
Abstract
Maternal immunization for prevention of morbidity and mortality of pregnant women and their neonates due to infectious diseases is ongoing worldwide. The complexity of vaccine research and development in this population is challenging. Not only do vaccines for pregnant women require evidence of immunogenicity, potency, stability, and limited reactogenicity, they must also provide efficacy in decreasing morbidity for the pregnant woman, her fetus, and the neonate, demonstrate safety or lack of evidence of harm, and offer benefit or potential benefit of vaccination during pregnancy. Since the 19th century, evidence of protective effects of vaccination during pregnancy has been documented. Pandemic influenza and pertussis outbreaks in recent years have affected a paradigm shift in vaccine research and development as well as current policy regarding immunization in pregnancy. Studies of the immune system in pregnant women and neonates have shown that immune changes associated with pregnancy in women do not interfere with maternal vaccine responses, multiple factors are important in transplacental transfer of antibodies, and maternal antibodies are beneficial to neonates. In recent years, guidelines have been developed by expert panels to help design studies for maternal vaccinations and for harmonization of data collection, analysis, and adverse event reporting. Further research into maternal and neonatal immunology, transplacental antibody transfer, and epidemiology of diseases is needed, especially as new vaccines to respiratory syncytial virus, cytomegalovirus, and Group B streptococcus are developed. Maternal vaccinations have the potential to change the epidemiology of infectious diseases in reproductive health and pediatrics and may lead to new clinical applications to improve global maternal and neonatal health.
Introduction
M
Recent outbreaks of pandemic influenza and pertussis, in addition to new developments in vaccine research, have affected a paradigm shift in research and policy regarding vaccination in pregnancy. Maternal vaccinations have the potential to radically change the epidemiology of infectious diseases and may lead to new opportunities and clinical applications to improve maternal and neonatal health globally.
Historical and Current Developments
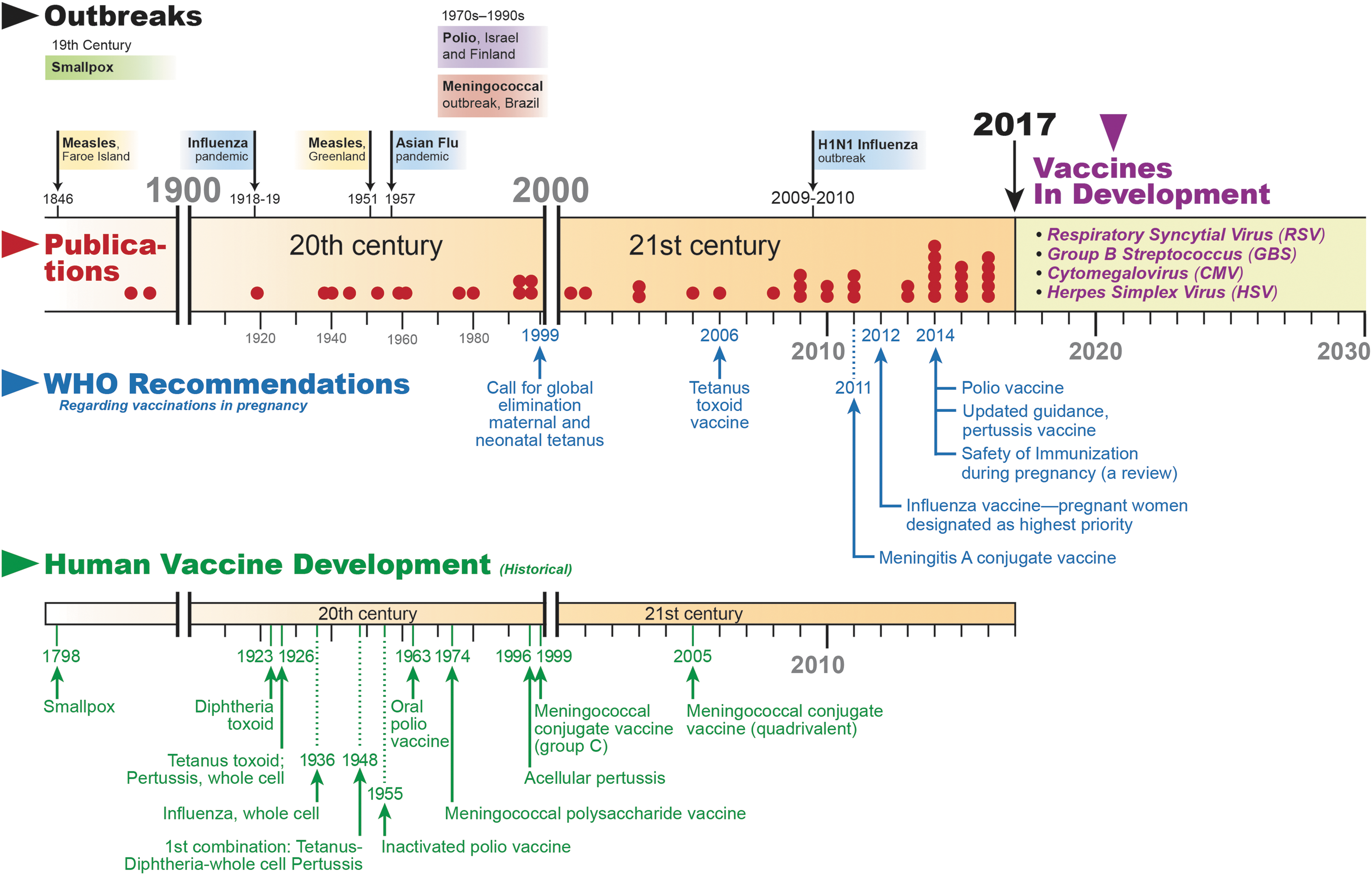
