
Abstract
Background:
This study aimed to demonstrate the technological means used to offer telerehabilitation and to evaluate the effect of physical exercise on the population affected by COVID-19.
Methods:
Clinical trials were searched in the electronic databases Cochrane Library, PubMed/MEDLINE, EBSCO (CINAHL), PEDro, and Web of Science from January 16 to 19, 2023. The effect measure was estimated as mean difference (MD) or standard MD (SMD) with 95% confidence intervals (CI). Subgroup analysis was used to study potential moderating factors.
Results:
Twenty-four articles, describing trials with a total of 1,344 individuals affected by COVID-19, were included in the qualitative synthesis and 14 articles in the meta-analysis. The pooled results revealed that telerehabilitation improves the functional capacity (MD 79.65 [63.57, 95.73]m, p < 0.00001), agility (MD −0.69 [−1.33, −0.04] s, p = 0.04), lower limb strength and endurance (SMD 0.74 [0.52, 0.96], p < 0.00001), forced expiratory volume in 1 s (MD 0.22 [−0.04, 0.49] L, p = 0.10), and dyspnea (SMD −0.94 [−1.64, −0.24], p = 0.009). The dynamic muscular resistance training associated or not with other exercise modalities led to improvements in muscular strength (MD 4.69 [0.44, 8.94] kg, p = 0.03) and fatigue (SMD −0.97 [−1.74, −0.20], p = 0.01). In addition, telerehabilitation showed improvements in the quality of life in the contagious-phase COVID-19 patients. Although this intervention improved inspiratory muscle strength (MD 13.71 [5.41, 22.0] cmH2O, p = 0.001), it did not favor forced vital capacity.
Conclusions:
Telerehabilitation contributed to improving functional capacity, inspiratory muscle strength, physical fitness, and quality of life, and reducing dyspnea and fatigue in COVID-19 adult survivors.
Introduction
In 2019, in the city of Wuhan, a new strain of the virus from the coronavirus family emerged, called SARS-CoV-2, which infected millions of people and, a few months later, was recognized by the World Health Organization as a COVID-19 pandemic. 1
The transmission of this virus occurs especially through the respiratory tract, mainly by droplets from coughing, sneezing, talking, or from contaminated regions and biological substances. 2 Some complications can occur as a result of infection, so that, depending on the degree of severity of the disease and, after clinical recovery, sequelae may remain for a long period. 3 Although the manifestations of COVID-19 are predominantly respiratory, the clinical framework is complemented by signs and symptoms with extrapulmonary involvement 4 that can trigger sequelae, among which the most prevalent in the long term are fatigue, muscle weakness, impaired lung function, dyspnea, stress, anxiety, and neurological and cognitive impairment. 5
With the aim of accelerating the recovery of patients in the acute and postviral phases of this disease, irrespective of whether the individuals were hospitalized or not, and due to the negative impacts on health, actions were implemented to promote rehabilitation of these patients with the help of exercise protocols offered in remote or virtual format. 6 Telerehabilitation began to be used as a strategy for patients with and after COVID-19, with the aim of minimizing health risks and offering supervised rehabilitation in real-time, between therapist and patient, using applications or videoconferencing, or with protocols using asynchronous tracking. 7
Remote rehabilitation makes it possible to perform virtual exercises safely and effectively to develop physical, pulmonary, and/or cognitive capacities for patients with COVID-19 sequelae. 8 To evaluate the effectiveness of telerehabilitation in this population, dome systematic reviews have been carried out. 8,9 The first systematic review with meta-analysis included six studies and suggested that telerehabilitation programs favor improvement in functional capacity, lower limb performance, dyspnea, and the physical component of quality of life, when compared with individuals who did not undergo any rehabilitation. 8 The review of Bernal-Utrera et al. 9 included five studies that evaluated lung function, functional capacity, pain, fatigue, handgrip strength, and physical performance in patients after hospital discharge and/or with sequelae of COVID-19. The authors verified that telerehabilitation with protocols that included aerobic, respiratory, and lower limb muscle strength and endurance exercises with low load appears to be an effective and safe strategy for people with short- and long-term post-COVID-19 sequelae.
Since the publication of these systematic reviews, other studies have proposed to assess the impact of telerehabilitation on different functional, clinical, and mental health outcomes. In this context, the current systematic review has the following three main objectives: (1) to identify the technological means used to offer telerehabilitation to patients affected by COVID-19; (2) to evaluate physical exercise protocols for this population in the acute phase of the disease (contagious phase) and post-COVID-19; and (3) to perform a meta-analysis of randomized clinical trials that evaluated the effect of telerehabilitation on exercise capacity, lung function, fatigue, dyspnea, physical performance, and quality of life in patients affected by COVID-19.
Methods
The study followed the methodological approaches of reporting standards established by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 10 This study was registered in the International Prospective Register of Systematic Reviews: PROSPERO (CRD42022347642).
SEARCH STRATEGY AND SELECTION CRITERIA
This systematic review included single-arm and parallel-arm clinical trials, without language restrictions, that were published from March 2020 to January 2023 in the CINAHL Database|EBSCO, Cochrane Central Register of Controlled Trials (CENTRAL), PEDro Physiotherapy Evidence Database, PubMed/MEDLINE, and Web of Science. The search for articles in databases was carried out between January 16 and 19, 2023. The descriptors extracted from the MESH were “COVID-19,” “Post COVID-19,” “Exercise,” “Telerehabilitation,” and “Tele-rehabilitation,” using the Boolean operators AND/OR (Supplementary Data S1). To structure the eligibility criteria, the PICOS (Patient/Population; Intervention; Comparison; Outcome; Study design) 11 approach was used. Eligible studies for this meta-analysis included those that: (1) Investigated participants aged 18 years or older with COVID-19 or post-COVID-19 (hospitalized or not), with a diagnosis confirmed by reverse transcription polymerase chain reaction (RT-PCR) testing for SARS-CoV-2. (2) Investigated an exercise training intervention via telerehabilitation lasting for at least 1 week. (3) Compared the telerehabilitation group with the control group without exercise, such as usual care, face-to-face rehabilitation, or no treatment. (4) Examined primary outcomes such as functional capacity determined by the 6-minute walk test (6MWT); muscular strength and endurance determined by the sit-to-stand test (STST); muscle strength assessed by handgrip dynamometer; lung function evaluated by forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC), both measured by spirometry; respiratory muscle strength based on the maximum respiratory pressure test and measured by manovacuometry or PowerBreathe; and quality of life determined by any validated instrument. Secondary outcomes included dyspnea determined by the modified Medical Research Council (mMRC) Scale and Multidimensional Dyspnea 12 Scale (MD12), and fatigue determined by the Fatigue Severity Scale (FSS), Visual Analog Fatigue Scale (VAFS), or Borg Scale. (5) Included randomized controlled trials (RCTs), non-RCTs, and quasiexperimental studies published in peer-reviewed journals. Review studies, meta-analyses, observational studies, books/chapters, and studies published in the proceedings of scientific events were excluded.
