
Abstract
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, which caused the coronavirus disease 2019 (COVID-19) pandemic as declared by the World Health Organization, has created havoc worldwide. The highly transmissible infection can be contained only by accurate diagnosis, quarantining, and exercising social distancing. Therefore, quick and massive deployment of SARS-CoV-2 testing plays a crucial role in the identification and isolation of infected patients. Reverse transcription-polymerase chain reaction is the gold standard for COVID-19 detection; however, it needs expertise, facilities, and time. Hence, for the ease of population-wide screening, serology-based diagnostic assays were introduced. These can help determine the prevalence of infection, understand the epidemiology of the disease, and assist in suitable public health interventions while being user-friendly and less time consuming. Although serological testing kits in markets soared, their sensitivity and specificity were questioned in reports from different parts of the world. In this article, we have reviewed 40 Food and Drug Administration (FDA) and CE-approved clinically evaluated serological kits (8 enzyme-linked immunosorbent assay [ELISA] kits, 10 chemiluminescent immunoassay [CLIA] kits, and 22 lateral flow immunoassay [LFIA] kits) for their sensitivity and specificity and discussed the apparent reasons behind their performance. We observed appreciable sensitivity in the kits detecting total antibodies compared to the kits targeting single isotype antibodies. Tests that determined antibodies against nucleocapsid protein were found to be more sensitive and those detecting antibodies against spike protein were found to have greater specificity. This study was conducted to help the decision-making while acquiring antibody kits and concurrently to be mindful of their shortcomings.
Introduction
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), which originated in China in December 2019, is a novel virus belonging to the genus Betacoronavirus (27). This virus is responsible for the coronavirus disease 2019 (COVID-19) that was declared as a Public Health Emergency of International Concern (PHEIC) on January 30, 2020, and a pandemic on March 11, 2020, by World Health Organization (WHO, Diagnostics). As of April 30, 2021, it has infected 234 million people worldwide and 33 million people in India (92).
SARS-CoV-2 is primarily transmitted through direct contact and droplets generated from phlegm when an infected person coughs, sneezes, or exhales. Even though some asymptomatic people may be able to spread the virus (34), the most common clinical manifestations of COVID-19 include but are not limited to dry cough, fever, vomiting, diarrhea, shortness of breath, and myalgia. As a fraction of patients is prone to serious complications like acute respiratory distress syndrome and cytokine storm, they may be a victim of COVID-19 caused death (30,95). The elementary symptoms are similar to those caused by influenza or the common cold and may often remain overlooked and undiagnosed.
Therefore, the most crucial aspect of the current scenario is to have an early, efficient, and accurate diagnosis of the disease preferably during the early stages of infection to pinpoint COVID-19 patients from those with other illnesses. This process ensures isolation of the confirmed and suspected people, faster treatment times, and timely quarantining to avoid the further spread of infection (76). The current race to develop cost-effective test kits and efficient laboratory techniques for confirmation of SARS-CoV-2 infection has fuelled a new frontier of diagnostic innovation. Therefore, understanding the immunological aspect of the infection combined with the diagnostic performance of different serological assays for SARS-CoV-2 based on sensitivity and specificity is essential in the fight against the pandemic.
As it's been more than a year since the virus emerged, there are >130 million subjects globally with confirmed COVID-19 infection and 2 million deaths recorded globally. Apart from taking a dramatic toll on human physical and mental health, this pandemic has significantly impacted daily life and created ripples with huge psychosocial implications on a global scale (65,92). Therefore, during this public health emergency, it is of utmost importance to screen and diagnose patients quickly to aid containment of the infection.
Even though the reverse transcription-polymerase chain reaction (RT-PCR) test is the gold standard in COVID-19 diagnosis, it demands a laboratory setup and a trained health care professional to collect the specimens. This is generally not possible in most countries that have weaker health care infrastructures making the test less feasible for population-wide screening (49). Antibody tests can address the above issue to an extent, and effective serology testing can play a crucial role in identifying individuals with the infection helping in assessing the prevalence of the same in the region.
Acknowledging the usefulness of serological tests in the surveillance of the infection in a community, the Centres for Disease Control and Prevention (CDC) has published guidelines for their usage in both clinical and public health domains (32). CDC is not alone in taking this leap; organizations like International Federation for Clinical Chemistry and Laboratory Medicine (IFCC) and many countries, including India, Peru, and Singapore, have extended their testing strategy with antibody-based rapid tests (9,19,38,39,47,59,65,73).
Consequently, the use of these rapid kits has relieved the backlog, relaxed the waiting time for molecular testing, while aiding the tracking of individuals exposed to viruses at a population level and breaking the chain of transmission to an extent. In addition to the epidemiological perspective, studying the seroprevalence with such kits helps to understand the frequency of asymptomatic transmission and the risk factors associated with the disease (25).
