
Abstract
Objective:
To analyze the impact of applying criteria for patient selection and interruption of dispensation in a telepharmacy program. Secondary objective: to conduct a socioeconomic analysis of requests for telepharmacy after applying the criteria.
Methods:
A retrospective observational study was conducted. We applied the criteria from September 1, 2021 to December 31, 2021 and reviewed the impact of their application by comparing the prior period (October 14, 2020–August 31, 2021) with the period when the criteria were applied. We analyzed the evolution of applications over time, the number of users, the evolution over time of rejected applications, and the associated reasons. Finally, we studied how the average income and distance to hospital are related to the number of requests. This study was reviewed by the authors' institutional ethics committee and was considered exempted from further review.
Results:
We applied the criteria to 2,379 patients. Dispensations by telepharmacy increased progressively. We provided telepharmacy services to 41.7% of all outpatients and rejected 962 applications (65% after the criteria were applied). The main pre- and postcriteria reasons for rejecting applications were refusal without express reason and the patient having sufficient medication, respectively. All patients corrected the situation that caused rejection. Telepharmacy requests and distance to hospital were not related, although the number of requests and average income were related.
Conclusions:
We provided pharmaceutical care with this protocol and encouraged patients to correct the reasons for interrupted dispensations. The new criteria render telepharmacy available to all patients, regardless of where they live or their purchasing power. Lower-income individuals use telepharmacy more often.
Introduction
Outpatient hospital pharmacy prescription drugs (OHPPDs) are a group of drugs with peculiarities that warrant their safe use and a follow-up; therefore, their dispensation should be reserved for hospital pharmacy services (HPSs). These are drugs usually costly and used for complex pathologies. Dispensation of such drugs to outpatients through hospitals began in Spain in 1982 with drugs for hemophiliac patients and later expanded to groups such as antiretrovirals for those affected by HIV, drugs for multiple sclerosis, biological drugs for immune-mediated diseases, and oral medications for cancer patients, among others. 1 –4 This method of dispensing, in addition to improved monitoring, adherence, and clinical control, has led to reducing costs by not necessarily needing commercial packaging adjustments and instead allowing dispensation in unit doses.
Outpatients under treatment with an OHPPD must travel to HPSs for treatment. These HPSs dispense drugs and provide pharmaceutical care, such as collaborating with the doctor regarding prescription decision-making; providing recommendations to patients on their use, administration, and precautions; providing advice on medication use; monitoring of pharmacotherapeutic treatments to be followed by patients; adherence to such treatments; and monitoring possible adverse reactions. 5,6 After the first confirmed case of SARS-CoV-2 infection in Spain, the government declared on March 14, 2020 a state of alarm resulting in the population being confined to their residences.
The pandemic posed a challenge to the pharmaceutical care of outpatients, which until now had been done mainly in person. HPS began to implement measures to adapt to the new situation and reduce the risk of contagion, such as the use of “telehealth,” 7 understood as the delivery of health services through information and communication technologies (ICT). HPSs began the implementation and management of remote pharmaceutical care programs. Different professional associations of pharmacists employ their own definitions of telepharmacy, which can vary widely.
The Spanish Society of Hospital Pharmacy (SEFH) has defined the concept as “remote pharmaceutical practice via ICT”. 8 Regarding the dispensing of OHPPDs, Margusino-Framiñán et al. 9 analyzed the advantages and drawbacks of some of the main outpatient remote care models, which are home dispensing from HPS, coordination of HPS with primary-care pharmacists, coordination of the HPS with community pharmacists, geolocation and hospital dispensing, and coordination of the HPS with patient associations.
In March 2020, motivated by the quarantine, our HPS began using telepharmacy to deliver medication to outpatients using the HPS coordination model with community pharmacists, which we have described. 10 Our HPS delivered OHPPDs through distribution warehouses to community pharmacies in the province upon requests from patients in the respective pharmacies. With each request, we send a sufficient amount of a drug until the next medical review, with a 2-month treatment maximum. When the medication is finished, the patient made a new request. A joint protocol was developed to ensure correct pharmaceutical care and safe and traceable distribution and dispensing of medications.
On October 14, 2020, the Andalusian Council of Official Pharmaceutical Associations, in collaboration with hospital pharmacists, developed a module on the platform AxónFarma®, with which we began to work systematically. This is a tool to process the medication requests that patients make every day in pharmacy offices.