Two independent reviewers (R.L.M. and E.S.S.M.) were responsible for selecting the articles included in the Rayyan platform (https://www.rayyan.ai/). Initially, the duplicate articles were identified and excluded, and subsequently, the selection of articles was performed blindly by the reviewers, based on the evaluation of titles and abstracts considering the eligibility criteria and, in cases where the information presented was insufficient, the complete text was checked. After each reviewer independently selected the studies, blinding was removed to assess possible disagreements between the two reviewers about the studies, and when necessary, a third reviewer (M.S.B.S.) was invited to participate in the final decision. After defining the articles eligible for the systematic review, the full reading was carried out to assess the quality of the studies and collect information for presenting the results and constructing the meta-analysis.
STUDY SELECTION AND DATA EXTRACTION
Data extraction was performed by two reviewers (R.L.M. and E.S.S.M.) and verified by a third reviewer (M.S.B.S.). Information on health status (COVID-19 or post-COVID-19), study design (single-arm and parallel-arm clinical trials), technology used to offer remote rehabilitation, participant information (number of subjects, age, sex, BMI), instruments used to assess outcomes, and main outcomes are given in Table 1. The characteristics of the telerehabilitation protocol offered to the participants, such as the type of exercise, intensity, frequency of sessions (days/week), and duration (weeks) are shown in Table 2.
Demographic Data of the Subjects from the Included Studies
*median (IQR); ↑: Increase; ↓: Decrease; ↔: Maintenance.
RCT, randomized controlled trials; N-RCT, nonrandomized controlled trials; 6MWT, 6-minute walking test; LLMSE, lower limb muscle strength and endurance; TUG test, Timed Up-and-Go test; IMT, inspiratory muscle training; RMT, resistance muscle training; SGRQ, the St George’s Respiratory Questionnaire; NHP, The Nottingham Health Profile; y, years; 30STST, 30-second Sit-To-Stand Test; 1-STST, 1-minute Sit-To-Stand Test; CVF, forced vital capacity; FEV1, forced expiratory volume in 1 s; BBS, Berg Balance Scale; ABC, activities-specific balance confidence; SF-12, Short Form 12 item; SF-36, Short Form 36 item; MD12, Multidimensional Dyspnea-12; mMRC, Modified Medical Research Council; VAFS, Visual Analog Fatigue Scale; FSS, The Fatigue Severity Scale.
Telerehabilitation Protocol Parameters and Effects of Exercise on Functional Capacity, Pulmonary Function, Dyspnea, Fatigue, Physical Fitness, and Quality of Life in the Included Studies
*Median (IQR).
W, walking; c, cycling; r, running; s, swimming; a, auto walk; s, seconds; min, minutes; m, meter; HRR, heart rate reserve; MIP, maximal inspiratory pressure; DMRT, dynamic muscular resistance training; IMT, inspiratory muscle training; EMT, expiratory muscle training; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; PCS, physical component score; MCS, mental component score; SPPB, Short Physical Performance Battery; VPT, virtual physical therapy; HPT, home in-person physical therapy; IE, independent exercise; None, referred to physical therapy but did not attend.
STUDY QUALITY/REPORTING AND LEVEL OF EVIDENCE
The methodological quality of the studies was assessed using the Tool for the Assessment of Study Quality and Reporting in Exercise (TESTEX) Scale. 36 This scale contains two sections, denominated study quality and reporting. The final score ranges from a minimum of 0 to a maximum of 15 points, where higher scores indicated better study quality (0–5 points) and reporting (0–10 points). To analyze the level of evidence of the studies, the GRADE scale was used, following the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions 37 . This scale evaluates factors such as risk of bias, inconsistency, indirectness, and imprecision, classifying studies into the following four levels: high, moderate, low, and very low. These assessments were conducted independently by two reviewers (RLM and ESSM) for outcomes related to telerehabilitation.
DATA ANALYSIS
This meta-analysis used Review Manager Software (RevMan 5.4) and analyses were carried out to measure the between-trial standard mean difference (SMD), mean difference (MD), and 95% confidence intervals (95% CI). The SMD and MD were calculated using the postintervention outcome mean, standard deviation (SD), and sample size for the telerehabilitation (experimental) and nontelerehabilitation (control) groups. When these metrics were not reported, the authors were contacted. 14,23,30,34,35 If a study had more than one experimental group, separate meta-analyses were performed. 16,21,32 The effect size (ES) of the SMD or MD was classified as large (>0.8), moderate (0.5–0.8), small (0.2–0.5), or trivial (<0.2). The consistency between studies was evaluated by the I 2, and the risk of heterogeneity was categorized as low [I 2 < 25%], moderate [I 2 = 25–75%], and high [I 2 > 75%]. 38 Sensitivity analyses were conducted by excluding one study at a time to test the robustness of the combined results. These analyses were performed on results with an I 2 greater than 50%. Due to the high heterogeneity, studies with diverse population characteristics and/or a higher risk of bias were removed from the pooled analysis (Supplementary Data S3). Testing for an overall effect (Z score) was significant when p < 0.05. A random-effects model with I 2 statistics was used and a meta-analysis was performed. The fixed-effect model was used when heterogeneity was low and the randomized effect model was used when heterogeneity was moderate or high. To examine possible variables that may have affected training effectiveness, subgroup analyses were also performed based on health status, type of intervention, and time of intervention.