In this study, we are summarizing the immunological aspects of SARS-CoV-2, shedding light on early and competent diagnostic requirement and reviewing the clinical performance of serology based assay kits available for detecting SARS-CoV-2 antibodies. For well-defined and patient-centric guidelines, a better understanding of our immune response to SARS-CoV-2 and its level and duration of protective immunity combined with a study of the advantages and limitations of commercially available serologic assays is essential.
Immune Response Evoked by SARS-CoV-2 Infection
After the invasion of a virus, the immune system of a host produces antibodies to fight against the virus (56). Understanding the nature of an immune response to the infection helps find strategies to eliminate the invader (75). In the known coronavirus family, six viruses have been found to be pathogenic; four of them cause mild respiratory symptoms, while SARS-CoV and Middle East respiratory syndrome corona virus, responsible for the outbreaks in 2003 and 2012, respectively, cause severe respiratory symptoms. The emergence of SARS-CoV-2 made it the seventh member of the list of pathogenic coronaviruses and the third zoonotic virus in the CoV family (46).
There are four structural glycoproteins present in SARS-CoV-2, namely Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N) glycoproteins. The S protein is transmembrane and is cleaved into S1 and S2 subunits by Furin-like protease present in the host cells. While the S1 subunit is involved in the binding of the virus to the angiotensin-converting enzyme (ACE2) receptor present in the lower respiratory tract, the S2 subunit mediates the virus fusion in transmitting host cells.
The N protein is bound to the nucleic acid material of the virus and is involved in the functions related to the viral genome, viral replication cycle, and the cellular response of the host cells to the viral infection. The M protein determines the shape of the viral envelope and stabilizes the viral assembly. The E protein is the smallest among the structural proteins and it plays a crucial role in the production and maturation of the virus (2). On assessing the members in the CoV family, S and N structural glycoproteins appeared to have important antigenic sites for the development of serological assays (81). Serological methods for detecting serum antibodies against spike and nucleocapsid proteins of coronavirus have been established (15,28).
A rapid and well-coordinated immune response is the first line of defense against a viral infection. SARS-CoV-2 activates both innate and adaptive immune responses. Findings from the studies conducted in severe COVID-19 cases suggest that there is a reduction in T helper and suppressor cells (14). One of the indispensable aspects of T-cell mediated immunity is the differentiation of naive T helper cells into effector and memory subsets. The balance between naive T helper cells and memory T cells is elementary to maintain an efficient immune response (66). Among T helper cells, a decrease in regulatory T cells (involved in regulating inflammatory allergic responses at the mucosal surface) and memory cells has been observed, whereas an increase in naive T cells was noted in COVID 19 cases (14,66).
In many viral infections, B cells are activated by T helper cells (thymus-dependent activation). The antibodies produced as a result of a viral infection are crucial in restricting the infection's spread (75). In the case of B cells, naive B cells have been observed to decrease; however, the plasma cells have been found to increase significantly in COVID-19 patients (91).
Characterization of the immune response against the infection indicated that the primary immune response is associated with IgM antibodies, which can be used to diagnose acute exposure to an immunogen, thus making IgM antibodies markers of current or recent infection. This is followed by IgG, which persists for weeks to months and is responsible for long-term immunity or immunological memory and is a marker of recent or postinfection.
Serum levels of IgA tend to be higher than IgM but are considerably lower than IgG. At the mucosal surface, IgA eliminates pathogens either by preventing their binding to the mucosal surface or by direct neutralization. Thus, IgA levels at the mucosal surface are higher than IgG (44,70). Observations from the viral infection studies can form a pattern; viruses at the mucosal surface evoke secretory IgA response, followed by transient IgM and further by IgG antibodies (48).
The kinetics of antibody development varies from individual to individual (28). Antibodies specific to SARS-CoV-2 can be detected in the serum of ∼40% COVID-19 patients as early as 7 days after the onset of symptoms. The seroconversion quickly elevates by day 14 to ≥90% (40). On comparing the onset of seropositivity between antibodies against N protein and receptor-binding domain (RBD) of S protein, it was observed that at a relatively early stage of infection, more patients developed detectable amounts of antibodies against RBD compared with N protein. A lower anti-RBD IgG level was observed among patients with comorbidities (83).
Unsurprisingly, shorter median seroconversion was observed for short incubation period patients of COVID-19. Likewise, median seroconversion was longer for longer incubation period patients. Six days after the onset of infection, antibody levels in the blood have been observed to increase followed by a decline in viral load (44).
Role of Antibodies in Virus Clearance
After being infected by the SARS CoV-2, the immune response of a host is initiated by the innate immune system followed by the activation of antigen-specific B and T cell responses. The mechanism through which the infected individual is protected, followed by pathogen clearance, is through neutralizing antibodies (NAbs) in almost all acute diseases (3). Nevertheless, studies on humoral immune response against viral infections indicate multifacet functional pathways of antibodies involved in many inhibitory mechanisms, out of which, one is virus neutralization (51).
