
Abstract
Introduction:
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) led to the rapid adoption of telehealth to provide HIV care and treatment. However, limited information exists about the feasibility, acceptability, and efficacy of telehealth interventions at different points of the HIV care continuum.
Methods:
A systematic search was conducted of Ovid MEDLINE, PsycINFO, and CINAHL databases to synthesize evidence regarding the feasibility, acceptability, and efficacy of videoconferencing and video-based interventions for HIV testing and treatment in adult populations. Seventeen articles published through July 2021 were included in the review. We used descriptive methods to analyze data, and findings were reported using frequencies and percentages.
Results:
Findings show that videoconferencing and video-based interventions are generally feasible and acceptable. Videoconferencing is effective in improving adherence to HIV treatment and in promoting HIV testing. In addition, video-based interventions were effective in promoting HIV testing, treatment initiation, and adherence to medication. Both modalities enhanced linkage and retention in treatment for HIV-positive patients.
Conclusions:
Video-based and videoconferencing interventions are beneficial in HIV testing and treatment. However, the scarcity of primary studies employing these telehealth modalities means that there is a need for more research in these areas. Also, reviewed studies suffered from several limitations, including reliance on subjective measures, lack of standardized ways of evaluating acceptability and feasibility, use of small sample sizes, and short follow-up durations. In addition, there was less representation of studies from resource-limited settings disproportionately affected by HIV and AIDS. Thus, future research should focus on addressing these challenges.
Introduction
HIV remains an enormous public health challenge globally. By the end of 2020, about 37.7 million people were living with HIV worldwide, and more than half a million people died of AIDS-related illnesses. 1 Worldwide, about 28.2 million people living with HIV were accessing antiretroviral therapy (ART) by the end of June 2021, a fourfold increase from a decade prior. 1 Despite the progress in expanding access to ART, people living with HIV still face multiple barriers that impede access to HIV testing, and engagement in HIV care and treatment. Such barriers include expensive and unreliable transport, competing life events, mental illness, HIV stigma, beliefs about ART medicines, and negative patient–provider experiences. 2,3 Addressing these obstacles is critical to ensuring optimum medication adherence and the attainment of the Joint United Nations Programme goal of ending AIDS by 2030. 4
Telehealth has the potential to address some of the above barriers. The Health Resources and Services Administration defines telehealth as “the use of electronic information and telecommunication technologies to support long-distance clinical health care, patient and professional health-related education, health administration, and public health.” 5 For the purpose of this study, telehealth means the use of video-based and videoconferencing approaches to deliver HIV testing and treatment services. Video-based interventions were defined as those interventions that use content recorded in the form of videos to influence health behavior.
Videoconferencing interventions were interventions that use synchronous methods to facilitate provider-to-patient interactions. 6 The use of telehealth in HIV care offers several benefits, including reducing delays in seeking care because of fear of stigma and addressing transportation challenges, a common barrier to HIV care. 7 Other possible benefits of using telehealth in HIV care include reduced missed clinic appointments and increased flexibility, which may help address the issue of competing life events. 8
About a decade ago, Lester et al published the first study to demonstrate the effectiveness of a technology-mediated intervention using a short message service (SMS) to enhance adherence to ART among HIV-positive patients in Kenya. 9 Multiple studies in Nigeria, 10 India, 11 Cameroon, 12 and Kenya 13 have evaluated the effectiveness of mobile health (mHealth) for promoting HIV testing, medication adherence, and retention in care. Subsequently, several reviews have assessed whether text messages, interactive voice response reminders, or phone calls promote adherence and retention to ART; 14 –18 the findings from these reviews have been inconclusive. For instance, a recent review by Demena et al found that only 41% of the studies that examined medication adherence reported positive and significant results, and 12% improved retention in HIV care. 17
Until recently, SMS, interactive voice reminders, and phone calls have been the dominant mHealth modalities utilized to boost engagement in care for persons living with HIV. The emergence of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, which resulted in rapid telehealth adoption, transformed how health care is delivered to persons living with HIV. 6,19 Videoconferencing via several platforms such as Zoom became a viable way of sustaining patient engagement in HIV care. While several providers of HIV care services quickly implemented video-based approaches, little was known about these telehealth modalities' efficacy, acceptability, and feasibility.
