
Abstract
Objective:
To measure prevalence of prior/current Plasmodium vivax and Plasmodium falciparum (PV and PF), Brucella spp. (BR), dengue virus (DENV), Leishmania donovani (visceral leishmaniasis; VL), and Crimean-Congo hemorrhagic fever (CCHF) virus exposure among Afghan National Army (ANA) recruits.
Methods:
Randomly chosen, nationally representative serum samples from consenting men aged 18–40 years and who were screened between February 2010 and January 2011 were tested, with ∼25 samples/province. Samples were screened for PV and PF antigens and VL antibody with rapid diagnostic tests. Reactive malaria screening results were confirmed with polymerase chain reaction assay. Enzyme-linked immunosorbent assays were used to screen for CCHF and DENV antibodies; reactive DENV samples were confirmed with the plaque-reduction neutralization test. BR screening and confirmatory testing was performed with slide and tube agglutination, respectively. Correlates of BR titres >1:80 were analyzed using logistic regression.
Results:
Of 809 participants contributing specimens, 62% had previously lived outside Afghanistan, predominantly in Pakistan and Iran. CCHF (4.1%, n = 33), DENV (2.1%, n = 17), and VL (1.0%, n = 8) antibody prevalence was low. For PV and PF, only 7 out of 56 reactive samples had detectable nucleic acid. For BR, 8.0% (n = 65) of samples had screening titers >1:40, of which 83.1% had confirmatory titers >1:80. Participants from Kabul and surrounding provinces had lower odds (OR = 0.19, 95% CI: 0.04–1.00) of BR antibody compared with other regions.
Conclusions:
BR exposure was relatively common with a nearly national distribution, whereas geographic distribution for other pathogens aligned roughly with the expected vector distribution. Public health protection measures should include vector control, food safety, and enhanced diagnostics for acute febrile illness.
Introduction
A
One approach to improving differential diagnosis is by improving knowledge of the geographic distribution of these infections. In the 2008 CCHF outbreak, 11.2% of asymptomatic individuals who were household contacts of cases had CCHF virus antibody (Mustafa et al. 2011). There are few data regarding asymptomatic or general population prevalence for these infections; a study from Iran detected 1.6% prevalence of PV in blood smears taken from 446 asymptomatic Afghan immigrants in Iranshahr district, whereas a seroprevalence assessment of deployed British troops in Helmand revealed no samples reactive for CCHF antibody (Nateghpour et al. 2011, Newman et al. 2014).
Opportunities for serologic surveillance in the general population are limited, though banked serum from nationally representative groups provides the ability to estimate general population prevalence and the geographic distribution of pathogen exposure. One such population group are the armed forces, who may provide samples for routine testing during health checks (Brown et al. 2011, Ribeiro et al. 2012, Wickremasinghe et al. 2014). In 2010–2011, a large cross-sectional seroprevalence assessment of 4750 randomly selected Afghan National Army (ANA) recruits was conducted to assess prevalence and correlates of HIV, syphilis, herpes simplex-2 virus, and hepatitis B and C virus (Todd et al. 2012). Serum samples from participants consenting to additional testing from de-identified specimens were stored and available for public health testing. The Disease Early Warning System department within the Afghan Public Health Institute of the Ministry of Public Health prioritized testing for CCHF, visceral leishmaniasis (VL), dengue virus (DENV), PV and PF malaria, and brucellosis from a representative group of specimens. The purpose of this analysis is to measure the prevalence of markers of past exposure to or current infection with the selected vector-borne and zoonotic pathogens and to describe the distribution of detected cases among a nationally representative sample from male ANA recruits.
Materials and Methods
The ANA seroprevalence study methods have been previously described (Todd et al. 2012). Briefly, randomly selected male recruits presenting at the Kabul Military Training Center for medical screening and enlistment were approached for study participation. Eligible participants were male, aged 18 years or older, Dari or Pashto speaking, and able to provide informed consent. Consenting participants completed an interviewer-administered questionnaire detailing sociodemographic characteristics and risk behaviors, provided an intravenous specimen for testing and serum storage, and received pre- and post-test counseling. Participant names were not recorded; assigned study numbers were the sole identifier for all study materials. Approval for the original study and the amendment for this nested analysis were obtained from the institutional review boards of the Columbia University, the Walter Reed Army Institute of Research, and the Ministry of Public Health of the Islamic Republic of Afghanistan before performing testing.