Generally, NAbs exert a protective function by blocking the binding of the virus to cellular receptors thus preventing the virus from entering cells (3,36). They have also been identified to have functions that prevent conformational change, which is crucial for proteolytic cleavage or fusion of a virus with the cell membrane. In addition to that, NAbs can recognize antigens on infected cells, targeting external proteins of the virion which is likely to be expressed on infected host cells (3,75).
These antibodies, in the case of SARS-CoV-2, have been detected in a study from days 10 to 15 after the onset of the disease and remained thereafter (93). Titers of NAb have been associated with several Nucleocapsid protein-specific T cells (55). Furthermore, a functional analysis of RBD within Spike protein of SARS-CoV-2 revealed that RBD can induce excellent immunogenicity and lead to the production of NAbs in mice (96). Compared with other viral infections, COVID-19 patients produce less NAbs than non-neutralizing ones (65). Variation in titers of NAb has also been observed in COVID-19 recovered patients (55). In a study, it was seen that elderly patients were most likely to have high titers of NAbs compared to younger patients (93).
Although NAbs are vital in virus clearance and confers protectivity against viral infections, they aren't the only way of protection (3,93). Research on the humoral response after infection and vaccines suggested that NAbs and non-neutralizing antibodies (nNAbs) should be considered as having complementary or synergistic humoral effector functions (23). These non-neutralizing but protective antibodies are involved in tagging the infected cells for destruction by effector cells before it buds. Through antibody-dependent cellular cytotoxicity (ADCC) or by agglutination of virions or complement-mediated cytotoxicity, these infected cells can be targeted and destroyed by effector cells (53). Thus, along with NAb, nNAb is indispensable for the prevention and clearance of infections.
Early and Competent Diagnosis as a Way Forward
The pandemic caused by SARS-CoV-2 is indisputably the biggest health care challenge of this decade. Thus, limiting its spread takes the center stage when we address the possible ways of overcoming this havoc (28).
Epidemiological determinants, which we can rely upon to understand the gravity of an epidemic, include the interval between infection and onset of symptoms, onset of hospital admission, and extent of contact mixing with a susceptible population (16). To estimate these determinants and further limit the spread of the virus, early and accurate diagnosis along with appropriate quarantining of infected individuals is of utmost importance (28) (Fig. 1).
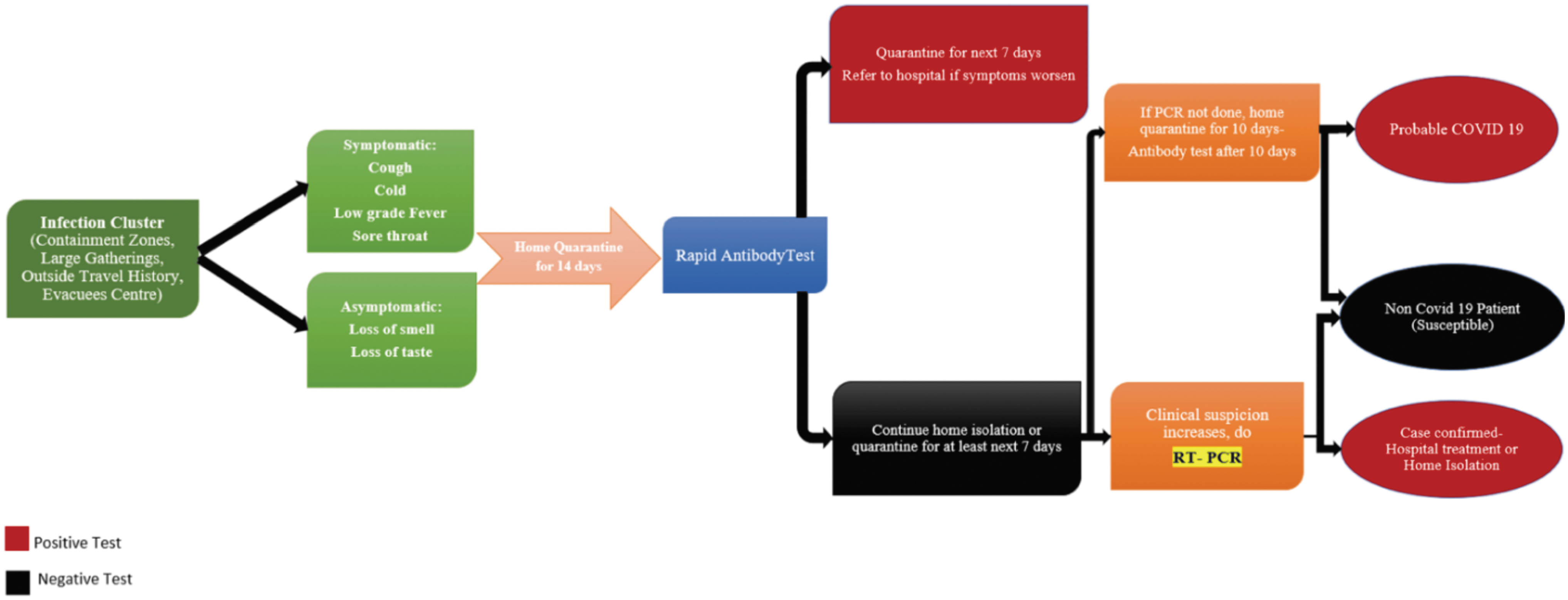
Diagnosis coding for COVID-19. COVID-19, coronavirus disease 2019. Color images are available online.
