
Abstract
Introduction:
The COVID-19 pandemic has led to the rapid and widespread adoption of telehealth services. Telehealth may aid in bridging gaps in access to care. The specific impact of telehealth on opioid use disorder (OUD) and its treatment remains uncertain.
Methods:
A retrospective review of commercial insurance claim records within the United States was conducted to investigate the association between the COVID-19 pandemic and changes in the rates of(a) OUD treatments with and without telehealth support and (b) prescriptions for medications for opioid use disorder (MOUD) with and without telehealth support among individuals diagnosed with OUD.
Results:
In a study population of 1,340,506 individuals, OUD diagnosis rates were 5 per 1,000 in-person and 1 per 1,000 via telehealth. COVID-19 decreased in-person OUD diagnoses by 0.89 per 1,000, while telehealth diagnoses increased by 0.83 per 1,000. In-person MOUD treatment rates increased by 0.07 per 1,000 during COVID-19, while telehealth rates remained low. The onset of COVID-19 saw a 1.13 per 1,000 higher increase in telehealth-supported MOUD treatment compared to solely in-person treatment.
Conclusions:
A retrospective review of commercial insurance claim records within the United States was conducted to investigate the association between the COVID-19 pandemic and changes in the rates of (a) OUD treatments with and without telehealth support and (b) prescriptions for MOUD with and without telehealth support among individuals diagnosed with OUD.
Introduction
Opioid use disorder (OUD) remains a significant public health crisis within the United States (U.S.). 1 The U.S. has witnessed an alarming surge in opioid-related fatalities, leading to heightened awareness and concerted efforts to combat the epidemic. 2 Characterized by the compulsive misuse of opioids, including prescription painkillers, OUD has negatively impacted individuals, families, and society, highlighting the pressing need for effective prevention and intervention strategies. 3 –5 These strategies demand a holistic approach involving prevention, education, and compassionate support.
A common treatment approach is the prescription of medications for opioid use disorder (MOUD), with methadone and buprenorphine emerging as primary options, supplemented by concurrent cognitive behavioral therapy. 4 MOUD may aid in the reduction of illicit opioid use, safeguard against relapse, enhance an individual's overall quality of life, and diminish the likelihood of adverse events and fatalities associated with OUD. 6,7 Despite persistent efforts in prevention and treatment advancement, the pervasive stigma surrounding addiction continues to impede access, possibly contributing to a sustained increase in the mortality rate linked to OUD. 1,8
The COVID-19 pandemic has necessitated unprecedented changes in health care delivery, including the rapid and widespread adoption of telehealth services. 9 Telehealth provides health providers with flexibility in delivering care and empowers them to treat patients while maintaining the necessary physical distance to prevent the spread of the virus.
Telehealth has not only emerged as a health care delivery model that allows for social distancing but also a potential solution to bridge the gap in access to care by providing a means for individuals with OUD to receive necessary treatment and support, both remotely and privately. 10 Telehealth fosters patient engagement and adherence while potentially also reducing disparities and expanding treatment among vulnerable populations. More specifically, telehealth may be instrumental in eliminating geographical, transportation, and stigma barriers. 11,12 As the pandemic gradually wanes and ushers in a future with a more integrated telehealth infrastructure, understanding the effect of telehealth services and the increased flexibility in policies regarding care delivery on OUD diagnosis and treatment access becomes paramount. 12
While telehealth has been evaluated in a variety of clinical areas and diverse health care settings, its specific impact on OUD and its treatment remains uncertain. 13 –17 The objective of this study was, therefore, to assess the impact of the pandemic on the utilization of telehealth for the diagnosis and treatment of OUD within a commercially insured population.
Methods
A retrospective review of commercial insurance claim records within the U.S. was conducted to investigate the association between the COVID-19 pandemic and the changes in the rates of (a) OUD diagnosis and (b) MOUD prescriptions with and without telehealth support. A comparative interrupted time series analysis design was used to assess the differences in the change in treatment rates with and without telehealth support.
SETTING AND STUDY POPULATION
The study cohort was derived from the IQVIA PharMetrics Plus database from 2019 to 2021. The IQVIA PharMetrics Plus is a nationally representative database that comprised inpatient and outpatient medical claims, pharmacy claims, and health plan enrollment information among individuals enrolled in a commercial health plan throughout the U.S. This study used the data from a 10% random sample of the IQVIA PharMetrics Plus accessed through the UAMS Translational Research Institute.