For this nested sub-study, study numbers of participants consenting to use of their donated specimen for additional public health testing were combined into a separate database. The database was stratified by province of birth or having been born outside Afghanistan, and 25 study numbers selected randomly from each group. Random selection was performed by taking the total number of participants from each province and then selecting 25 random numbers from that total (
Laboratory testing
Samples were tested for the following pathogens: PF and PV, VL (Leishmania donovani), DENV, CCHF virus, and Brucella spp (BR). Rapid diagnostic testing was performed for Plasmodium spp. antigens (CareStart™ Malaria Pf/Pv combo test; Access Bio, Inc.) and VL anti-K39 IgG antibody (Kala Azar Detect; InBios International, Inc.). Enzyme-linked immunosorbent assays (ELISA) were used to detect an antibody to DENV (Dengue IgG Capture; PanBio) and CCHF (Vektor-best) according to the manufacturer's instructions. No confirmatory testing was performed for VL or CCHF, in the latter case because select-agent-registered facilities of a sufficient biosafety level were not available to the authors. Specimens with reactive rapid test results for PV and PF were confirmed by melting-curve real-time polymerase chain reaction analysis for presence and Plasmodium species identification, as previously described by Mangold et al. (2005).
Confirmatory testing for DENV and Japanese encephalitis virus (JEV), another flavivirus with a known cross-reaction on DENV ELISA, was performed by plaque reduction neutralization test (PRNT50) for neutralizing antibody levels (Thomas et al. 2009). The reference strains used for PRNT50 were DENV-1 16007; DENV-2 16681; DENV-3 16562; DENV-4 C0036/06; and JEV 0423. Serum was diluted in a four-fold serial dilution and mixed with the virus in equal volumes before incubation in a 35°C water bath for 1 h. The mixture was inoculated into Rhesus monkey kidney epithelial cell (LLC-MK2 cells) in a 12-well plate and incubated at room temperature for 1 h on a rocker platform. The excess volume of the inoculum was removed. A first medium overlay containing low-melting-point agarose gel (Ultra Pure™ LMP agarose; Invitrogen) was added. DENV-infected cells were incubated for 6 days in a 5% CO2 incubator at 35°C before staining with 4% neutral red (Sigma) in a second medium overlay with LMP. The number of plaques was determined by manual counting. Neutralization test antibody titer was calculated with SPSS v21.0 (IBM Corporation), using regression with probit analysis at 50% reduction, which was identified as the highest dilution that can reduce the number of plaques by 50% as compared with the number of plaques in the virus control well. Screening for Brucella spp. was performed with slide agglutination, with confirmatory testing with tube agglutination using the Febrile Antigen Agglutination Test with Brucella abortus and Brucella melitensis antigens (product numbers 8810131 and 241049; Becton Dickinson).
Analysis
Descriptive statistics were generated to characterize the study population. The prevalence of each pathogen, based on reactive screening test results for VL, PV, and PF, and CCHF and reactive confirmatory test results for DENV, JEV, and Brucella spp., was categorized by region based on the reported province of birth. The rationale for displaying results by geographic region is that, due to language and ethnic commonalities, most Afghans reside or work near their province of birth. The need to seek refuge or work in other countries is noted as a limitation, and data are also included for those born outside Afghanistan for comparison. Associations between reactive tests and region of origin and other key factors were assessed with logistic regression. Data were analyzed with Stata 11.0 (Stata Corp LP).
