
Abstract
Objective:
The introduction of emergency telemedicine care models is a common theme in health jurisdictions that include rural and remote populations. How the availability of these models influences the way clinicians manage traumatic road crashes is not yet fully understood. This study seeks to compare road crashes where telemedicine was and was not used and to identify any variables that may increase the likelihood of telemedicine usage by treating clinicians.
Methods:
Road crashes reported in the state Department of Transport and Main Roads (Queensland, Australia) crash database between January 1, 2019, and November 30, 2020 (n = 23,734) were compared to videoconferencing call logs to determine which crashes resulted in treatment that was supported by telemedicine (n = 204). Analysis was performed to examine differences in characteristics related to the crash depending on whether telemedicine support was requested.
Results:
Road crashes where telemedicine support was requested on average involved more casualties (1.6 vs. 1.41; t(11,287) = −3.26, p < 0.001, relative risk = 1.13). Crashes that occurred in rural settings accounted for most requests for telemedicine (65.68%; X 2 = 159.2, p < 0.001) and a greater percentage of crashes in remote locations (3.36% vs. 2.35%; X 2 = 256.97, p < 0.001, relative risk = 1.43). The use of telemedicine support for crashes was associated with a 13% increase in the mean number of casualties, compared to crashes where telemedicine support was not used.
Conclusion:
Telemedicine support is requested by clinicians providing emergency treatment in the management of road crashes that produce more severe injuries, involve multiple casualties, and take place in more rural settings or remote locations.
Introduction
Despite a growing body of evidence that telemedicine is effective in the management of unscheduled hospital presentations in rural and remote locations, levels of usage vary greatly. 1 –12 Even in evaluations of emergency telemedicine models that describe positive effects such as improved clinical effectiveness, speed of care, or reduced transfers, telemedicine was used in as few as 0.8% of all possible opportunities. 9 Investigations have typically focused on the impact of telemedicine in instances where it was used and less frequently compare the circumstances between when telemedicine was and was not used. Understanding these differences may provide practical contributions to clinical guidelines and how clinicians are trained in the use of telemedicine technology.
Telemedicine support of emergency presentations has been used within Queensland to respond to the needs of Australia's most decentralized mainland population since 2006. Today, over 110 public hospitals and multipurpose health services throughout regional and remote Queensland are connected to emergency clinicians operated by Retrieval Services Queensland (RSQ) with high-definition video cameras. This technology allows frontline clinicians working in isolated health services to link with consultants from tertiary centers for assistance with an unscheduled patient presentation. Critical care continues to be provided until such time that the patient stabilizes or is retrieved.
Evaluating the use of telemedicine support for road crash victims is challenging because each event is a unique combination of many variables making their comparison difficult. Clinical users of emergency telemedicine support models have been asked for their opinions of its efficacy, 13 –15 and studies have produced evidence of improved system outcomes such as reductions in emergency wait times of 12 min. 15 –18 The authors, however, are not aware of any attempt to systematically compare specific road crashes grouped by whether telemedicine models of care were used or not.
While RSQ has developed several documents guiding the notification of severe trauma and the use of telemedicine in emergency settings (Figure 1), there are no prescriptive indications for the use of telemedicine in severe trauma. This project aimed to determine if there are patterns in the use of telemedicine among clinicians in the absence of any requirement to use of telemedicine. This may indicate that under certain circumstances, clinicians are independently determining that emergency telemedicine support would assist them in the management of their patients.
