
Abstract
Background:
The purpose of this study was to determine if any differences exist in patient satisfaction with office-based visits versus telemedicine visits following arthroscopic shoulder surgery.
Methods:
Patients undergoing shoulder arthroscopy were prospectively enrolled for 1 year. Patient demographic and clinical data (including complication events) and second postoperative visit satisfaction data were recorded and analyzed for statistical significance.
Results:
Ninety-six (n = 96) patients met inclusion criteria. Fifty-four patients (56.3%) participated in a traditional in-person office visit, and 42 participated in a video visit (43.8%). No significant differences were found between office and video appointments in terms of overall care satisfaction (9.46 ± 0.9 vs. 9.55 ± 1.0, p = 0.67). Females were significantly less satisfied with their second postoperative visit compared with males (8.3 ± 2.3 vs. 9.3 ± 1.5, p = 0.035). Significantly more females would also have preferred a traditional in person office visit compared with males (91% vs. 67%, p = 0.009). Video appointment patients spent significantly more time with their surgeon than office visit patients (57.64 mean rank vs. 41.39 mean rank, p = 0.003).
Discussion:
Video visit patients required significantly less time overall for their visit and spent significantly more time with their surgeon, although did not demonstrate differences in satisfaction.
Introduction
Since its inception in the 1950s, prevalence of hospital-based telemedicine has expanded rapidly, most notably in the last 5 years. 1 The utilization of telemedicine has perhaps never been more pertinent than with the onset of coronavirus disease 2019 (COVID-19), where telehealth-related services have been a major component of the medical field's response. 1 –3 The ability for physicians to provide instantaneous, direct care to patients at a distance is not only opportune for crises such as the coronavirus pandemic, but has also served in a broad scope of applications across multiple medical specialties. 2,4 –7
Within orthopedic surgery, telemedicine has been demonstrated to be feasible in settings, including outpatient care, 8,9 rehabilitation, 10,11 remote consultation, 12,13 and surgical follow-up. 14 –17 In an era where ∼90% of Americans have access to the internet, the use of virtual visits can circumvent obstacles, such as lack of transportation or time off of work, from impeding access to appropriate follow-up care and rehabilitation. 9,18,19 Furthermore, a 2019 study by Buvik et al. demonstrated that telemedicine actually saves money for the hospital when utilized in a relatively low quantity of patients. 13
Despite the demonstrated benefits of telemedicine for both patients and physicians, the effect on patient satisfaction with overall care is not yet clear. 14,15,20 The purpose of the current study was to compare satisfaction with overall quality of care between patients seen through telemedicine and those with office-based visits for their postoperative follow-up evaluation 6 weeks after arthroscopic shoulder surgery. The hypothesis for this study was that the two methods of postoperative follow-up would be equivalent with respect to overall patient satisfaction.
Methods
INCLUSION CRITERIA
Inclusion criteria consisted of: patients 18 years of age and older, consented to elective shoulder arthroscopy, and had the ability to properly utilize telemedicine software on a computer, tablet, or smartphone with a built-in camera. Patients were required to have access to a microphone (typically built-in), and Wi-Fi access whether at home or at work. Exclusion criteria included involvement in workers' compensation claims or ongoing legal actions, English as a second language, and subjects who were unable to properly utilize the necessary telecommunications software to conduct telemedicine visits. Telemedicine visits were conducted with a HIPAA-compliant telemedicine program that was integrated into the institutional electronic medical record, EPIC (Epic Systems, Verona, WI).
STUDY POPULATION
This was initially started before the COVID-19 pandemic as a prospective, randomized controlled trial, in which patients were recruited for study enrollment preoperatively if they met inclusion criteria. However, at the height of the pandemic, office-based care was significantly limited, and patients were seen only virtually for their postoperative visits. The pandemic led to the study instead of becoming a prospective comparative trial at the discretion of the surgeon. It was performed at a single institution with the approval of the authors' Institutional Review Board. This study received approval from NYU Langone's IRB (#19–01886). All patients in this study underwent shoulder arthroscopy performed by one of seven fellowship trained sports medicine or shoulder and elbow specialists between December 2019 and September 2020.