The study cohort encompassed individuals aged 18 to 65, both male and female, who maintained continuous insurance enrollment throughout the U.S. from April 2019 to March 2021. Cases with undisclosed sex information in enrollment records were excluded (N = 3), leading to a primary analysis sample size of 1,340,506 adults.
MEASUREMENTS
The primary outcome measures included the rate of enrollees who (a) had a record of an OUD diagnosis (b) were dispensed a MOUD medication with and without telehealth support, in the period of April 2019 through March 2021.
Diagnoses of OUD were identified using the International Classification of Diseases, tenth Revision, Clinical Modification (ICD-10-CM) codes. Receipt of a prescription for MOUD was determined by identifying MOUD-specific Health Care Common Procedure Coding System codes in medical records, or prescriptions for methadone, buprenorphine, or naltrexone, documented under product names, generic names, or Medi-Span Generic Product Identifier descriptions.
Medical records were classified as telehealth-supported based on the place of service, procedure code modifier, and revenue code. 18 To define telehealth-supported prescriptions, records of methadone, buprenorphine, or naltrexone prescriptions were linked to medical claims within 12 months of the prescription date, using the following algorithm: if the prescriber had a medical claim for the same individual indicating an OUD diagnosis within 12 months of the prescription date, the prescription was linked to the OUD medical record with the closest treatment date. If the prescriber did not have a medical claim with an OUD diagnosis for the individual, any medical record by the prescriber within 12 months of the prescription date and nearest to it in terms of the treatment date was linked. Successful linkage occurred for 76% of the methadone, buprenorphine, and naltrexone prescriptions.
The telehealth-support flag on the linked medical record was then used to ascertain whether the MOUD prescription was telehealth-supported. For the telehealth-supported prescription records, the date of the associated telehealth medical claim served as the index date.
Sex, age, and insurance type were all identified from insurance enrollment records. Individual residences were classified into four different regions: South, Midwest, West, and Northeast.
STATISTICAL METHODS
Descriptive analysis examined demographic factors (age, sex), insurance type (Commercial, Medicaid, Medicare, Self-Insured or Other/Unknown), and U.S. regions (South, Midwest, West, and Northeast) of insurance enrollees who (a) had at least one OUD diagnosis made in a telehealth setting and had an OUD diagnosis but never in a telehealth setting or (b) had at least one MOUD treatment supported by telehealth and had an MOUD treatment but never in a telehealth setting. A series of comparative interrupted time series models were applied to assess the impact of the COVID-19 pandemic on the delivery type of OUD and MOUD. The periods before and during the pandemic were distinguished at the initial public health emergency declaration (March 2020).
The model specification integrated a group-specific linear time series to establish the baseline trends in OUD diagnoses and MOUD rates for both telehealth and nontelehealth settings within the pre-COVID-19 public health emergency period (April 2019–February 2020). The changes in trends specific to each group following the initial public health emergency declaration were subsequently estimated and compared based on the delivery mode. Ordinary least square regressions were fitted using SAS, version 9.4.
SENSITIVITY AND SUBGROUP ANALYSES
Since not every prescription claim for MOUD is accompanied by a corresponding medical claim indicating OUD, a sensitivity analysis was conducted focusing only on individuals who had an MOUD prescription claim and a corresponding OUD diagnosis in their medical claims.
A subgroup analysis focused on pregnant women and investigated OUD and MOUD treatments during the 9 months preceding and the 3 months following their delivery date (N = 24,215). Pregnancy identification relied on ICD-10-CM and ICD-10 Procedure Coding System codes associated with pregnancy and guided by relevant literature. 19 –21
The rest of this article followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 22
This study was approved and determined as nonhuman subject research by the University of Arkansas for Medical Sciences Institutional Review Board (IRB No. 274548).
Result
Of the 1,340,506 individuals in the total study population, about half (50.5%) were female. The average age of the population was 42.3 (SD = 13.7), and most individuals (93.7%) were primarily covered by commercial insurance, and the largest portion of individuals were from the Midwest (33.5%).
