
Abstract
Hepatitis C virus (HCV) leads to liver cirrhosis and carcinoma worldwide. The data of HCV cirrhotic patients were collected from hospitals of Peshawar in the period from 2015 to 2018. A total sample of 267 patients, in the age limit (>19 and <87 years) were found to be cirrhotic and HCV positive. The samples were analyzed through different tests, that is, raised alkaline phosphatase (410 IU/L), aspartate aminotransferase (209 U/L), and reverse transcription-polymerase chain reaction (PCR) viral load (>5,000,000 IU/mL). The mean and standard deviation (SD) of alanine transaminase and alpha fetoprotein were noted, (121.46 ± 29.23) and (43.09 ± 28.08), respectively. Samples of HCV cirrhotic patients (59.6% males and 40.4% females) were included and their mean age and SD of the patients was 49.62 ± 12.65 years. The Child-Turcotte-Pugh Score system was assessed on the base of liver disease. High blood pressure was observed in 26.2%, low in 40.8%, and normal in 33% of patients. The ascites was recorded high in 59% patients (male 38.6%, female 20.6%) and the level of albumin was abnormal in 64.5% patients. Furthermore, multiplex PCR was run to determine HCV genotypes. The frequency of HCV genotype 3a was 47.9%, 2a and 3b was 11%, 1a was 6%, and 1b was 1%; 4.1% were mixed genotypes and 18.7% were untypable genotypes in these patients. The HCV genotype 3a was found a major prevalent genotype in Khyber Pakhtunkhwa patients and it was observed that the HCV cirrhosis issue was significantly increased in the province.
Introduction
Cirrhosis is a disruption of the normal liver structure due to fibrosis and regenerating nodule that hamper normal liver physiology. The risk factors for cirrhosis are chronic hepatitis C virus (HCV) infection, old age, and excessive alcoholism. Cirrhosis takes an average of 30 years to develop after the HCV infection, although the average period varies considerably from person to person (19,20). Cirrhosis is the cause of 4% annual deaths worldwide (9). HCV has been documented as the major cause of cirrhosis in the developing world, including Pakistan, which has second highest estimated HCV prevalence (1,11). Pakistan has very high hepatitis C to cirrhosis conversion ratio. Currently, Pakistan has 10 million HCV-infected patients who are at risk of developing cirrhosis (5).
Serious complications due to HCV cirrhosis include rectal varices, portal hypertension, ascites, and variceal hemorrhages, of which rectal varices are the most common (29). Cirrhosis causes resistance to blood flow inside the liver and increases blood flow in the portal system, leading to high blood pressure in the portal system. This portal hypertension causes ascite formation. Ascites, the abdominal interstitial fluid accumulation, become a serious issue when coupled with bacterial infection of the peritoneum and hepatorenal syndrome. The condition leads to the formation of portosystemic collateral veins. Esophagogastric varices, due to cirrhosis and hypertension, have 30% risk of hemorrhage and bleeding (10).
HCV, an enveloped single-stranded positive-sense RNA virus of the genus Hepacivirus and family Flaviviridae, is the most common cause of viral hepatitis and cirrhosis. It has a single open reading genome of ∼9.6 kb, encoding a polypeptide of 3,010 amino acids, flanked by an untranslated region at both 5′ and 3′ terminus (21). In the year 2004, annual deaths due to liver cancer caused by HCV and cirrhosis were 308,000 and 785,000, respectively (25).
There are currently six main HCV genotypes (1, 2, 3, 4, 5, and 6) and genotype 1, 2, and 3 are distributed worldwide (4,12,26). In some texts, genotypes 7, 8, 9, 10, and 11 are given as separated genotypes, but there is a consensus now that all these genotypes are subtypes of genotype 6 (24). The prevalence of these genotypes and subtypes in various populations is as follows: subtype 1a is the most common in the United States (18,28) followed by 1b, while 1b is the most common subtype in the Japanese population (18). HCV subtype 2a and 2b are more prevalent in North America, Europe, and Japan than anywhere else, while 2c is restricted and endemic to northern Italy. Genotype 6 and its subtypes have been reported only from South Africa, Vietnam, Hong Kong, and Indonesia. Genotype 5 is reported to be endemic to South Africa. Genotype 4 is prevalent only in North Africa and the Middle East (18,22).
This study was aimed to find the prevalence of HCV-related cirrhosis, and genotypes of HCV in the population of Khyber Pakhtunkhwa, and to compare the findings with reported data.
