
Abstract
Measles, Mumps, and Rubella (MMR) are vaccine preventable viral infections, which cause significant mortality and morbidity globally. Increased incidence rates of these infectious diseases are observed in young adults. Information on seroprevalence data on MMR in India is limited. The objective of this study was to determine the prevalence of IgG antibodies against MMR among young adults. This was a descriptive cross-sectional study involving 192 healthy college students from Maharshi Dayanand College, Mumbai. The project was approved by the Institutional Ethics Committee of Haffkine Institute. Between December 2012 and September 2013, blood samples were collected from individuals of age 18–23 years after obtaining written informed consent from them. The quantitative determination of IgG antibodies in serum specimens against MMR was determined using enzyme linked immunosorbent assay. Data on history of vaccination were also collected from participants. Among 192 healthy college students (age 18–23 years), MMR seroprevalence was 91%, 97%, and 88%, respectively. The overall seropositivity of MMR was 79%. The highest level of seronegativity was seen with regards to rubella-specific antibodies in 12% of cases. About 96% of the participants did not know about their vaccination history while none of the participants knew about their history of MMR infections. Despite unknown vaccination status, a majority of college students in our study were found seropositive for all three infections, which indicate natural boosting. However, the proportion of seronegativity for measles and rubella was relatively higher. Especially since the study population belonged to reproductive age group, there is a concern of congenital rubella syndrome in the offspring. Although a larger multicentric study is required to confirm the findings, the results indicate that a dose of measles–rubella (MR) vaccine should be offered to these college students.
Introduction
I
Measles is a highly contagious, acute exanthematous respiratory disease. In the prevaccination period, it was estimated that measles was responsible to cause 5–8 million deaths while more than 90% of individuals would acquire the disease by the age of 10 years. The common complications of measles include diarrhea, pneumonia, otitis media, and laryngotracheobronchitis, which are responsible for most of the deaths (1,21,22). During 1985–86, measles vaccination was introduced in India under the National Immunization Program. By 1996, 87% decline in the incidence of measles was observed. However, due to low immunization coverage in the urban slums, effective control of measles was hampered (4). In 2004, a pan-India measles mortality reduction strategic plan was launched, in which the inadequacy of vaccine coverage was attributed to the underreporting of the deaths due to measles. Therefore, in 2010, a second opportunity for measles immunization through either a second routine dose of measles vaccine or through supplemental immunization activities was initiated to target high-burden districts. Recent reports of measles surveillance from India estimate that between 2000 and 2011 measles mortality in India decreased by only 26–36% compared to 78% in rest of the World Health Organization (WHO) South East Asia region. This suggests that India still remains the leading country in deaths due to measles globally (20).
Mumps is an acute communicable viral infection characterized by parotitis and fever (1,22). Its typical clinical manifestations are characterized by pain and swelling of one or both parotid glands, fever, and fatigue. Other complications are orchitis among males, pancreatitis, and meningitis (1,13). Mumps is frequently reported in children aged 5 to 9 years, although college students and adults may also be affected. The use of specific immune prophylaxis has led to a significant success in reducing the instances of mumps epidemic at a global scale (14,22).
Rubella is an acute, mild viral infectious disease in children and adults that characteristically includes fever, rash, lymphadenopathy, and a broad spectrum of other manifestations (23). During the first trimester of pregnancy, the teratogenic potential of the virus may result in miscarriage, fetal death, or congenital defect known as congenital rubella syndrome (CRS). Complications associated with CRS include congenital heart defects, neurologic problems, auditory defects, ophthalmic problems, intrauterine growth retardation, hepatomegaly, and splenomegaly. The rubella vaccination targets to prevent congenital rubella infection (7,10,22). Even though the use of rubella vaccination has substantially reduced the incidence of rubella virus, over 100,000 infants are detected with CRS each year, mainly in developing countries worldwide (11,25). As several studies have demonstrated that rubella antibody may be waning in college students who were vaccinated with rubella vaccine (2), it becomes imperative to conduct such studies in India to gauge the current situation of the seroprevalence.
