
Abstract
Introduction:
This systematic review and meta-analysis aimed to investigate adherence and retention rates to home-based video exercise programs and identify key factors associated with these rates in older adults to understand the effectiveness of home-based video exercise interventions.
Methods:
We searched PubMed, Web of Science, and Scopus for articles addressing adherence to and retention of home-based video exercise programs. The study was conducted following PRISMA recommendations.
Results:
A total of 26 articles, including 1,292 participants older than 65, were included in the final qualitative and quantitative syntheses. The weighted mean of the retention rate was 91.1, and of the attendance rate was 85.0, with low I 2 = 3.5, not significant p = 0.409 heterogeneity. The generalized regression models showed a positive effect of session duration on the attendance rate (%), where the possible change from <20 min to >60 min duration could decrease the attendance rate (%) B = −24.390 (p <0.001). The delivery method had a significant effect, where the absence of live contact with the coach in web-based or DVD-delivered interventions could decrease the attendance rate (%) compared to the online sessions B = −11.482 (p = 0.010). The lockdown during the COVID-19 pandemic had a positive effect on both the attendance rate (%) B = 10.321 (p = 0.019) and retention rate (%) B = 9.577 (p = 0.032).
Conclusions:
This systematic review and meta-analysis indicate that supervised home-based video exercise programs lasting less than 60 min might be a suitable and sustainable exercise mode to keep older adults active, especially in times resembling feelings of confinement
Introduction
The beginning of the 21st century is characterized by the rapid ageing of the world’s population, which carries profound medical problems, among others. 1 One of these problems is related to older adults’ quality of life and functional capacity, which are attributes of health closely linked to physical fitness. 2 Generally, older adults are advised to engage in varied, multicomponent physical activity that emphasizes functional balance and strength training at moderate (150 min a week) or higher (75 min a week) intensity two or more days per week to improve functional capacity and prevent falls. 3,4 These recommendations are based on physical exercise programs, which have been demonstrated to be the most effective way to increase physical fitness in older adults. 5 However, Mora and Valencia 6 recommend that older people should always aim to be physically active within their abilities and health limits. In fact, regular physical activity is essential for promoting healthy ageing and has many benefits, including a reduced likelihood of all-cause mortality, chronic diseases, and premature death. 7,8
During the global COVID-19 pandemic, remotely delivered home-based exercise programs became quite popular because of the imposed restrictions, specifically for the population of older adults. 9,10 Our recently published meta-analysis 11 showed that these programs positively affected essential components of physical fitness, such as balance and strength (crucial components for preventing falls) in older adults and, as such, might serve as a preventative measure in age-related physical fitness declines. However, only after assessing factors such as participant adherence and retention can the overall impact of these programs and their potential for more widespread adoption be accurately interpreted. In fact, high adherence and retention rates are desirable to ensure the effectiveness of prescribed exercise interventions.