Materials and Methods
Subjects
A total of 267 cirrhotic patients infected with HCV were selected to study the prevalence of various HCV genotypes. Information regarding the age, gender, area, treatments, diagnosis, blood pressure, and viral loads were taken (from polymerase chain reaction [PCR] test results available with patients charts) after getting written informed consents from the patients, with an estimated time of infection along with address of the patients. The study had the approval of the Ethics Committee, Center of Biotechnology and Microbiology, University of Peshawar. Blood samples were collected from patients at two tertiary hospitals of Peshawar, from February 2016 to May 2018, and serum was stored at −60°C. Auto-Analyzers were used for liver function tests that is, alanine aminotransferase, aspartate aminotransferase, and bilirubin. All the patients were screened for HCV antibodies using the Immunochromatographic Technique kit (Accurate Diagnostics™ Canada) and the sera of patients were tested by enzyme-linked immunosorbent assay by means of commercially available kits (Axen Diagnostic™, Germany).
RNA extraction and complementary DNA synthesis
RNA was extracted from the 150 μL serum according to the manufacturer's protocol by using RNA extraction kit (Favorgene Viral Nucleic Acid Extraction Kit I, Taiwan, Cat. No. FAVNK 001-2). The complementary DNA (cDNA) was synthesized using outer antisense (OAS) primer 1 μL, 10 μL of RNA with 1 μL (200 U) of M-MLV reverse transcriptase enzyme (BIORON Life Science cDNA Kit), 4 μL complete RT buffer, 2.5 μL PCR water, 1 μL dNTPs, and 0.5 μL RNAs inhibitors with total volume 20 μL at 37°C for 60 min followed by 70°C for 10 min in thermocycler. The OAS primer is the reverse primer used in the first round of nested PCR amplification of 5′-untranslated region of HCV.
Qualitative detection and genotyping of HCV
For HCV qualitative detection, nested PCR was used for the amplification of 5′-untranslated region (UTR). The HCV genotyping was performed by multiplex PCR using the procedure of Idrees et al. (14). The 4 μL cDNA was amplified in the first round of PCR using outer sense primer (5′CTCTTACGAGGCGACACTCC3′) and OAS primer (5′CAAGCACCCTATCAGGCAGT3′) of the 5′ UTR. Similarly, 4 μL of first-round PCR product was amplified in round 2 PCR, using inner sense primer (5′GATCACTCCCCTGTGAGGAA3′) and inner antisense primer (5′CTTTCGCGACCCAACACTAC3′). In both the rounds of PCR, 7.1 μL PCR water, 6.9 μL master mix (BIORON Life Science), and 1 μL each primer were used. It was followed by PCR for which the cycling conditions were initial denaturation (2 min) at 94°C and 35 cycles of 94°C (30 sec), 54°C (30 sec), and 72°C (45 sec) and final extension at 72°C (10 min).
After confirmation of the HCV-positive result of 5′ UTR, multiplex PCR was done to determine the HCV genotypes. The first round of multiplex PCR has specific forward and reverse primer. The 4 μL of the first-round PCR product was further amplified by genotype-specific primers (1a, 1b, 2a, 2b, 3a, 3b, 4a, 5a, and 6a) in two mixtures. Mixture-A consists of antisense primers 1a, 3a, 4a, 5a, and 6a, while Mixture-B included the antisense primers 1b, 2a, 2b, 2c, and 3b. The reaction mixture contained 5.5 μL PCR water, 4.5 μL master mix, and 1 μL each primer to make total volume of 20 μL followed by denaturation at 94°C (2 min), 94°C (1 min), and 64°C (1 min), and 72°C (1 min) annealing with final extension at 72°C (10 min) in PCR. Total cycles of round 1 and 2 were 35. PCR products were separated by agarose gel electrophoresis on 1.2% agarose gel stained with ethidium bromide along with 100 bp DNA ladder. The results were visualized under UV transilluminator. The study was approved by the Ethical Committee of the University of Peshawar, Peshawar.
Statistical analysis
The statistical analysis was carried out using the Statistical Package for Social Science (SPSS) 2016 for Windows version 10.0. The results area, gender, age, and genotyping variables were given in the form of mean and standard deviation (SD) (Supplementary Table S1).
Results
In this study, 267 HCV cirrhotic patients were genotyped to find the frequency of different HCV genotypes. The frequency of cirrhosis patients was high in Peshawar (89; 33.3%) followed by Mardan and Kohat with the frequency of 10.5% and 5.2%, respectively. Female (F) patients were 40.4% and male (M) patients were 59.6%; the age group of the patients ranges from ≥19 to ≥87 years and their mean age and SD were 49.62 ± 12.65 years. Patients with <20 years of age were 4.1%, while patients between 21 and 40 years of age were 17.2%. Patients from 41 to 60 years of age were 67.1%, and 10.5% of the patients were in the age of 61–80 years. The socioeconomic status of the patients was also reported in terms of marital, education, and financial status. The married patients were 77%. In addition, 69% were illiterate and 21% of the patients were middle-class citizens. The demographic characteristics and medical data of patients from different districts revealed high prevalence rate of HCV infection among the persons with dental procedures (33.8%), early HCV running in family (15%), surgical operations (11%), and blood transfusion with the least HCV transmission rates (10%). In 28% of the patients, the source of HCV infection was unknown (Supplementary Table S1).