Results
STUDY SELECTION
A flowchart describing the selection process is shown in Fig. 1. Our initial database search identified 4,408 potentially eligible articles. Following the screening of titles and abstracts, 3,598 articles were excluded, and based on the inclusion criteria, 51 potentially eligible articles were identified and three studies were included from the author library. After reviewing the full content of these articles, 30 were excluded for not meeting the eligibility criteria. Finally, 24 articles satisfied the inclusion criteria.
Flowchart of the rewiew.
CHARACTERISTICS OF THE INCLUDED STUDIES
The characteristics of the studies included in the systematic review and meta-analysis are summarized in Tables 1 and 2. The trials were conducted in Spain (n = 9), 12,13,16,18,19,24,31 –33 Italy (n = 2), 17,29 Turkey (n = 2), 30,34 the United States (n = 2), 14,21 Belgium (n = 1), 25 Brazil (n = 1), 35 Greece (n = 1), 22 the Islamic Republic of Iran (n = 1), 26 Netherlands (n = 1), 20 Peru (n = 1), 28 the Republic of Chile (n = 1), 15 the Republic of China (n = 1), 23 and the United Kingdom (n = 1). 27
Twenty-four studies were included in this systematic review, 16 evaluating post-COVID-19 patients 12,15 –18,20 –25,27 –30,33 –35 and eight with patients in the acute phase of COVID-19 (contamination phase). 19,21 –24,26,31,32
The total number of participants was 1,344 (600 male, 744 female) with a median sample size of 56 participants per study (range 15–148). Participant age ranged from 21 to 70 years (median 52.5 years). The median duration of the studies was 6 weeks (range 1–12 weeks). The study by Rodriguez–Blanco et al. (2022) included participants with a lower mean age (34.8 ± 11.8 years) and Martin et al. (2021) included the highest age range (61.9 ± 10.7 years).
Regarding the study design, eight studies included one experimental group 12,13,15,18,20,22,29,31 and 16 were parallel-arm studies. 14,16,19,21,23 –28,30 –35 Of these parallel-arm studies, 13 included two experimental groups, 14,19,23 –28,30,31,33 –35 one included three experimental groups, 32 and two studies included four experimental groups. 16,21
TECHNOLOGY USED TO PROVIDE REHABILITATION AND STRATEGY USED TO ASSESS THE OUTCOMES
Ten studies used videoconferencing to offer telerehabilitation, 13,16,20,21,24,25,27,30 –33 five studies used specific apps and/or software, 17,18,20,23,28 , three studies used video-chat or video-call with a leaflet on a specific platform, 12,26,29 two studies used WhatsApp, YouTube videos, and/or e-mail, 34,35 two studies made use of Smartphones for calls or application of this equipment, 15,22 and one study used the Video-Health in Motion Application. 14 In 13 studies, the rehabilitation protocol was monitored 13,14,16,18,21,22,24 –26,30 –32 with two of them being monitored by a physical therapist, 21,22 while in seven studies there was no monitoring. 15,20,23,27,29,34,35 When it was necessary, telemonitoring was used only during certain sessions of the rehabilitation protocol. 12,17,19,28 Regarding outcome measures, most were assessed in person 14 –16,18,23 –26,28,34,35 in the hospital, 14,17,25,28 laboratory, 35 office, 26 or remotely, 12,21,27,29 –33 using specific platforms, 12 telephone calls, 19 video calls, 27,31 –33 or videoconference. 30 Some studies did not report at all. 13,20,29
STUDY QUALITY AND REPORTING AND PUBLICATION BIAS
The results of the quality assessment are presented in Supplementary Data S2. The average score on the checklist was nine points (range 1–14). Thirteen studies presented between 11 and 14 points 14,16,21,23 –25,27,28,31 –35 six studies between 6 and 10 points, 15,18,22,26,30 and six between 1 and 5 points. 12,13,17,20,21,29
The lowest score assigned was 1 point, 12 and the highest score was 14 points 16 (representing 93.3% of the total TESTEX score). No randomized clinical trials attained the maximum score. Some essential methodological criteria were identified in the studies included in the meta-analysis, such as lack of information about the groups at baseline, 12,13,15,17 –22,24,26,30,31 lack of information on evaluator blinding in at least one of the outcomes 12,13,15,17,20 –22,25 –29 or on the monitoring of activities in the control group, 12,13,15,16,18 –35 lack of information on the intensity 12,13,20,26,30,31 or volume of training, 13,14,17,20,29,30 not reporting sample losses or losses greater than 15%, not informing how the telemonitoring of participation in the exercise protocol was performed, and not reporting adverse events. 12,17
LEVEL OF EVIDENCE AND SENSITIVITY ANALYSIS
The study evaluated the level of evidence for outcomes favoring telerehabilitation in pooled results, including functional capacity, agility, dyspnea, lower limb muscle strength and endurance, and maximum inspiratory strength. The results are presented in Fig. 2 (panels A, B, and D), Fig. 3 (panel C), and Fig. 5 (panel A). Functional capacity and agility presented a moderate level of evidence, while dyspnea, lower limb muscle strength and endurance, and maximum inspiratory strength were considered to have a high level of evidence.
Changes in functional capacity (6MWT; Panel A), agility (Panel B), muscular strength (Panel C) and lower limb muscle strength and endurance (Panel D) between telerehabilitation and control groups in the randomized controlled trials.
Forest plot showing the effect of telerehabilitation on forced expiratory volume in 1 second (Panel A), forced vital capacity (Panel B) and maximum inspiratory pressure (Panel C) between telerehabilitation and control groups in the randomized controlled trials.