Large-scale development and implementation of vaccines is considered one of the greatest public health achievements of the 20th century. Vaccines for pregnant and nonpregnant individuals have now become part of routine preventive healthcare (86). Observations of the increased morbidity and mortality among pregnant women and their fetuses due to infectious diseases and potential benefits of immunizations, however, began centuries ago. One of the first historic records of the effect of vaccines on pregnancy outcome and maternal immunization, published in the 19th century, demonstrated that smallpox vaccine before pregnancy provided increased protection to immunized pregnant women compared with those who were not immunized (75). A small study published in 1879 showed that administration of smallpox vaccine to pregnant women protected infants against smallpox disease (12).
Increased morbidity and mortality of unvaccinated pregnant women and their fetuses with exposure to a viral illness were demonstrated during measles outbreaks in the Faroe Islands in 1846 and in Greenland in 1951, as well as during the 1918 worldwide influenza pandemic (8,19,37,42,56,76,84,89). In the 1930s and 1940s, reports of beneficial effects of transplacental antibody transfer in preventing neonatal pertussis were published, and, in the 1950s and 1960s, immunization of pregnant women against influenza and polio was recommended, given the high disease prevalence (48,54,60). In 1961, a landmark study of tetanus disease in New Guinea, an important cause of neonatal mortality globally, demonstrated significant neonatal benefit after maternal inoculation with multiple doses of the tetanus vaccine (93,98). In the 1970s–1990s, outbreaks of polio in Finland and Israel and meningococcal infections in Brazil prompted mass immunization campaigns that included pregnant women. Subsequent studies showed no adverse effects of these vaccines to the mothers or their fetuses (40,41,61,67,82).
The worldwide H1N1 influenza pandemic in 2009–2010 demonstrated both the increased risk of mortality among pregnant women infected with the virus and the beneficial effects of maternal influenza immunization (39,97). In more recent years, maternal pertussis vaccination has been shown to be effective in decreasing infant mortality due to pertussis infection via transplacental antibody transfer and by decreasing maternal infection and risk of postnatal infant exposure (Fig. 1) (6).
Currently, routine vaccinations recommended in pregnancy by the World Health Organization (WHO) and national health authorities in the United States, the United Kingdom, and an increasing number of countries include inactivated influenza, tetanus toxoid, and acellular pertussis-containing vaccines (Table 1) (13,16,88,108,110). In addition, WHO's Strategic Advisory Group of Experts on immunizations recommends the meningococcal conjugate vaccine and the yellow fever vaccine in pregnant women who have not yet been immunized and who are at increased risk for endemic or epidemic exposure (113). Hepatitis A and B vaccinations can be administered under certain circumstances (13).
