
Abstract
A woman presented with at least four manifestations of varicella-zoster virus (VZV) infection, including central nervous system vasculitis, during her first 2 years of HIV infection. We evaluated her CD4 T cell responses to VZV given the infrequency with which multiple recurrences of VZV occurred, especially following immune reconstitution on antiretroviral therapy.
Background
B
Case Presentation
A 31-year-old woman presented with memory loss, emotional lability, and impulsivity progressing over several months without focal neurologic complaints. Her history was notable for primary varicella 18 months before admission and HZ of the left leg approximately 1 year ago. She was born in the United States, without any significant travel history. She was sexually active with one male partner in the last 2 years, who later disclosed that he was HIV infected; she had tested negative for HIV 2 years before admission. She did not smoke or use illicit substances.
Gadolinium-enhanced magnetic resonance imaging (MRI) of the brain demonstrated T2/FLAIR periventricular enhancement consistent with ventriculitis and her lumbar puncture (LP) had a lymphocytic pleocytosis. Cerebrospinal fluid (CSF) cytomegalovirus (CMV) by polymerase chain reaction (PCR) was positive at 2,800,000 IU/mL and negative for herpes simplex virus (HSV) 1/2, VZV, and human herpesvirus 6. Her HIV antigen/antibody test was positive, plasma HIV RNA level (VL) was 1,747,000 copies/mL, and CSF VL was 22,250 copies/mL. Initial CD4 T cell count was 26 cells/μL. She was initiated on foscarnet and ganciclovir intravenously. ART (tenofovir/emtricitabine/raltegravir) was initiated after 3 weeks of anti-CMV therapy. Plasma HIV RNA became undetectable within 6 weeks of initiating ART.
After 6 months of anti-CMV therapy, complicated by pancytopenia and development of a CMV UL97 mutation resulting in delayed clearance of CMV from CSF, there was no CMV detected in CSF or plasma. She now had a CD4 count of 245 cells/μL. Four weeks after stopping anti-CMV therapy, she presented to an outside clinic with HZ limited to the right L4 dermatome and was prescribed 7 days of oral acyclovir. The lesions healed completely, but she developed somnolence and ataxia over the next month. CSF was notable for 4 red blood cells and 56 nucleated cells/μL (94% lymphocytes). She was reinitiated on foscarnet given concern for recurrent CMV meningoencephalitis, but CSF PCR revealed 470 copies/mL of VZV and was negative for CMV DNA by a sensitive PCR assay. MRI showed improvement compared with initial CMV presentation without new lesions. VZV detected in CSF was interpreted by the treating physicians as a residual consequence of VZV reactivation rather than true CNS disease (9). All symptoms resolved by hospital day 3 and no further antiherpesvirus therapy was administered. She remained well for 3 months off anti-VZV therapy before experiencing sudden onset 2- to 3-minute episodes of paresis and paresthesias in bilateral legs and right arm and word-finding difficulty. Black-blood MR angiography reflected multifocal vessel narrowing and intraluminal enhancement involving left anterior cerebral, bilateral middle cerebral, left posterior cerebral, and left carotid arteries. Repeat CSF evaluation included 12,000 copies/mL of VZV and 64 nucleated cells/μL (97% lymphocytes) and no CMV DNA. She initiated intravenous acyclovir at 12.5 mg/kg thrice daily and a 5-day pulse of methylprednisolone for CNS VZV vasculitis.
She was given a prolonged course of 6 weeks of intravenous acyclovir because VZV DNA was still detectable in repeat LP on day 20 of therapy, followed by transition to valacyclovir at 6 g daily (2 g thrice daily) to target therapeutic CNS levels (17) once VZV was no longer detectable in the CSF. She was later transitioned to valacyclovir at 1 g twice daily, and subsequently once daily for secondary prophylaxis, and continued successful ART. With the exception of mild ongoing ataxia and right arm weakness, she has no residual symptoms and subsequently has done well.
Sixteen months after her initial presentation (4 months after completing IV acyclovir), her CD4 count was 323 cells/μL and plasma HIV remained undetectable. We evaluated her CD4 T cell response to VZV given multiple episodes of severe VZV reactivation in the setting of CD4 T cell reconstitution on ART. We studied circulating CD4+ T cell gamma-interferon (IFN-γ) and interleukin-2 (IL-2) responses to VZV antigen ex vivo to help determine whether she has ongoing deficits in cellular responses to VZV.
Laboratory Methods
Informed consent was obtained. Heparinized blood was collected and peripheral blood mononuclear cells (PBMCs) cryopreserved within 8 h (12). A healthy HIV-negative donor who had received varicella vaccine (Zostavax) with known, VZV-specific CD4 T cell response was used to establish positive control responses for each antigen (13). VZV IgG serostatus was determined as described (13). Additionally, she was seropositive for HSV-1, but seronegative for HSV-2, by type-specific immunoblot.