Results
The demographic characteristics and travel history of participants contributing 809 samples for this analysis are displayed in Table 1. Generally, about two-thirds of participants had previously lived outside Afghanistan, usually in either or both Pakistan and Iran. In the screening tests, the overall prevalence of antibody to DENV (2.8%, n = 23), CCHF (4.1%, n = 33), and VL (1.0%, n = 8) was low. For malaria species, PV and PF antigens were detected in 2.1% (n = 17) and 4.3% (n = 35) of participants, with 0.5% (n = 4) reactive for both. For Brucella spp., 8.0% (n = 65) had titers >1:40 by slide agglutination testing. Distribution of reactive pathogen tests by region of birth is displayed in Figure 1.
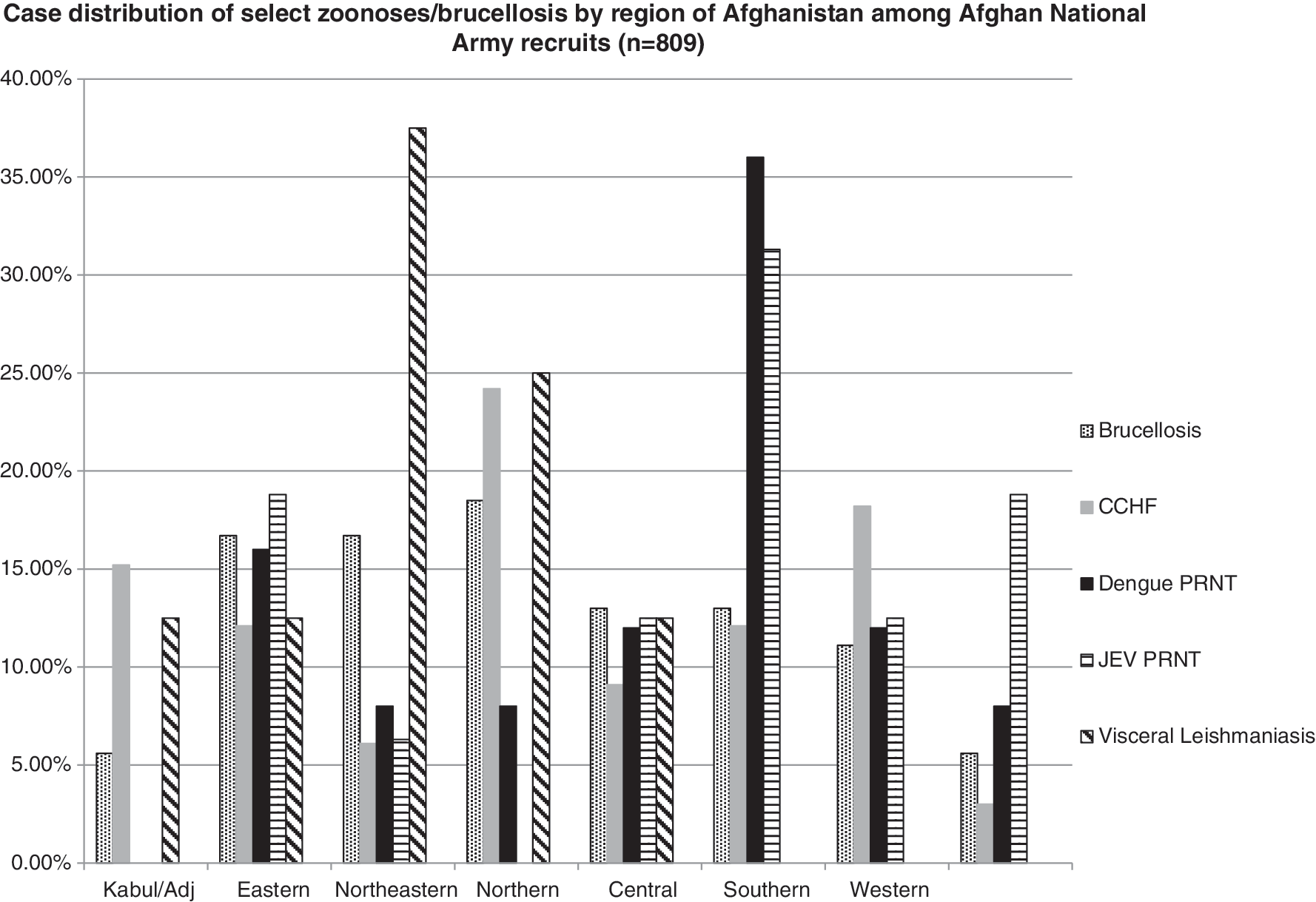
Case distribution of select zoonoses/brucellosis by region of Afghanistan among Afghan National Army recruits (n = 809). CCHF, Crimean-Congo hemorrhagic fever; PRNT, plaque reduction neutralization test; JEV, Japanese encephalitis virus.