The second postop visit was selected for this study because of the more hands-on approach (suture removal, neurovascular assessment and teaching/demonstration of the home exercise program) that is utilized during the first postop visit for shoulder arthroscopy at our institution. Therefore, all patients had an in-person visit for the first postoperative visit following surgery, in which surgical findings were reviewed, a neurovascular exam was performed, the patient's subjective thoughts about pain and their postoperative course, as well as any questions or concerns the patient may have had were addressed. Portal sites were also inspected, and sutures were removed. Patients were also taught a home exercise program and a formal physical therapy prescription was given. The first postoperative visit typically occurred between 5 and 14 days after surgery.
The second postoperative visit occurred ∼6 weeks after surgery. Office and video visits included another discussion of the patient's postoperative course, as well as a physical exam. The exam primarily included another inspection of the portal site incisions as well as evaluation of passive motion. The visit would conclude with a review of the next phase of rehabilitation based on the patient's procedure. The only difference between the telehealth and in-office visits was the surgeon's inability to palpate the shoulder and perform a manual assessment of strength.
An a-priori power analysis was performed before commencement to determine how many patients would be required to detect a statistical difference. Based on a similar pilot study on knee arthroscopy evaluating satisfaction with care between video and in-person visits, a mean difference of 0.5 and standard deviation of 0.75 was used. The pilot study had a smaller mean difference and standard deviation (0.25, 0.35, respectively), but to be conservative, values were approximately doubled to determine sample size. Setting alpha to 0.05, and beta to 0.2 (80% power), it was determined that 36 patients would be needed in each group.
RANDOMIZATION
Patients initially were randomized to the “telemedicine” group if they had a medical record number (MRN) ending in an even number (0-2-4-6-8), or they were randomized to the “office” group if they had an MRN ending in an odd number (1-3-5-7-9) at their preoperative office visit. However, the decision was made to discontinue the randomization and to instead turn the study into a prospective comparative trial given the heightened importance of being able to carry out video visits to provide patients with care during the pandemic. At that time the patients were placed into each group at the discretion of the surgeon. With the exception of this change, all other aspects of the study remained the same. All patients were seen by their orthopedic surgeon for their initial postoperative visit in person within 5 to 14 days after surgery.
After the second postoperative visit (in person or telemedicine), patients were then emailed a REDCap-based survey to complete. Questionnaires were based on the Consumer Assessment of Healthcare Providers and Systems Surgical Care Survey (S-CAHPS), a validated measurement tool for postoperative patient satisfaction after a single outpatient surgery. 21 –23 This survey consists of 47 questions related to perioperative counseling, quality of interaction with surgeon, patient experience on the day of surgery, quality of interaction with anesthesiologist, and demographic items. Additional questions regarding visit format (i.e., office versus telemedicine), time required for visit, and patient preference of visit format were included for this specific study.
If patients could not be reached over email, an attempt was made to contact the patients through telephone and were asked to fill out the study survey. If surveys were not filled out 2 weeks following the second postoperative visit, patients were excluded from the final analysis. Patients were also excluded from analysis if they did not return for their third postoperative visit (typically 6 to 8 weeks after their second postoperative visit). Following the third postoperative appointment, patients' charts were reviewed for any complications that had occurred since surgery and recorded for further reporting.
OUTCOME MEASURES
The primary endpoint was determining statistical and clinical equivalence through patient response to the question, “Using a number (0 to 10, where ‘0’ is not at all satisfied, and ‘10’ is completely satisfied), please rate your satisfaction with your overall care.” Similar questions were asked about satisfaction with the second postoperative visit, whether the patients felt adequately informed about the postoperative plan, how much the patients liked their surgeon, and the likelihood they would recommend their surgeon to a friend or family member. Other questions were related to time spent, including how much overall time was required for your visit, including travel to and from (1–20 min, 21–40 min, 41–60 min, 61–80 min, 80+ min); and how much time did you spend with your surgeon during your visit (Did not see my surgeon, 1–5 min, 6–10 min, 11–15 min, 20+ min). After considering their experience, patients were then asked, in retrospect, if they would have preferred an office visitor a video appointment.
STATISTICAL ANALYSES
Statistical analyses was performed using independent samples t-tests for continuous variables (data normality confirmed by Shapiro–Wilk test for normality), Mann–Whitney U tests for amount of time spent (these were compared as mean ranks, as ordinal responses were given), chi-squared test of homogeneity for multinomial group comparison, Fischer's exact, and chi-squared tests for dichotomous categorical comparisons, and one-way analysis of covariance (ANCOVA) testing to assess influence of covariates. All statistical analyses were done using SPSS 26.0 (IBM Corporation, Armonk, New York).