CMV, cytomegalovirus; GBS, Group B streptococcus; HSV, herpes simplex virus; RSV, respiratory syncytial virus.
Live vaccines are not recommended during pregnancy due to theoretical risks to the mother and fetus. These include vaccines against measles, mumps, rubella, varicella, and zoster viruses, as well as live attenuated influenza vaccine. Despite recommendations to avoid live vaccines during pregnancy, adverse effects on fetuses when live vaccines are inadvertently administered during pregnancy have not been found (113). Safety data on less commonly used vaccines are often not available and best practice in these cases is determined by weighing risk of exposure against the theoretical risk of the vaccine in the mother and fetus.
Factors Involved in the Mechanism and Efficacy of Maternal Immunization
The principle of maternal immunization to protect the mother, the fetus, and the neonate relies on multiple factors: the ability of the pregnant woman's immune system to respond to a vaccine and generate high concentrations of antibodies, the ability of the placenta to transfer antibodies from the maternal circulation to the fetal circulation, and the characteristics of the maternal antibodies, including their quantity and quality to fight infections in the neonate. In addition, antibodies generated as a response to the vaccine must be able to sufficiently protect the mother from morbidity due to a pathogen, the fetus from injury due to maternal illness or transfer of pathogen across the placenta, and the neonate from infection given its immature adaptive immune response in the first months of life. Finally, studies of a specific vaccine should not demonstrate harm to mother, fetus, or neonate. The effect of vaccines on very different and yet connected immune systems and hosts adds to the complexity of maternal immunization.
The maternal immune system
Pregnancy is a time during which complex immunological adaptations occur. While the changes in the maternal immune system were previously thought to be due to a primarily T helper cell type 2 response of the maternal immune system to the allograft fetus, pregnancy is now considered to be a time of maternal–placental tolerance during which maternal cells interact with trophoblast cells of the placenta with the goal of protecting the fetus (20,68). To facilitate implantation of the blastocyst and growth and development of the fetus, the immune system of a pregnant woman shifts from a baseline proinflammatory to an anti-inflammatory immune state and then reverts back to a proinflammatory state for parturition (18,120). Adaptation of the activity of maternal immune cells such as natural killer cells, macrophages, and T cells at the level of the decidua allows for implantation of the blastocyst and protection of the placenta and developing fetus (34,73).
Changes in T cell response may also explain the susceptibility of the decidua to cytomegalovirus (CMV) and listeria monocytogenes infections (34,100). Immunologic adaptations are modulated, in part, by increased levels of estrogen and progesterone (120). While a relative decrease in immunoglobulin G (IgG) concentration can be seen in pregnancy, likely due to hemodilution, pregnant women are nevertheless able to mount antibody responses and produce immunologic memory at a similar rate to nonpregnant women following exposure to vaccination or infection (5,52).
Transplacental antibody transfer
Neonatal blood in term infants contains high concentrations of maternally derived IgG at birth due to active transfer of maternal IgG across the placenta. This occurs via FcRn receptors of synchiotrophoblast receptors in the chorionic villi that bind to IgG and facilitate transport and release of IgG into the fetal circulation (26,57,96,102,117). IgG is selectively transported across the placenta while other immunoglobulin types, such as IgM, IgE, and IgA, are essentially excluded. Breast milk contains secretory IgA in high concentrations as well as IgG in lower concentrations, which may have an immunological benefit for newborns via the gastrointestinal tract (36,77). Breast milk antibodies, however, are not absorbed into the infant circulation (64,96,102).
A number of factors affect the transfer of IgG across the placenta following maternal immunization. These include IgG subtype produced following vaccination, timing of the vaccine, fetal gestational age, placental integrity, and total maternal IgG levels (44,83,101). While IgG transport begins in the second trimester, fetal IgG concentrations begin to equal maternal concentrations at 32–36 weeks and surpass maternal levels generally after 37 weeks of estimated gestational age (65).