Descriptive statistics for OUD diagnosed individuals indicate that a rate of 5 per 1,000 individuals had an OUD diagnosis through an in-person setting. In comparison, only 1 per 1,000 individuals had an OUD diagnosis at least once through a telehealth setting. The distribution of sex was comparable between in-person only and telehealth OUD diagnosis groups (p = 0.83). Statistically significant differences were observed in the distributions of age category, payment type, and regions of individuals who received OUD diagnosis in-person compared to those who received it via telehealth. The highest proportion of individuals diagnosed through in-person only settings was in the age category of 56–65 years old, whereas those diagnosed via telehealth settings were predominantly within the age range of 36–45 years. The proportion of Medicare enrollees was higher in the telehealth OUD diagnosis group compared to the in-person-only group, shown in Table 1.
Demographic Characteristics of Population with Opioid Use Disorder Diagnosis and Medication for Opioid Use Disorder Recipients
Data were obtained from IQVIA Pharmetrics Plus from April 2019 to March 2021.
Row proportion per 1,000 is presented in this row. Percentages presented in the rest of rows are column percentage. t-test was used to calculate p-values to test the difference of age (continuous variable) by delivery type. There was a statistically significant difference in average age between telehealth and nontelehealth OUD diagnoses (p = 0.012) but no statistically significant difference in average age between telehealth and nontelehealth delivery of MOUD treatment (p = 0.067).
Chi-Square p-value was calculated for categorical variables and were all <0.05 except for gender (p = 0.83) by OUD diagnosis delivery type and gender (p = 0.505) and region (p = 0.153) by MOUD delivery type.
MOUD, medication for opioid use disorder; OUD, opioid use disorder; SD, standard deviation.
During the study period, 4 per 1,000 individuals received an MOUD treatment through an in-person-only setting, while 1 per 1,000 individuals received an MOUD treatment through a telehealth setting. Similar demographic distributions for both the in-person setting group and the telehealth setting group among MOUD recipients were observed for continuous age (p = 0.067), gender (p = 0.505), and regions (p = 0.153). There were statistically significant differences in the distribution of age category and payment type of individuals who received an OUD diagnosis in-person versus in a telehealth setting. The telehealth MOUD recipient group had a higher proportion of Medicare enrollees than the in-person only group.
Figure 1 presents the trends in the number of individuals who received diagnoses of OUD in a telehealth versus in-person setting pre- and during-COVID-19 (March 2020). The summary for an estimation of a comparative interrupted time series is summarized in Table 2. There is a 1.72 per 1,000 (p < 0.001) difference between the changes in the number of individuals who received OUD diagnoses via telehealth and patients who received OUD diagnoses in-person only (Table 2). During-COVID-19, the in-person OUD diagnosis trend increased by 0.04 per 1,000 from the baseline (p < 0.001; Table 3). From April 2019 to February 2020, the monthly rates of OUD diagnoses in a telehealth setting were consistently below 0.1 per 1,000 (baseline mean 0.01, p = 0.881; baseline trend 0.002, p = 0.828; Table 4), whereas the rates of OUD diagnoses in-person were higher (baseline mean 1.7 per 1,000) and trending upwards at the monthly rate of 0.05 per 1,000 (p < 0.001). Compared to the baseline trend, the number of individuals who received an OUD diagnosis in the in-person setting fell by 0.89 per 1,000 (p < 0.001) following the emergence of COVID-19. Meanwhile, COVID-19 led to an increase of 0.83 per 1,000 (p < 0.001) in the number of individuals who received OUD diagnoses via telehealth (Table 4). Similar to OUD diagnosis outcomes, the monthly rates of MOUD treatment in a telehealth setting are consistently low (baseline mean 0.008, p = 0.932; baseline trend; Table 5). Figure 2 presents the trends in the number of individuals F2 who received MOUD treatments in a telehealth versus nontelehealth setting, pre- and during-COVID-19.