For the sensitivity analysis, four studies 26,28,30,35 were excluded from the pooled analysis due to high heterogeneity: mean BMI > 30 kg/m2, 28,35 TESTEX score < 10 points, 26 and high age range. 30 The best results in functional capacity heterogeneity were obtained when one study 26 was excluded (I 2 = 52% to I 2 = 50%). The heterogeneity of dyspnea also decreased (I 2 = 89% to I 2 = 74%) with the exclusion of two studies. 28,30 The heterogeneity of FEV1 showed a significant change from I 2 = 63% to I 2 = 0% when one study 28 was removed. Similarly, when three studies 26,28,35 were excluded from the pooled analysis, the FVC heterogeneity had a greater change (I 2 = 63% to I 2 = 0%). In addition, a significant reduction in quality-of-life heterogeneity was observed when one study 28 was excluded from the combined analysis (I 2 = 91% to I 2 = 25%). The degree of evidence and sensitivity results are presented in Supplementary Data S3.
CHARACTERISTICS OF TELEREHABILITATION PROTOCOL
The studies used different intervention protocols. Three studies used only respiratory training, 15,16,18 seven studies associated respiratory training with dynamic muscular resistance training (DMRT) 12,21,22,26,30,32,33 or with aerobic training, 13,28 and six studies associated aerobic, respiratory, and DMRT. 14,17,18,23,24,30 Aerobic training associated with dynamic muscular resistance was evaluated in three studies, 20,29,35 and two studies performed only DMRT 25,31 or associated with balance training. 24
To assess exercise intensity in aerobic and/or dynamic muscular endurance exercise protocols, nine studies used the Borg Scale, 12,15,19,22,25,30 –32,35 three studies used the Modified Borg Scale, 24,28,34 one study reported between 30% to 60% heart rate reserve, 23 one study used weekly load increments between 5% and 10%, 18 one study was based on the Short Physical Performance Battery, 29 and seven did not inform how exercise intensity was evaluated. 13,14,17,20,26,33 The studies that performed respiratory training used the limit of 80% of the sustained maximal inspiratory pressure in three consecutive breaths 27 or a weekly increase of 10% of the load, 16 and two studies did not report how the training intensity increment was performed. 28
The number of weekly training sessions ranged from two 25 to seven times a week. 19,21,28,31 –34 The studies by Gonzalez-Gerez et al. (2021) 19 and Rodriguez-Blanco et al. (2021) 31 included the intervention protocol with the shortest duration (1 week), whereas the studies by Teixeira do Amaral et al. (2022) 35 and Capin et al. (2022) 14 used the protocol with the longest intervention time (12 weeks).
THE EFFECT OF EXERCISE TRAINING BY TELEREHABILITATION
Functional capacity (6MWT)
Twelve studies evaluated functional capacity using the 6MWT. 13,19,20,23,26,28,29,31 –35 Calvo-Paniagua et al. (2022) 13 presented the greatest change in distance covered from pre- to postintervention (560.1 ± 98.9 m, 699.7 ± 57.2 m). The study included an aerobic training protocol associated with respiratory training lasting 40 min per session, 3×/week, for seven weeks.
Data synthesis from telerehabilitation trials revealed significant improvements in functional capacity with exercise (fixed effect: MD 79.65 [63.57, 95.73] p < 0.00001). However, these studies were characterized by significant heterogeneity (X2 = 18.62, I 2 = 52%) (Fig. 2, panel A). Furthermore, the subgroup analysis showed similar modifications in functional capacity after interventions for >5 weeks or <2 weeks with telerehabilitation, and both analyses presented reduced heterogeneity (I 2 = 0%, p = 0.0006; I 2 = 6%, p = 0.00001, respectively) (Table 3). In addition, significant differences were observed for both intervention types, such as respiratory training only and DMRT alone or combined with other exercise modalities (fixed effect: MD 99.10 [42.66, 55.54], I 2 = 0%, p = 0.0006; 77.94 [61.16, 94.71], I 2 = 61%, p < 0.00001) and disease status, such as acute phase and post-COVID-19 (fixed effect: MD 78.20 [58.68, 97.71], I 2 = 30%, P = <0.00001; 80.70 [54.97, 106.43], I 2 = 74%, p < 0.00001) (Table 3).
Subgroup Analyses of the Effect of Telerehabilitation on Pulmonary Function, Functional Capacity, Muscular Strength, Lower Limb Muscle Strength and Endurance, Dyspnea, Fatigue, and Quality of Life According to Intervention Time or Type, and COVID-19 Status of the Included Participants
Trial or participant number.
*Respiratory, balance, agility, and/or aerobic training.
DMRT, dynamic muscular resistance training; 6MWT, 6-minute walking test; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity.
Physical fitness (strength, endurance, balance, and agility)
Five studies assessed muscular strength across maximum voluntary contraction using a handgrip dynamometer (Table 1). 16,20,24,34,35 Data synthesis from telerehabilitation RCTs (224 participants) revealed a nonsignificant improvement in muscular strength (MD 2.68 [−0.19, 5.55], X2 = 2.22, I 2 = 0% heterogeneity, p = 0.07] (Fig. 2, panel C). Moreover, subgroup analyses showed significantly greater improvement in muscular strength after excluding the studies with only a respiratory intervention protocol (4.69 [0.44, 8.94], X2 = 0.51, I 2 = 0% heterogeneity, p = 0.03] (Table 3).
Eight studies evaluated lower limb muscle strength and endurance using the 30STST tool, 14,17,19 –21,24,31 –34 and six studies with the 1-STST and/or 3-minute step test, 15,16,18,22,25,29 (Table 1). The meta-analysis of telerehabilitation studies (399 participants) demonstrated significant improvement in lower limb muscle strength and endurance (SMD 0.74 [0.52, 0.96], X2 = 8.87, I 2 = 10% heterogeneity p < 0.00001) (Fig. 2, panel D).