India is one of the densely populated countries in the world. Few studies on seroepidemiology have been conducted so far. Although India has already initiated the routine immunization program for infants aged 16–24 months through the second dose of (Measles containing vaccine) MCV in 21 states (30), MMR is yet to be considered in the national immunization program. According to the policy initiated by the Department of Family Welfare, Delhi in 1999, MMR vaccination has been included in its Expanded Program of Immunization for improving child survival (12). The present study was undertaken to assess natural immunity developed against MMR among Indian college students.
Materials and Methods
Study design
This descriptive cross-sectional study was conducted in healthy college students from the Maharshi Dayanand College, Mumbai. The study was conducted between December 2012 and September 2013. The inclusion criteria included healthy individuals of 18–23 years of age, willing to sign informed consent as a volunteer, and acceptance to participate in the study. The exclusion criteria included individuals below 18 years of age, individuals with acute febrile illness and any other infections, and individuals who were immunocompromised and were on immunosuppressive therapy.
Ethical aspects
The project was approved by the Institutional Ethics Committee of Haffkine Institute. All subjects signed a written informed consent for the study. Confidentiality was ensured by coding the questionnaire and samples before data entry and analysis.
Sample and data collection
A total of 192 adolescents were enrolled for the present study. A sample size of 192 achieves 95% power to detect a difference (P1-P0) of −0.10 using a one-sided binomial test. The target significance level is 0.0250. The actual significance level achieved by this test is 0.0242. These results assume that the population proportion under the null hypothesis is 0.8500 (5,9,17,19,31). Information on demographic characteristics and immunization status was collected at the time of enrollment.
Analysis of specimens
Up to 5 mL blood samples were collected from all subjects. Serum was separated by centrifugation, and samples were stored at −20°C. Blood samples were analyzed at the Department of Virology and Immunology, Haffkine Institute for Training, Research and Testing. Commercially available ELISA kits of Trinity Biotech, namely Captia Measles IgG, Captia Mumps IgG, and Captia Rubella IgG, were used for detection and quantitative determination of IgG antibodies in serum specimens. The test