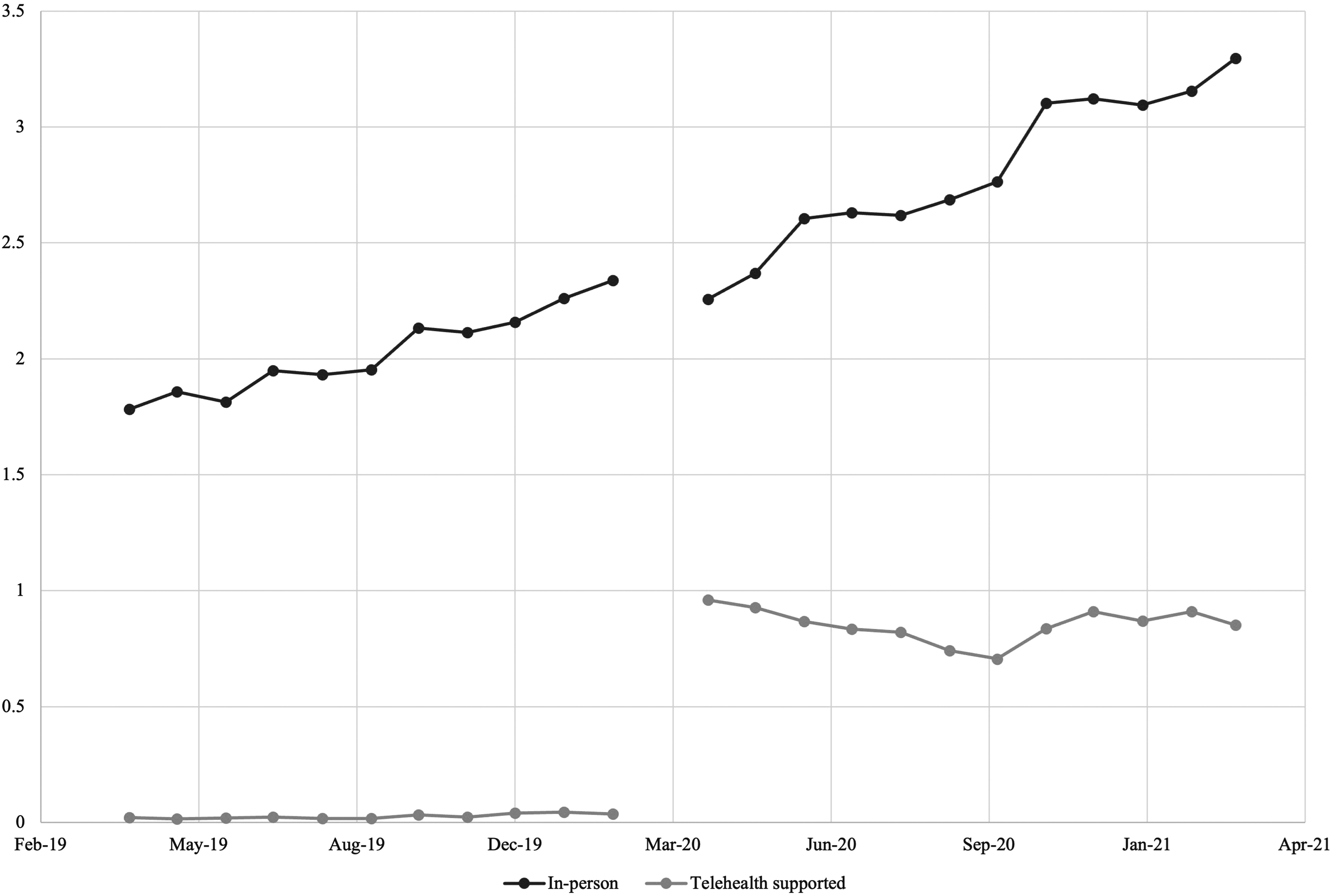
This figure presents proportions (per 1,000) of individuals who received an OUD diagnosis in a telehealth versus nontelehealth setting per month, pre- and during-COVID-19. The blue line represents the monthly proportion of individuals who received an OUD diagnosis in any delivery mode. The orange line represents the monthly proportion of individuals who received an OUD diagnosis in in-person setting only while the gray line stands for the monthly proportion of individuals who received an OUD diagnosis in telehealth setting. OUD, opioid use disorder.