The number of patients on the base of Child-Turcotte-Pugh Score system with 5–6 was referred as Child Class A, 7–9 as Child Class B, and 10–15 as Child Class C of liver disease. The frequency of ascites was high in 157 patients, moderate in 71, and mild in 29. Elevated levels of the liver function tests were recorded and alpha fetoprotein (AFP) level of 151 (57%) patients, including (67 F and 84 M), was <40 ng/mL. The AFP level was in the range of 41–150 ng/mL in 89 patients (33%) (29 F and 60 M), and in 10% (27) of the patients (12 F and 15 M), the level was >150 ng/mL. Albumin level was abnormal in 174 patients (108 M and 66 F) and was normal in 93 (51 M and 42 F) cirrhosis patients. High blood pressure was recorded in 70 patients (26.2%), consisting of 29 females and 41 males, 88 patients (33%) had normal blood pressure values, while 109 (40.8%) had low blood pressure. Spleen enlargement was reported in 171 patients (103 M and 68 F), while 96 patients (56 M and 40 F) had normal spleen in size. The respiratory process was found abnormal in 16 patients (10 M and 6 F), while 251 cirrhotic patients (149 M, 102 F) had a normal respiratory process. Majority of the HCV cirrhotic patients had gastrointestinal problems. The swollen abdomen was observed in 89 patients (57 M and 32 F), and nontenderness in 175 patients (101 M and 74 F). The peripheral HCV RNA load was ranged from as low as 50,000 copies to as high as 9.7 × 108 copies/mL (Supplementary Table S1). Beside these, different complications such as fever, vomiting, diarrhea, constipation, jaundice, and anemia were found during treatment of these patients, as given in Figures 1 and 2 and Supplementary Table S2.
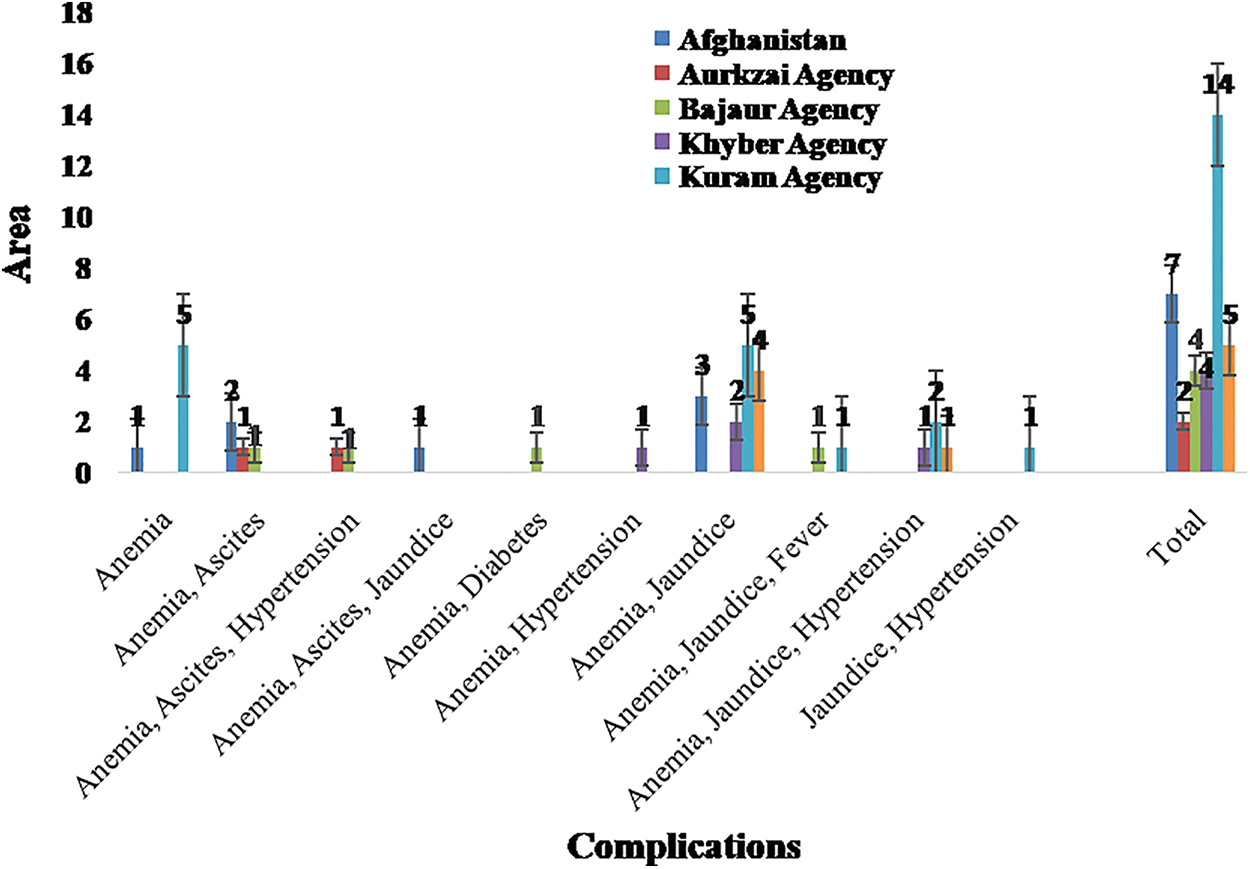
Complications of HCV cirrhotic patients by area. HCV, hepatitis C virus. Color images are available online.