This review sought to synthesize available data about the acceptability and feasibility of video-based approaches for telehealth HIV care and examine the efficacy of these modalities in helping persons living with HIV to achieve favorable health outcomes. The goal of this review was to extend our knowledge beyond the analysis by Budak et al 6 which had two limitations: first, restrictions to studies conducted in the United States, and second, a focus only on videoconferencing. The study also represents an update to the previous analysis by Tuong et al 20 regarding the effectiveness of videos for health behavior change. Specifically, this review sought to answer the following questions: (1) in adult populations, are video-based and synchronous videoconferencing interventions feasible and acceptable for HIV testing and treatment and (2) what is the efficacy of live videoconferencing and video-based interventions for HIV testing and treatment for adult populations?
Methods
SEARCH STRATEGY
The following databases were searched for relevant original articles: Ovid MEDLINE, PsycINFO, and CINAHL. Searches were conducted using the following keywords: exp *HIV/or exp *HIV Infections/, HIV*.ti., exp *telemedicine/, (telehealth, telemedicine, or video*).ti, (feasib* or accept*).mp. Search terms were combined using Boolean operators of AND, OR. Additional records were identified by hand-searching reference lists of primary and review articles deemed to be relevant for the review. All the searches were restricted to peer-reviewed articles written in English. Relevant articles published through July 2021 were included in the review. For the purpose of this review, acceptability was defined as the degree of receptivity and satisfaction with videoconferencing and video-based interventions. 21 Feasibility was defined as perceived convenience in using videoconferencing and video-based interventions 21 and includes aspects of completion and retention of participants in a study.
ELIGIBILITY CRITERIA
Studies were included in this systematic review if they met the following criteria: (1) included any of the following designs: randomized controlled trials (RCTs), quasi-experimental, prospective cohort, descriptive quantitative, descriptive qualitative, or exploratory qualitative, (2) had a study population of adults aged 18 years and older, (3) reported any of the following outcomes: linkage to HIV treatment, treatment initiation, HIV testing proportions, medication adherence, viral suppression, feasibility and/or acceptability of videoconferencing, and feasibility and/or acceptability of video-based interventions. Articles were excluded from the review if they compared two or more video-based or videoconferencing approaches, reported results from interventions based on SMSs, interactive voice recording, reminder phone calls, and evaluation studies.
STUDY SELECTION PROCESS
From the search of databases identified above, 1,394 records were retrieved, which included 2 additional articles identified through hand-searching references of relevant publications. After reviewing the titles of the retrieved articles, 1,352 records were excluded because their focus was irrelevant to the review questions. Forty-two studies were subjected to full-text review.
Twenty-five articles were excluded because (1) outcomes measured (such as HIV testing knowledge, chronic pain, substance use, smoking cessation, alcohol drinking, depression/mental health) were not relevant to review questions (n = 17); (2) the study population included participants aged <18 years (n = 3); (3) the intervention evaluated was not clearly defined (n = 1); (4) compared two video-based/videoconferencing approaches (n = 2); (5) the study design was not clearly stated (n = 1); and (6) one study reported results of a program evaluation. In summary, 17 articles were selected for review, and details of the review process are indicated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart in Figure 1.