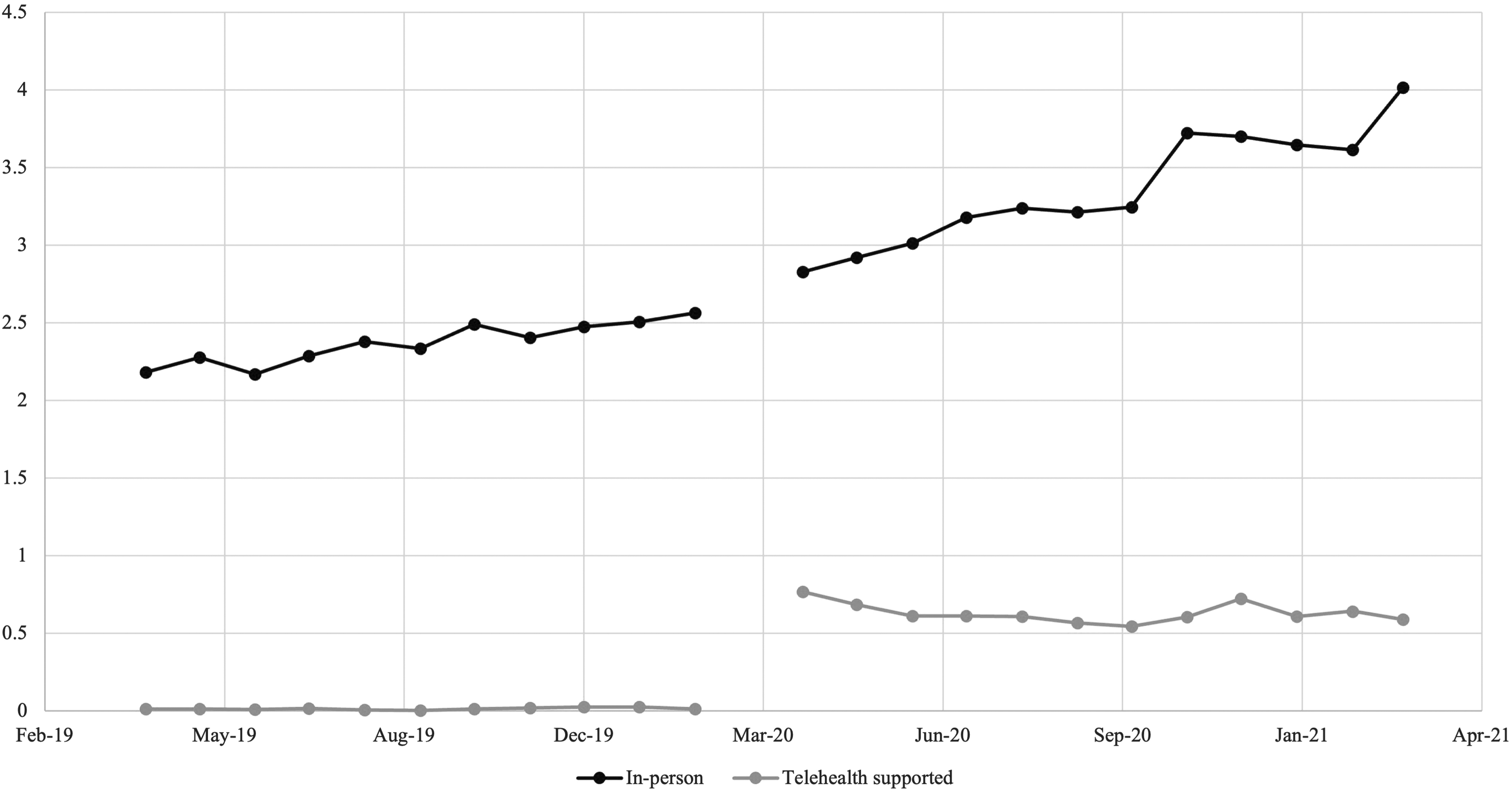
This figure presents proportions (per 1,000) of individuals who received a MOUD treatment in a telehealth versus nontelehealth setting per month, pre- and during-COVID-19. The blue line represents the monthly proportion of individuals who received a MOUD treatment in any delivery mode. The orange line represents the monthly proportion of individuals who received a MOUD treatment in in-person setting only while the gray line stands for the monthly proportion of individuals who received a MOUD treatment in telehealth setting. MOUD, medication for opioid use disorder.
Estimates of the Association Between Covid-19 Pandemic Emergency Declaration and Telehealth Supported Opioid Use Disorder Treatments; Opioid Use Disorder Diagnosis
Authors' analysis of data from IQVIA Pharmetrics Plus, 2019 to 2021.
Regression estimates are from respective comparative interrupted time series models specified in the Supplementary Material. The modeled outcomes are rates per 1,000 individuals. R-squared = 0.9943.
p < 0.001.