IgG1, as well as IgG4 and IgG3 at lower levels, is preferentially transported, increasing exponentially during pregnancy. At full term, IgG1 and IgG4 concentrations are higher in the fetus than in the mother. The transport of IgG2 across the placenta also increases during pregnancy, however, fetal concentrations at term are significantly lower than those of the mother (65). The preferential transfer of IgG subtypes explains the greater efficacy of maternal immunization with conjugated Haemophilus influenzae type b (Hib) capsular vaccine, for example, which results in the production of high concentrations of IgG1 antibody to polysaccharide PRP (polyribosylribitol phosphate) (33). By comparison, prepregnancy immunization with the unconjugated form of Hib vaccine, capsular PRP, has been shown to stimulate IgG2 production resulting in lower overall levels of PRP antibody in the infant at birth compared to prepregnancy immunization with the conjugated form (92).
The timing of vaccination affects transplacental antibody transfer. While little is known about antibody transfer in the first trimester, IgG transfer begins in the early second trimester and reaches its peak around 32–36 weeks (65). In 2014, a study on maternal tetanus, diphtheria, and acellular pertussis immunization during pregnancy showed that neonatal antibody titers are higher when the vaccine is administered at 27–31 weeks of estimated gestational age compared with later gestational ages (2). In addition, infants born prematurely have lower antibody titers than infants born at term (47,79).
An increase in neonatal vaccine-specific antibody titers is generally not seen until ∼2 weeks after maternal immunization. Another study demonstrated that transplacental antibody transfer was greatest if delivery occurred 4 weeks following vaccination with the Hib vaccine (33). Neonatal antibody levels were also higher when mothers were immunized in pregnancy compared with prepregnancy immunization (65,69,92). The ideal timing for vaccination has therefore been considered to be early in the third trimester before peak IgG transfer and 2 weeks or more before time of delivery to maximize time for maternal immune response and transplacental antibody transfer (Table 2) (2,33,44,45,57,65,83,92,101).
FHA, filamentous hemagglutinin; FIM, fimbrial proteins; PRN, pertactin; PT, pertussis toxin.
The US Advisory Committee on Immunization Practices (ACIP) recommends maternal immunization against tetanus and pertussis in the third trimester of pregnancy. Recently, a study has suggested increased neonatal antibody titer levels when acellular pertussis vaccine was administered in the second trimester between 13 and 25 weeks of estimated gestational age compared with greater than 26 weeks and the beginning of the third trimester. This could be of particular benefit to infants born prematurely and merits further investigation (28,29). The United Kingdom (UK) Joint Committee on Vaccinations and Immunisations recommendations for maternal immunization with tetanus and pertussis have since been updated to be administered from 16 weeks onward (88). The influenza vaccination is recommended at any point in pregnancy to protect women, given the increased morbidity and mortality associated with influenza in pregnancy (14,112).
Transplacental antibody transfer relies on placental integrity and lack of inhibiting factors. Malarial infection causes injury to the placenta and has been shown to negatively impact IgG transport across the placenta despite the presence of typical concentrations of maternal antibody in the mother. This may occur due to impairment of the Fc receptor (11,35). The placental Fc receptor is similarly thought to be affected in HIV-positive women and the degree of impairment may be associated with viral load level (26,35,51). In addition, high levels of maternal total IgG may inhibit or significantly reduce antigen-specific IgG transfer due to competitive inhibition for the Fc receptor in the chorionic villi (9,26,83).
The neonatal immune system
Infectious diseases are the leading cause of morbidity and mortality among neonates and infants worldwide. Diseases such as pneumonia, diarrhea, and measles are large contributors to under-five mortality (62). The susceptibility of neonates and infants to infectious diseases stems mainly from their immature adaptive immune systems (3). Due to lack of ability to form a mature humoral or cell-mediated response to infections, the neonatal protection against viral pathogens is dominated by the innate immune system with its nonspecific cytotoxic effects (93). This also explains why active immunization is rarely successful in achieving long-lasting and protective antibody titers if vaccines are administered before 6 months of age (59,94). By providing passive immunity to infants, maternal immunization has the potential to significantly decrease morbidity and mortality from vaccine-specific infectious pathogens.