Why serological test?
During an infectious disease outbreak, two types of testing are generally used: molecular-level and serological. Molecular testing such as real-time polymerase chain reaction (PCR) serves as the gold standard for COVID-19 diagnosis and is based on the presence of replicating virus within the limit of detection of PCR. These tests can detect a pathogen while it is circulating in a body. It may also detect fragments of the pathogen even if it isn't fully cleared from the body and therefore is unable to replicate or cause disease. This is a sensitive technique; however, its accuracy can be compromised if the collection of the sample is not optimal or the patient has low viral load due to an early stage of disease or viral suppression by host immunity (28).
The overall throughput of nucleic acid tests (NATs) is limited due to their nature of needing a high workload, the demand for skilled operators for sample collection, and testing in addition to the requirement of costly instruments and specialized operating places. A missed diagnosis can hinder an opportunity of receiving early preventive care before the disease progresses to an acute respiratory syndrome which has an over 60% mortality rate (101).
Serological tests or “antibody tests,” on the other hand, can detect traces of the body's immune response to an infection, which can provide information on both current and prior infection. Thus, they are capable of detecting past infections even after the immune system has successfully cleared the pathogen from the system (16) (Fig. 1). On the epidemiology of SARS and other such infection outbreaks, serological methods have already proven their importance (18). Especially in the case of individuals with very low viral load and below the detection limit of RT-PCR assays, serological tests are crucial (83). In the early stages of the COVID-19 outbreak, the immune response toward SARS-CoV-2 was manifested and observed in patients having pneumonia (94).
Incidentally, the clinical and laboratory findings of COVID-19 are not distinguishable from pneumonia caused by common respiratory tract pathogens such as influenza virus, Streptococcus pneumoniae, and Mycoplasma pneumoniae (1). Like missed diagnosis, misdiagnosis of COVID-19 would be disastrous. Misdiagnosis in less-infective coronavirus diseases like HCoV-OC43, HCoV-NL63, HCoV-229E, and HCoV-HKU1 infection as SARS-CoV-2 can send thousands of people to the already overloaded hospitals and increase the risk of infection by SARS-CoV-2 (101). Thus, timely diagnosis of SARS-CoV-2 is essential in providing appropriate medical support and limiting its spread (72).
Considering the central role played by the B cells in humoral immune response, evaluating seroconversion of antibody response to an infection helps in the clinical diagnosis of a disease (14). Tracing host response to an infection by serological means is an indirect measure of infection (81). Even a reliable test of this kind can't indicate whether someone is immune to reinfection (48). Patients with mild to moderate illness, after the first 2 weeks of illness onset, can take advantage of antibody tests. These tests prove useful in understanding the extent of the spread of COVID-19 in a given community (72).
To understand the disease transmission within a society, identifying the subacutely infected individuals and the individuals recovered from COVID-19 is necessary. This can be successfully carried out using antibody tests (4). Although areas with a high prevalence of COVID-19 can rely on antibody tests, areas with lower prevalence require a high accuracy antibody test with consistent performance (50). Like a NAT, sometime negative antibody test report in the early stage of illness could not rule out the possibility of infection (44).
Detection of COVID-19 with the aid of serological kits
Commercial immunoassays which include LFIA—lateral flow immunoassay, CLIA—chemiluminescent immunoassay, and ELISA—enzyme-linked immunosorbent assay use IgM and IgG antibodies as biomarkers for the detection of COVID-19 (88). Countries all around the globe are turning to serological tests for the detection of SARS-CoV-2 associated IgM and IgG antibodies, especially at the population level or in specific groups such as health workers and suspected cases. WHO supports this approach as serological tests give insights into the extent of infection in a community at large.
According to virologists, a high-quality and competent test is expected to achieve ≥99% sensitivity and specificity (48). The number of people with a given disease in proportion to the number which tests positive for the said disease is termed as clinical sensitivity or true positive rate, and the proportion of people without the said disease who indeed test negative refers to clinical specificity or true negative rate. These properties are innate to a screening test itself and it is exclusive of the prevalence of disease in a given population (4). Notably, many serological kits are approved with the restriction that they may only be used as companion tests for the NAT and not for general screening of SARS-CoV-2 due to unreliable sensitivity and specificity (48).