Estimates of the Association Between Covid-19 Pandemic Emergency Declaration and Telehealth Supported Opioid Use Disorder Treatments; Medication for Opioid Use Disorder Treatment
Authors' analysis of data from IQVIA Pharmetrics Plus, 2019 to 2021.
Regression estimates are from respective comparative interrupted time series models specified in the Appendix. The modeled outcomes are rates per 1,000 individuals. R-squared = 0.9966.
p < 0.01.
p < 0.001.
Opioid Use Disorder Diagnoses Rates (Per 1,000)
Authors' analysis of data from IQVIA Pharmetrics Plus, 2019 to 2021.
Calculations for the overall OUD diagnoses come directly from the regression estimates presented in Table 2, except for during-COVID-19 trend, which is calculated as
Baseline trend =
Standard errors are presented in parentheses next to the coefficient estimates.
p < 0.001.
Medication for Opioid Use Disorder Treatment Rates (Per 1,000)
Authors' analysis of data from IQVIA Pharmetrics Plus, 2019 to 2021.
Calculations for the overall MOUD treatment come directly from the regression estimates presented in Table 3, except for during-COVID-19 trend, which is calculated as
Baseline trend =
Standard errors are presented in parentheses next to the coefficient estimates.
p < 0.001.
Sensitivity analyses restricting the sample to only individuals who had an MOUD prescription claim and a corresponding OUD diagnosis in their medical claims yielded similar results. Model estimates for the sensitivity analysis are summarized in Supplementary Material S1 and Supplementary Material S2. The rates and temporal trends in MOUD receipt in a telehealth versus nontelehealth setting are shown in Supplementary Material S3. In the subgroup analysis, only 99 pregnant women with a formal OUD diagnosis and 63 pregnant women being dispensed MOUD prescriptions were identified. The change in rate for OUD diagnosis of pregnant women pre- and during-COVID-19 was 0.98 in the in-person setting and 0.59 in the telehealth setting. The change in MOUD rates of pregnant women pre- and during- COVID-19 was 1.15 in the in-person setting and 0.18 in the telehealth setting, as discussed in Supplementary Material S4.
Discussion
Before the COVID-19 pandemic, there was a minimal utilization of telehealth services for the diagnosis and treatment of OUD. The nonstatistically significant trends seen in the telehealth rates over time suggest that telehealth had a limited role within this clinical area during this period. In alignment with previous studies, 23,24 in-person OUD diagnosis and MOUD prescription rates were increasing pre-COVID. Subsequent to the declaration of the public health emergency, a remarkable surge in the use of telehealth in OUD diagnoses and MOUD prescriptions demonstrated a substantial shift in the health care delivery modes. However, after this initial increase, telehealth uses slowly fell. In contrast, after the initial reduction at the onset of the pandemic, the in-person OUD diagnoses and MOUD prescription rates recovered as providers gradually returned to see patients in-person.
Despite these during-COVID trends, telehealth-supported care continued to play a significant role in the care, with more than 20% of OUD diagnoses sustained to be supported by telehealth at the end of the study period. Supported by technology, overall OUD diagnoses and MOUD treatment rates did not decrease during the pandemic, despite reduced clinic hours and worsening access.
The absence of a continuous growth in telehealth utilization during the pandemic signaled challenges in implementing and sustaining telehealth supported OUD treatment. Prior studies have documented challenges associated with telehealth treatment compared to face-to-face interventions. These challenges include limited access to operational devices, inadequate broadband infrastructure, unreliable internet connections, concerns with data privacy and security due to the sensitive nature of medical information, limited familiarity with digital tools, and variations in licensing and reimbursement policies across jurisdictions. 25 –32 During the pandemic, the Centers for Medicare and Medicaid (CMS) and many private payers enacted payment parity rules offering equal payment rates for care whether provided via telehealth or in-person. 33 Some temporary federal telehealth changes and flexibilities are ending at the close of 2024. 34
In addition, many state Medicaid programs are limiting the scope of telehealth reimbursement, and about half of the states have yet to enact private payer payment parity laws. 35 These factors together raise concerns about the long-term sustainability of telehealth services. 35
Regulatory relaxations have played a crucial role in the rapid expansion of telehealth services for MOUD at the onset of the pandemic. The Drug Enforcement Administration and the Substance Abuse and Mental Health Services Administration temporarily terminated the initial in-person visit requirement and allowed phone visits for a buprenorphine prescription 36 and increased allowable take-home methadone doses 37 in response to the pandemic. CMS issued a guidance to encourage state Medicaid agencies to set higher reimbursement rates for telehealth visits, including visits for MOUD prescribing. The U.S. Department of Health and Human Services increased allowance of eligible physicians to prescribe OUD to up to 30 patients, exempting them from certain federal requirements. 38,39
Within the cohort of commercially insured pregnant women, the number of individuals with documented OUD diagnoses or those undergoing MOUD treatment, whether through in-person or telehealth services, proved insufficient for deriving significant conclusions. Considering the vulnerability of this group, it is imperative to initiate further research that utilizes alternative data sources explicitly tailored to encompass this population. A comprehensive understanding of the role of these services within this demographic is crucial, especially as stakeholders evaluate the future of telehealth.