Whole cell-associated VZV antigen and negative control antigen were prepared as previously described (10,13). PBMC CD4 T cell reactivity to VZV antigen was tested using a modification of published methods. Briefly, PBMCs were stimulated for 18 h with VZV or mock control antigen or phytohemagglutinin (PHA) positive control, with costimulatory antibodies and Brefeldin A. Medium was used as a negative control. Staining, dead cell exclusion, and analysis of cytokine responses were performed as described (13).
Laboratory Results
The subject was VZV IgG seropositive. The CD4 T cell response to whole VZV antigen was readily detectable and similar in magnitude to a healthy HIV-uninfected control who had recently been boosted with live attenuated VZV and to a series of 12 HIV-uninfected healthy persons aged 50 years and above recently studied with the same method (13).
Intracellular cytokine staining assay results were consistent with detection of VZV-specific CD4 T cell responses. Both case and control subjects had very low background reactivity to negative control antigens. Both case and control were similarly reactive to PHA. Net IL-2 and IFN-γ responses (percent of CD4 cells with response to VZV minus response to mock) were similar between participants at 0.9% for the case and 0.4% for the control (Fig. 1).
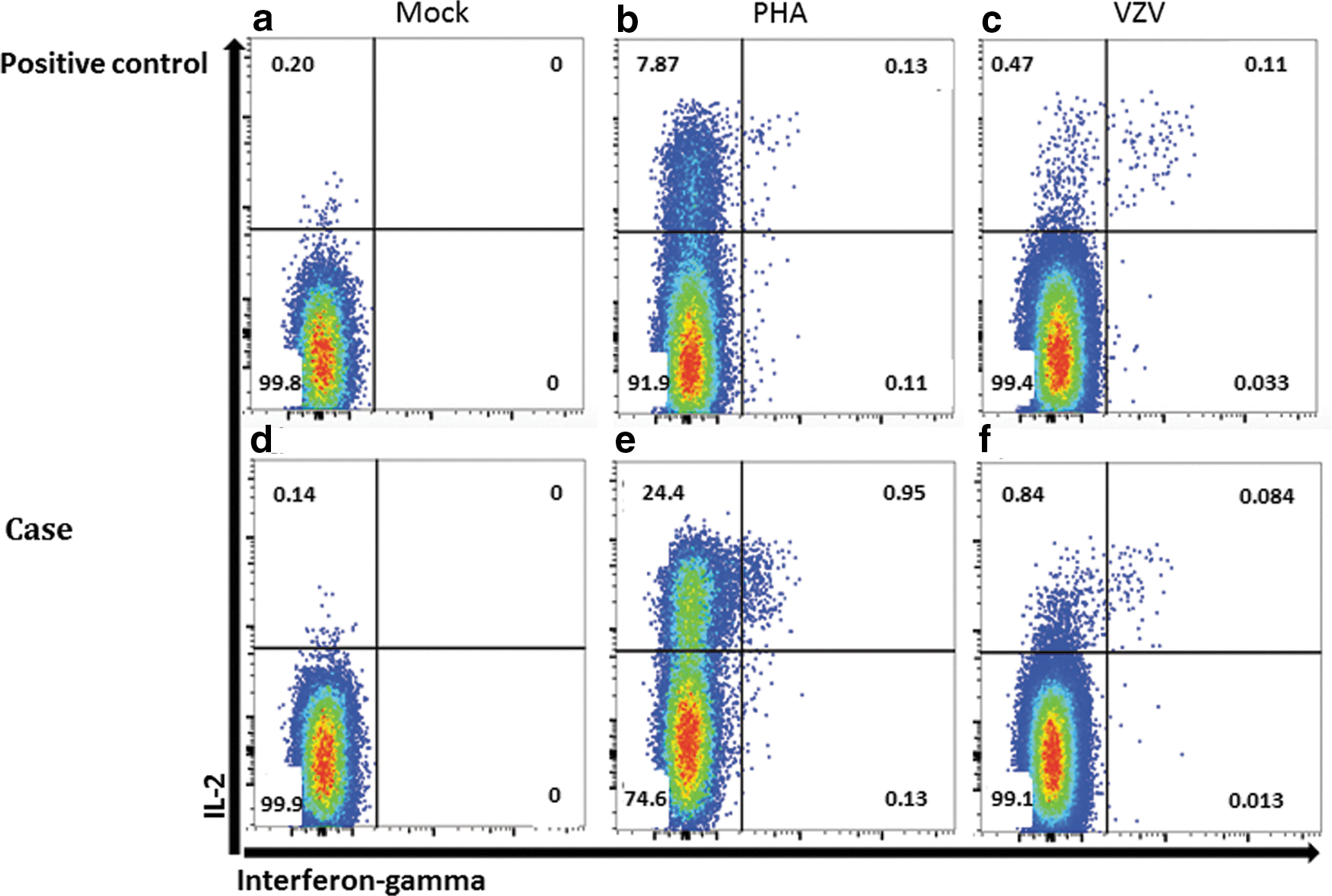
Representative dot plots showing the frequency of cytokine-positive events in CD4+ T cells by intracellular cytokine staining in a postvaccine HIV-negative control participant and the HIV-infected case patient described. Net responses are to a mock control antigen
Discussion
VZV-specific T cells are considered essential to prevent severe or recurrent disease, but options to prevent recurrent VZV in persons with deficient cellular immunity are limited (18). Oral acyclovir has been shown to reduce incidence of first zoster occurrence in HIV-infected persons and following bone marrow transplant, but evidence does not support chronic acyclovir or prodrug to prevent recurrent VZV disease (1,2). Zostavax, the live attenuated therapeutic VZV vaccination, is not FDA approved for HIV-infected patients, but may be safe for those with CD4 count >200 (3,19).
