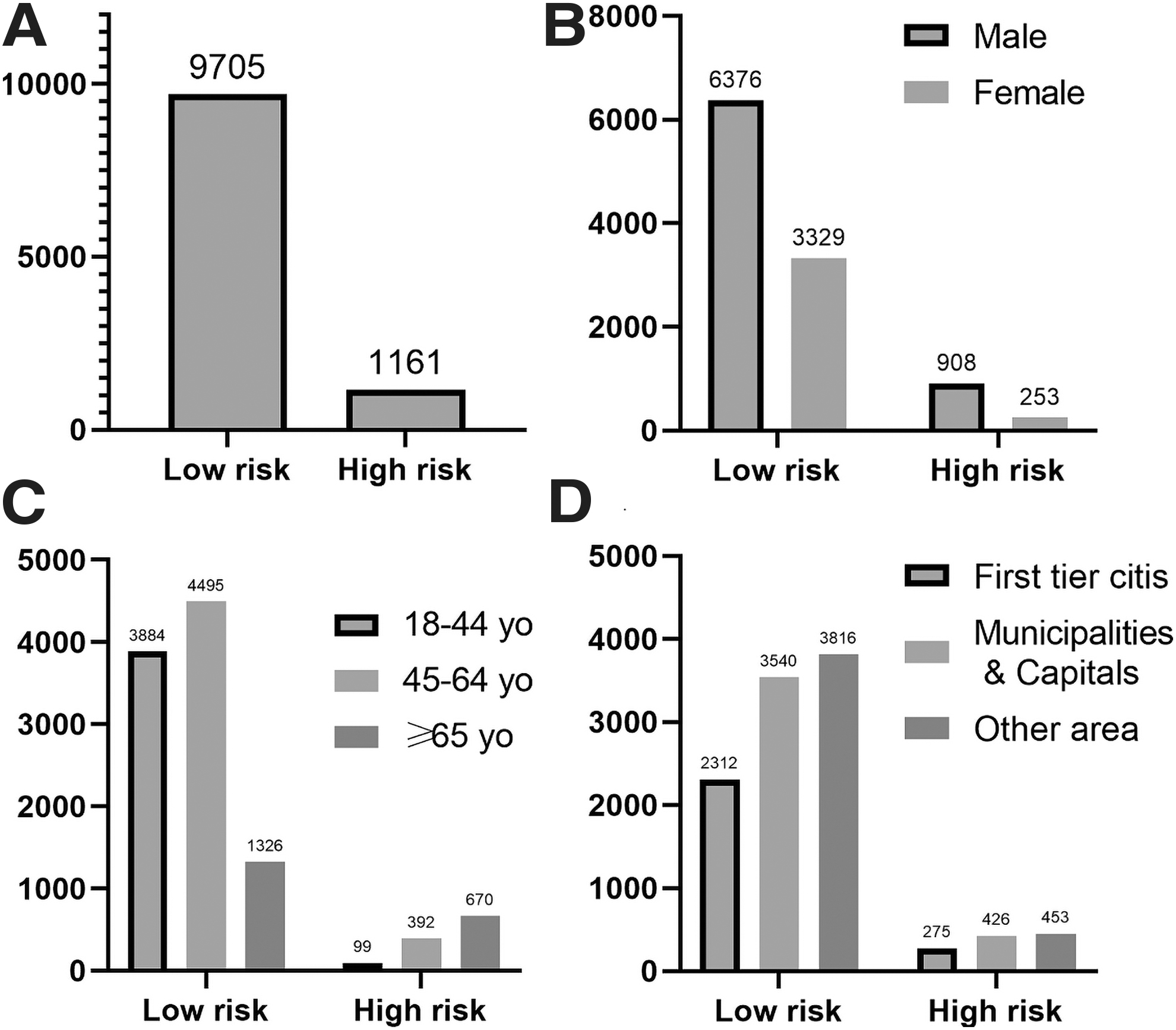
The comparative numbers of low-risk and high-risk total subjects
The Characteristics and Risk Factors for Subjects in the High- and Low-Risk Groups
The ratio of the number of high-risk subjects in each group to the overall number of subjects is presented in the last column as a percentage. The number of subjects in each subgroup is expressed as a percentage of the overall number of subjects in parentheses.
The risk factors involved in WHO/ISH risk stratification charts.
SBP, systolic blood pressure.
Discussion
To the best of our knowledge, this is the first study to implement CVD risk stratification for wearable device users; it describes the basic characteristics of users of wrist wearable devices using the “Amazfit health” app.