Balance was assessed in two studies, which used the Activities-Specific Balance Confidence Scale 14 and the Berg Balance Scale (BBS) 17 (Table 1). Agility was evaluated in four studies by the Timed Up-and-Go test (TUG test). 14,17,20,30 Data synthesis from RCTs (110 participants) revealed a significant improvement in agility with combined training (aerobic and resistance exercise) (MD −0.69 [−1.33, −0.04], X2 = 0.41, I 2 = 0% heterogeneity, p < 0.04) (Fig. 2, panel B).
Pulmonary function and respiratory muscle strength
Four studies assessed lung function. 16,23,26,28,35 Del Corral et al. (2022) 16 observed no significant difference in pre- versus postintervention for the FVC in the experimental group (3.8 ± 0.7 L; 3.9 ± 0.8 L, respectively) and control group (4.0 ± 1.0 L; 4.0 ± 0.9 L). A similar finding was verified for FEV1, with a mean difference of 0.1 L for the experimental group and −0.1 L for the control group. In the study by Mashhadi et al. (2022), 26 the experimental group had an increase in FVC of 2.15 L and FEV1 of 0.93 L, whereas in the control group it was 0.34 L and 0.06 L, respectively. In the study of Okan et al. (2022), 28 there was an increase for all pulmonary function parameters in the experimental group and a decrease for the control group. Differently, Teixeira do Amaral et al. (2022) 35 reported that FVC and FEV1 increased similarly in the experimental and control groups.
In the five trials that assessed pulmonary function (318 participants), absolute changes in FEV1 [random effect: MD 0.22 [−0.04, 0.49], X2 = 11.09, I 2 = 55% heterogeneity, p = 0.10] and FVC [random effect: MD 0.29 [−0.07, 0.65], X2 = 13.66, I 2 = 63% heterogeneity, p = 0.12] did not reach statistical significance (Fig. 3, panels A and B). In the subgroup analysis, pulmonary function also showed nonstatistical significance for intervention time and disease status (Table 3).
The maximum inspiratory strength was evaluated in two studies. Del Corral et al. (2022) 16 observed that both the inspiratory muscle training and resistance muscle training (RMT) groups in relation to the respective control groups presented differences in the maximum inspiratory pressure of 16.2 cmH2O and 20.4 cmH2O, respectively. Similar results were observed by McNarry et al. (2022), with an increase of 27.4 cmH2O for the experimental group and 7.7cmH2O for the control group.
Data synthesis (236 participants) showed that telerehabilitation had a significant effect on increasing the inspiratory muscle strength evaluated by maximum inspiratory pressure [fixed effect: MD 13.71 [5.41, 22.00], X2 = 0.68, I 2 = 0%, p = 0.001] (Fig. 3, panel C).
Quality of life
Quality of life was assessed in nine studies, three using the St George’s Respiratory Questionnaire (SGRQ), 13,28,30 one study used the EuroQol-5D Questionnaire, 16 two studies used the SF-36, 15,22 two studies the SF-12, 20,23 and one study used the Nottingham Health Profile (NHP). 34 Data analysis from telerehabilitation exercise trials (556 participants) showed nonsignificant improvement in quality of life (random effect; SMD −0.15 [−0.82, 0.52], X2 = 63.57, I 2 = 91%, p = 0.66), with significant heterogeneity between studies (Fig. 4).
Changes in quality of life between telerehabilitation and control groups in the randomized controlled trials.
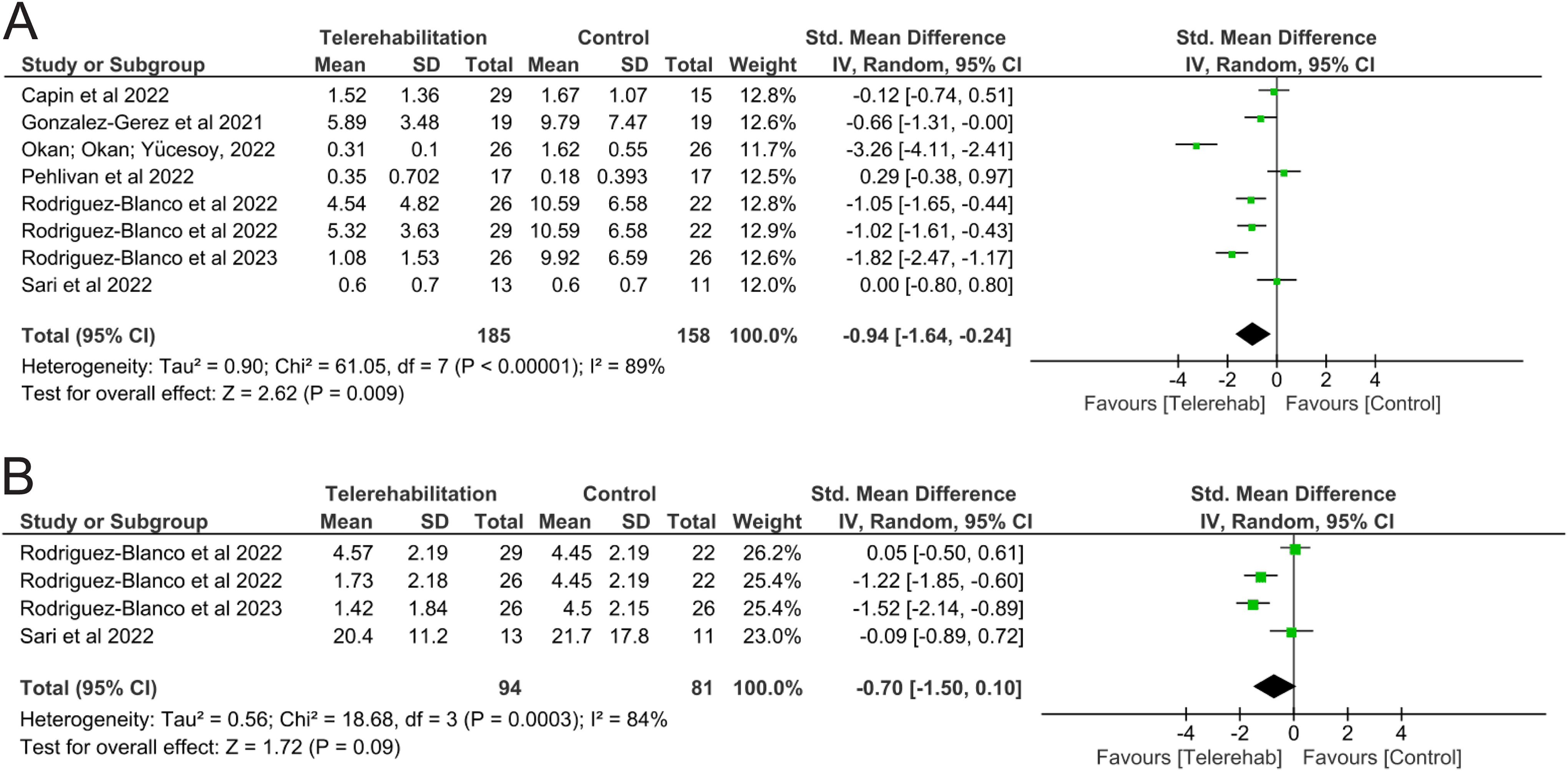
Changes in dyspnea (Panel A) and fatigue (Panel B) between telerehabilitation and control groups in the randomized controlled trials.