Most studies regarding OUD treatment through telehealth have primarily concentrated on evaluating clinical effectiveness, with a particular focus on using retention and abstinence rates as key indicators. 40,41 Some of these studies showed that telehealth is comparable to and, in some cases, superior to in-person treatment rates. 23,24,40 A national survey conducted among addiction medicine doctors indicated a preference for patients to engage in telehealth visits at a clinical facility as opposed to their residences. This inclination stemmed from the necessity for technology that complies with the Health Insurance Portability and Accountability Act, as well as a lack of on-site urine screening and accessible local counseling for patients being cared for virtually. 42
Addressing these factors was deemed essential for the physicians to feel sufficiently at ease with providing MOUD telehealth services. 42,43 Remote urine testing is susceptible to issues that can compromise its accuracy, including technical errors at the time of the collection or manipulation of the samples. The need for in-person urinalysis testing suggests that while telehealth can play a supporting role in OUD treatment, it should be optimally combined with in-person interventions and monitoring to provide comprehensive and personalized care.
This study has several strengths and limitations. The IQVIA dataset offers a comprehensive representation of a diverse range of commercially insured adults spanning multiple states, each impacted differently by the pandemic and its associated policies. Because of this, the study enabled a generalizability to the broader commercially insured U.S. population. 44,45 The dataset, however, does not include individuals with primary alternative insurance types, such as Medicaid and most of Medicare, or those lacking insurance coverage altogether. This omission is significant, as this demographic is often disproportionately affected by OUD and faces challenges in accessing treatment, particularly to telehealth. 46
While the dataset comprehensively captures diagnosis and prescription data, it may not encompass prescriptions that were paid for out-of-pocket. Moreover, the prescription records exclusively indicate medication dispensation, offering no insight into actual patient consumption. In addition, the hesitation among physicians to formally code OUD due to its stigma and potential repercussions for the patient might lead to underreporting and a discrepancy between diagnosis records and therapeutic interventions. Although the dataset consistently captures services rendered through telehealth, the surge in telehealth utilization and the modifications in reimbursement mechanisms during the pandemic might have introduced inconsistencies in coding practices across different care settings.
Conclusion
The findings strongly indicate that the COVID-19 pandemic had a discernible influence on the utilization of telehealth for OUD diagnoses and MOUD prescriptions. This aligns with existing documentation of the potential versatility, adaptability, and significance of telehealth in providing vital health care services in various settings. 47,48 The findings also emphasize the need for continued research that evaluates the long-term consequences of these transformations and optimizes telehealth care delivery for both patients and health care systems.
Footnotes
Authors' Contribution
K.L. conceptualized and designed the study, performed the final analyses, drafted the initial article, and reviewed and revised the article. D.Z. conducted data curation and investigation, designed analytic methodology, and reviewed and revised the article. G.C. drafted the initial article, provided a clinical interpretation, and reviewed and revised the article. H.E. and C.H. obtained the funding, supported the administration of the project, provided resources, and reviewed and revised the article. L.G. conceptualized and designed the study, designed analytic methodology, drafted the initial article, and reviewed and revised the article.
All authors approved the final as submitted and agreed to be accountable for all aspects of the work.
Disclosure Statement
No financial disclosures were reported by the authors of this article.
Funding Information
Research reported in this publication was supported by the U.S. Health Resources & Services Administration under Award Number U3GRH40001. The dataset leveraged in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR003107. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health and U.S. Health Resources & Services Administration.
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
Supplementary Material S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.