Results
A total of 96 patients met inclusion and exclusion criteria. Seven surgeons were included, with patient contributions ranging from 7 to 23. Mean patient age was 50.0 ± 14 years, with 63 males and 33 females. Of the included patients, 54 (56.3%) participated in an in-person office visit, and 42 participated in a video visit (43.8%). Patient demographics for the total cohort can be found in Table 1. A majority of patients underwent either an arthroscopic rotator cuff repair (55 patients) or arthroscopic labral repair (22 patients) and the surgical demographics can be found in Table 2.
Patient Demographics
Surgical Demographics
RC, rotator cuff.
For the total patient cohort, surgeon, race, and education did not significantly affect any outcome measure assessed (p > 0.05). Females were significantly less satisfied with their second postoperative visit compared with males (8.3 ± 2.3 vs. 9.3 ± 1.5, p = 0.035). Significantly more females would also have preferred a traditional in-person office visit compared with males (91% vs. 67%, p = 0.009). There were no other significant differences in outcomes between male and female patients (Table 3).
Comparison Based on Sex
Significance was defined as p < 0.05. Values that crossed this threshold (statistically significant) are in bold.
There were no differences between office visit and video appointment cohorts in terms of age, sex, race, education level, or procedure type (p > 0.05). Demographic comparisons between the office visit and video appointment cohorts can be found in Table 4. No significant differences were found between office and video appointments in terms of overall care satisfaction (9.46 ± 0.9 vs. 9.55 ± 1.0, p = 0.67) or satisfaction with the second postoperative visit (8.92 ± 1.9 vs. 8.95 ± 1.8, p = 0.94). Other variables, including how adequate information regarding postoperative plan was conveyed, how much patients liked their surgeon, and likelihood to recommend their surgeon were similarly not significantly different between groups (p > 0.05) (Table 4). Each comparison was run subsequently as an ANCOVA to correct for effect of surgeon, sex, race, and education. No changes in relationships were found.