Subgroup analyses of telerehabilitation studies showed nonsignificant differences for intervention time (random effect: SMD 0.34 [−0.30, 0.99], I 2 = 56%, p = 0.29; −0.37 [−1.29, 0.56], I 2 = 93%, p = 0.44) Differently, for disease status, it was shown that telerehabilitation favors improvement in quality of life in participants with COVID-19 (random effect: SMD 0.39 [0.13, 0.64], I 2 = 0%, p = 0.003) but nonsignificant in post-COVID-19 (SMD: −0.41 [−1.53, 0.71], I 2 = 93%, p = 0.48) (Table 3).
Fatigue and dyspnea
Dyspnea was studied in 12 studies, which used the Borg Scale and/or mMRC Dyspnea Scale 13 –15,22,23,28,30,34 or MD12 Scale 19,32 or Barthel Dyspnea Index. 29 Telerehabilitation was able to reduce dyspnea in 9 studies, 13,15,19,28 –30,32,33 while 3 studies did not find improvement in this outcome. 14,22,23
Data synthesis from telerehabilitation RCTs (343 participants) revealed a significant improvement in dyspnea (random effect: SMD −0.94 [−1.64, −0.24], X2 = 61.05, I 2 = 89%, p = 0.009] (Fig. 5, panel A). Subgroup analyses for the respiratory intervention-only protocol showed significant improvement in dyspnea (random effect: MD −4.72 [−7.07, 2.36], X2 = 0.31, I 2 = 0%, p = 0.0001) (Table 3) as well as in the acute phase of COVID-19 patients [MD −5.16 [−7.08, 3.24], I 2 = 0%, p < 0.00001] (Table 3).
Fatigue was assessed in seven studies. 12,15,20,30,32 –34 Of these studies, four were RCTs that were used in the meta-analysis (Table 1). Rodriguez–Blanco et al. (2022; 2023) 32,33 and Pehlivan et al. (2022) 30 evaluated fatigue using the Visual Analog Scale and found a reduction in this outcome only in the experimental group. Sari et al. (2022) 34 assessed fatigue using the FSS and observed improvement in both the experimental and control groups. A meta-analysis of telerehabilitation studies (175 participants) demonstrated nonsignificant improvement in fatigue (random effect, SMD −0.70 [−1.50, 0.10], X2 = 18.68, I 2 = 84% heterogeneity p = 0.09) (Fig. 5, panel B). In the subgroup analyses, when the groups that performed a respiratory intervention only were excluded, 32 a significant reduction was observed in fatigue (random effect, SMD −0.97 [−1.74, −0.20], X2 = 7.77, I 2 = 74% heterogeneity p = 0.01). No differences were observed according to disease status, such as acute COVID-19 (random effect, SMD −0.58 [−1.83, 0.68], I 2 = 89% heterogeneity, p = 0.37) and post-COVID-19 (random effect, SMD −0.82 [−2.23, 0.58], I 2 = 87% heterogeneity, p = 0.5) (Table 3).
PARTICIPANT ADHERENCE TO TELEREHABILITATION PROGRAMS
Fifteen studies reported more than 85% adherence to the telerehabilitation protocol, 14,16,18 –20,24 –26,28,29,31 –34,38 of which 10 were RCTs, 14,16,19,24,26,28,31 –34 4 were single-arm studies, 13,18,20,29 and 1 was a non-RCT. 25 On the contrary, seven studies reported adherence of less than 85%, 15,17,23,27,29,30,35 of which four were RCTs 23,27,30,35 and three were single-arm studies. 15,17,29 Adherence rates were as 84%, 30 80%, 17 77%, 15 and 75%, 23 with lowest rates reported in three trials 15,22,35 (64%, 56%, and 50%, respectively). Two studies did not report adherence to telerehabilitation protocols. 21,32
Discussion
The current systematic review presented the technological means that were used by the studies to offer telerehabilitation, and evaluated the physical exercise protocols for this population with and after COVID-19 to evaluate the effect of telerehabilitation on the outcomes of functional capacity, physical fitness, respiratory, fatigue, dyspnea, and quality of life in patients affected by COVID-19.
Monitoring of intervention protocols was supervised and/or individualized in most trials, using videoconferencing and video calls as technological tools. The format of the outcome assessment varied from face-to-face, conducted in hospital, office, or laboratory settings, and remote assessments were carried out through video calls, videoconferencing, telephone calls, and application of a specific platform. Instead of offering a rehabilitation protocol to a COVID-19 patient, a strategy was used to aid in improving the functional capacity, inspiratory muscle strength, lower limb strength and endurance, and dyspnea. The improvement in fatigue, handgrip strength, and FEV1 depends on exercise modalities performed by participants.