Owing to the emergency situation and to facilitate access to this service to the greatest number of patients, we did not initially use any inclusion or exclusion criteria for patients. Starting in September 2021, we decided to incorporate criteria for selecting the patients likely to benefit from the telepharmacy program and criteria for interrupting remote dispensing. According to a survey conducted by the SEFH, 11 30.2% of hospitals that use inclusion criteria for telepharmacy eligibility select patients based on their personal circumstances, 9.7% do so based on their condition, and 4.3% depending on the nature of their medication. We conducted a search on the main selection criteria used for the remote dispensing of medication in our environment. We consulted the telematic pharmaceutical care plan in the outpatient pharmaceutical care units of the hospitals of the Valencian Community published in June 2021. 12 Taking all this into account and using our professional judgment and experience, we finally developed our own patient selection protocol.
This study aims to analyze the impact of applying the patient selection criteria and remote-dispensing-interruption criteria that we have used in our telepharmacy program. As a secondary objective, we performed a socioeconomic analysis of the telepharmacy requests after applying the criteria.
Methods
This was a retrospective observational study conducted in a single hospital center.
PATIENT SELECTION CRITERIA
Included in the telepharmacy program were patients who had received at least two in-person dispensations in the HPS, had clinical stability, and had no hospital admissions. It was considered essential that the patient attend an in-person visit in which the entire procedure of the telepharmacy process was explained and the first remote visit for pharmacotherapy was coordinated. The patient also had to sign an authorization to carry out this remote visit by telephone. Remote pharmacotherapeutic follow-up visits allow hospital pharmacists the implementation of pharmacovigilance services and pharmaceutical care plans for patients with comorbidities and for special populations. 13,14 They also allow to perform a remote clinical-therapeutic assessment, which contributes to the fundamental objective of pharmacotherapeutic follow-up, namely, guaranteeing achievement of the pharmacotherapeutic objectives. 8,15
CRITERIA FOR INTERRUPTING REMOTE DISPENSING
Telepharmacy requests from patients who no longer met any one of the selection criteria were denied, as were patients who
refused remote pharmacotherapeutic follow-up visits;
had changes or modifications to their treatments: if the doctor performing a review modifies the dose, route, or schedule of administration of a drug or adds or suspends an active principle, the patient will visit the HPS to notify staff of the changes;
did not adhere to treatment: patients who are not compliant with their treatments may resume telepharmacy after three adherent dispensations from the HPS;
did not take the medicine properly (doubled the dose, took it more frequently or less frequently, etc.);
failed to attend medical appointments of the drug-prescribing specialty; shipments can be resumed by telepharmacy when the patient attends a new medical appointment;
had to discard any of the medications dispensed due to poor storage, breakage, or loss, in which case they were excluded for 1 year;
had prescriptions or reports older than 1 year or that were not updated; telepharmacy may be resumed when new reports are submitted; or
still had medication at the time of making the request or had enough medication to last until the next medical appointment; the delivery of medication was accepted only in the 10 days before the patient needed more.
Dispensing was stopped until all the aforementioned items were remedied. The excluded patients were able to continue picking up their medication in person at the HPS, where they were re-evaluated for telepharmacy continuation.
We excluded narcotic drugs and growth hormones from the program because of their regulatory characteristics, along with drugs that need to be frozen for their conservation because these are difficult to transport and maintain in the cold chain.
APPLICATION OF THE CRITERIA TO THE TELEPHARMACY PROGRAM
Together with the Provincial Official College of Pharmacists, we prepared a document summarizing all the information about the telepharmacy program. After giving all the appropriate indications in the consultation, we reinforced this information by delivering the written document. We sent this document for distribution to patients, pharmacy offices, and those responsible for hospital medical services. In the HPS, three pharmacists were in charge of evaluating the applications for inclusion in the telepharmacy program and even offered inclusion to patients in appropriate cases. They evaluated each medication request made in AxónFarma to accept or deny it under these criteria.
ANALYSIS OF RESULTS
We applied the protocol to all patients who requested telepharmacy from September 1 to December 31, 2021.
We analyzed the impact of the application of these criteria by comparing the period prior (October 14, 2020–August 31, 2021) with the criteria application period. We analyzed the evolution of medication requests over time, the number of patients using telepharmacy, the evolution of rejected requests over time, and the reasons for rejection.
Finally, we analyzed whether the average income or the distance to the hospital in each locality influenced the number of telepharmacy requests. To do this, we prepared a map of the province with the number of telepharmacy requests of each locality to which the requesting pharmacy belonged. We calculated the number of applications per inhabitant after applying the criteria. We made a second map of the province with the average per capita income of each locality.
Results
We applied the selection and interruption criteria to a total of 2,379 patients.