Therefore, the aim of the present systematic review and meta-analysis was to investigate adherence and retention rates to home-based video exercise programs (which were assessed in our previous work for primary outcomes) and identify key factors associated with these rates in older adults.
Methods
This systematic review and meta-analysis were carried out per the recommendations and criteria outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 12 (Fig. 1), and the review protocol has been registered in the international prospective register of systematic reviews (PROSPERO: CRD42022381761).
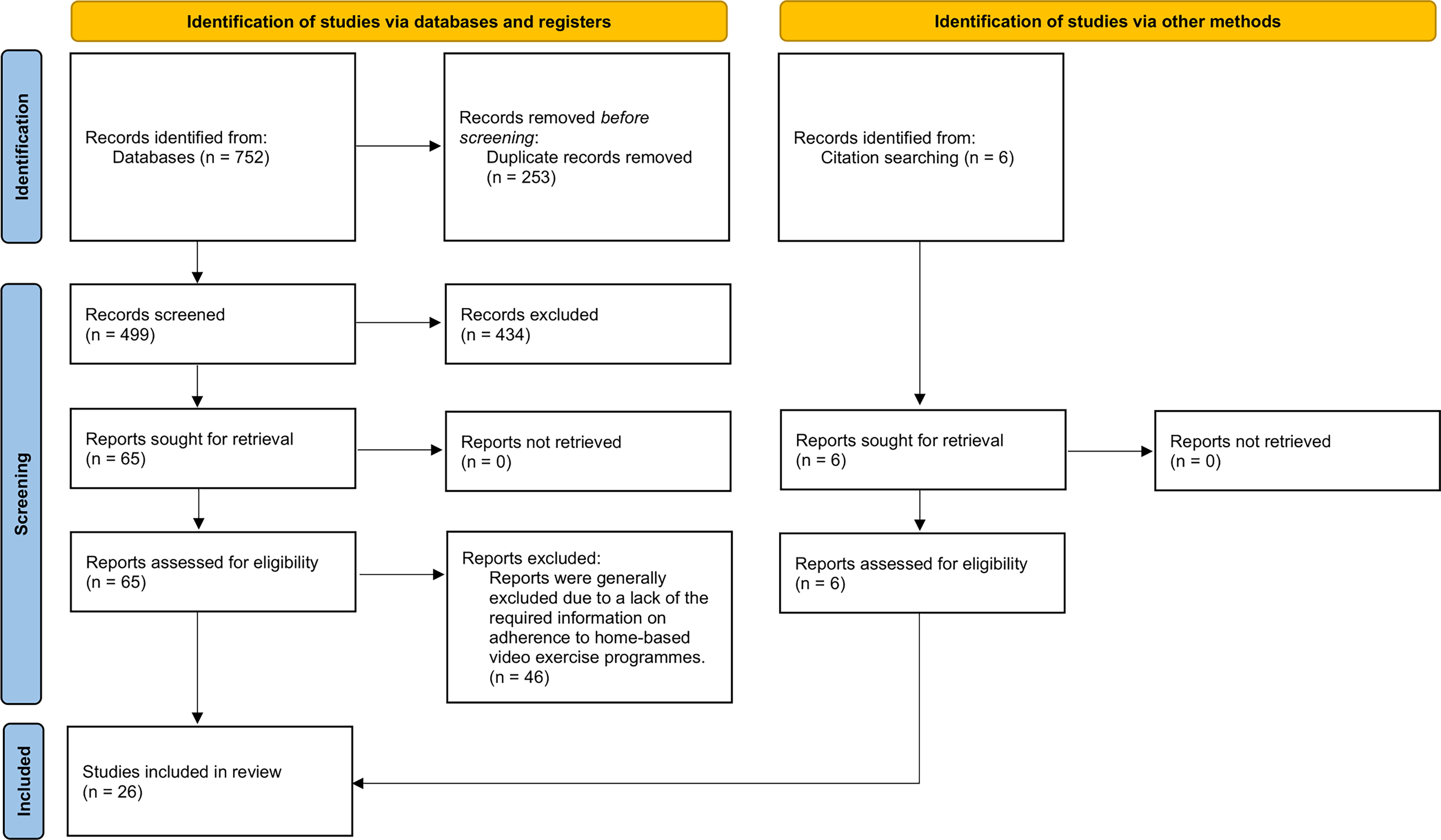
Flowchart illustrating the different phases of the search and study selection.
CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW
Studies focusing on the feasibility and acceptability of home-based video exercise programs for older adults >65 years, published in peer-reviewed journals, were included.
TYPES OF STUDIES
We considered single-group trials and either randomized controlled trials or nonrandomized controlled trials that focused on the feasibility and acceptability of home-based video exercise programs in older adults.
TYPES OF PARTICIPANTS
Medically-stable older adults 13 aged ≥65 years, either female or male, were considered for this study.
TYPES OF INTERVENTIONS
We included all studies focusing on the feasibility and acceptability of home-based video exercise programs for older adults.
TYPES OF OUTCOME MEASURES
The outcome measures were adherence, represented by the attendance rate (95% confidence interval [CI]), calculated as the number of completed sessions divided by the total number of possible sessions, and retention rate (%), calculated as the proportion of participants who completed the study divided by the total number of participants initially enrolled in the exercise group.
SEARCH METHODS FOR IDENTIFICATION OF STUDIES
Appropriate papers were identified by searching three electronic databases: PubMed, Scopus, and Web of Science. We used the same stream of keywords but adapted them according to the rules of each database (Table 1).
Search Results from Electronic Databases
DATA COLLECTION AND ANALYSIS
All potential papers were first downloaded using a reference manager, and then all duplicates were removed. If the papers appeared suitable after briefly screening the abstracts, three independent reviewers examined the full text in detail. In addition, further potential papers were identified from the reference lists of papers and reviews obtained from the database search.
DATA EXTRACTION AND MANAGEMENT
We collected the following data for the training groups only: attendance rate (%), and to see the variability, we collected either standard deviation (SD) or 95% CI: and retention rate (%). We collected the following independent variables for further analysis: session duration, delivery method, and lockdown presence during the study.