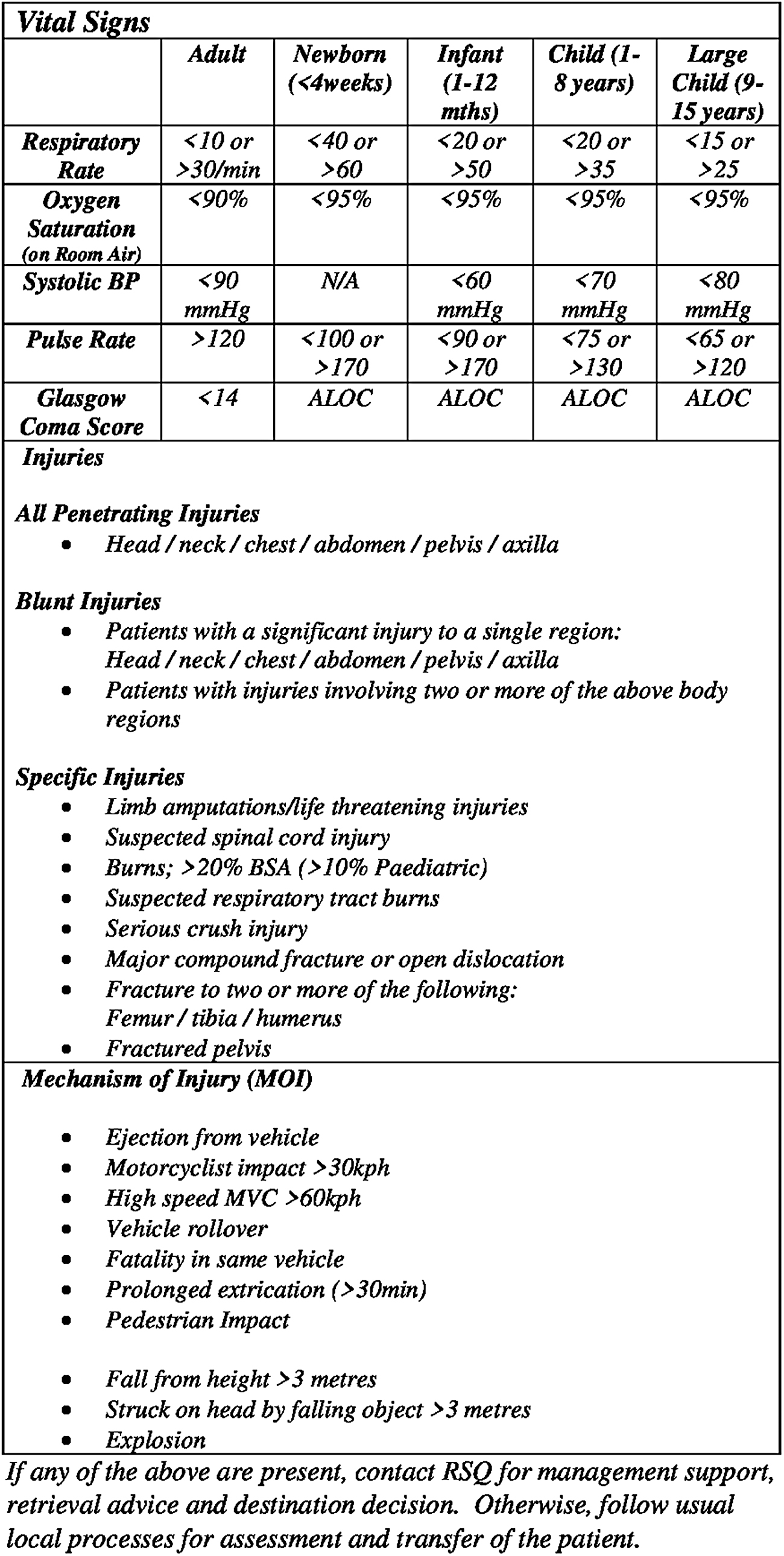
Criteria for early notification of trauma for interfacility transfer.
Methods
The Department of Transport and Main Roads (Queensland, Australia) was contacted for an extract from their crash database of all crashes reported on public roads in Queensland between January 1, 2019, and November 30, 2020, the most recent validated data available at the time of analysis. The Human Research Ethics Committee at The Royal Brisbane and Women's Hospital determined the retrospective nature of this research involved no more then minimal risk to the subjects. Crashes in which occupants were uninjured or resulted in injuries that did not require hospitalization were removed to create a subset of crashes that could potentially require remote telemedicine support.
A data matching exercise was performed to compare video call history logs that closely match in both time and location to a road crash that required hospitalization (a video call made to a hospital within 2 h and in the same Local Government Area of a reported crash was proposed to be in response to that crash). Proposed matches were then validated by the review of patient-level records retained by RSQ by an emergency physician to confirm that treatment provided was consistent with that which would be provided to a road crash victim (Fig. 2).