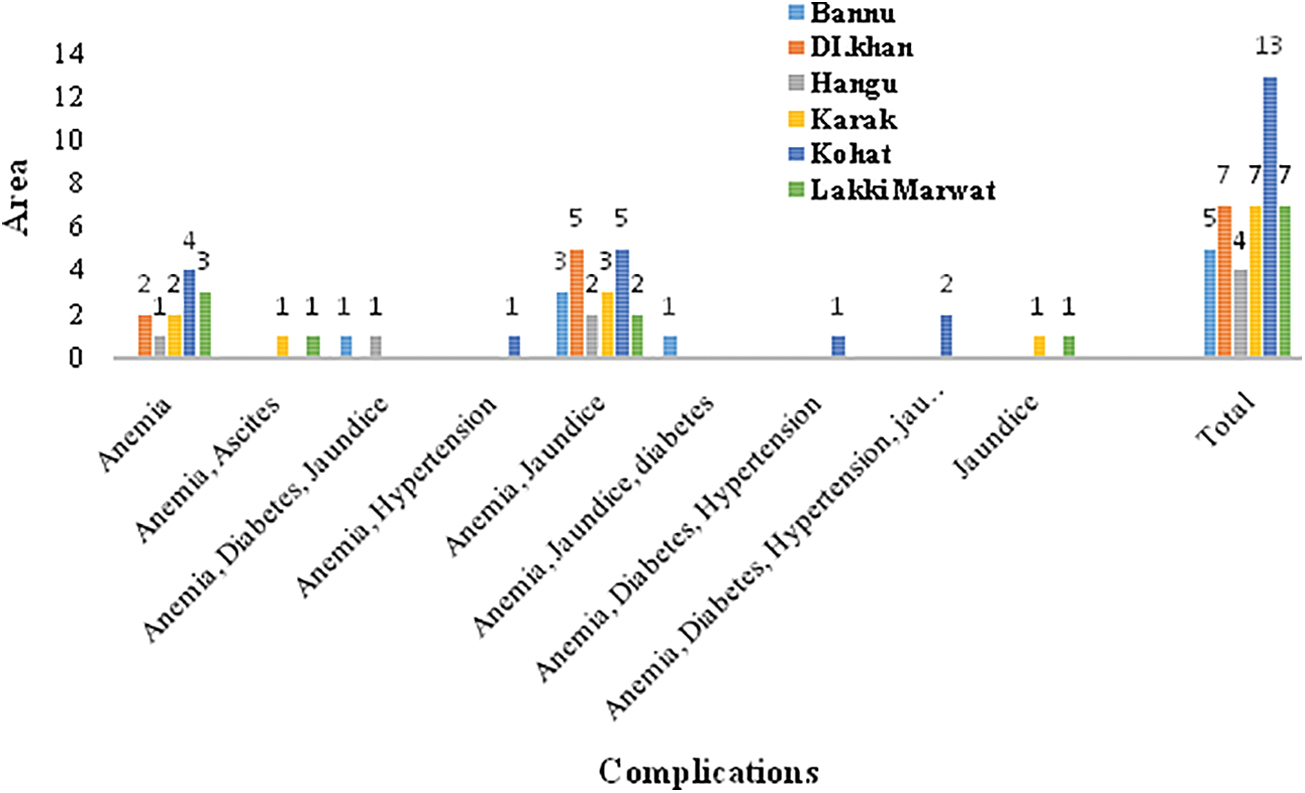
Complications of HCV cirrhotic patients by area. Color images are available online.
Prevalence of HCV genotypes based on area
The blood samples of all selected HCV-RNA positive cirrhotic patients were further subjected for specific genotyping assay. The prevalence of different HCV genotypes reported was as follows: 3a (48.3%), 3b (10.5%), 2a (11.2%), 1a (6%), and 1b (1.1%). In 50 patients (18.7%), the genotype was untyped, while 11 patients (4.1%) showed mixed infections of HCV genotypes. The highest frequency of HCV-induced cirrhosis was noted in Peshawar area (89), where the genotype frequency was as follows: 36 patients with genotype 3a, 4 patients with genotype 1a, 8 patients with genotype 2a, 1 patient with genotype 2b, 13 patients with genotype 3b, 5 patients with mixed genotypes, and 22 patients with untyped genotype (Table 1).