Based on the data synthesis, this meta-analysis showed that telerehabilitation encompassing several training protocols, without considering the duration of the intervention and the status of the disease, was favorable for improving functional capacity (I 2 = 52%, moderate heterogeneity; p < 0.00001), inspiratory muscle strength (I 2 = 0%, low heterogeneity; p = 0.001), lower limb muscle strength and endurance (I 2 = 10%, low heterogeneity; p < 0.00001), agility (I 2 = 0%, low heterogeneity, p = 0.04), and dyspnea (I 2 = 89%, high heterogeneity; p = 0.009). However, it was not favorable for lung function (FEV1 [I 2 = 66%, moderate heterogeneity; p = 0.21]; FVC [I 2 = 69% moderate heterogeneity, p = 0.16], muscular strength (I 2 = 0%, low heterogeneity; p = 0.07), fatigue (I 2 = 84%, high heterogeneity; p = 0.09), and quality of life (I 2 = 91%, high heterogeneity; p = 0.05).
To assess the type or time of intervention, as well as the status of the disease (intervention offered to patients in the contagious phase of COVID-19 and in the post-COVID-19 phase), subgroup analyses were performed in the meta-analysis (Table 3). In the assessment of functional capacity assessing the status of the disease, telerehabilitation was favorable to improve the distance covered, both in patients who were in the contagious phase of the disease and post-COVID-19 (I 2 = 30%, moderate heterogeneity; p < 0.00001; I 2 = 74%, high heterogeneity; p < 0.00001). In the subgroup analysis on the offer of the intervention, it was verified that telerehabilitation was favorable to improve the distance covered, with intervention lasting ≤2 weeks (p = 0.00001) or ≥5 weeks (p = 0.00001), both analyses with low heterogeneity (I 2 = 6%; I 2 = 0%, respectively).
Regarding the type of intervention, telerehabilitation was favorable to improve the distance covered, both in studies that performed isolated respiratory intervention (I 2 = 0%, low heterogeneity; p = 0.0006) 19,32 and in studies that used DMRT alone or associated with other interventions (respiratory, aerobic, agility, and/or balance), with moderate heterogeneity (I 2 = 61%, p < 0.00001). Similar results were observed in a previous meta-analysis, which demonstrated that combined exercises (assessed in four studies) or breathing exercises in isolation (assessed in two studies) delivered via telerehabilitation improved the distance covered in the 6MWT (MD 101 m [61, 141]; MD 62 m [42, 82], respectively). 10
Similar to the assessment of lung function with clustered physical interventions, in the subgroup analysis from six evaluated studies, there is no significant difference in FVC, either related to the type of intervention or the status of the disease. This finding should be viewed with caution, as two to three studies were pooled for each assessment for this analysis (Table 3). There was a significant difference in FEV1 when participants performed DMRT alone or associated with other interventions (I 2 = 66%, p = 0.004). Improvement was observed in the strength of the inspiratory muscles (I 2 = 0%, low heterogeneity; p = 0.001), although it was not possible to perform subgroup analysis.
In the subgroup analysis, assessing the impact of the type of intervention on muscle strength using handgrip strength, it appears that telerehabilitation offered by DMRT alone or associated with other interventions was able to significantly increase this outcome (I 2 = 0%, low heterogeneity; p = 0.03), without being favorable to protocols with isolated breathing exercises (I 2 = 0%, low heterogeneity; p = 0.62). This subgroup analysis shows the importance of working on various systemic components to improve physical capabilities, which has been recommended by the American College of Sports Medicine regarding the prescription of physical exercises, 39 A randomized clinical trial, which used functional training (which comprises the association of aerobic exercises, muscular endurance, agility, balance, and power) via telehealth technological resources, verified improvement in muscle strength with a handgrip dynamometer in post-COVID-19 patients. 40
In the subgroup analysis of physical fitness components, it was verified that the exercise protocols with remote monitoring were favorable to increase lower limb muscle strength and endurance with respiratory protocols (I 2 = 0%, p = 0.00001) or DMRT alone and/or combined with other exercise modalities (I 2 52%, moderate heterogeneity; p= 0.0006), for participants with COVID-19 (I 2 0%, p < 0.00001) or post-COVID-19 (I 2 = 51%, moderate heterogeneity; p = 0.001). Similar results were observed by Vieira et al. (2022), who showed improvement in lower limb muscle strength and endurance performed by the 30-second STST via telerehabilitation in breathing exercises (2.2 repetitions [1.5, 2.8]; two studies) and other exercise protocols (2.0 repetitions [1.3 to 2.7]; two studies).
Telerehabilitation enabled improvement in dyspnea for protocols with breathing exercises (I 2 = 0%, low heterogeneity; p = 0.0001) and in people who were in the contagious phase of COVID-19 (I 2 = 0%, low heterogeneity; p < 0.00001). A previous meta-analysis showed that breathing exercises in isolation (two studies) delivered via telerehabilitation reduced dyspnea by the MD12 questionnaire scores (–6.0 [–7.0, –5.0]). Similar results showed that DMRT associated or not with other exercise protocols significantly reduced fatigue (I 2 = 74%, p = 0.01), but disease status was not impacted (Table 3). Fatigue and dyspnea are two important symptoms of people affected by COVID-19, however, there are some factors that affect the appearance and continuation of these symptoms, such as age, disease status, comorbidities, and level of physical activity. 41 –43 Previous studies have shown that COVID-19 predisposes to fatigue due to muscle damage, whether from immobilization, corticosteroid therapy, or catabolic effects, 44,45 and dyspnea leads to greater impairments in pulmonary gas exchange. 46 In this sense, this meta-analysis identified that the type of intervention can be directed based on the symptoms presented by the patient, since fatigue was reduced after the DMRT protocols associated or not with other physical interventions, while dyspnea was also reduced in the protocols that included only breathing exercises.