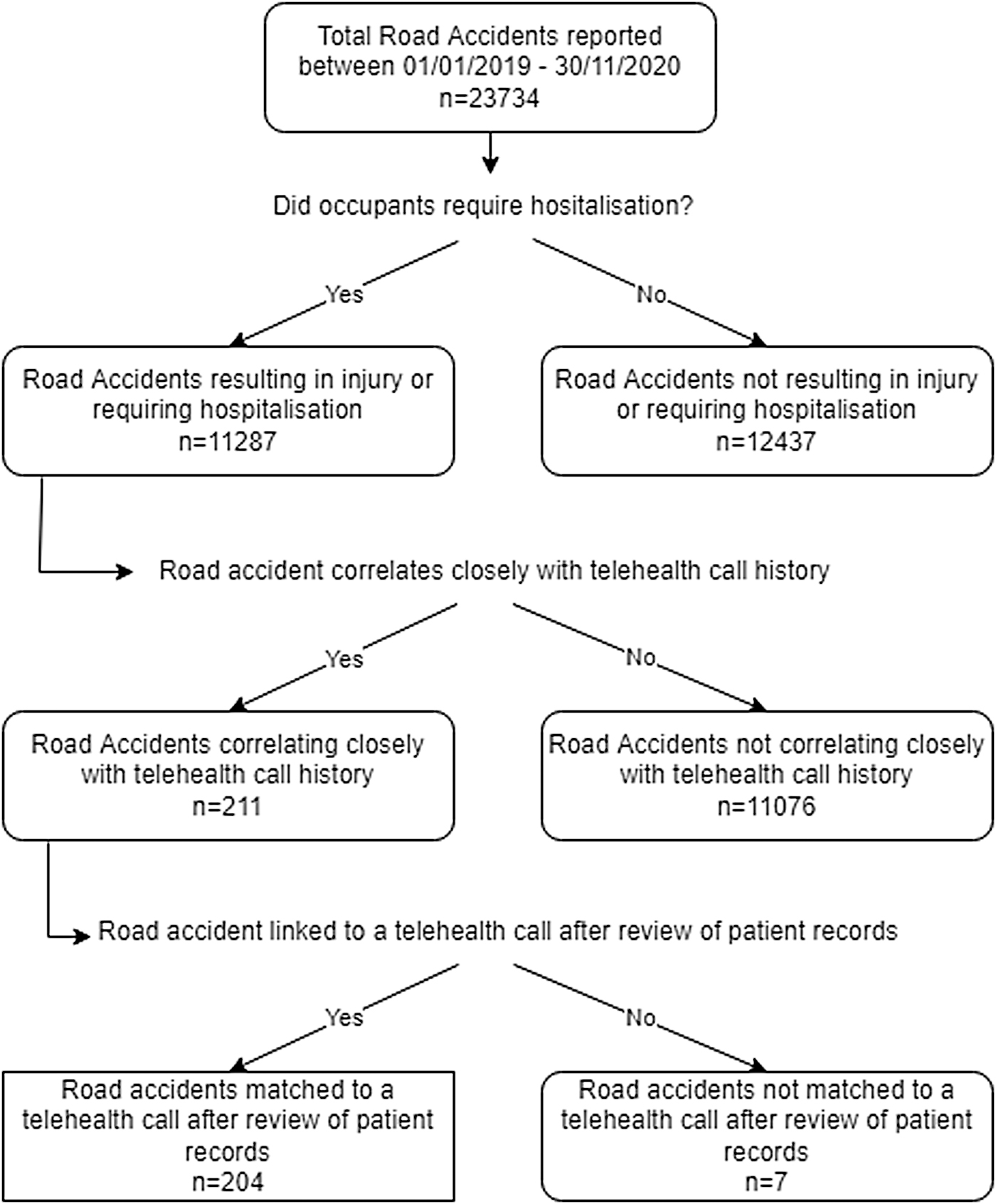
Selection of 204 cases for further analysis from the original dataset.
A total of 23,734 road crashes occurring within Queensland during the study timeframe were reduced to a subset of 11,287 when crashes not producing injuries that require hospitalization were removed. From this list, 211 (1.87%) potential instances of RSQ making a video call to a regional hospital in response to the presentation of road crash victim(s) were identified. A validated list of 204 (1.81%) matches were produced after reviewing available medical records.
Variables were collected on each crash including
Remoteness. The Accessibility and Remoteness Index of Australia (ARIA) divides the nation into five classes of remoteness based on a measure of relative access to services (major cities, inner regional, outer regional, remote, or very remote).
Setting. Significant Urban Areas (SUAs) represent Urban Centres, or groups of Urban Centres that contain a population of 10,000 or more. A crash occurring within an SUA is considered urban otherwise classed as a rural setting.
Severity. The severity of injuries to all occupants in a road crash is recorded and includes minor injury or medically treated where paramedic or hospital staff provide care to a person, but they are not admitted to hospital, hospitalized when they are admitted to a hospital or a fatality, where a person dies within 30 days of a crash as a result of injuries received in the crash.