This drawback of serological tests could be contributed to the type, quality, and quantity of the antigens used for detecting specific biomarkers. These antigens include recombinant N protein from SARS-CoV-2 (highly conserved among all 7 members of the coronavirus family that can lead to poor specificity in the general population), CHO-expressed S1 protein from SARS-CoV (studies show that S1 of SARS-CoV has very different antigenicity from its counterpart in SARS-CoV-2), and RBD of SARS-CoV-2 (200 amino acid long with one glycosylation) (101). However, it is important to note that antibody tests can't detect the presence of NAbs (48).
Numerous SARS-CoV-2 immunoassays are rapidly being developed due to the urgency and demand with limited validation on clinical samples. For accurate use in the diagnosis of an infection, a thorough validation of any serological test is necessary. This facilitates appropriate patient care, as well as tracking of COVID-19 infected individuals, including asymptomatic carriers who need to be isolated to limit the virus spread (40).
Table 1 accounts for the sensitivity, specificity, and other characteristics of some of the US FDA (United States Food and Drug Administration) and CE-IVD (CE marking for Europe's In Vitro Diagnostic) approved serological kits, which are verified in clinical samples.
Summary of Serological Kits Validated in Clinical Samples
CLIA, chemiluminescent immunoassay; CMIA, chemiluminescent microparticle immunoassay; COVID-19, coronavirus disease 2019; ELISA, enzyme-linked immunosorbent assay; HAMA, human anti-murine antibody; HRP, horseradish peroxidase; IFU, Instruction for Use; LFIA, lateral flow immunoassay; MERS-CoV, Middle East respiratory syndrome corona virus; MNT, microneutralization; PCR, polymerase chain reaction; POC, point-of-care; RBD, receptor-binding domain; RF, rheumatoid factor; S protein, Spike protein; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Methods
A literature search was carried out for publications that focused on the detection of SARS-CoV-2 in human samples by serological assays using FDA and CE-approved kits. PubMed, SCOPUS, Google Scholar, WHO, and Centers for Disease Control and Prevention websites were searched without language restrictions from inception through to July 2020. Additional articles were identified from the bibliographies of included studies. For the main objective of this review, all original publications reporting on the sensitivities and specificities of antibodies through FDA and CE-approved assays against SARS-CoV-2 were included in the analysis.
Results and Discussion
For a vast and densely populated country like India, quick and user-friendly diagnostic techniques are important for screening the population and curbing the spread of pandemics on a mass scale. Currently, until everyone is vaccinated, the only available strategy to slow the pandemic is through identifying and isolating contagious persons through early and massive deployment of SARS-CoV-2 testing. This may reveal the prevalence and pattern of infection in a given population and could help the public health experts in understanding the trajectory of the infection. Essentially, these data can help countries in preparing the alterations in public health mediations from time to time and may affect the entire outcome of the scenario. For a timely diagnosis and isolation of an infected individual from the susceptible population, there is a need for swift and user-friendly diagnostic techniques.
Since serological testing is quick and easy to perform, it would give public health experts an idea of the prevalence of the infection in the given population and would help in modulating public health policies and practices accordingly. Retrospectively, this can contribute toward the evaluation of epidemiological determinants.
Serological testing is relevant in the following settings: (i) patients who necessitate attention after 7 days of the onset of symptoms; (ii) evaluating potential immunity and risk of infection; (iii) contact tracing; and (iv) epidemiological studies to understand the extent of COVID-19 spread (40). During this study, a search on CE or FDA approved clinically evaluated kits divulged a total of 40 kits; 8 ELISA kits, 10 CLIA kits, and 22 LFIA kits (Table 1), which are included in this review article. Multiple research articles based on FDA and CE-approved kits were referred for this study. However, the data from those having a larger sample size were considered here.
Enzyme-linked immunosorbent assay
The comparative study of ELISA kits (Table 1) revealed that among the kits targeting the RBD domain of SARS-CoV-2 Spike protein, the one that detects total antibodies has greater sensitivity. Although the Euroimmun IgA kit exhibited the highest clinical sensitivity (93.3%) among all the ELISA kits considered in this study, its sensitivity was comparable with the Wantai total antibody (93.1%). Euroimmun IgG displayed low sensitivity in the initial days after symptom onset but showed 100% sensitivity after 15 days of commencement of symptoms. It is important to note that Euroimmun IgA and IgG ELISA are both prone to cross-reactivity with negative sera (40). However, the Euroimmun SARS-CoV-2 IgG ELISA Kit has been used to determine seroprevalence in Geneva (a–d in Table 2).
Overall Diagnostic Performance of the Enzyme-Linked Immunosorbent Assay Kits for IgA, IgM Alone, IgG Alone, and IgM and IgG
N protein, Nucleocapsid protein.
Among the kits that target the N protein of SARS-CoV-2, the ELISA Kit by Lizhu exhibited higher sensitivity in the initial days of symptom onset. Its IgG and combined IgM/IgG achieved 100% sensitivity after 31 days of symptom onset. Even though Epitope's IgG kit achieved 100% sensitivity after 15 days of symptom onset, they had lesser sensitivity in the initial stages. It was observed that combining IgM and IgG improved the detection sensitivity of the Hotgen ELISA Kit (Figs. 2–6).