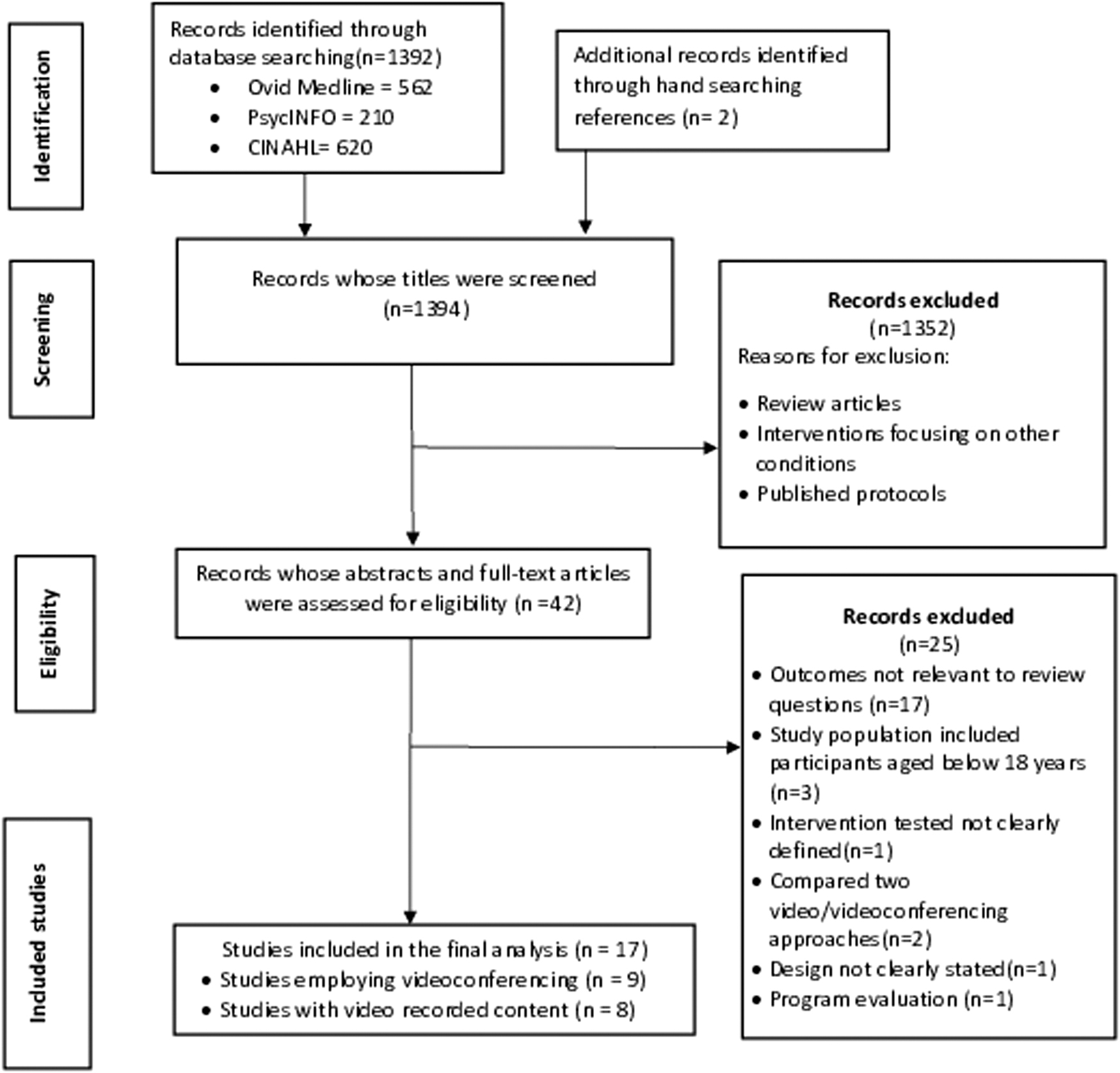
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
DATA EXTRACTION AND ANALYSIS
The following information was extracted from each study: first author and year of publication, study design, study setting, study population, sample characteristics (i.e., sample size, sex, mean and median age), intervention condition, comparator, outcome(s), outcome measures, measurement time points, study duration, and results/findings. For studies evaluating feasibility and acceptability, data were also abstracted about whether the study involved videoconferencing or video-based technology. Descriptive methods were used to analyze the data, and findings are reported using frequencies and percentages.