The subjects included for risk stratification were inconsistent with respect to the basic characteristics of all users. The subjects seemed older, were of the male sex, were living in poor economic and sanitary conditions, and had better wearing compliance. We speculate that the subjects were users who cared more about their health and had better compliance.
Even if it is expected that the number of CVD patients or CVD high-risk rate in users with sufficient data for risk stratification may be higher than the entire user population, the high-risk groups only accounted for 10.7% of all subjects. This shows that most of the users of wrist wearable devices in this study were people with a low risk of CVD. The services in the app pushed for users of wrist wearable devices may require differentiation based on risk levels. The education and intervention in the app may focus on encouraging healthy lifestyles for the majority of low-risk users. For a smaller population of high-risk users, intensive education and intervention may be required to reduce the occurrence of CVD events in the future.
There are currently many self-evaluating apps for risk stratification utilized by smartphone users. 9 –11 A study of atrial fibrillation patients using telehealth showed that the telehealth program may be beneficial for patients with higher CHA2DS2-VASc scores. 12
In some clinical studies from third world countries, similar risk stratification results using SCORE and FRS have been reported. 13,14 Although the definition of high CVD risk is different, Ranawaka et al. used WHO/ISH charts to assess participants with a 10-year CVD risk greater than 20%, accounting for ∼8.2% of total subjects, and the high-risk participants estimated by the SCORE criteria accounted for ∼11.8% of all subjects, which is similar to our results. 13
In a study conducted in eastern China using the Chinese population risk stratification tool China-PAR, the 10-year high risk of CVD (>10%) in the general population was ∼4.7%, which is lower than that observed in this study using WHO/ISH charts. 15 In a study reported by The WHO CVD Risk Chart Working Group to evaluate the revised WHO CVD risk prediction charts, the proportion of high-risk subjects (>10%) of the total participants was ∼10% in South Asia and Southeast Asia. 16 These results reflect that risk stratification using information collected by an e-health app may be feasible.
For CVD risk stratification in Asian regions, stratification tools, such as FRS, SCORE, and PCE, would be appropriate, and in China, the China-PAR algorism may be valuable. The information required by the WHO/ISH risk prediction chart was easy to collect, and no laboratory result was necessary. Laboratory results are difficult to obtain from relatively healthy people and areas with insufficient medical resources.
The study population only involved a relatively small group comprising users of Huami wrist wearable devices. The study results showed that this risk assessment tool can be used for screening in a larger population. However, this risk stratification method is less accurate than those used in other studies with a more rigorous design. Nevertheless, promoting this risk stratification method among users of all models of Huami wearable devices may help identify those with high CVD risk.
Several possible interventions may be employed for the selected population at high risk for CVD in the future: (1) targeted push contents about risk factor control in the app, such as calorie calculator, sodium intake calculator, smoking cessation guides, target exercise, and heart rate advice, to encourage users to actively report and control risk factors through an incentive mechanism in the app; (2) push CVD education materials in the app to inform users about CVD prodromal symptoms and shorten the time from event occurrence to medical intervention; and (3) recommendation to join the in-app-purchased health program, including ECG interpretation and online doctor consultation.
Nevertheless, further clinical studies are warranted to establish more evidence on the effective reduction of the actual occurrence of CVD events by these interventions in a high-risk user population.
Limitations
The study population was limited to the users of health-focused wrist wearable devices using the “Amazfit health” app and, therefore, did not include all users of Huami wrist wearable devices. Further risk stratification analysis of wrist wearable commercial device users and advising users with high CVD risk to utilize health-focused wearable devices may be beneficial. Since the data used in this study were all self-reported by the users without professional guidance, there may be data errors caused by user cognitive limitations or incorrect operations. The blood pressure and cholesterol data collected in this study may not be recent. Similarly, the information on whether the patient had persistent high blood pressure or renal disease was not available.
This study was not completely consistent with the WHO/ISH risk prediction chart; therefore, we speculate that it may have underestimated the proportion of high-risk users. This was merely a retrospective study to provide evidence for wider and more precise future user risk stratification and intervention practice trials.
Footnotes
Disclosure Statement
H.W. served as the vice president of Health & Medical Business Group of Huami Beijing Medical Health Technology Co. Ltd., R.S. served as Medical Director, R.Z. served as big data R&D director, and G.S. served as senior big data engineer. All other authors report that they have no conflicts of interest relevant to the content of this article to disclose.
Funding Information
This work was funded by Huami Beijing, without a titled research funding.
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.