ASSESSMENT OF RISK OF BIAS IN INCLUDED STUDIES
A modified version of the Cochrane risk of bias tool ROBINS-I for nonrandomized comparative studies was used to assess the methodological quality of the included studies. 14
STATISTICAL ANALYSIS
First, we calculated the 95% CI: for the retention rate (%) using binomial exact calculation with a one-sided 97.5% CI: when the retention rate (%) = 100. Second, we used a fixed method approach 15 to calculate the overall weighted proportion for retention and attendance rates and then separately for session duration and delivery method. For the attendance rate, we estimated heterogeneity using Cochran’s Q test and the I 2 index. 16
We then used either one-way ANOVA with Tukey HSD post hoc test or independent samples t-test to test for differences in retention and attendance rates according to session duration and delivery method. Additionally, we ran generalized linear models to estimate the association between session duration, delivery methods and lockdown presence as independent factors and retention and attendance rates (%) separately as dependent variables. We calculated the unstandardized regression coefficient B as the primary outcome for each independent factor. Statistical significance was set at α = 0.05 for all analyses. Statistical analysis was performed using IBM SPSS Statistics 24 software.
Results
DESCRIPTION OF STUDIES
This systematic review included 26 trials. A total of 1,292 participants were included in the exercise groups. The average age of the participants was 66.9–83.0 years. Healthy older adults living independently were included in 14 trials, prefrail older adults with a presumed range of severity were included in 8 trials, and older adults with mild cognitive impairment were included in 2 trials. Except for one trial that included only women, the rest included women and men together. Eight trials were conducted during the COVID lockdown. The basic description of the included studies is shown in Table 2.
Basic Description of the Included Studies
Median [IQR].
MCI, mild cognitive impairment.
RISK OF BIAS IN INCLUDED STUDIES
The methodological quality of most of the included studies showed an acceptable risk of bias, according to ROBINS-I. No serious risk of bias was identified. Only four studies 19,23,32,33 were classified as moderate quality (Fig. 2).
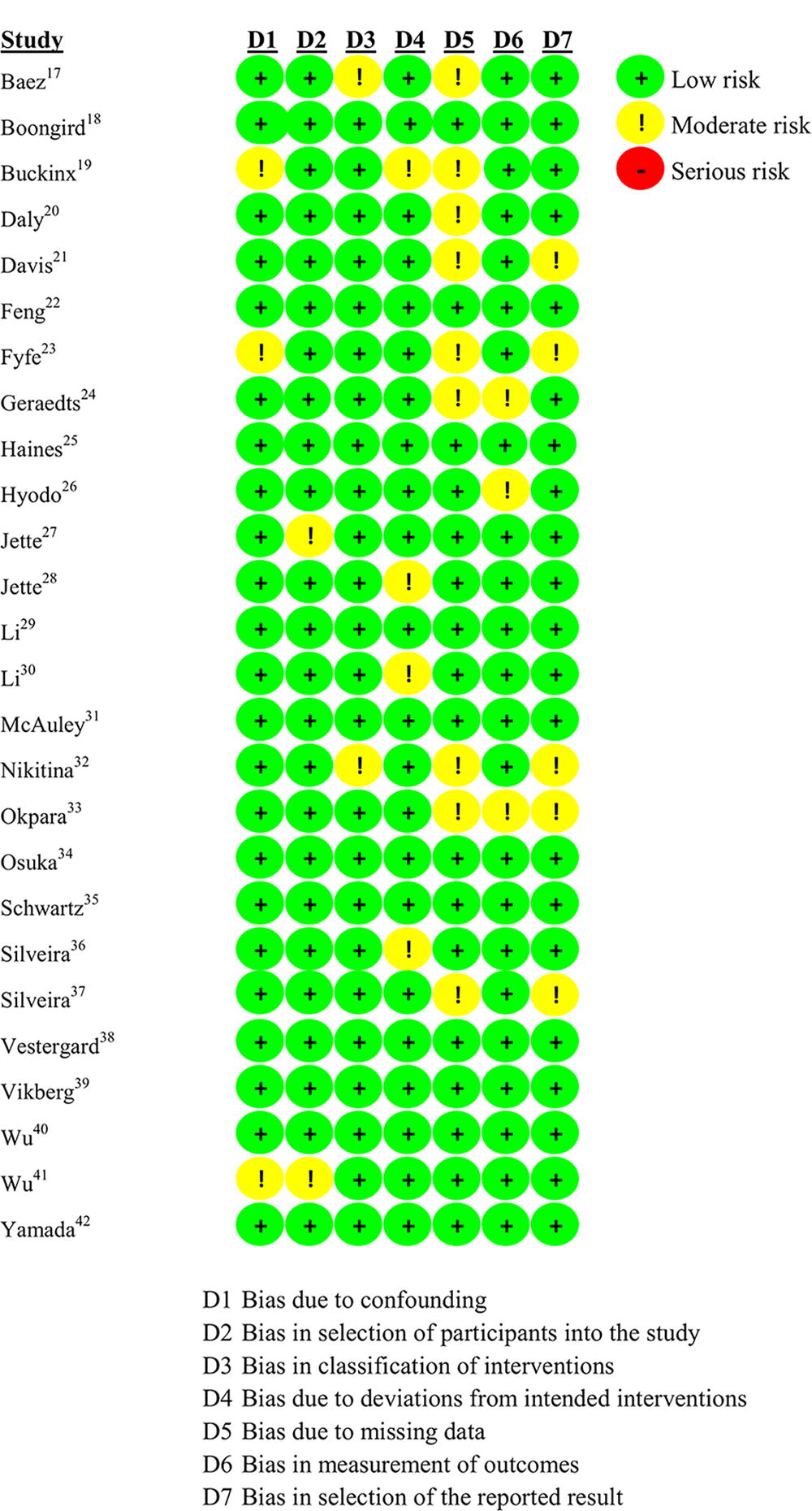
Risk of bias assessment using the ROBINS-I tool.