Distribution of Hepatitis C Virus Genotype by Area
”—” symbol shows zero value.
There were 28 HCV cirrhotic patients (10.8%) from Mardan with genotype distribution as follows: 8 patients with 3a, 5 patients with 3b, 4 patients with 1a, 3 patients with 2a, 1 patient with1b, 1 patient with mixed genotype, and 6 patients with untyped genotype. A number of patients reported from Kohat and Kuram Agency were 14 from each district. Genotype distribution in Kohat was follows: 3a genotype was observed in 3 patients, untyped genotype in 5 patients, 2a genotype in 2 patients, and 3a genotype in 1 patient. Mixed genotype was observed in one patient, and genotype 1a was present in two patients. In Kuram, 3a genotype was observed in eight patients, untyped genotype in two patients, 2a genotype in two patients, 3a genotype in one patient, and 1a genotype in one patient. Genotype 1b was not reported in Kohat and Kuram.
There was a total six HCV cirrhotic patients from Abbottabad with one patient having genotype 2a and five patients having genotype 3a infection. There were five patients each from Bannu, Waziristan, and Swabi districts. Genotype 1a and 1b were present in one patient each from Waziristan and both of the genotypes were absent in patients from Bannu and Swabi. Genotype 2a was not found in Waziristan patients, but was reported in Bannu and Swabi districts in one and two patients, respectively. Genotype 3a was recorded in three patients from Bannu, five patients in Swabi, and two patients from Waziristan.
Thirteen patients were reported from district Charsada, where two patients had HCV genotype 2a, five patients had genotype 3a infection, and genotype 3b was found in one patient. Mixed genotype was present in two patients, while three patients were untypable. There were seven patients each from the districts Lakki Marwat, Karak, Dir, DI Khan, and Afghanistan. Genotype 2a was recorded in two patients in district DI Khan, Afghanistan. Genotype 3a was found in one patient from Afghanistan, four patients in DI khan, five patients in Dir, and six patients in Lakki Marwat. The genotype of two patients from Afghanistan and one patient each from these districts was untypable. There were four patients each from Hangu, Bajaur, and Khyber agency. Genotypes 1b, 3b, mixed, and untypable were not reported in these districts. Genotype 1a was found in one patient from Khyber Agency. Genotype 2a was present in one patient each from these districts. HCV genotype 3a was reported in three patients each of Bajaur and Hangu, and two patients of Khyber Agency. A total of 11 HCV patients were reported from district Swat, where 1 patient had genotype 1a, 2 patients had genotype 2a, and 3 patients had genotype 3a infections, 1 patient had the mixed genotype, and in 4 patients, the genotype was untypable.
There were eight patients from Mansehra, in which five patients had 3a genotype, two patients had the 3b genotype, and in one patient the genotype was untypable. There were 10 patients from Malakand where 2 patients each had genotype 2a and 3b, and 6 patients had 3a genotype. Battagram and Orakzai agency had 1 and 2 patients of HCV genotype 3a, respectively. In total of 267 cirrhotic patients, male patients were 159, while female patients were 108. Genotype 3a was most commonly found among female patients (22.1%), genotype 2a was present in 5.2% patients, genotype 3b was found in 3.4% of patients, mixed genotype (3a + 3b, 3a + 2a) was found in 1.9% of patients, genotype 1a was present in 0.7% female patients, and genotype 1b was present in 0.4% patients, and in 6.7% patients, the genotype was untypable (Table 1).
Gender-based prevalence of HCV genotype
In all the HCV cirrhotic patients, genotype 3a was most common genotype in male patients (26.2%), genotype 2a was found in 6% patients, genotype 3b was present in 7.1% patients, genotype 1a was found in 5.7% patients, and genotype 1b was present in 1.1% patients, 2.2% of the patients had mixed genotype, and the genotype of 12% patients was untypable. Genotype 3a is the predominant HCV genotype in both male and female cirrhotic patients from Khyber Pakhtunkhwa (Figs. 3 and 4). The frequency of genotypes 1a and 3b was higher in male patients compared to female patients.