While circulating maternal IgG is transported to the fetus to some degree throughout the latter half of pregnancy, immunization of the mother during pregnancy increases vaccine-specific antibody titers in mothers and therefore also in neonates to allow for effective protection against these pathogens. Studies of pertussis vaccination in pregnancy, for example, have shown significantly higher cord blood concentrations of pertussis-specific antibodies compared with cord blood of mothers who did not receive a booster in pregnancy (45,70). Epidemiologic studies of pertussis cases in early infancy have shown a decreased rate of infection among infants whose mothers received the pertussis vaccine during pregnancy compared with those whose mothers did not receive the vaccine (6,10,24). In addition, if the infant does acquire pertussis, the disease manifestations are less severe. One study demonstrated that compared with infants with pertussis in unimmunized mothers, infants of immunized mothers were less likely to have classic pertussis symptoms, the disease manifested later in life, there were significantly fewer hospital and ICU admissions, and there was no associated mortality (118).
Protective antibody titers and length of protection vary by specific vaccine and by nature of the antigen (87). Most pregnant women have received routine immunizations in the past or have developed natural immunity to pathogens, however, vaccination in pregnancy boosts antibody production, increases transfer of antibodies across the placenta, affects an increased neonatal vaccine-specific antibody titer, and thereby protects neonates from certain infectious diseases in the first months of life.
Recent studies on the neonatal response to vaccination following maternal immunization have focused on the ability of the neonatal or infant's immune system to mount an immune response to vaccinations (49,58,70,103). The inhibitory response of maternal antibodies to infant vaccine responses and length of effect varies from vaccine to vaccine.
Mechanisms of maternal antibody impact on the infant immune response are hypothesized to include rapid neutralization of vaccine antigens after inoculation, inhibition of infant B cell activation by Fcγ-receptor-mediated signaling, elimination of maternal antibody-coated antigens by Fc-dependent phagocytes, and epitope masking by maternal antibodies thereby preventing the binding of antigens to B cells (95). Another more recent theory is that maternal antibodies inhibit neonatal B cell response to antigens by interacting with the inhibitory/regulatory FcγRIIB receptor on B cells. This inhibitory action increases with higher concentrations of maternal antibodies (55,74).
It is thought that infant vaccine responses depend on the maternal antibody to vaccine antigen ratio, which has been demonstrated in studies using high-titer hepatitis A and measles vaccine, although severe side effects were found in the case of high-titer measles vaccine (23,25,95). However, maternal antibodies do not appear to inhibit T cell priming, which has been observed in both animal models and human studies. This results in priming of the infant immune response with the potential for the infant's antibody response to be boosted with subsequent doses of vaccines, depending on the vaccine-specific antigen (30,95).
Benefits and Potential Concerns
For the mother and her fetus
Immunizations during pregnancy can benefit both mother and fetus by allowing for a more robust immune response to infectious pathogens. Specific vaccines that are currently considered for administration during pregnancy include tetanus, pertussis, meningococcus, and polio (Table 1). The protection of vaccines may be especially important depending on season or geographic location. During the H1N1 influenza pandemic, pregnant women and their fetuses were shown to be at increased risk for morbidity and mortality compared with those who were not pregnant (39,80,97). Seasonal influenza was more severe in pregnant compared with nonpregnant women, particularly in those with an underlying medical condition, necessitating hospitalization (22,43). Influenza vaccine may also decrease the risk for influenza-related preterm delivery and small for gestational age birthweight (80). Pregnant women are therefore designated by the WHO as a priority group for the influenza vaccine (112).
From a public health perspective, women are more likely to access healthcare when they are pregnant. Globally, around 80% of women are seen for at least one prenatal appointment. In the years 2007 to 2014, at least 60% of pregnant women worldwide had four or more prenatal visits (107). This increase in utilization of healthcare services during pregnancy provides an optimal window during which women can be immunized.