Since dispensing by telepharmacy began in October 2020, total requests, regardless of whether medications were delivered or applications were rejected, increased progressively, as shown in Figure 1. From 749 requests in the first full month (November 2020), the number of applications reached a maximum of 1,148 in November 2021. There were no differences in this trend after applying the criteria in September 2021.
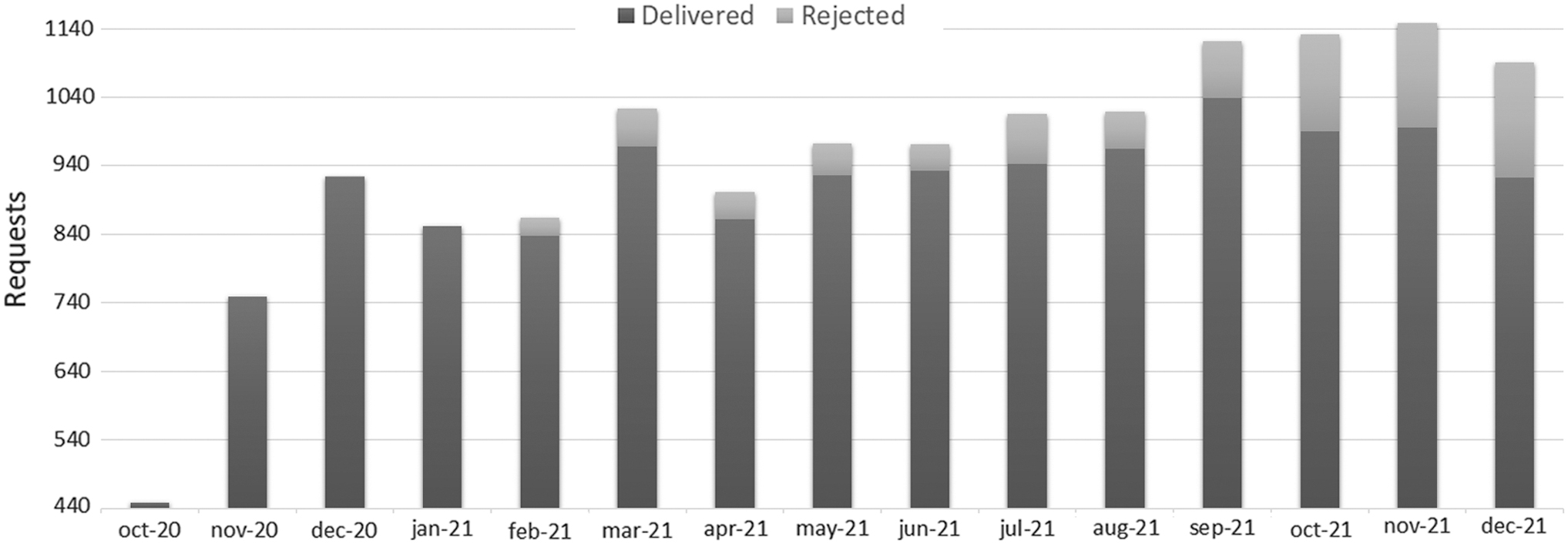
Evolution of the number of requests for medication by telepharmacy since its implementation.
During the period before applying the specific selection and interruption criteria (from October 14, 2020 to September 1, 2021), which was 10.5 months, medications were delivered to 2,608 patients, for whom a total of 9,408 remote medication deliveries were made. During the study period (4 months), the number of medication deliveries was 3,089 for 2,013 patients, of whom 245 were new patients who had never requested medication by telepharmacy and 1,768 were patients who were already receiving medication by telepharmacy.
Regarding the number of patients with active treatments, an average of 41.7% of all outpatients were treated by telepharmacy each month; 46.2% in October 2021 was the highest value, and 33.8% in the eligible period of October 2020 was the lowest value (Table 1).
Total Outpatients and Telepharmacy Patients Seen Each Month
The evolution over time of the number of applications denied for meeting any of the interruption criteria is shown in Figure 1. From the beginning of the telepharmacy service until February 11, 2021 (∼4 months), no requests were rejected. Since March 2021, rejected applications have increased each month, and more markedly since the application of the criteria in September 2021. We rejected a total of 962 medication applications: 334 before the implementation of the criteria and 628 after. Table 2 shows the number of requests denied under each criterion before and after working with the protocol.
Number of Rejected Applications Under Each Rejection Reason
HPS, hospital pharmacy service; OHPPDs, outpatient hospital pharmacy prescription drugs.
Even though we compared a 10.5-month period before the criteria and a 4-month period after their application, the number of refusals for any of the reasons was higher after applying the criteria, except in those where no reason was specified to the pharmacy. The main reason for refusal before applying the criteria was refusal without an express reason in AxónFarma, followed by the patient having enough medication at home. After applying the criteria, the main reason for refusal was that the patient had enough medication at home (28%), followed by lack of adherence (6%) and outdated medical reports (4.8%).