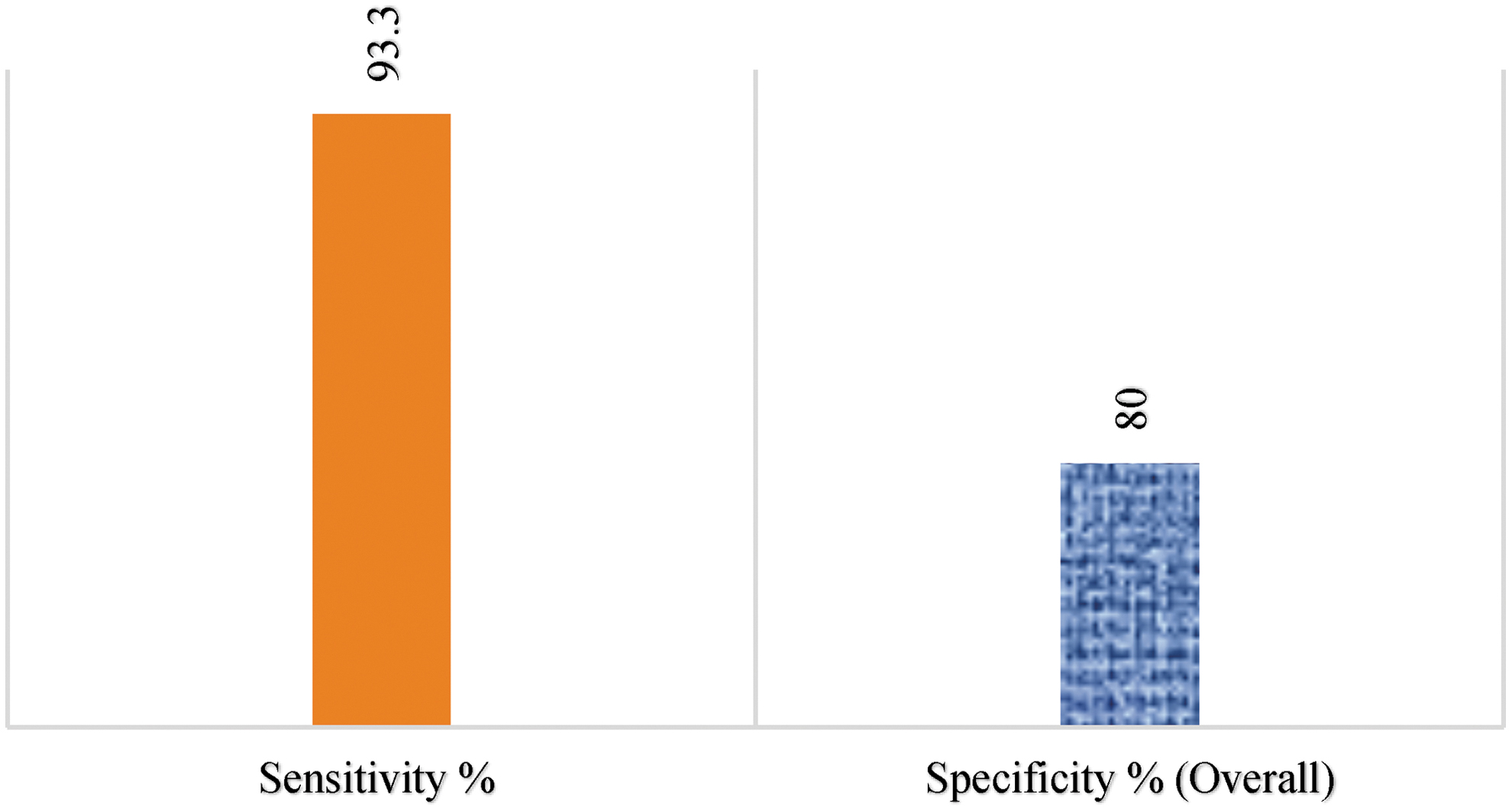
Performance of Euroimmun Kit of ELISA for IgA detection. ELISA, enzyme-linked immunosorbent assay. Color images are available online.