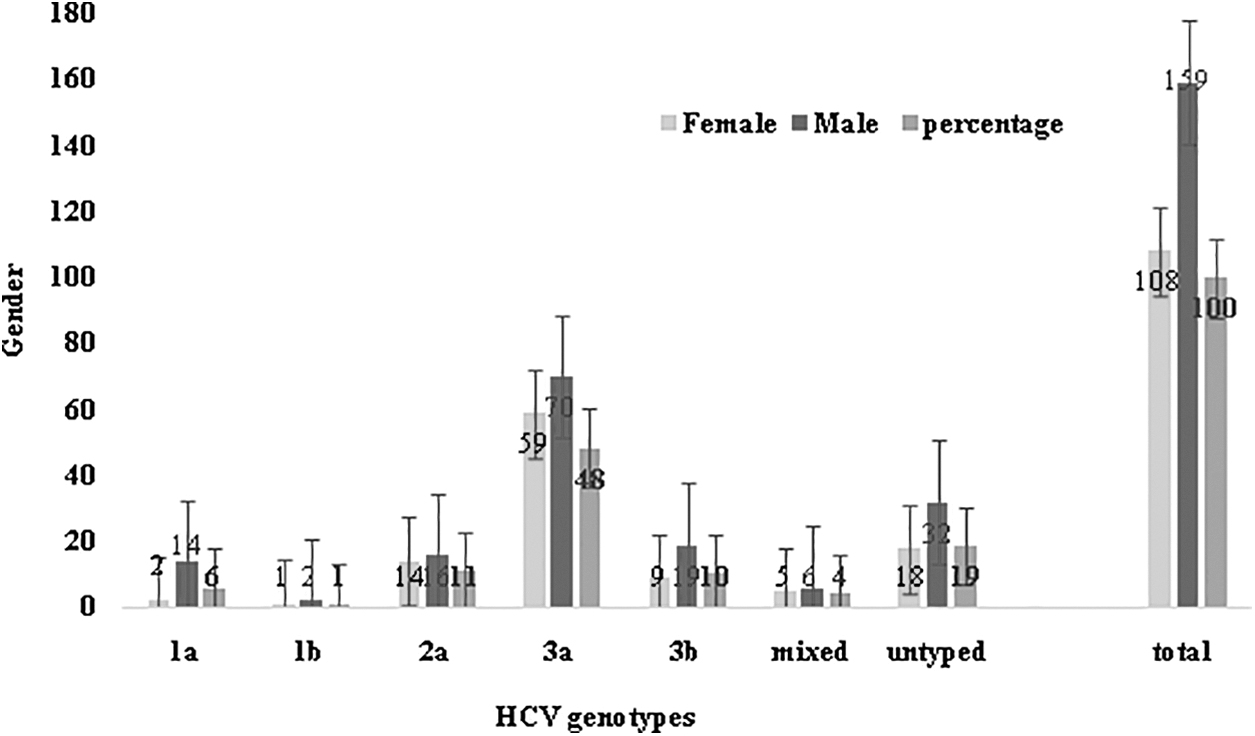
HCV genotypes based on gender distribution.
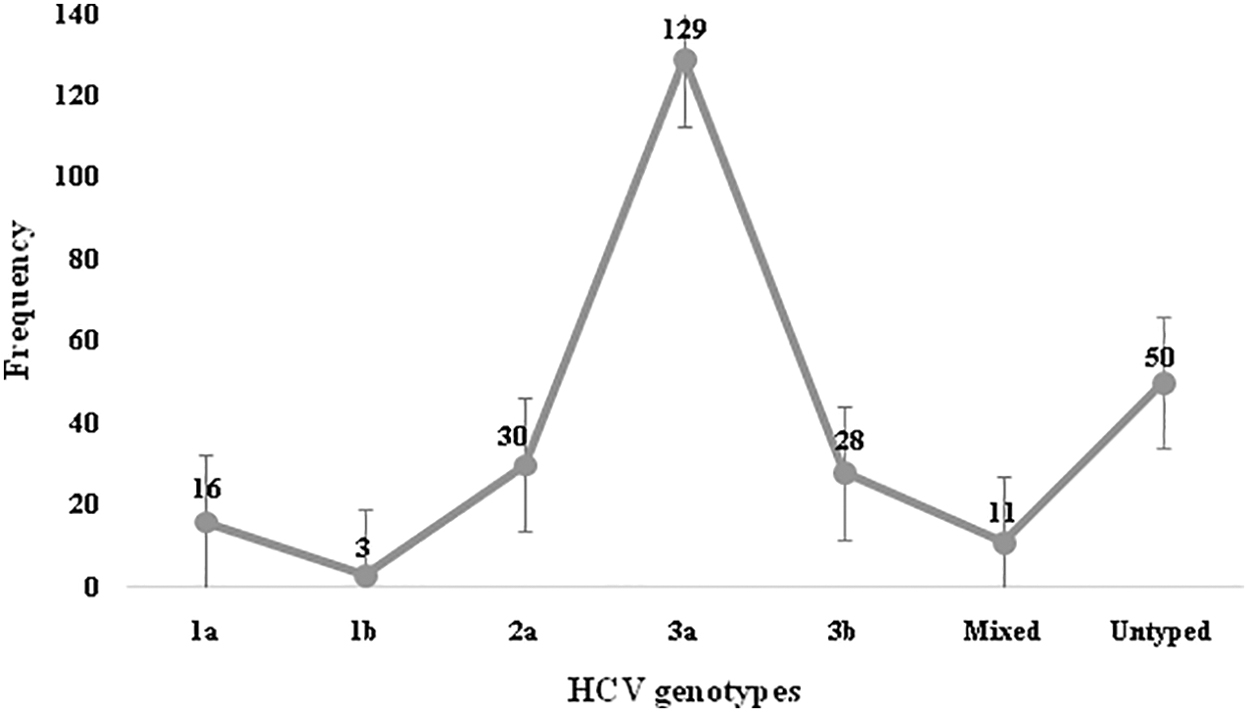
Frequency distribution of genotypes in patients (n = 267).