SYSTEMATIC REVIEW
Regarding exercise type, eight studies used modifications of the Otago exercise program originally introduced by Campbell et al., 43 one used FlexTuBe, 31 and six used different Tai Chi programs. The other studies used several different exercises, primarily focusing on strength and balance, and two studies used stretching exercises, one used dual-task stepping, and one used aerobic dance. Fourteen studies delivered exercises online with coaches via ZOOM, Skype or Teams; the rest used web-based (YouTube) or DVD without direct contact with coaches. The intervention period ranged from 4 weeks to 12 months, the number of sessions was 2 per week to 3 sessions per day, and the duration of sessions ranged from 9 to 100 min. The mean attendance rate started at 50.7 (95% CI: 40.7–60.7), and the highest was 97.4 (95% CI: 97.4–100.1). The average retention rate ranged from 54.5% to 100%, averaging 87.3% across all study groups. Table 3 shows the results of the studies included in this systematic review.
Results of the Studies Included in This Systematic Review
Note: CI, Confidence interval.
META-ANALYSIS
The weighted mean of the retention rate was 91.1 (95% CI: 73.9–108.3), and the weighted mean of the attendance rate was 85.0 (95% CI: 80.6–89.5), the heterogeneity was low I 2 = 3.5 not significant p = 0.409. The forest plots of the distribution of both retention and attendance rates are shown in Fig. 3 and Fig. 4. There was no significant difference between web-based or DVD (92.2, 95% CI: 71.1–113.4) and online (88.8, 95% CI: 59.1–118.5) delivery in the retention rate, nor in the duration where the retention rate was ≥60 min = 86.3, 95% CI: 50.8–121.8; 20–60 min = 90.2, 95% CI: 64.7–115.8; <20 min = 95.9, 95% CI 65.1–126.8 (Fig. 5a). There were significant differences in attendance rates in both analyses (Fig. 5b). The attendance rate in web-based or DVD was 84.5, 95% CI: 79.8–89.3 with low nonsignificant heterogeneity I 2 = 28.1%, p = 0.109; in online was 89.1, 95% CI: 75.7–102.5 with negligible heterogeneity I 2 = 0, p = 0.953; in ≥60 min was 75.1, 95% CI: 53.0–97.3, I 2 = 0, p = 0.991; 20–60 min was 79.9, 95% CI: 61.9–97.8, I 2 = 0, p = 0.990; <20 min was 85.8, 95% CI: 91.1–90.5, with substantial heterogeneity I 2 = 67.8, p = 0.002.