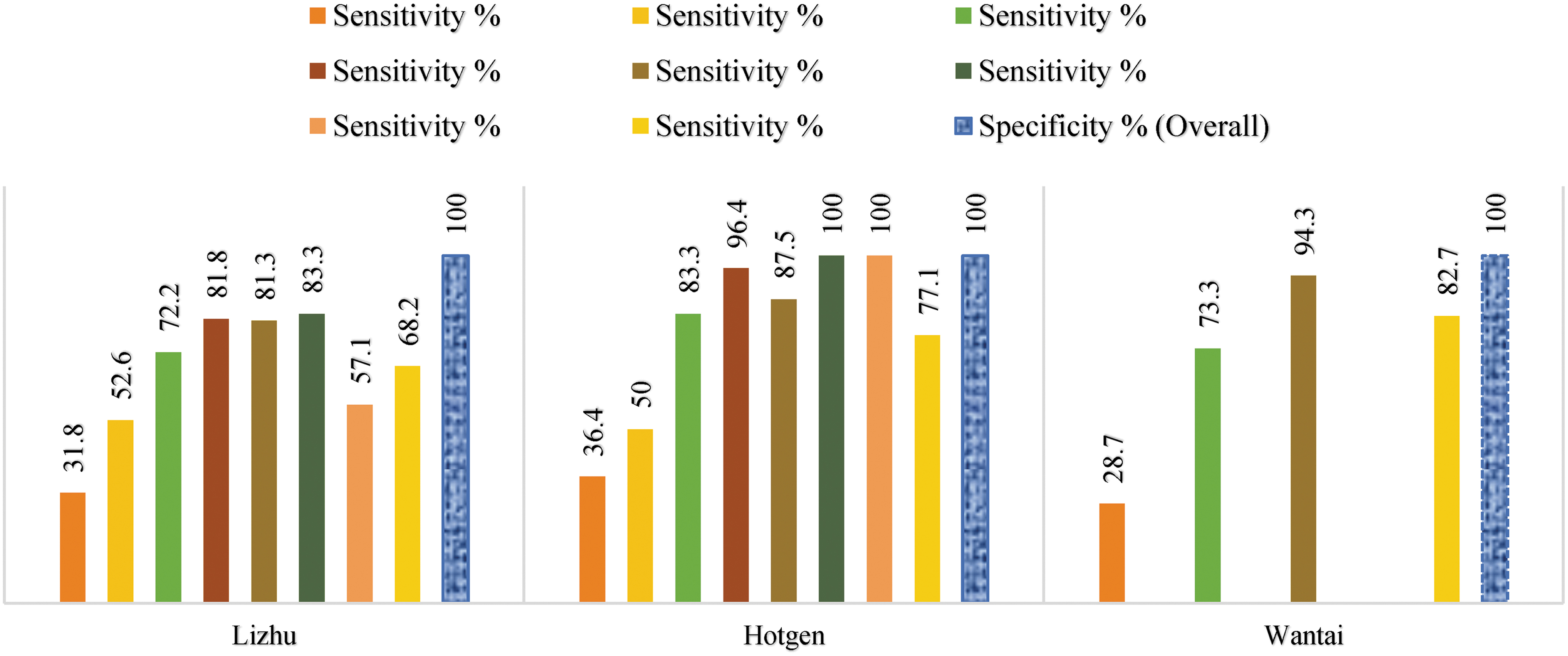
Comparative performances of three kits of ELISA for IgM detection from 0 to >35 days. Color images are available online.
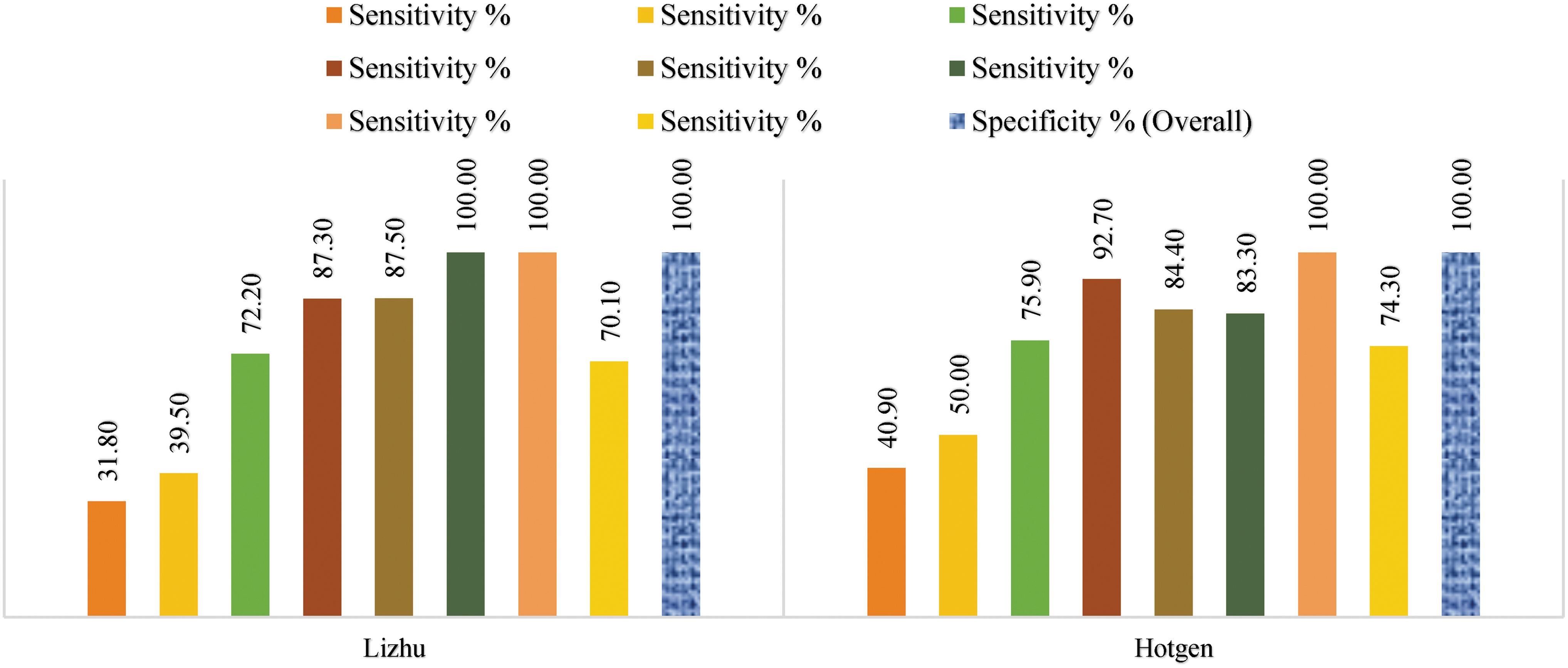
Comparative performances of two kits of ELISA for IgG detection from 0 to >35 days. Color images are available online.