QUALITY ASSESSMENT
RCTs included in the review were appraised using the Joanna Briggs Institute critical appraisal tools. 22 Specifically, the following aspects were assessed: randomization, allocation concealment, similarity of groups at baseline, blinding of patients, treatment providers, outcomes assessors, identical treatment other than intervention, completeness of follow-up, whether intention-to-treat analysis was conducted, and appropriateness of trial design. Responses to each of the items were recorded as Y (Yes), N (No), UC (Unclear), NR (Not reported), and NA (Not applicable). Nonrandomized controlledl trials were not evaluated for quality due to lack of consensus on quality assessment of non-RCT studies. 17
Results
OVERVIEW AND CHARACTERISTICS OF REVIEWED STUDIES
Seventeen studies were reviewed. In terms of location, 76% (13/17) were conducted in the United States, 23 –35 two were from Malawi, 36,37 and one each from Peru 38 and Spain. 39 Almost half (47%, n = 8) of reviewed studies were RCTs. 25,28,29,33,35,38,39 A quarter (n = 4) were pre–postintervention studies, 24,30,32,35 two were cohort evaluations (n = 2), 23,31 and the remaining three (18%) were descriptive qualitative and cross-section studies. 26,27,36
Fifty-two percent (n = 9) of the studies reviewed focused on videoconferencing technology. 23,24,26 –31,39 Seven of these were experimental and observational studies, and the remaining two employed descriptive methods. Across these nine studies, participants totaled 3,285; the largest study had 1,670 participants. Approximately half (4/9) of these studies had small sample sizes of less than 100 participants, and participants were predominantly males. Most RCTs compared videoconferencing with either delayed availability of telehealth visits or usual care. The number of videoconferencing sessions ranged from 1 to 12, and each session lasted 20 to 45 min. One study did not explicitly state the number and duration of the videoconferencing sessions. The study duration varied widely, ranging from 6 weeks to 3 years.
A total of 5,468 participants were involved in eight video-based studies; participants were recruited in a variety of settings, including emergency departments, 32,33 outpatient clinics, 34,37 and several online platforms. 25,38 A majority of the interventions utilized a single video except for studies by Aronson et al 32 and Washington et al 25 that employed multiple videos, lasting between 1 and 3 min each. Videos varied in length from 1 to 27 min and were, in some cases, followed by a question and answer session to clarify issues that participants did not understand. 33,37 Some of these studies sent daily electronic mail and weekly text message reminders to participants to complete required assessments. The major comparisons for videos were face-to-face counseling sessions delivered by trained health workers and standard text messages. For studies that explicitly stated study duration (n = 6), the range was from 1 to 10 months.
FEASIBILITY AND ACCEPTABILITY OF VIDEOCONFERENCING
Of the 17 studies included in this review, 5 (29%) examined the feasibility and acceptability of videoconferencing for HIV testing and treatment. 24,26,27,29,30 In three studies, feasibility and acceptability were assessed in combination with other HIV treatment outcomes. 24,29,30 Two studies evaluated these parameters separately. 26,27 Acceptability was determined in multiple ways, including Likert-type items administered as exit interviews or during the study, and qualitatively using open-ended questions.
Overall, the results indicate that a videoconferencing modality for HIV testing and treatment is acceptable. Satisfaction ratings were high, and ratings for willingness to use the service ranged from 57% to 100%. Feasibility was gauged in terms of study retention, video call completion rates, and incorporating patient experiences with the service. Studies employing retention rate at follow-up and call completion rate found videoconferencing feasible with 80.3% to 90% rates. Patients described videoconference services as convenient, efficient, and less intimidating than face-to-face consultations. 27,36
EFFICACY OF VIDEOCONFERENCING IN HIV TESTING AND TREATMENT
Seven of the 17 (41%) studies reviewed used experimental and observational methods to examine the efficacy of videoconferencing in HIV testing and treatment (Table 1). Outcomes evaluated were HIV testing rates, medication adherence (gauged using viral suppression or subjectively by patient self-reports), linkage, and retention in treatment. Of the five studies that focused on medication adherence, 28 –31,39 four (80%) found positive results; three studies reported significant results. 27,28,31 Two studies utilized videoconferencing to promote HIV testing and linkage to treatment. 23,24 The study that focused on HIV testing found a positive result, 24 but the study that investigated linkage to HIV treatment did not yield a statistically significant result. 23 Only one study examined the utility of videoconferencing in enhancing retention in treatment for persons living with HIV, and no significant difference was found between the treatment and control groups. 28
Summary of Studies That Evaluated Videoconferencing Interventions
AOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence interval; RCT, randomized controlled trial; RR, risk ratio; VBPC, videophone-based pill count; VL, viral load.