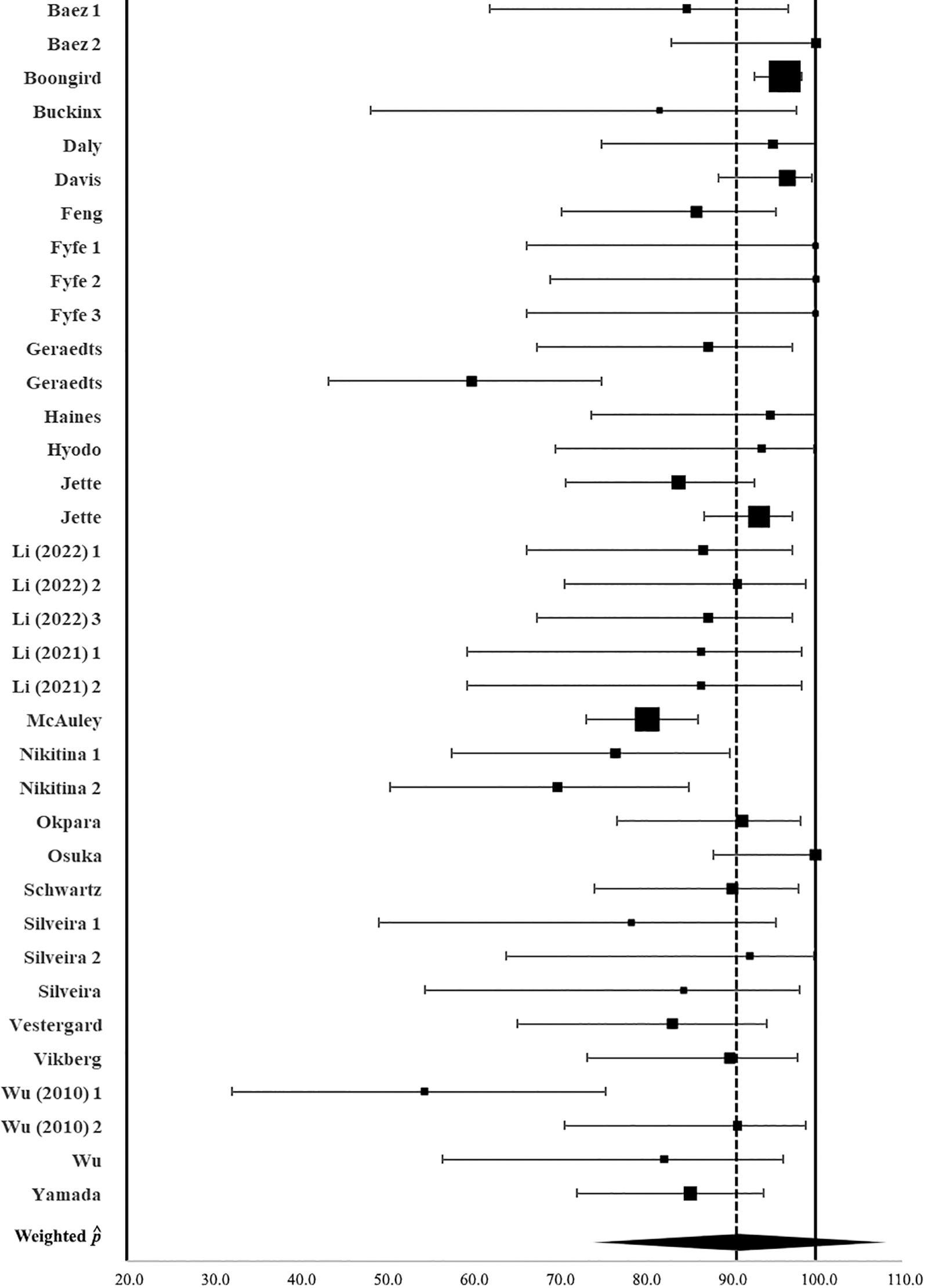
The forest plots of weighted mean of retention rate (%).
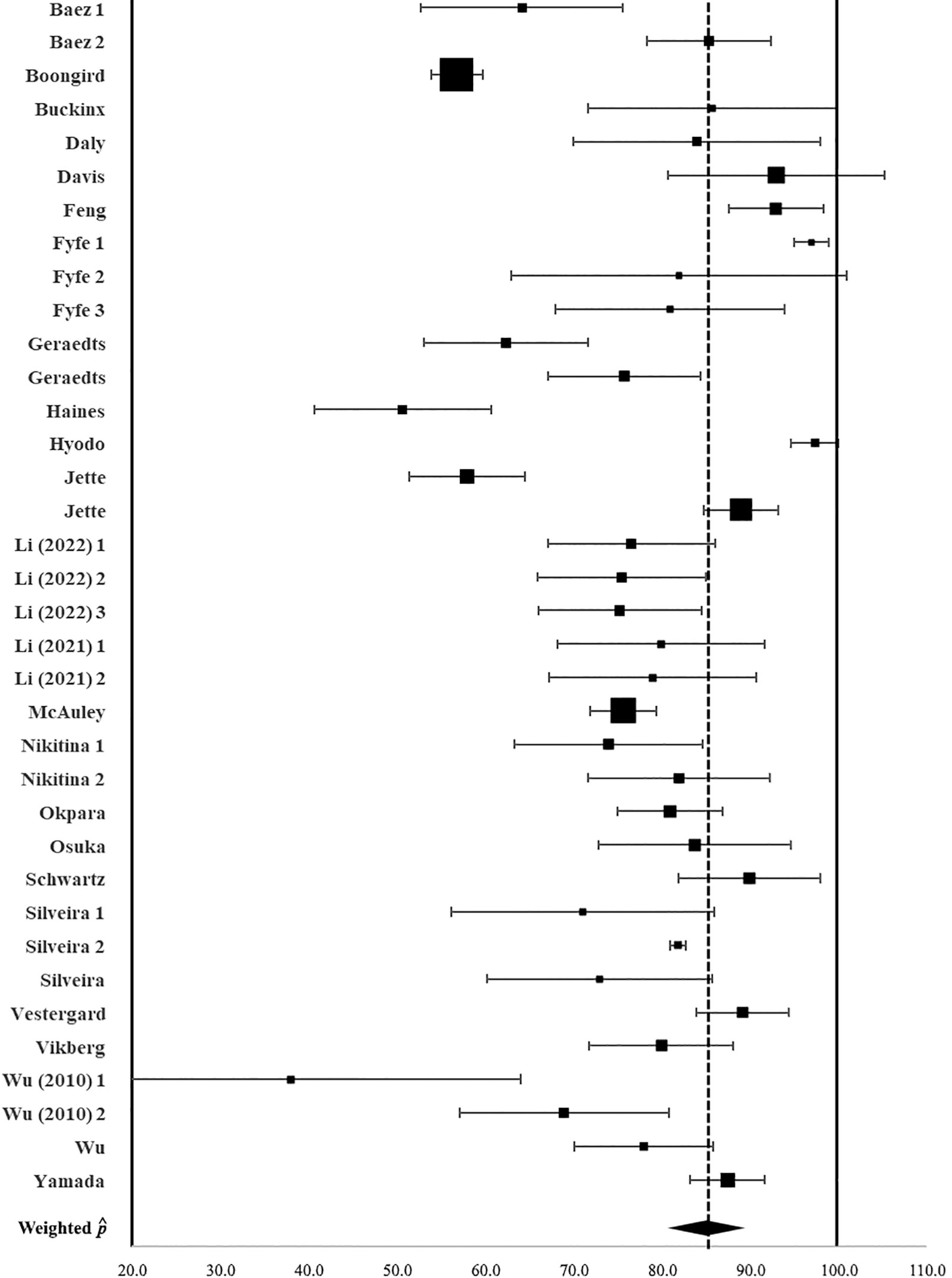
The forest plots of weighted mean of attendance rate (%).