Prevalence of HCV genotype based on age
A total of 11 HCV cirrhotic patients were in the age group of <20 years with 7 patients of genotype 3a, 3 patients had genotype 3b, and 1 patient was untypable. Forty-six patients were in the age group of 21–40 years, in which 17 patients had genotype 3a, 8 patients had genotype 1a, 1 patient had genotype 1b, and 3 patients had genotype 3b, 2 patients had a mixed genotype infection, and in 9 patients, the genotype was untypable. A total of 179 HCV cirrhotic patients were in the age group of 41–60 years, in which 85 patients were genotype 3a, 7 patients were genotype 1a, 2 patients were genotype 1b, 21 patients with genotype 2a, and 21 patients with genotype 3b, 7 patients had mixed genotype infection, and in the remaining 36 patients, the genotype was untypable. HCV cirrhotic patients in the age group 61–80 years were 28, in which 20 patients were with genotype 3a, 1 patient each had genotype 1a and genotype 2a, and 2 patients had mixed genotypes infection, while 4 patients were untypable. There were three patients in the age group >81 years, in which one patient had genotype 3b infection and two patients had genotype 2a infection (Fig. 5).
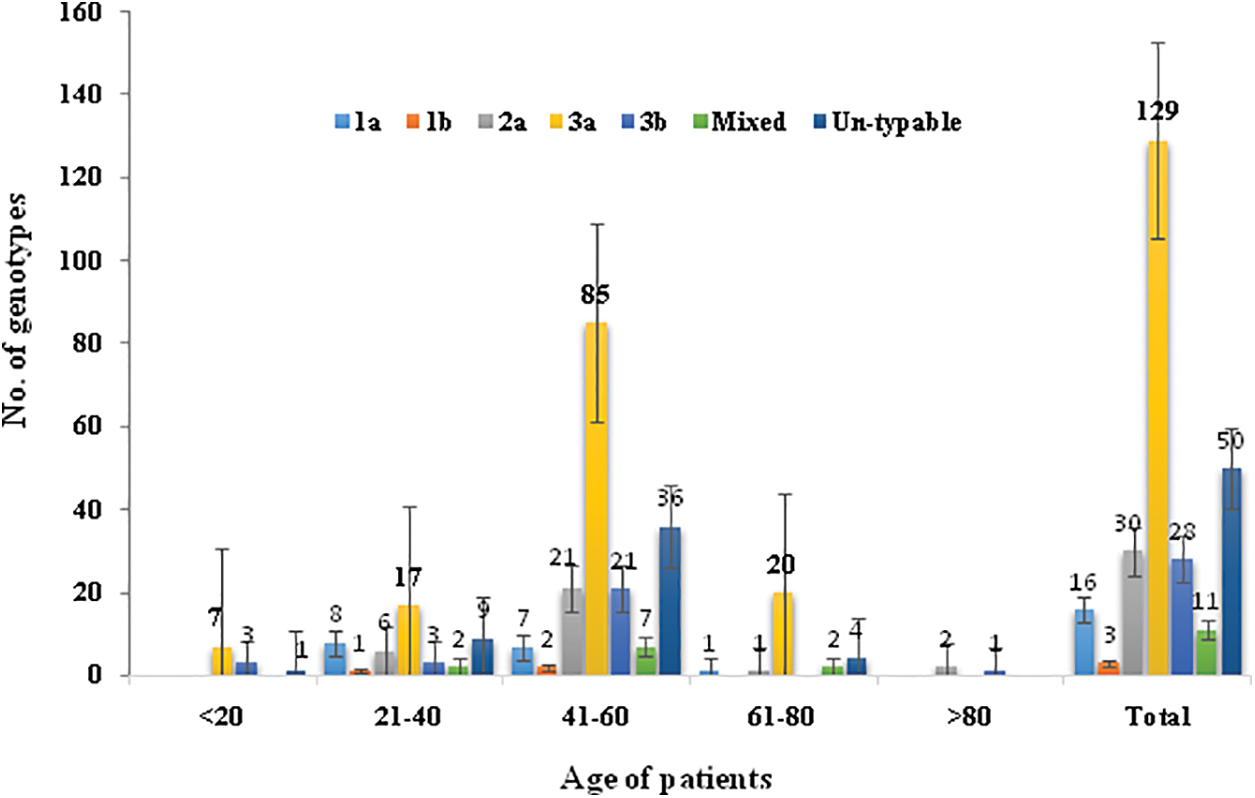
Distribution of HCV genotypes by age. Color images are available online.