Comparison Based on Visit Type
Significance was defined as p < 0.05. Values that crossed this threshold (statistically significant) are in bold.
Patients assigned to the video appointment spent significantly less time with the overall appointment than those that had office visits, with 73.8% of the video visit cohort reporting the visit taking less than 20 min, as opposed to 55.6% in the office visit cohort (41.45 mean rank vs. 53.98 mean rank, p = 0.012) (Fig. 1).
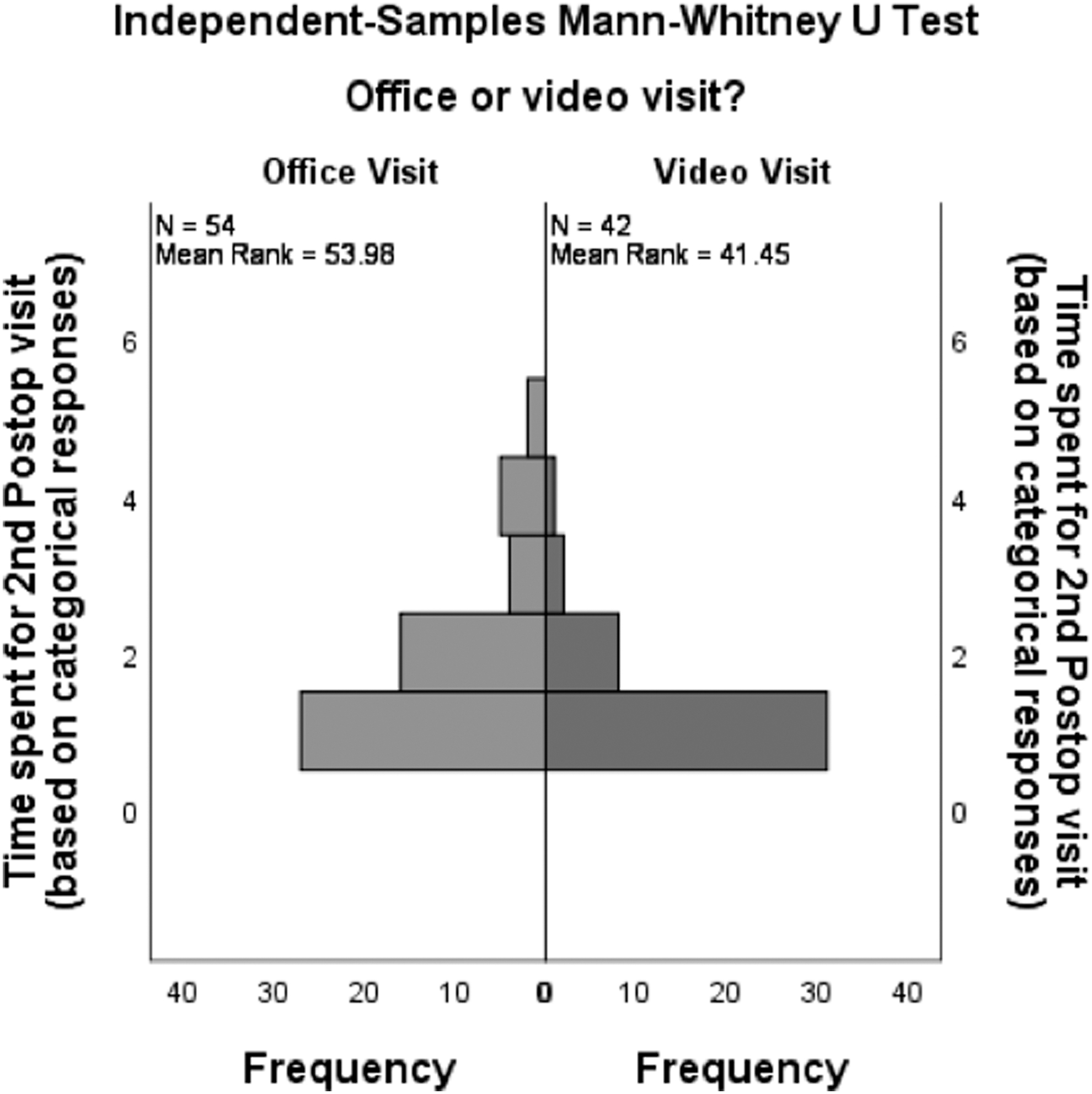
Comparison of the time spent overall during second postoperative visit, represented as categorical variables.
Conversely, video appointment patients spent significantly more time with their surgeon than office visit patients, such that 92.9% of video visit patients spent more than 5 min speaking to their surgeon as compared with 74.1% of the office visit patients (57.64 mean rank vs. 41.39 mean rank, p = 0.003). Of note, the mean rank does not represent specific number of minutes spent, as the options provided to the patient in the survey were categorical. Therefore, with multiple choice options presented in increasing increments of time, the mean rank indicates which group selected a higher (or lower) time bracket overall in comparison to the other group (Fig. 2).
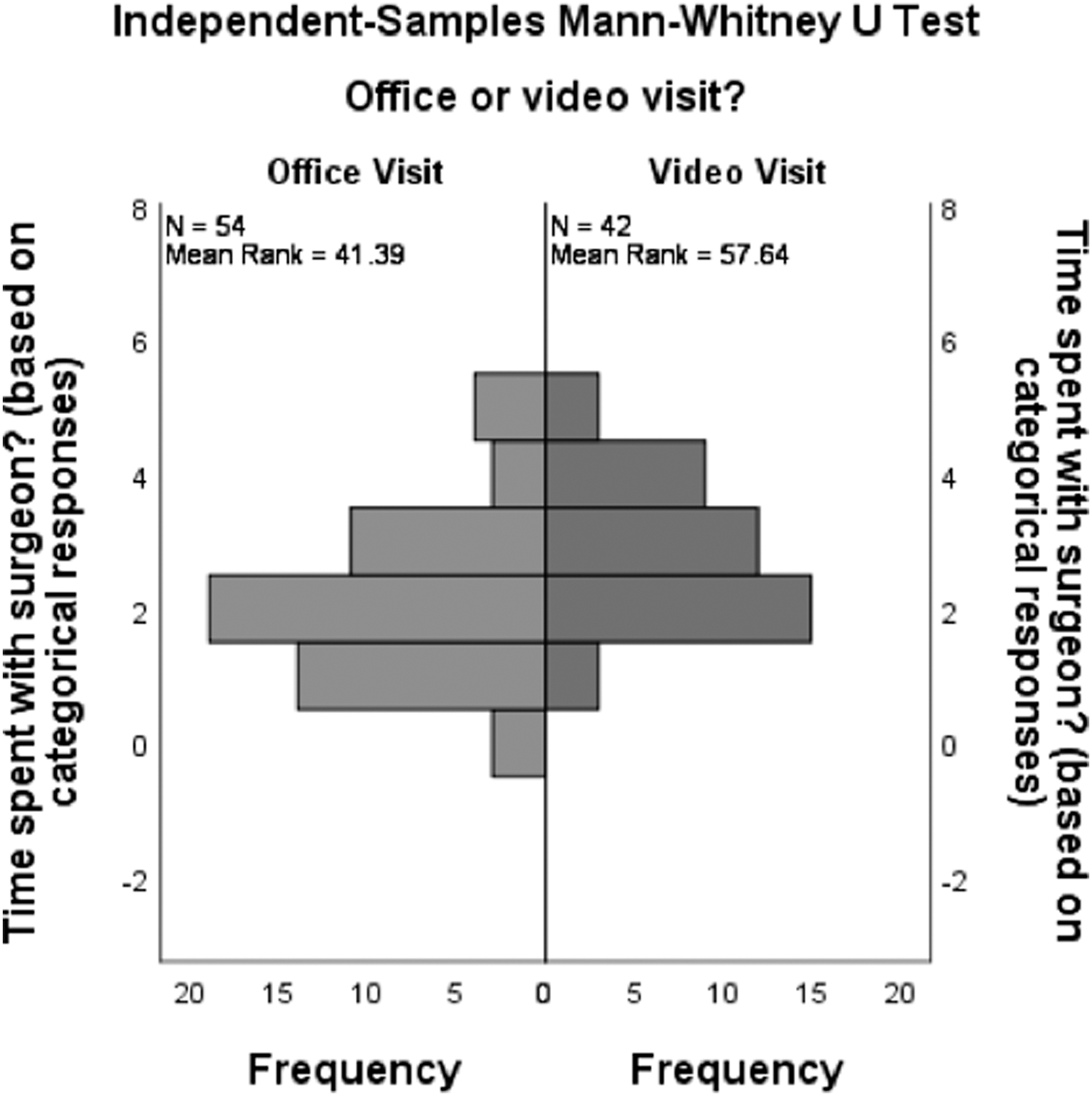
Comparison of the time spent with surgeon during second post-operative visit, represented as categorical variables.
When asked which visit type they would have preferred, significantly more office visit patients would have preferred in-office appointments (92.6%) compared with video visit patients (52.4%) p < 0.001 (Table 4).
Discussion
The most important finding of the present study was that there was no difference in patient satisfaction or perceived care between traditional in-office and video visits for the second postoperative visit after arthroscopic shoulder surgery. Additionally, video visits required less overall time for the visit, while simultaneously providing patients more time with their surgeon. Despite the favorable metrics for video visits, the majority of patients still reported they preferred in-office visits; however, the proportion of patients that preferred office versus video visits was significantly different between groups, with significantly more video visit patients preferring video visits. This suggests that, with more telemedicine appointment exposure, patients may prefer video visits in the future.