FEASIBILITY AND ACCEPTABILITY OF VIDEO-BASED INTERVENTIONS
Three of the 17 studies in this review assessed the feasibility and acceptability of video-based HIV testing and treatment interventions. Two studies utilized Likert scale-type items for assessing these variables. 37,38 One study qualitatively explored patients' perceptions about using videos to enhance maternal medication adherence and retention in HIV treatment. 36 Generally, video-based interventions were feasible and highly acceptable. In one study, more than 90% of patients felt comfortable watching the videos, and patients found the content easy to use and understand. 37
EFFICACY OF VIDEO-BASED SERVICES IN HIV TESTING AND TREATMENT
Five randomized controlled trials 25,33,34,37,38 and two quasi-experimental 32,35 studies tested the modality of video-based methods in improving HIV testing and treatment (Table 2). The outcomes assessed were the proportion of participants accepting to test for HIV, initiation, adherence, and retention in HIV treatment. Of the five studies that examined the effect of video-based content on HIV testing behaviors, 25,32 –34,38 80% found positive results in favor of the intervention. Specifically, three of these five studies (60%) reported statistically significant increases in testing in treatment groups relative to control groups. 25,34,38
Summary of Studies That Evaluated Video-Based Interventions
Con, control; Int, intervention; MSM, men having sex with men.
The two studies that investigated the effect of a video-based intervention on adherence used disparate measures of establishing adherence, and both reported significant results in medication adherence. 35,37 Only one study explored the use of video-based content in promoting the initiation of treatment in persons living with HIV. 35 The results from this quasi-experimental study indicated a statistically significant increase in ART initiation. Neither of the two studies that were conducted to investigate the effect of videos on the retention of patients in HIV treatment found a statistically significant difference between the exposed and control groups.
Overall, this review found that the use of videoconferencing and video-recorded content is a feasible and acceptable approach for enhancing HIV testing and treatment (Table 3). Videoconferencing approaches appear to promote adherence to HIV treatment but were not found to help enhance linkage and retention in care. However, video-based methods demonstrated effectiveness in promoting HIV testing, initiation, and adherence to medication.
Descriptive Studies That Separately Evaluated Feasibility and Acceptability of Videoconferencing and Video-Based Interventions for HIV Treatment
RISK OF BIAS ASSESSMENT
Table 4 represents a risk of bias assessment for the eight RCTs included in the review. All the RCTs randomly allocated participants to either intervention or control group. Only three studies reported allocation concealment. 29,33,38 Furthermore, six of the eight studies reported that the intervention and control groups were comparable at baseline. 25,28,33,34,38,39 There was an elevated risk of performance bias in most studies because none reported whether patients or outcome assessors were blinded. Four of the RCTs did not report intention-to-treat analyses, which increase the risk for attrition bias. The risk of self-report bias was observed in 50% of studies that relied on subjective measures for evaluating adherence to ART medication. 29,37,39
Risk of Bias Assessment for the Randomized Controlled Trials Included in the Review
N, no; NA, not applicable; NR, not reported; UC, unclear; Y, yes.
Discussion
This review aimed to examine the feasibility, acceptability, and efficacy of videoconferencing and video-based interventions for HIV testing and treatment in adult populations. We found that videoconferencing and video-based interventions were generally feasible and highly acceptable. High satisfaction scores were reported with videoconferencing services. Low attrition and high call completion rates demonstrated the increased feasibility of videoconferencing services. All (100%) videoconferencing interventions that investigated adherence found either no difference between the treatment and control groups or increase in adherence from baseline levels.
Similarly, the only study that examined HIV testing using video chatting reported 100% testing rates. Thus, videoconferencing seems effective in improving adherence to HIV treatment and promoting HIV testing. However, none of the two studies that sought to improve linkage and retention in care reported significant results, which indicate that the use of a videoconferencing modality did not appear to help enhance linkage and retention in treatment for HIV-positive patients. Of the two video-based interventions that reported retention in care as an outcome, all found null results.