We evaluated cellular responses to VZV in a person who had experienced primary varicella, followed by at least three distinct recurrences within 3 years of their earliest possible date of HIV infection. It is possible that this patient initially did not create a memory T cell repertoire against VZV due to acquiring HIV and primary VZV in short succession or had experienced destruction of this specific CD4 T cell population in the setting of rapidly progressive AIDS. While our experiment does not evaluate the full breadth of immunological response to VZV, we found that the IL-2 and IFN-γ responses of VZV-specific CD4 T cells to whole VZV antigen in our patient were comparable with an HIV-negative control. This relatively normal cellular response brings into question whether immune reconstitution inflammatory syndrome played into the development of CNS vasculitis, an association that is rarely described in the literature (20). Alternatively, it is possible that our case initially had little VZV-specific immunity, and subsequent VZV reactivations improved responses to the virus once on ART. Unfortunately, we were not able to survey her cellular response to VZV before ART initiation or longitudinally during immune reconstitution, nor could we evaluate her response to CMV at those time points.
It is known that CD4 T cells and antibodies are important to prevent VZV reactivation and severe disease, but more studies are needed to elucidate correlates of protective immunity (7,11,14,18). It is unclear if deficits in qualitative or quantitative aspects of cellular immunity predispose to VZV reactivation. Another remaining question is whether, following ART-facilitated immune reconstitution, the expanded but naive CD4 T cell repertoire is able to respond to VZV. This case suggests that this HIV-infected patient, who initially failed to control VZV, later acquired a suitable CD4 T cell response to whole-virus antigen as studied ex vivo. We opted to use secondary VZV prophylaxis with high-dose valacyclovir for this patient following treatment of CNS vasculitis until we had greater confidence in her VZV-specific immunity because of the potentially devastating effects of recurrent vasculitis, adopting concepts from the literature on CMV prophylaxis following transplant (15) without availability of formal guidance for this specific scenario. We therefore used the results of this ex vivo assay to assist our decision on whether she needed lifelong secondary prophylaxis. Although newer data suggest that risk of several opportunistic infections is much more strongly associated with unsuppressed HIV VL than absolute CD4 count, this patient continued to have VZV recurrences with both CD4 >200 and suppressed VL (4,5,21). We therefore conclude that VZV-specific immunity may not always be well predicted by these two traditional risk factors. Better longitudinal data on how to assess VZV-specific immunity are needed in this clinical setting to help delineate populations for whom secondary VZV prophylaxis is still beneficial despite modern ART.
Footnotes
Acknowledgments
The authors would like to thank their patient for agreeing to participate in this work. They thank the Virology Research Clinic at the University of Washington for helping unite their patients and the research laboratory. This work was supported by a grant from the National Cancer Institute at the National Institutes of Health (2T32CA080416-16A1 to R.B.I.) and the National Institute of Allergy and Infectious Diseases (P01AI031731 to K.J.L., C.M.J., and D.M.K.) and a Contract from the National Institutes of Health (HHSN272201400049C to D.M.K.).
Author Disclosure Statement
C.M.J. reports conducting sponsored research with Sanofi Pasteur, Genocea, Vical, and Agenus (research funding paid to University). D.M.K. is a consultant for GlaxoSmithKline and EISAI and conducts sponsored research with Sanofi Pasteur, Admedus Vaccines, Merk, and the Immune Design Corporation (research funding paid to University). All other authors declare that they have no conflicts of interest to report.