In light of the current COVID-19 pandemic, telemedicine and accessibility of health care from the safety of one's home is more relevant than ever and, as such, a tremendous amount of literature discussing its benefits and utilization has been published. In a recent systematic review, including multiple surgical subspecialties, Gunter et al. 7 highlighted high overall patient satisfaction with postoperative telemedicine visits. In a series of 78 patients that underwent total knee arthroplasty, Sharareh and Schwarzkopf 15 demonstrated superior patient satisfaction with postoperative telemedicine visits compared with in-office visits. Similarly, in a randomized control trial following 58 patients (28 telehealth vs. 30 office visit controls) postoperatively after arthroscopic rotator cuff repair, Kane et al. 14 reported greater than 90% patient satisfaction in both cohorts of patients, however, there was no attempt to demonstrate equivalence with respect to visit modalities. The current study also demonstrated high patient satisfaction between both cohorts, with no difference in overall satisfaction or perceived care at the second postoperative visit between video and in-person appointments.
Routine follow-up after shoulder arthroscopy is both time consuming and financially costly for both patients and surgeons. In a recent economic analysis of 273 patients who underwent rotator cuff repair, Murphy et al. 24 highlighted that a significant proportion of cost burden for the patient was associated with postoperative follow-up. In a prospective randomized control trial following 229 patients after total joint arthroplasty who were randomized to either in-office versus telemedicine visits, Marsh et al. 20 calculated a cost reduction greater than 60% for both patient and surgeon when considering time associated with each visit, time away from work, time for travel, and cost of travel when comparing in-office versus video visits.