Regarding the feasibility and acceptability of videoconferencing and video-based interventions, the findings from this synthesis are consistent with those from a review conducted by Daher et al, who found that digital innovations for HIV care were acceptable, feasible, and generated impact. 21 Indeed, Simoni et al argued that the prevalence of favorable attitudes toward digital technologies is a sign that the field is ready to advance to more rigorous and well-powered RCTs. 40 However, it is critical to note that most of the studies examined by the extant reviews are from developed countries. For instance, the review by Budak et al 6 focused entirely on studies conducted in the United States, and 63% of the studies analyzed by Daher et al 21 were conducted in America or Europe. Future research is needed to explore the feasibility and acceptability of these telehealth solutions for patients and health providers from regions that have not been sufficiently represented in the literature.
Although this review found that both telehealth modalities appeared effective in improving medication adherence, caution should be exercised in interpreting this finding because about 67% (4/6) of studies that evaluated adherence relied on patient self-reports. The reliance on single subjective measures has been cited as a common challenge that merits serious attention in future studies to reduce the possibility of introducing bias. 21 Reliance on self-reports was observed in the assessment of acceptability and feasibility of videoconferencing and video-based interventions. Across the analyzed studies, diverse methods such as the use of qualitative exit interviews, Likert scales, and analog scales were used to assess acceptability and feasibility, which posed a challenge in making comparisons across studies. Future research will benefit from the use of standardized ways of evaluating acceptability and feasibility.
In addition, this review found that studies suffered from several limitations, such as the use of small sample sizes, which leads to a lack of power to detect intervention effects. For studies investigating retention in HIV care, the follow-up time ranged from 3 months to about 1 year. These short study durations may also have compromised the intervention's ability to detect meaningful effects. Future studies should aim to recruit large samples and utilize sufficient follow-up periods, both of which are argued to be necessary conditions for studies to improve adherence and retention of patients in HIV treatment. 41
Compared with previous reviews that have been based on the use of SMS, 18,21,42,43 interactive voice recordings, 17 phone calls, 17,21,43 social media, 21,42 online websites, 44 and mobile applications, 44 this review broadens the understanding of the utility of newer approaches such as videoconferencing in HIV care and treatment.
LIMITATIONS
This review had several limitations, which must be considered when interpreting the findings. First, only published articles were included in the review. We did not search grey literature or contact authors who have published in this area. Because of this, there is a possibility that some relevant literature was not included. Second, only articles published in the English language were included. However, because most scientific literature tends to be published in English, this review is expected to cover most of the current studies on this topic. Third, no technology-based database was searched.
However, because most studies testing technology-based interventions in the realm of health science tend to publish their findings in journals indexed in the databases searched in this review, there is a minimal chance that relevant studies were missed. Fourth, from the years of published studies included in this review, it is very likely that we missed videoconferencing use deployed during the peak of COVID-19 pandemic. Finally, our ability to compare across studies was limited because multiple operationalizations of similar outcomes were used.
Conclusions
We reviewed studies that tested video-based and videoconferencing interventions for HIV testing and treatment. Previous reviews about the application of information and communication technology in the HIV care continuum have heavily focused on the use of SMS, phone calls, social media, and online platforms at different points in the HIV care continuum. Findings show that videoconferencing and video-based interventions are generally feasible and acceptable. Videoconferencing is effective in improving adherence to HIV treatment and in promoting HIV testing.
In addition, video-based interventions were effective in promoting HIV testing, treatment initiation, and adherence to medication. Both modalities enhanced linkage and retention in treatment for HIV-positive patients. However, some studies analyzed in this review used small sample sizes; others followed participants for relatively short periods. Both limitations may have negatively affected the quality of evidence reported. Furthermore, our review found less representation of studies from resource-limited settings disproportionately affected by HIV and AIDS. Hence, studies are needed in regions underrepresented in the literature.
Footnotes
Acknowledgment
The authors wish to acknowledge the University of Minnesota Graduate School for the Doctoral Dissertation Fellowship support awarded to Charles Peter Osingada.
Authors' Contributions
C.P.O.: Conceptualization (lead), data analysis (lead), and writing original draft (lead). B.M., T.F.P., M.F.T., and C.M.P.: Conceptualization (supporting), and critical review and editing (equal).
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive enternal funding.