None of the patients who had been denied a request for medication according to the interruption criteria were still excluded from telepharmacy as of this writing, except those denied in the past month and a half. All of the patients denied before that have corrected the reason (interruption criterion) that caused the denial of this request and have been included in the telepharmacy program again.
In the socioeconomic analysis shown in Figure 2, the frequency dispersion map shows that there was no relationship between the volume of requests for telepharmacy and the distance to the hospital. Even so, data for some of the most distant areas showed fewer applications, whereas areas very close to the hospital were among the four locations with the most applications per inhabitant. We have found a certain relationship between the number of telepharmacy requests from each locality and its average income. The eastern zone of the province, which has many of the localities with the highest incomes, generally had fewer applications per inhabitant, whereas more applications tended to be associated with the western zone, which has lower incomes. This relationship was not absolute in all localities, although there was a general trend. Exceptions were areas such as Bellavista and Sanlúcar de Guadiana, with high incomes but many applications.
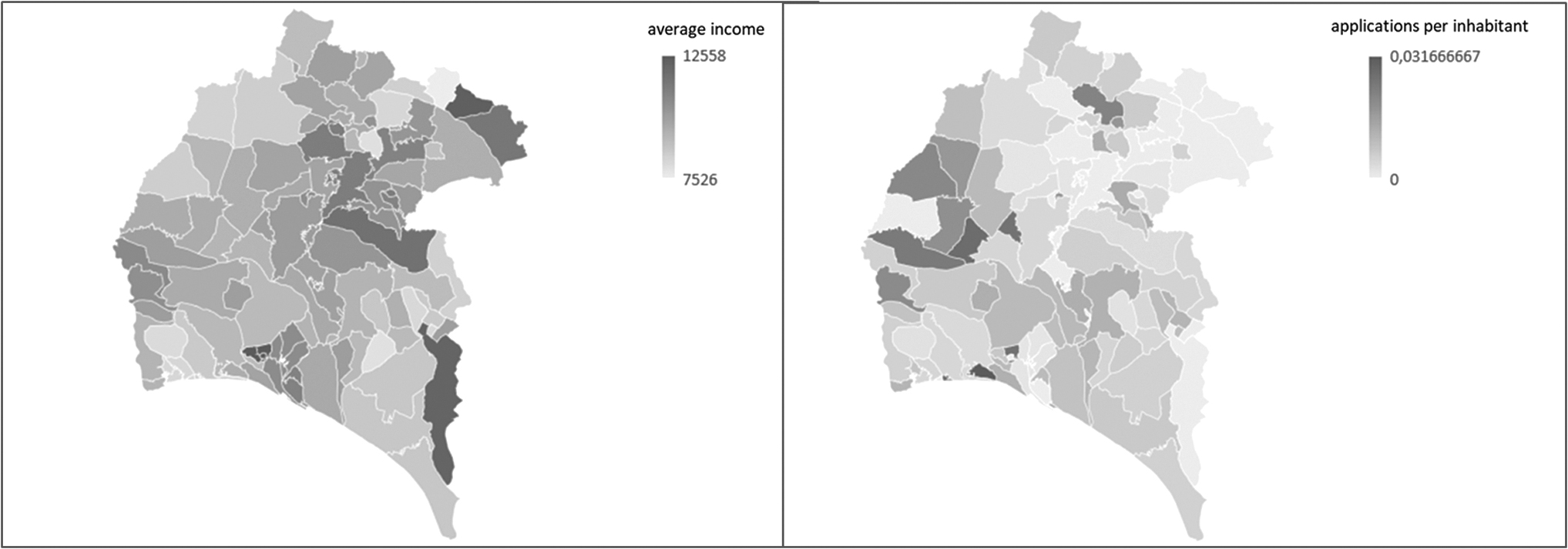
Map of application frequency dispersion and map of average income per capita.
Discussion
In March 2020, after the confinement caused by the COVID-19 pandemic in Spain, the HPS evolved a way of providing pharmaceutical care to outpatients, beginning to use telepharmacy programs to dispense OHPPDs that until now had been exclusively and by definition in person, with few exceptions. Owing to the urgency of the situation and to avoid the need for patients to travel, the majority of HPSs begin to use telepharmacy without applying any type of inclusion/exclusion criteria for selecting patients. Those who used such criteria based them on the personal circumstances of the patient or according to the type of drug. 11 Later, consensus documents of working groups 8 and guidelines appeared, which were issued by governing bodies of some autonomous communities, 12 where the use of certain criteria was recommended for selecting patients who would benefit from delivering medication through telepharmacy systems.