Discussion
Hepatitis C patients have a greater risk of developing the chronic liver disease and liver carcinoma (27). Hepatitis C has no demarcating clinical features and the initial symptoms vary from person to person, depending on age, gender, and HCV genotype, or may not be evident at all. This study was carried out in Khyber Pakhtunkhwa, which is one of the four administrative provinces of Pakistan, located in the northwestern region of the country along the international border with Afghanistan. The focus of the study was to determine the prevalence of HCV cirrhotic patients who had proceeded to liver cirrhosis and their genotypes.
The main source of HCV infection reported are the needles and swabs used at dental clinics, which account for 33.97% (82) of the patients. Previous family history of HCV, blood transfusions, surgeries, and unknown sources account for 23.97% (64), 4.11% (11), 10.86% (29), and 28.05% (75) of the patients, respectively. Aziz et al. also reported the dentistry tools as the main source of HCV infection in patients from Punjab, Pakistan (5). Similar studies have also demonstrated the route and source of transmission (7), blood transfusion, as well as sedentary lifestyle to be associated with HCV infection among the Pakistani population (8).
HCV genotype 3a was reported by Butt et al. (6) to be the predominant genotype (screened from 62% to 70% patients). Increase in the prevalence and spread of genotype 3a has been reported in the years 2000–2009 (6). This study was carried out to get a recent update about the prevalence of the various HCV genotypes among the different districts of KP, as it will help to guide the therapeutic choices and identify the prognostic implications of HCV infections. In this study, the predominant HCV genotype in patients was genotype 3, with a prevalence rate of 128 (47.9%). Idrees and Riazuddin (2008) studied 3,351 HCV-infected patients, in which 1,664 patients (49.7%) had genotype 3a, 592 patients (17.7%) had genotype 3b, 280 patients (8.4%) had genotype 1a, 252 patients (7.5%) had genotype 2a, 101 patients (3.0%) had 1b, and 50 patients (1.5%) had genotype 4 (14). HCV Genotype 3 has also been reported as the most prevalent genotype in India, Nepal, and Bangladesh (17,23,24). A high prevalence of HCV genotype 3 is reported here in the different areas of KP (Table 1), which is similar to the reports of Idrees et al. (13) and Afridi et al. (2). Contrary to the previous reports, the untypable genotypes in our study are considerably high (2,13).
In the recent study, Akhtar et al. reported genotype 3 as the most frequent genotype, followed by genotype 2a in a total of 3,800 HCV patients of KP (3). The increase in relative frequency of genotype 3a may be associated with the reuse of syringes for antibiotics, vitamins, or drugs, one of the major sources of transmission for genotype 3a, given the fact that Pakistan has the highest reusage frequency of injections (more than nine injections per year per individual on average) (14 –16).
It has been observed that the frequency of HCV genotype 1a (6%) and genotype 1b (1%) decreased in the HCV patients of KP compared to the previous reports. It is worthwhile to mention that these two genotypes (especially 1b) are considered a poor responder to antiviral therapies compared to other genotypes. The primer set used for the HCV genotyping did not amplify the viral genome of 50 patients (18.1%), so these HCV genotypes were found untypable by this genotyping system. These undetectable HCV genotypes may be new subtypes, which may be beyond the scope of the currently used genotyping methods. HCV genotypes 4, 5, and 6 were not detected in these patients. In the study of Butt et al., (6) the genotype 4, 5, and 6 were reported with less frequent genotypes in Punjab.
Genotype 2 was the second most frequent HCV genotype in the HCV patients studied here. Mixed HCV genotype infections were found in 11 (4.1%) individuals, which suggests that a person suffering from one HCV genotype may also be at risk of acquiring infection with other HCV genotypes (15). The frequency of individuals suffering from mixed infections is comparable to the report of Idrees et al., with 4.8% prevalence of mixed HCV genotype infections in Pakistan (14).
Conclusions
This study reports HCV genotype 3a as the most prevalent genotype in the HCV cirrhotic patients of KP, Pakistan, with the majority of the patients in the age group of 41–60 years. These findings may suggest for the specific genotype-based anti-HCV therapy and monitoring HCV infections.
Footnotes
Acknowledgments
We are thankful to all the persons who participated in the study and the staff in Hayatabad Medical Complex and Khyber Teaching Hospital, Khyber Pakhtunkhwa, for their assistance in data and sample collection. The authors are highly obliged to Dr. Margarete Odenthal, Professor in Institute of Pathology (Laboratory of Translational Molecular Pathology) University Hospital, Cologne, Germany, for the helpful discussion and proofreading of the article.
Ethics Approval and Consent to Participate
The study was approved by the Ethical Committee of the University of Peshawar, Peshawar. Written informed consent was obtained from all the individuals who participated in the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Authors' Contributions
A.U. and B.A. conceived the study and design, and A.U. did the experiments and wrote the article. All the authors participated in the experimentation and optimizations. S.A. and I.u.R. reviewed the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.