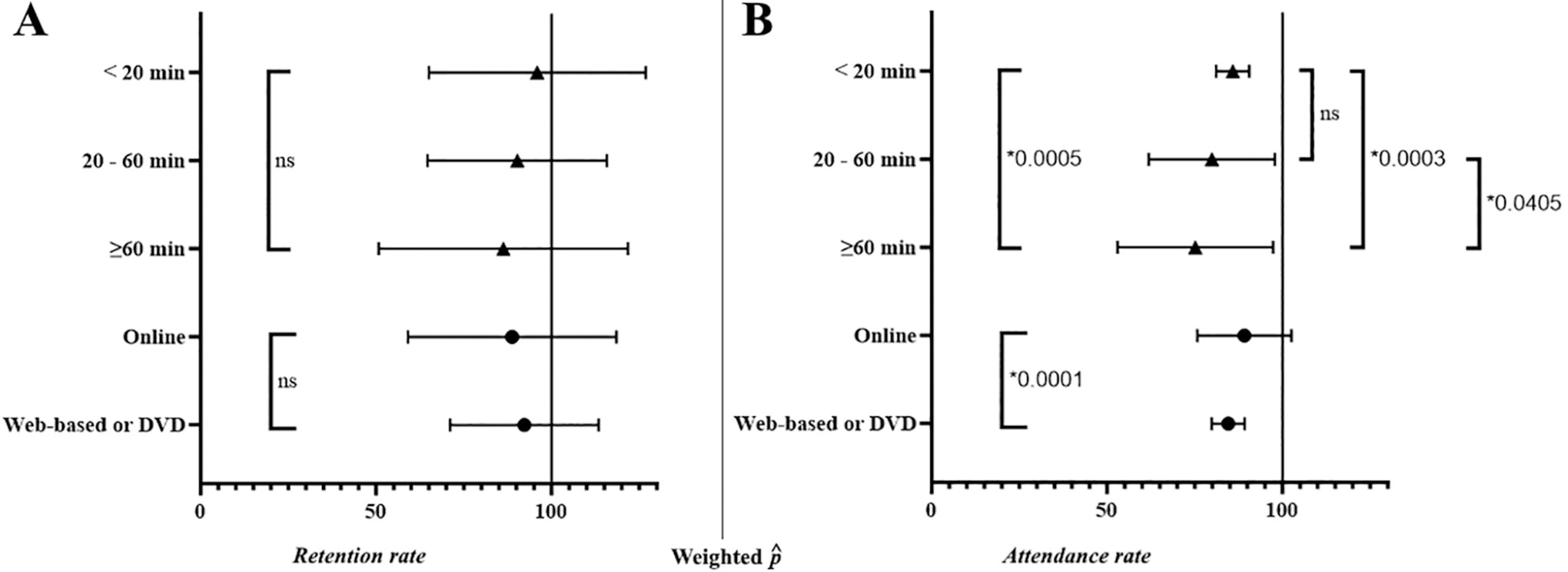
The forest plots of comparison of weighted mean of retention and attendance rates (%) divided according to different factors.