was performed and interpreted as directed by the kit manufacturer. The assay was considered valid when the reagent blank, negative control, calibrator, and positive control were within their respective ranges. Immune status ratio (ISR) value for each specimen was calculated by dividing optical density (OD) value of the specimen by the cutoff value proposed by the manufacturer. ISRs ≥1.1 were interpreted as seropositive. For data analysis, values below 1.1 were considered negative.
Statistical analysis
The age and gender-wise distribution of the participants were expressed as number and percentage. Other demographic and baseline characteristics are expressed as respective data sets. The number of participants with positive antibody titers for MMR was calculated along with 95% confidence interval (CI).
Results
Demographics
The demographic data (Table 1) indicate the age group and gender-wise distribution of the participants in the study.
Serology
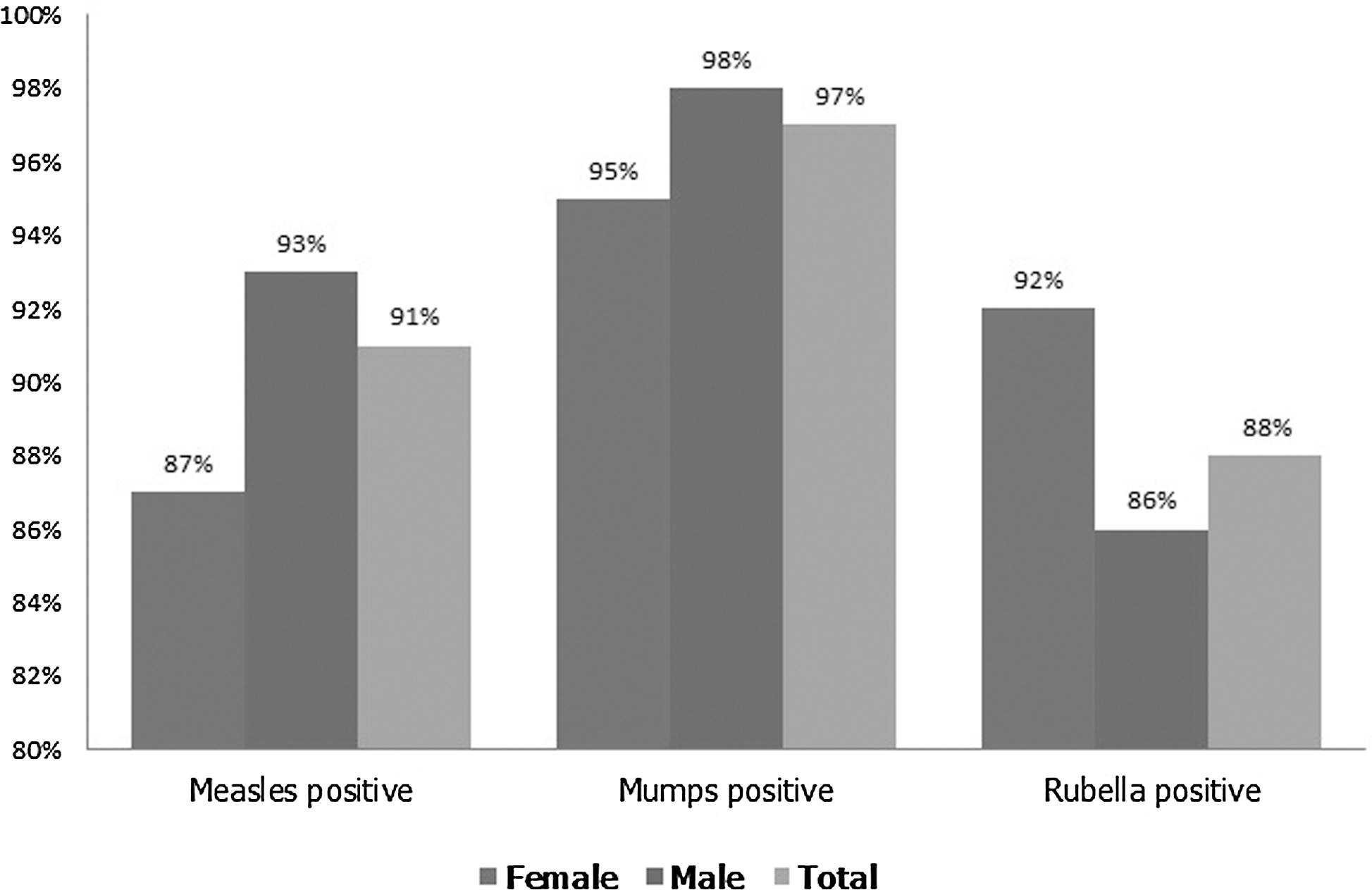
The overall seropositivity for measles IgG was 175 (91%; 95% CI 87–95%), seropositivity for mumps IgG was 187 (97%; 95% CI 95–100%), and seropositivity for rubella IgG was 169 (88%, 95% CI 80–96%) (Fig. 1).The geometric mean of ISRs for MMR for seropositive antibody titers is given in Table 2.
Overall distribution for measles, mumps, and rubella IgG antibodies.
CI, confidence interval; ISR, immune status ratio.
Of the 63 females under evaluation, 55 were seropositive for measles IgG (87%; 95% CI 79–96%), 60 were seropositive for mumps IgG (95%; 95% CI 90–100%), and 58 were seropositive for rubella IgG (92%; 95% CI 86–99%). Of the 129 males studied, 120 were seropositive for measles IgG (93%; 95% CI 89–97%), 127 were seropositive for mumps IgG (98%; 95% CI 96–100%), and 111 were seropositive for rubella IgG (86%; 95% CI 78–94%).
Seroprevalence of MMR IgG positivity by age is represented in Table 3. In females, the overall distribution of seropositivity for MMR was highest in the age group of 18–19 years, while in males, maximum seropositivity was seen in the age group of 20–21 years.
MMR, measles, mumps, and rubella.
The overall gender-wise distribution of MMR is denoted in Table 4. The prevalence of MMR antibodies was higher in males (79%; 95% CI 73–87%). The prevalence of antibodies to measles and mumps in the absence of rubella-specific antibodies was the most frequent pattern of antibody prevalence (89%; 95% CI 84–93%). In the absence of mumps antibodies, the seroprevalence of antibodies to measles and rubella was lowest (81%; 95% CI 76–87%).