Individuals could report time living in more than one country.
n, number.
For DENV, 60 specimens received PRNT testing, including the 23 with reactive results by ELISA and a further 37 randomly selected samples from this nested study population with nonreactive ELISA results for validation purposes. Specific DENV subtype distribution by PRNT assay for all 60 specimens is displayed in Table 2. Among specimens nonreactive by ELISA, all those with evidence of DENV by PRNT were positive for subtype 3. For malaria, only 7 out of 56 reactive samples had detectable parasitic DNA. Specifically, one sample had DNA detected for both PV and PF though it was reactive only for PF antigen by RDT, whereas 17% (n = 6) of samples with RDT reactive for PV had detectable DNA.
DENV, dengue virus; PRNT, plaque reduction neutralization test.
For Brucella spp., 83.1% (n = 54) of samples with titers >1:40 by slide agglutination also had titers >1:80 by tube agglutination. Due to lack of statistical power from the small sample size, only confirmed brucellosis infection was assessed for correlates. Those born in Kabul and the surrounding provinces had lower odds (OR = 0.19, 95% CI: 0.04–1.00) of having Brucella spp. antibody compared with other provinces, with those born outside Afghanistan serving as the reference. No socioeconomic indicators were associated with Brucella spp. antibody (data not shown).
Discussion
Key findings from this analysis include a nearly national distribution and a relatively high prevalence of Brucella spp. antibody, a prevalence >10% of CCHF antibody predominantly in the northern and western regions, and evidence of flavivirus exposure with similar prevalence between regions in Afghanistan and those having been born outside Afghanistan. This effort represents the first attempt to describe national distribution of priority zoonotic and vector-borne pathogens; however, certain limitations should be considered when interpreting these data. Military populations, due to their national representation, are ideal for estimating exposure risk and prevalence, with important caveats. The ANA recruit population was nominally healthy, though a review of systems to elicit recent fevers and other symptoms of the specified infections was not included in parent study data or in routine medical screening conducted by the ANA at enrollment. Further, no questions regarding recent insect stings/bites or exposure to or participation in slaughter or processing of animal carcasses were asked during routine screening or by the parent study. Participant vital signs were also not measured and it is possible that some recruits may have been febrile at the time of study entry, though they otherwise appeared well.
Because most laboratory results represent evidence of only prior exposure, there is no way to ascertain the geographic location at which the individual was exposed. Among the tested population, 62% reported previously living outside Afghanistan and some infections may have been acquired during that time. Further, though test result regions are determined by birth province, it is possible that some individuals did not recently reside in or repatriate to their native provinces. Infection distribution data are provided by region, as determined by reported province of birth, to reduce this effect. Last, several of the screening tests would have detected active infection/recent exposure only, particularly the histidine-rich protein 2 (HRP2) antigen for PF malaria, which remains present for up to 3 weeks after resolution of infection. Additionally, for pathogens for which screening and confirmatory testing was available, screening tests may have over-estimated prevalence, particularly for malaria and DENV. This may also have been the case for pathogens where only a single test was used. For example, CCHF ELISA results should be interpreted with caution, as no confirmatory assay was performed and cross-reactivity with antigenically similar nairoviruses is possible. Further work may be justified to clarify whether other nairoviruses are circulating in Afghanistan.