As part of the meta-analysis, we ran generalized regression models, which showed that lockdown during the COVID-19 pandemic positively affected retention rate (%) B = 9.577 (p = 0.032). There were no other significant associations in the analysis of retention rates (Table 4). The generalized regression models showed a positive effect of session duration on the attendance rate (%), where the possible change from <20 min to >60 min duration could decrease the attendance rate (%) B = −24.390 (p <0.001). The delivery method also had a significant effect, where the absence of live contact with the coach in web-based or DVD-delivered interventions could decrease the attendance rate (%) compared to the online sessions B = −11.482 (p = 0.010). As well as the retention rate (%), the lockdown during the COVID-19 pandemic had a positive effect on the attendance rate (%) B = 10.321 (p = 0.019). The results of the generalized linear model for the attendance rate (%) are shown in Table 5.
The Generalized Regression Model with Retention Rate (%) as the Dependent Variable
Set to zero because this parameter is redundant.
The Generalized Regression Model with Attendance Rate (%) as the Dependent Variable
Set to zero because this parameter is redundant.
Discussion
SUMMARY OF MAIN RESULTS AND INTERPRETATION
This systematic review and meta-analysis focused on estimating adherence and retention rates to home-based video exercise programs and identifying key factors associated with these rates in older adults. The results of this study indicate that adherence and retention rates to such programs were relatively high across all the trials, with means of 91.1% for retention and 85.0% for adherence rates, respectively. We then identified the following key factors as positive to promote these rates: (1) lockdown during the COVID-19 pandemic positively affected both retention and adherence rates; (2) session duration of fewer than 60 min positively affected the adherence rates; and (3) the presence of live contact with the coach in web-based or DVD-delivered programs positively affected the adherence rates again. These results are discussed in more detail in the following lines.
Unless older people engage in feasible physical activity, the constant increases in the average mean length of life will come with the onset of comorbid conditions, disability, and compromised quality of life. 44 In general, the extent to which a patient correctly follows medical advice is crucial to the success of any intervention 45 and in terms of exercise interventions, that goes double. It was estimated that only about 50% of patients living in developed countries adhere to treatment recommendations, including rehabilitation or physical exercise regimes. 45 –47 Adherence to and retention of an exercise program is of fundamental importance for evaluating the program’s efficacy and is challenging across all ages, particularly among older adults. 48 The mean adherence and retention rates (Table 3) to home-based video exercise programs in older adults analyzed in our study were relatively high. These rate ranges were similar to those reported by Cyarto et al. 49 for home-based resistance training programs in older adults and by Cox et al. 50 for home exercise interventions in females between 40 and 65 years of age. However, it should be emphasized that this similar trend is specific to included studies conducted in the pre-COVID era, which exhibited substantially lower rates.
LOCKDOWN DURING THE COVID-19 PANDEMIC
Adherence to and retention of exercise programs in older adults depends on many biopsychosocial factors and exercise program characteristics. 48,51,52 Consider In 2020, Brooke and Jackson reported...' rather than an article published in The Journal of Clinical Nursing 10 reported that prolonged homestay and social isolation have adverse effects on many aspects of physical and mental health, specifically in older individuals. Of great concern were specifically the sudden reduction of physical activity patterns and increased sedentary behavior, which is known to be significantly associated with higher sarcopenia rates. 53
In addition, the lack of social interactions that are often crucial to encouraging older people to exercise dropped significantly; therefore, one would expect lower adherence and retention rates during the lockdown. Contrary to our belief, our generalized regression models in the meta-analysis showed quite the opposite trend: lockdown during the COVID-19 pandemic positively affected both these rates. We can only speculate that this result might be due to increased free time compared to everyday routine without lockdown or the knowledge of the importance of being active, as reported elsewhere. 54 However, it would be worth investigating this phenomenon in future studies by suitable empirical methods (i.e., questionnaires). Our results suggest that home-based video exercise programs might be more effective regarding adherence and retention rates, perhaps during periods resembling feelings of confinement, such as in winter or nursing homes. 55
THE PRESENCE OF LIVE CONTACT WITH THE COACH
It is well known that personal interactions between participants and coaches during training sessions positively affect older adult participants, including their adherence rates. 48,50,52,56 The results of the present meta-analysis also revealed that live (remote) contact between the coach and participants during the home-based video exercise programs positively affects adherence rates. Indeed, it may also be possible that the lockdown during the COVID-19 pandemic has facilitated these higher rates due to the need for social interactions, 57 which in our case has come through the live coaches. Nevertheless, incorporating supervision during home-based exercise programs in older adults may improve adherence rates and, in turn, may lead to greater primary outcomes, as suggested previously, 48 which is the sought-after result of exercise interventions. For example, telerehabilitation in the form of videoconferencing has already proved to be as effective as usual care, 58 which is an exciting and important finding that could also work for home-based exercise programs.