There is currently no evidence of risk to the mother or the fetus with inactivated or toxoid vaccines during pregnancy. One recently published study showed, in a post hoc analysis, an association between spontaneous abortion after receipt of influenza vaccine in the preceding 28 days in women who had received pH1N1-containing vaccine in the previous influenza season. However, these findings are not supported by other studies, involve a small sample size in a post hoc analysis, and do not prove causality (17,27). No other associated adverse outcomes after administration of the influenza vaccine in pregnancies have been found. Live vaccines are not recommended due to theoretical risks to the fetus (113). The safety of inactivated influenza, tetanus, and pertussis vaccines in pregnancy has been demonstrated in multiple studies (15,53,99,113).
For the neonate
Transplacental antibody transfer is a safe, natural, and effective way to passively immunize and thereby increase the immune protection of neonates. It is also much less expensive than immunoglobulin preparations. Maternal immunizations have been shown to be effective in protecting neonates against multiple pathogens, including tetanus, pertussis, and influenza (6,31,63,93,119). Vaccinations administered during pregnancy can therefore be considered an important part of infectious disease control not only among women but also in pediatric populations (21).
One aspect of passive immunization to consider in neonates is the potential of maternal antibodies to interfere with the infant's response to active immunization within the recommended pediatric vaccine schedule. Maternal antibodies have been shown to affect antibody production after infant immunization with measles, tetanus, pertussis, and pneumococcal vaccines, however, maternal antibody concentrations may fall rapidly enough to allow for typical infant immune responses to vaccine-specific antigens before completion of the immunization series (49,70). Infants born to immunized and unimmunized mothers may have similar antibody titers if they receive a delayed booster dose of vaccine, for example, in the second year of life, resulting in little effect of maternal immunization on the overall response of infants to vaccine (32,49,70,94).
While no clinical significant effects have been found in recent studies, consideration of the effect of maternal immunizations on neonatal and infant response should be given particularly in low-resource settings where no booster vaccines are available and in countries where infant vaccination schedules differ from those in which past immunologic studies were completed (58,70,103). Future recommendations for infant and children vaccination schedules may consider delay of entire series or boosters to counteract any long-lasting effects of maternal immunizations and antibodies. In general, however, the overall consensus is that concerns regarding the infant vaccination response should not impede the study of maternal immunizations to protect neonates in the critical first months of life (95).
Next Steps
Vaccines in development and clinical trials
Several vaccines for use in pregnancy are currently under development. Promising respiratory syncytial virus (RSV) vaccines are being developed, with the RSV F nanoparticle vaccine by Novavax (Gaithersburg, MD) currently in phase 3 clinical trials in pregnant women (
Another target for maternal immunization is Group B streptococcus (GBS). A multivalent conjugate vaccine against GBS by Novartis was recently tested in a clinical trial in South Africa (
Challenges
The design and development of vaccinations for use in pregnancy are a complex, multifaceted process. Obstacles include pregnancy-specific issues such as timing of vaccination, immunogenicity of the vaccine, and half-life of maternal antibodies in the neonate. Regulatory and legal issues in addition to medical–legal liability and risk for vaccine manufacturers continue to be important considerations in vaccine development and implementation. Two of the largest factors in maternal immunization research are safety and ethical considerations, although there is now a paradigm shift underway from protecting pregnant women from research to protecting them through research (90). Nevertheless, acceptability of vaccines during pregnancy by women will remain a challenge, particularly as the number of recommended maternal immunizations increases in the future. To date, no vaccine has been licensed by regulatory authorities for use during pregnancy.
Criteria for recommendation of a vaccination in pregnancy as set forth by the ACIP and the American College of Obstetricians and Gynecologists in the United States are that the specific infectious pathogen poses a risk to the pregnant woman, that there is risk to the fetus or infant, that the infection can be prevented via a safe and effective vaccine, and that the vaccine has the potential to benefit and is unlikely to harm the mother and/or infant (4,21,72). Guidelines for maternal vaccination clinical trial study design and safety assessment in pregnancy have been developed by a panel of experts sponsored by the Division of Microbiology and Infectious Diseases at the National Institute of Allergy and Infectious Diseases, National Institutes of Health, and were published in 2013 (72).