With those caveats, some interesting patterns emerge with regard to regional distribution of pathogen exposure. The results suggest that exposure rates to key causes of acute febrile illness are low, yet measurable, and not evenly distributed through the country. For example, our data describe a higher percentage of reactive CCHF tests among those originating in the north and west; whereas brucellosis is fairly evenly distributed throughout the country, and mosquito and sandfly vector-borne infections are generally more prevalent in the southern region (Leslie et al. 2006, Adimi et al. 2010).
An antibody to Brucella spp. detected by slide agglutination, indicative of prior exposure, was present in all regions and among those born outside Afghanistan (largely in Pakistan and Iran), consistent with its endemic distribution across Central Asia (Pappas et al. 2006, Dürr et al. 2013). Confirmed flavivirus antibodies were largely clustered in southern and eastern regions comprising provinces with populations with a high mobility to and from Pakistan, or among those born outside Afghanistan, consistent with endemicity of DENV and JEV in Pakistan, where many participants were born or had previously resided (Erlanger et al. 2009, Hasan et al. 2014). A recent flavivirus prevalence study from Afghanistan identified an antibody for West Nile virus, JEV, and DENV among symptomatic patients from several southern provinces bordering Pakistan and from Kabul (Elyan et al. 2014). Antibody detection for JEV has been documented in Helmand (south) and Kunduz (northeast) provinces, with DENV additionally identified in Helmand three decades earlier (Wallace et al. 2002).
A relatively high level of reactivity to the VL K39 epitope was observed in the northeast region, consistent with case distribution from a 2006 report (Leslie et al. 2006). This was particularly true for samples among those hailing from Nuristan, a remote eastern province with very limited access to healthcare due to poor transportation infrastructure and chronic insecurity; there are sparse health data regarding clinical leishmaniasis cases for this province. Further assessment is needed to determine whether VL represents a serious health threat in this region.
Conclusions
This analysis highlights the need for geographic and temporal correlation with case reporting and screening, as the results from this study cannot be linked to the site of exposure. The findings also lead to a call for further monitoring of vaccine preventable infections such as JEV. Additionally, continued surveillance for other vector-borne etiologies will be necessary to monitor the effectiveness of control measures, such as the distribution of long-lasting insecticide-treated bednets, indoor residual spraying, and the use of repellants. Finally, enhanced point-of-care (POC) diagnostics are essential to identify diseases such as brucellosis, leishmaniasis, and malaria to allow for effective treatment and prevention of long-term sequelae. Greater availability and accuracy of POC diagnostics deserves particular emphasis, as the settings in which cases arise are often remote where lack of capacity to perform ELISAs and molecular diagnostics is not available and cost and limited infrastructure (lack of electricity and refrigeration) remain as barriers to introducing these technologies. These data indicate that further improvements are needed in the diagnostic accuracy of commercially available assays for the assessed pathogens; more than 25% of those nonreactive for DENV IgG by ELISA had evidence of flavivirus antibody by PRNT assay. Since these diseases infect both humans and animals and cross-transmit, inter-sectoral collaboration is recommended to ensure a One Health Approach in which the animal health, human health, and environment protection sectors collaborate to address zoonotic diseases. Future studies need to focus on both animals and humans to assess potential reservoirs of infection and to determine prevalence of and risk factors for transmission of zoonotic diseases in this region to provide an evidence base for public health policies and infectious disease control programs.
Footnotes
Acknowledgments
The authors thank their colleagues at the Ministries of Defense and Public Health for their collaborative efforts, particularly National Public Health Laboratory and the Central Veterinary Diagnostic and Research Laboratory staff and Brigadier General Gul Aqa and General Sola Mal. They appreciate the assistance of Ms. Tippa Wongstitwilairoong with figure generation. Lastly, they are grateful to their participants for their time and trust.
This study was funded by the Global Emerging Infections Surveillance (GEIS) division of the U.S. Armed Forces Health Surveillance Center. The opinions or assertions contained here are the private views of the authors, and they are not to be construed as official, or as reflecting the true views of the United States Department of the Army or the Department of Defense.
Author Disclosure Statement
No competing financial interests exist.