EXERCISE SESSION DURATION
Findings related to exercise durations are extremely important in order to create suitable and sustainable exercise programs for different populations. This study identified session duration as the most important key factor for the adherence rates and, as such, confirms previous findings that the longer the duration of the intervention, the lower the adherence rates. 51,59 More precisely, our findings suggest that more than 60 min of exercise duration is related to lower adherence rates to the home-based video exercise programs. The reason for better adherence rates to shorter exercise sessions might be the same as for the shorter duration of the entire exercise intervention program, such as not having the time or not fitting well into the daily routine, as well as to avoid interventions that could bore or overwhelm the patients. 60,61
Therefore, it is not only the duration of the entire intervention that might put older people off committing to long-term exercise regimes but it is also the session duration. In this regard, it would be vital to measure adherence to exercise interventions that allow for all sorts of shorter-duration sessions to determine the most effective intervention regarding both adherence and improved physiological factors related to physical fitness. Indeed, this may conflict with some scientific aims as certain variables may need longer session duration. However, researchers must try to find the most adequate and sustainable exercise programs to keep older people active. In this regard, home-based video exercise programs seem suitable because (1) they have been shown to improve physical fitness parameters 11 and (2) they could be easily incorporated into the daily routine of older adults.
There are limitations in this work that must be considered. First, it is possible that the search strategy, which focused on the words adherence, retention, feasibility, and acceptability in the title, may have omitted some articles, which may have described similar definitions by other concepts. Nevertheless, the number of studies in our work allows us to analyze the existing evidence to draw firm conclusions. Furthermore, we must consider that different characteristics vary among the studies with different evaluations of adherence and retention parameters, which the authors of the included studies interpreted. Moreover, none of these studies have reported compliance to assess or ascertain the intensity of exercise, which would otherwise provide valuable information about potential setbacks during the exercise sessions. Despite these limitations, the current study has found important factors to consider when prescribing exercise programs for the older population.
QUALITY OF EVIDENCE
The studies included in this review and meta-analysis were randomized and nonrandomized trials and assessed as having no serious risk for bias and quality of reporting data.
POTENTIAL BIASES IN THE REVIEW PROCESS
Our review might be biased as only published research was included.
Agreements and disagreements with other studies or reviews.
This study partially confirms and extends recent findings by Collado-Mateo et al., 51 who, in their meta-analysis, have identified 14 key factors to improve adherence to exercise in patients with chronic diseases and older adults, and among them, supervision during exercise sessions has also been identified as an essential factor to improve adherence.
Conclusions
The present systematic review and meta-analysis indicate that adherence and retention rates to home-based video exercise programs are on the higher end in older adults, especially during times of confinement. Notably, the results of our work suggest that less than 60 min of exercise duration and live contact with the coach in web-based or DVD-delivered interventions seem to improve adherence rates in older adults. Home-based video-assisted exercise cannot be the only physical activity; however, it can increase the provision of and access to appropriate opportunities and help all older adults maintain an active lifestyle according to their abilities in order to avoid sedentary behavior, which is detrimental to health. Future studies should focus on compliance with prescribed exercise programs to investigate any potential setbacks older adults may encounter.
PRACTICAL IMPLICATIONS
Home-based video exercise programs might be more effective regarding adherence and retention rates at home during periods resembling feelings of confinement, such as in winter or in nursing homes.
Home-based video exercise programs should be of <60 min in duration and ideally with a live coach to improve adherence rates in older adults.
Participant compliance with home-based video exercise programs is an essential but unreported outcome that should be investigated in future studies to understand the potential setbacks of prescribed exercise in older adults.
Footnotes
Acknowledgment
The authors highly acknowledge the financial support from the Grant of the Ministry of Health of the Czech Republic [grant number NU22-09–00447] and the grant of Charles University-Cooperatio.
Authors’ Contributions
M.R.: Writing—original draft. T.J.: Writing—original draft (lead); writing—review and editing (equal). T.V.: Methodology (lead); writin—review and editing (equal). K.M.: Writing—review and editing (equal). V.K.: Funding acquisition; conceptualization (supporting); Writing—original draft. M.S.: Formal analysis (lead); writing—review and editing (equal). P.H.: Development or design of methodology. M.M.: Review and editing (equal). I.H.: Conceptualization (lead); supervision.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This project was supported by the