Discussions on regulatory pathways for licensing vaccinations for use in pregnancy have emphasized two unique aspects concerning the assessment of vaccine safety in pregnancy. The first is that despite benefit to mother or infant or both, there may be risk involved. Vaccine studies therefore need to demonstrate safety relatively early before advanced clinical trials are started. The second issue is that complications in pregnancy are common, even in a “low-risk” pregnancy (91). In addition, background rates of adverse events, major congenital anomalies, stillbirths, and miscarriages are not known in many global settings. In regions such as sub-Saharan Africa, for example, where ethical considerations preclude the use of a pure placebo in maternal immunization clinical trials, mathematical modeling may help approximate background rates of adverse events in pregnancy (81). Temporal association and impact of maternal immunization on a pregnancy can also be difficult to discern, and therefore, it is recommended to develop a systematic approach to evaluate causality in these studies (91).
Guidelines for maternal immunization safety data collection, harmonization, analysis, and presentation were developed by the Brighton Collaboration Working Group composed of an expert panel and were published in 2016 (50). Finally, reporting of adverse events in vaccination trials in pregnancy has been hindered by the lack of common definitions for adverse events in mothers and neonates that can be used to compare international or multinational data and to optimally monitor safety in maternal immunization. In 2014, the Brighton Collaboration with the WHO began developing definitions for adverse maternal and neonatal events that could be used across all research settings globally (71). Please see Table 3 for a list of maternal immunization study guidance documents.
Finally, important aspects to consider in maternal immunization studies are the legal factors. As discussed previously, pregnancy complications are not unusual. In countries with high rates of medical litigation such as the United States, pharmaceutical and vaccine manufacturers may be less willing to pursue vaccine licensure and marketing given the high financial risk. Typically, indemnification is required in order for companies to participate in research and development of maternal vaccines. Licensure by a regulatory body such as the US Food and Drug Administration may help mitigate medical–legal issues regarding vaccine trials in pregnancy; however, licensure has not yet been obtained.
Future research
Given the multidimensional nature of maternal immunizations, there are many areas of research that have not yet been fully explored. These range from general basic science topics to specific pathogens to clinical applications to global questions. Recently, a group of experts identified areas with need for further research via surveys. These areas included factors related to immunization during pregnancy, transplacental transfer of antibodies, and protection of fetuses and newborn infants, as well as questions related to the RSV, GBS, and pertussis vaccines (66). Other investigative needs include assessing differences in aspects of maternal immunization between high-, middle-, and low-income countries to prevent global newborn mortality (66,67).
Identified gaps in knowledge regarding pertussis and influenza vaccines in pregnancy involve epidemiology, immunology, and clinical factors. In addition, more studies are needed on acellular pertussis vaccines and whole-cell pertussis vaccines (1). Areas of future research involving GBS and RSV relate to epidemiology of the pathogens, the maternal and neonatal immune responses, and the neonatal and the effect of vaccination on short-term and long-term outcomes (46). Finally, widespread implementation of maternal immunization platforms worldwide will require increasing support for and availability of antenatal maternal care conducted by trained healthcare personnel who have access to vaccines and medical supplies.
Conclusion
Maternal immunization is an area of medicine with a rich history and a bright future. Who is the target? Maternal immunization can and does benefit both the mother and infant. In fact, recent data also show fetal benefit. Factors such as immunogenicity of the vaccines in the pregnant women, transplacental antibody transfer, the benefit to the neonate, and potential adverse effects on mother and infant must all be taken into consideration. New vaccines in development as well as a renewed focus on maternal immunization have led to the identification of important gaps of knowledge for future research.
Challenges that will be faced in future studies include application and utilization of guidelines for study design, data collection, and harmonization and analysis of findings, especially given the increasingly international nature of research collaboration resulting in large multinational trials. Evaluation of risks and benefits, particularly considering the complex nature of pregnancy and maternal immunization, will continue to challenge and inspire efforts to decrease global maternal and neonatal morbidity and mortality in the future.
Footnotes
Acknowledgments
Author Disclosure Statement
A.K. and L.O.E. have no financial conflicts to disclose. J.E. has received research support to her institution from GlaxoSmithKline, Novavax, Pfizer, Novavax, and Chimerix. She has served as a consultant for Pfizer and Gilead.