Interestingly, in a subsequent study, Marsh et al. 20 observed that, despite the decreased financial burden and time requirements for both patient and surgeon over a 12-month period, there were higher levels of satisfaction among the in-office cohort compared with telemedicine cohort. In the present study, the telemedicine cohort reported significantly longer time spent talking to their surgeon, as well as significantly less time in their appointments compared with the in-office cohort. Despite favorable metrics for video visits, 92% of patients in the office visit cohort reported a preference for an in-office visit in the future, compared with 52% of patients in the video visit cohort. This suggests an element of patient unfamiliarity associated with video visits.
However, it also suggests that, with more exposure, patients may prefer video visits in the future. Conversely, the office visit patients, who have never had a video visit for an orthopedic issue, had a strong preference for in-person office visits in the future, possibly explained by their lack of video visit exposure. Another interesting finding of this study, which has not been addressed elsewhere in the literature, is the influence of gender and its potential role on patient satisfaction rate. Subgroup analysis found that of the 33 females included in this study, 91% prefer an in-office visit compared with 67% of the 63 males included. Additionally, females overall were less satisfied with their second postoperative visit than males, even though, on average, females spent more time talking to their surgeon compared with males. Ultimately, future studies looking specifically at the influence of gender and its potential role on patient satisfaction rate are warranted to draw further conclusions.
Data regarding patient safety with postoperative telemedicine is still somewhat limited and, as such, some have raised concerns. Despite these concerns, in the wake of the COVID-19 pandemic, telemedicine utilization went from 2% of outpatient visits to nearly 100% of all outpatient orthopedic visits. 25 Ultimately, the widespread adoption of telehealth visits since the onset of the COVID-19 pandemic has given providers the ability to care for patients remotely, which has the potential to permanently change the expectations of all those intimately involved with the way care is provided in orthopedics. However, despite this inevitable outcome, one of the most interesting findings from the current study is that the vast majority of patients preferred an in-office visit compared with telemedicine visit, even being located in the epicenter of the pandemic.
This finding speaks to the value, comfort, and reassurance that a face-to-face interaction provides patients when they see their orthopedic surgeon in the office. It also brings to light the utility of symptom screening, temperature checks, frequent use of hand sanitizer, and the mandating of masks—as there were no reported cases of COVID-19 in either the in-office cohort of patients or the health care staff taking care of those patients. Regarding complication rates, there were 13 report complications, which were approximately evenly distributed between office and video cohorts (6 vs. 7, respectively). This correlates closely to the findings of Kane et al. 14 who reported an overall complication rate of 12%, three patients (10.7%) in the telehealth cohort compared with four patients (13.3%) in the office-based cohort, all of whom experienced symptoms of tenderness and/or drainage in the first 2 weeks after surgery. These findings only further suggest the equal safety and efficacy of telemedicine visits compared with the traditional in-office visit.
LIMITATIONS
This study is not without its limitations. First, this study cannot be generalized to all patients, as we excluded non-English-speaking patients. Telemedicine may exacerbate the language barrier between health care providers and non-English speakers or partially fluent English speakers as well as complicate the use of a qualified translator. Both of these factors may play a role in patient satisfaction. Furthermore, patients were aware that the purpose of this study was to analyze postoperative satisfaction, which may have introduced a degree of bias. Additionally, we only examined the short-term follow-up at ∼6 weeks postop, although our results are promising—showing no significant differences in patient satisfaction for the second postoperative visit.
Of note, while not statistically significant, there was a much higher percentage of males in the in-office cohort compared with females, which may have been a possible reason for females being overall less satisfied with their second postoperative visit than males and having a stronger preference for in-office visits afterward. The time spent with surgeons was based on patient perception and not actually measured times, and therefore is subject to recall bias. Lastly, patients were followed up at different time intervals, which may have contributed to a degree of recall bias. The fact that the pandemic also led to a change in the study design from a randomized controlled trial to a comparative study is also a potential limitation given that the surgeons used their discretion to assign patients to groups for the second half of the study.
Conclusions
High rates of patient satisfaction were seen with both in-office and video visits for the second postoperative visit after arthroscopic shoulder surgery. Video visit patients required significantly less time overall for their visit and spent significantly more time with their surgeon. Data from the current study demonstrates the utility of telemedicine in the postoperative care of patients undergoing shoulder arthroscopy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.