Crash Nature. Determine by the initial event in any sequence of events in a road traffic crash. Crash Nature categories include angle, fall from vehicle, head-on, hit animal, hit object, hit parked car, hit pedestrian, overturned, rear-end, and sideswipe.
Crash Type. A logical category into which one or more similar crash natures is classified. Crash natures can be grouped into the following crash types: Single vehicle (hit parked vehicle, hit fixed obstruction or temporary object, overturned, and fall from moving vehicle), Multivehicle (angle, sideswipe, rear-end, and head-on) or Hit Pedestrian.
A series of Two Sample t-test or Chi-Square tests (developed in R ver 4.0.5) used the newly combined dataset containing road crash variables (crash severity, crash nature, crash setting, and telemedicine usage) to determine association between telemedicine usage and (1) number of casualties per crash, (2) remoteness, and (3) setting (Table 1).
Comparison of Crashes by Telemedicine Use
ARIA, Accessibility and Remoteness Index of Australia.
Results
Road crashes that prompted the use of a telemedicine support model to assist with management produced a higher average number of casualties in the dataset used by this study compared to those that did not (1.6 vs. 1.41; t(11,287) = −3.26, p < 0.001, relative risk = 1.13). A strong association between telemedicine use and setting was observed with 65.68% of total crashes prompting telemedicine support occurring rurally (X 2 = 159.2, p < 0.001). Similarly, crashes occurring in remote locations compared to regional locations (3.36% vs. 2.35%; X 2 = 256.97, p < 0.001, relative risk = 1.43) were more likely to initiate a request for telemedicine support. Finally, Crash Type (X 2 = 16.878, p < 0.001) and Crash Nature (X 2 = 31.89, p < 0.001) were found to be associated with the use of telemedicine support. A visualization of how different crash variables increases the predicted number of casualties in a crash is presented in Figure 3.
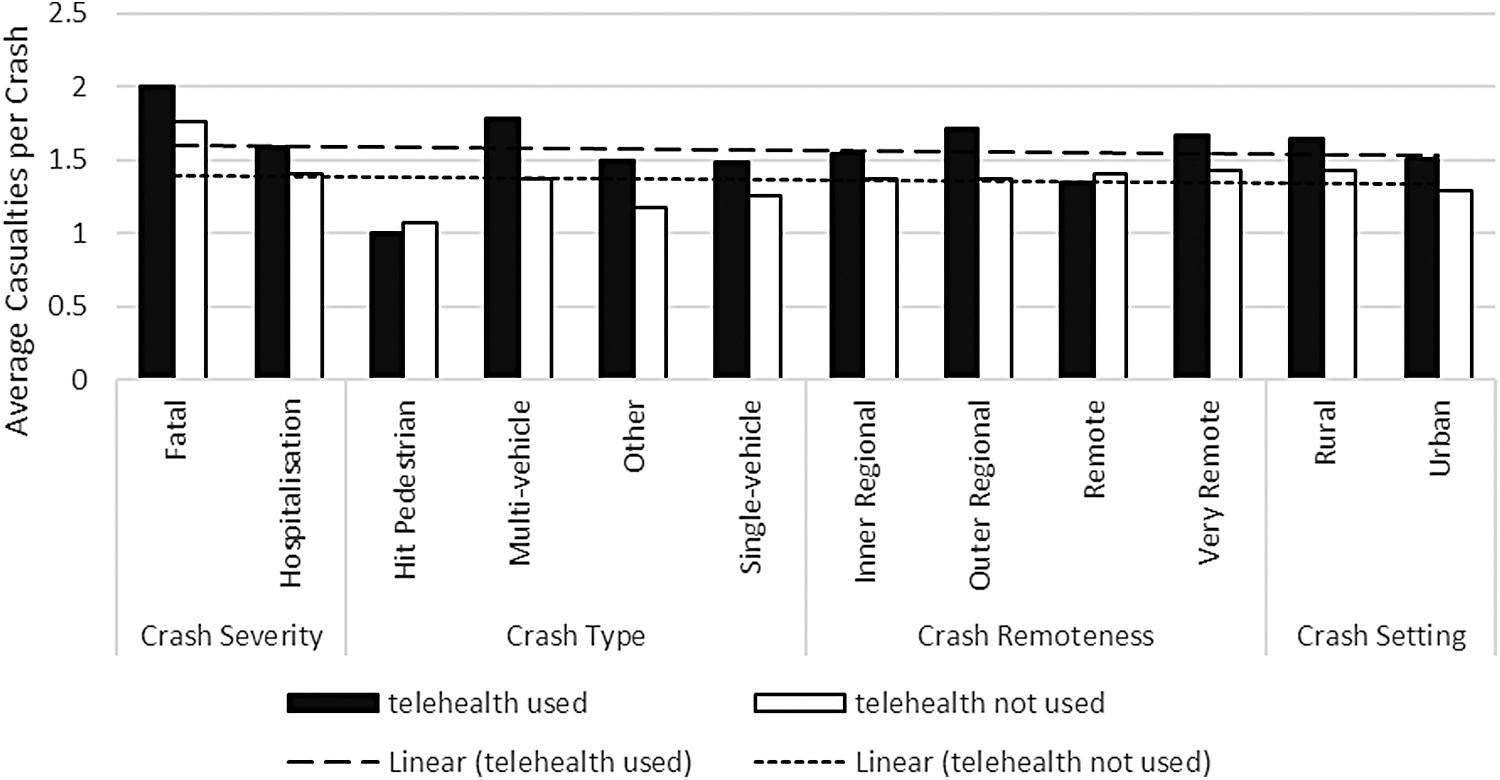
Average casualties per crash by crash variable (telemedicine used vs. not used).
Discussion
Traumatic road crashes are a well-suited subset of hospitalizations to conduct this retrospective study due to the large number of details about each crash that are routinely collected for law enforcement, insurance, and for ongoing safety improvements to the state road network. The collection of crash severity details, for example, makes it possible to establish a correlation between increased complexity and increased likelihood of telemedicine use which previously had not been conclusively established. 3
The results generated in this study support previously observed findings regarding the likelihood of casualties based on the nature of a road crash 19 –21 as well as published literature that describes clinician attitudes toward the value of emergency telemedicine support in the management of complex presentations. 13 –15 The use of emergency telemedicine support in response to a traumatic road crash is associated with a 13% increase in the predicted mean number of casualties. Although a modest effect compared to other crash variables, in particular crash nature, the increased reliance of this telemedicine model in the management of road crashes that involve multiple, severe casualties and take place in rural settings is a strong indication that the model provides benefits to the remote clinical workforce. This benefit is most acutely felt when an emergency presentation threatens to overwhelm staff such as a traumatic road accident managed by a small, rural health service.