Regarding quality of life, the subgroup analysis showed that neither interventions offering protocols with breathing exercises (I 2 = 56%, moderate heterogeneity; p = 0.29) or those with DMRT alone or associated with other physical interventions (I 2 = 93%, high heterogeneity; p = 0.44) favored the improvement in the quality of life. Similar results were found regarding disease status in the post-COVID-19 phase (I 2 = 93%, high heterogeneity; p = 0.48), but the offer of telerehabilitation in the contagious phase was able to improve the quality of life (I 2 = 0%, low heterogeneity; p = 0.003). This result should be evaluated with caution, since this outcome was evaluated based on the physical and mental component of the study by Li et al. (2022). 23 A previous review concluded that the quality of life is compromised in patients with COVID-19, having a greater impact in patients who were in the acute phase (confirmed or suspected) than with long-term COVID. In addition, other factors can affect this outcome, such as age and comorbidities, and the impact does not reduce considerably over time (i.e., even two months after the illness). 47
Many COVID-19 survivors may develop sequelae related to the consequences of organ or tissue damage caused by SARS-CoV-2. 48 Previous studies have reported several deficiencies in the musculoskeletal, respiratory, and cardiovascular systems that may reduce their quality of life and well-being. 49 To ameliorate these disabilities, rehabilitation strategies have been proposed to improve the physical and mental health of this population, especially through the use of telerehabilitation 9,10,15 and telemonitoring. 15,20,23,27,29,34,35 It is known that SARS-CoV-2 causes mitochondrial dysfunction in muscle cells, resulting in reduced energy production and persistent fatigue, 50 which affects the body and may promote or increase sedentary behavior. In this sense, the “musculoskeletal system” seems to be the main point connecting the meta-analysis results.
Since the aerobic capacity required during the 6MWT depends on the ability to deliver oxygen to the muscles and use it to generate energy, 51 muscular deficiency will affect physical performance. On the contrary, the provision of regular physical exercise leads to local adaptations in skeletal muscle, such as increased mitochondrial biogenesis and capillary density, which enhance the body’s ability to transport oxygen and use it to generate energy. 52 Therefore, it is logical to assume that improving aerobic capacity and respiratory and peripheral muscle strength through exercise will promote a reduction in symptoms of dyspnea in people affected by COVID-19.
Some limitations regarding the offer of telerehabilitation were pointed out in some of the randomized clinical trials included in this meta-analysis. Capin et al. (2022) 14 cited that a major confounding factor in their study was that individuals in the control group had access to the Health in Motion app, including functional tests. Li et al. (2021) 23 emphasized the importance of considering that an intervention may not be suitable for people with disabilities and very severe sequelae of COVID-19, as well as for those who are not familiar with Smartphone technology. These factors result in sample loss, and limitations on the possibility of potential benefit from social interaction. Another interesting evaluation point reported in the study by Mashhadi et al. (2022) 26 suggests that protocols offered via telehealth technology, with respiratory and systemic exercises, can be used to assess the effect of rehabilitation and monitor the lasting symptoms of COVID-19 survivors who were discharged from hospital.
McNarry et al. (2022) 27 reported difficulties in contacting many of the participants to find out why they withdrew from the study. Despite the dropout rate in this study being higher than what is commonly reported in interventions that precede the pandemic, as this is the only situation in which the interventions were delivered remotely, comparisons with prepandemic interventions are impossible. Okan et al. (2022) 28 reported that during the telemedicine process, saturation and heart rate values were not evaluated due to financial constraints in relation to available technologies. Pehlivan et al. (2022) 30 identified problems related to the internet and difficulties in using technical devices. Rodriguez-Blanco et al. (2022; 2023) 32,33 pointed out that remote assessments have the disadvantage of the dependence of the researcher with regard to the participants’ self-assessment. Consequently, these results may not be extrapolated to some populations, especially those who may face difficulties in dealing with these tools, such as older people. Finally, it is important to consider the methodological quality of the studies. Eight studies did not have a control group, which made it impossible to perform radomization and allocation secrecy. In addition, the lack of blinding of assessors for at least one key outcome contributed to the low quality of these studies. On the contrary, the study quality was considered good in 14 clinical trials (13 RCTs; 1 non-RCT), indicating a low risk of bias.
Despite the limitations pointed out by the studies included in this systematic review, the results show that telerehabilitation is a therapeutic strategy to serve the population with assistance protocols, treatments, and follow-ups, especially those who are geographically distant from the health networks offered by the public or private system or those who are physically unable to attend. Although 24 studies were included in this systematic review, and 14 randomized clinical trials were included in the meta-analysis, more studies with methodological rigor are needed, especially to assess lung function, and quality of life, in addition to physical performance outcomes.
Conclusions
In conclusion, the current meta-analysis suggests that telerehabilitation contributed to improvement in functional capacity, muscular strength and endurance, and agility, and reductions in dyspnea and fatigue in COVID-19 adult survivors. In COVID-19 contagious-phase patients, quality of life was improved after a telerehabilitation protocol. Although the respiratory training-only protocol showed improvement in functional capacity, lower limb muscle strength and endurance, and dyspnea, combined training (DMRT associated with aerobic and/or respiratory exercise) should be indicated as an exercise prescription for COVID-19 survivors. Although no randomized clinical trial achieved the maximum score, the majority of them had good methodological and reporting quality indicating a low risk of bias. In RCTs, the evidence of functional capacity, agility, dyspnea, lower limb muscle strength and endurance, and maximum inspiratory strength ranged from moderate to high levels of evidence. Further studies with a longer duration of follow-up (more than 12 weeks) and more comprehensive data are needed to clarify the mechanisms underlying the changes in these outcomes, and to evaluate the influence according to sex. Despite the great response observed with combined training, no studies assessed aerobic training alone, and therefore, further studies could focus on this training modality.
Footnotes
Acknowledgments
The authors thank the authors who sent us information important to this article.
Data Sharing
The authors will make all relevant data available upon reasonable request.
Disclosure Statement
The authors have no conflicts of interest or financial conflicts to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.