In females, rubella seronegativity was 8% (95% CI 1.2–15%), whereas in males, it was 14% (95% CI 8–20%). Differences were even more pronounced for measles between females 13% (95% CI 20–40%) and males 7% (95% CI 11–20%), respectively. The total seronegativity for MMR was 9%, 3%, and 12%, respectively (Fig. 2).
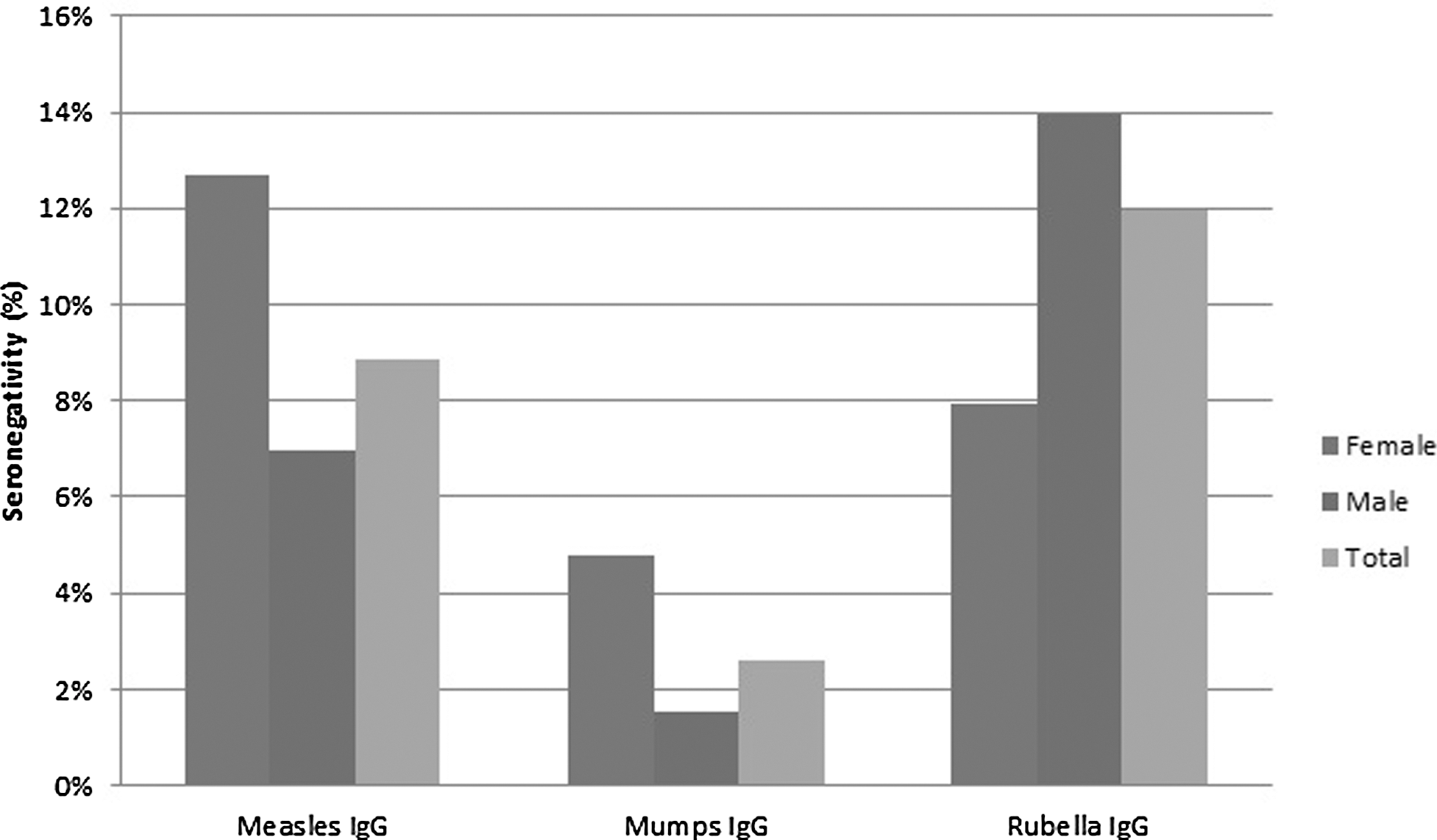
Gender-wise distribution of seronegativity for measles, mumps, and rubella IgG antibody titers.