Care must be exercised to determine the correct temporal order of this study. Unlike the other variables relating to the severity, nature, and setting of the road crash, the increase in predicted casualties caused using emergency telemedicine models is not the result of individuals being placed at increased risk before the road crash occurring. It is likely that the result of the inclination of clinicians to request this service in the management of road crashes that produce more severe injuries, involve multiple casualties, and take place in more rural settings after they occur. Alternatively put, although a head-on car crash and the use of telemedicine support in the management of a crash are both associated with increased casualties, the former is due to a more dangerous crash nature, while the latter is due to clinicians being more likely to request support for more severe crashes that have occurred.
Emergency telemedicine models of care have been demonstrated to be broadly effective in the management of critical and noncritical presentations as well as delivering additional benefits including reductions in patient retrievals and wait times. This study establishes that in an environment such as a rural health service which experiences frequent low acuity presentations and infrequent high acuity presentations, clinicians do seek support via an emergency telemedicine model to manage a road crash that produce more severe injuries and involve multiple casualties.
Between 1% and 2% of all road crashes that require treatment in Queensland are supported by telemedicine. This number increases when only crashes that occur in remote locations are examined; however, most crashes do not prompt a request for telemedicine support. This may be due to clinicians believing that telemedicine support would not be helpful for all but the most serious crashes or a perception among clinicians that treating injured occupants of a road crash is a situation that they and their colleagues should be independently capable of. If the latter applies, the authors hope that in sharing the results of this study in clinical guidelines and during training on the use of telemedicine will reduce hesitancy to request support when it may be helpful.
Conclusion
Predicting the use of emergency telemedicine support in response to a road crash is a difficult task. Remotely located and isolated clinicians providing initial assessment and treatment to road crash victims may seek collegial support in response to high acuity presentations such as a road crash. This includes the use of emergency telemedicine support when it is available; however, this is not consistently requested. Sharing the patterns of use of emergency telemedicine support models among the rural workforce during telemedicine training and awareness exercises should reduce hesitancy to request telemedicine support when it may be helpful.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.