In September 2021, we protocolized the use of specific criteria for patient selection and dispensation interruption in our service. We selected the optimal conditions that an outpatient should meet in terms of medication and clinical processes and all items for adequate pharmaceutical care. Instead of including those conditions as selection criteria, we use them as remediable interruption criteria. In this way, we offered telepharmacy in a very broad way and with few conditions (having completed two in-person dispensations, no hospital admissions, and clinical stability). Once the patients were included in the program, we analyzed each request to reject only those that met some interruption criterion. When a patient who made a request for medication met any of these criteria, this request was denied and the patient was dropped from the telepharmacy program until the reason was corrected, after which the patient could be included in the program again.
In this way, we carried out pharmaceutical care by encouraging adherence to medication, adequate attendance at medical appointments, adequate storage of medications, and updating of medical reports, since all these criteria are interruption criteria, and patients who already had used telepharmacy would like to use it again, as stated in the satisfaction survey distributed in our previous study. 10
Remote pharmacotherapy follow-up visits by telephone allowed the hospital pharmacist to help patients who were denied telepharmacy. With these calls, the patients not only received pharmaceutical care but were also provided support to correct the reason for which they were discharged from the program.
Creating a document that was consistent with the College of Pharmacists regarding all available information on telepharmacy allowed us to work seamlessly with the pharmacy offices, since pharmacists knew the reasons applications were denied. In addition, it allowed patients to have this information available for their better understanding and easier remembering.
The growing demand for telepharmacy is a reality that has completely transformed our service. By choosing to offer telepharmacy at a broad scale, implementing the protocol has caused not a decrease but rather an increase in the number of requests. The mean number of patients using telepharmacy compared with the total number of outpatients confirms this trend, which has not been affected by the implementation of the selection criteria.
Regarding the rejected applications, none were rejected from the beginning of telepharmacy through February 2021. The average from March 2021 to when the protocol was implemented ranged between 3% and 5.3% of all applications. Since the implementation of the criteria, rejections increased from 7.5% in September 2021 to 15% in December 2021. We could think that this increase is due to the implementation of specific criteria for interruption of dispensing that did not exist before, added to the growing demand for applications for inclusion in the telepharmacy program that were widely accepted.
Rejecting a request generates more work since the patient must make another request by telepharmacy once the reason is corrected or must come to an in-person visit if expelled from the telepharmacy program. Therefore, rejecting one request will probably generate another one later.
All patients who at some point were denied a request according to the interruption criteria corrected the reason for being refused (except those denied in the past month and a half, since too little time has elapsed). The pharmacist must analyze each telepharmacy request by entering the patient's digital medical record to confirm that it does not meet any of the interruption criteria. For this reason, the use of this protocol is a method that quickly detects any incident with the medication and tries to encourage its correction, since we believe that patients prefer dispensing by telepharmacy for its convenience.
The new criteria have made telepharmacy available to all patients, regardless of where they live or their purchasing power. This implies a democratization of a service that was originally designed only for patients with mobility problems, socioeconomic problems, or residences in remote or excluded areas. We offer telepharmacy dispensation to patients regardless of the distance from their places of residence and their economic situation. This is reflected in the application dispersion map. Those furthest do not always utilize more telepharmacy. However, the current panorama of telepharmacy in our service is such that the lowest-income people use telepharmacy the most, who are also those who have more difficulty traveling to the hospital.
The limitation of this study is that it is a single-center study. It would be desirable to expand the research with new joint analyses among several centers.
Conclusions
We believe that the work of outpatient consultation is changing. The widespread use of telepharmacy and the use of remedial interruption criteria have allowed us to provide pharmaceutical care using tools such as telepharmacy and ICTs. Application of the protocol has not altered the growing trend of telepharmacy. The new criteria have made telepharmacy available to all patients, regardless of where they live or their purchasing power.
Footnotes
Acknowledgments
We wish to thank the College of Pharmacists, all community pharmacies in the province of Huelva, and the pharmaceutical cooperative Bidafarma, all of whom have collaborated selflessly in this project during the COVID-19 pandemic.
Authors' Contributions
Conception and design of the study, data collection, and analysis and interpretation of the data by L.D.S., G.D.B., and D.Y.F. Writing of the article or its critical review with important intellectual contributions by G.D.B., D.Y.F., E.S.G., M.D.S.-R., and L.D.S. Approval of the final version for publication by M.D.S.-R., E.S.G., and L.D.S.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.