During the course of the study, it was observed that the MMR vaccination status of 96% of participants was not known while 2% was unvaccinated. None of the participants had any history of MMR infections.
Discussion
Serological studies define epidemiology and consequences of infectious disease and also help define vaccination strategy. Seroprevalence data on MMR in India are scanty. Our results are the first to document the prevalence of MMR antibodies in college students from Mumbai. Mumbai being a cosmopolitan city, with an estimated population of more than 10 million, represents the country on a small scale. Serological surveillance helps to identify the proportion of susceptible individuals in the study population.
The seropositivity of college students in the present study was 91% for measles, 97% for mumps, and 88% for rubella. The overall prevalence of MMR antibodies in our study was 79%. Maximum seronegativity (13%) with regards to measles-specific antibodies in the present study was observed in females. Previous studies have revealed that girls in India are at higher risk than boys with respect to infectious diseases, as well as mortality (20). The reasons for higher mortality in girls could be worse nutrition, lower Vitamin A supplementation, and lower medical attention. It has been estimated that to interrupt the virus transmission, the population level immunity against measles needs to be minimum 93–95% (20). The total measles seropositivity in the present study was 91%, which suggest that a second dose of measles vaccination is necessary in reducing the disease burden.
Numerous studies from United Kingdom have estimated seropositivity for mumps to range from 75% to 92% (16). Immune status against mumps assessed in different countries has demonstrated that 90% of the population by the age of 14–15 years was seropositive (6,29). Other studies have also found high seroprevalence rates of mumps antibody (26). In the present study too, the seroprevalence to mumps virus was 97%. Most of these countries provide two doses of MMR vaccine in their routine immunization program; hence, the vaccine-derived immunity is increased and virus circulation is greatly reduced. A study similar to our present study, with a larger cross-sectional cohort, is necessary to derive data representative of Indian population and evaluate the MMR immunization program.
Globally, there is a considerable variation in the seroprevalence of rubella antibodies among adolescent girls and women of childbearing age. Previous studies have shown that European women have relatively higher rubella immunity (93%) compared to women of African (87%) and Asian origin (70–78%) (18). In a study in Tamil Nadu, 11–20% of females among 18–40 years age group were seronegative to rubella (28). The present study reveals that there are still 8% girl college students who are at risk of contracting rubella infection, which can be critical during their childbearing age.
In this study, an apparent difference by gender is seen, with higher rubella seronegativity in males compared with females. A similar observation was seen in Germany where boys in the adolescent age group had higher seronegativity. This could be because girls are vaccinated against rubella more often than boys due to the fear of CRS in future pregnancies (22). In addition, >90% of participants did not know the history of vaccination. The susceptible young individuals could have either escaped a natural infection or missed childhood vaccination (3).
The caveats of the study include that the study was from a single city in India, although we feel that the cosmopolitan nature of Mumbai could aid in relating this study outcome to most parts of the country. In addition, the sample size was small. Hence, our findings need to be corroborated in larger multicentric cross-sectional studies. Overall, seropositivity to measles and rubella antibodies was around 10% in the study group. Considering the importance of protection against measles and rubella (especially for women of childbearing age), a booster dose of measles-rubella (MR) vaccine should be considered for young adults.
Footnotes
Acknowledgments
The authors acknowledge Dr. Mrudula Phadke for her guidance and support throughout the project and the financial support from the Serum Institute of India Research Foundation, Pune. The authors also acknowledge the technical support from the staff of Haffkine Institute for Training, Research and Testing and Maharshi Dayanand College, Mumbai.
Author Disclosure Statement
Amol Chaudhari, Bhagwat Gunale, and Prasad Kulkarni are employed by the Serum Institute of India Ltd, which manufactures Measles, Rubella, MR, and MMR vaccines.