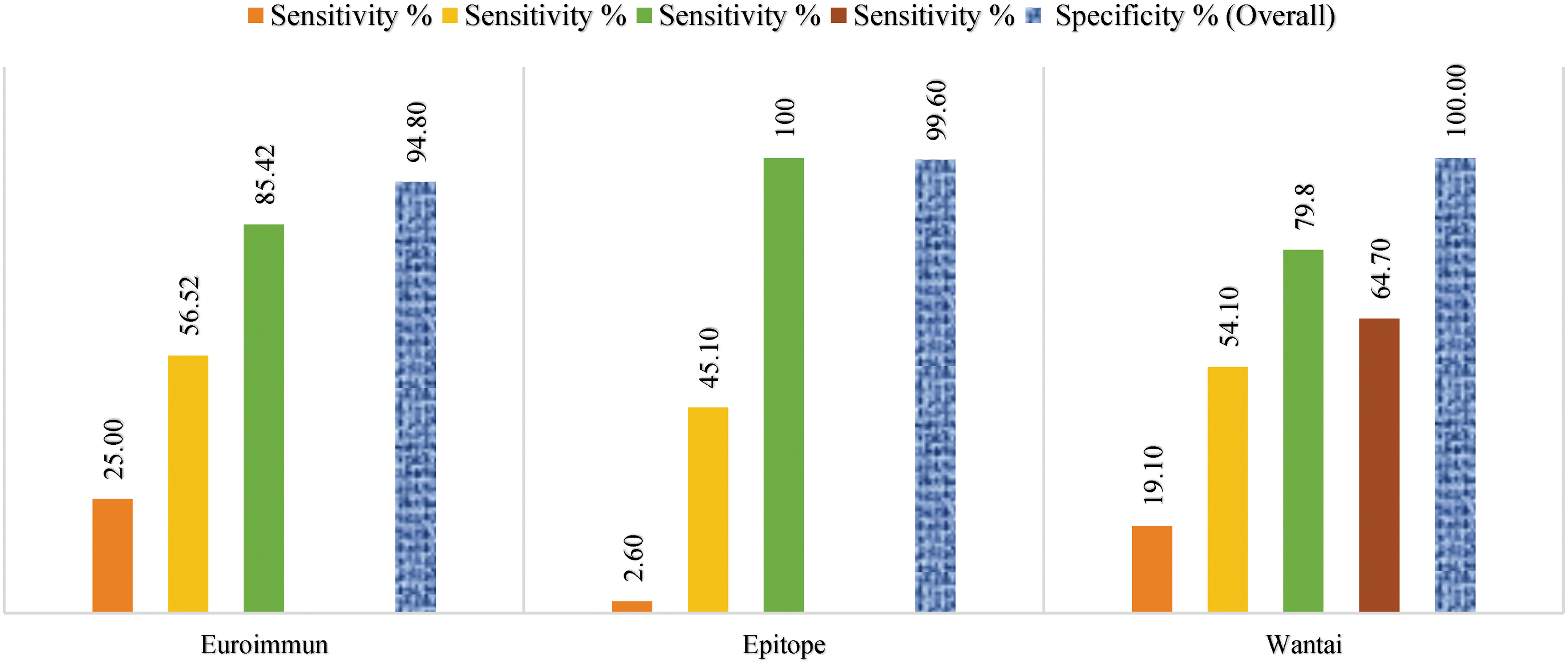
Comparative performances of three kits of ELISA for IgG detection from 0 to ≥15 days. Color images are available online.
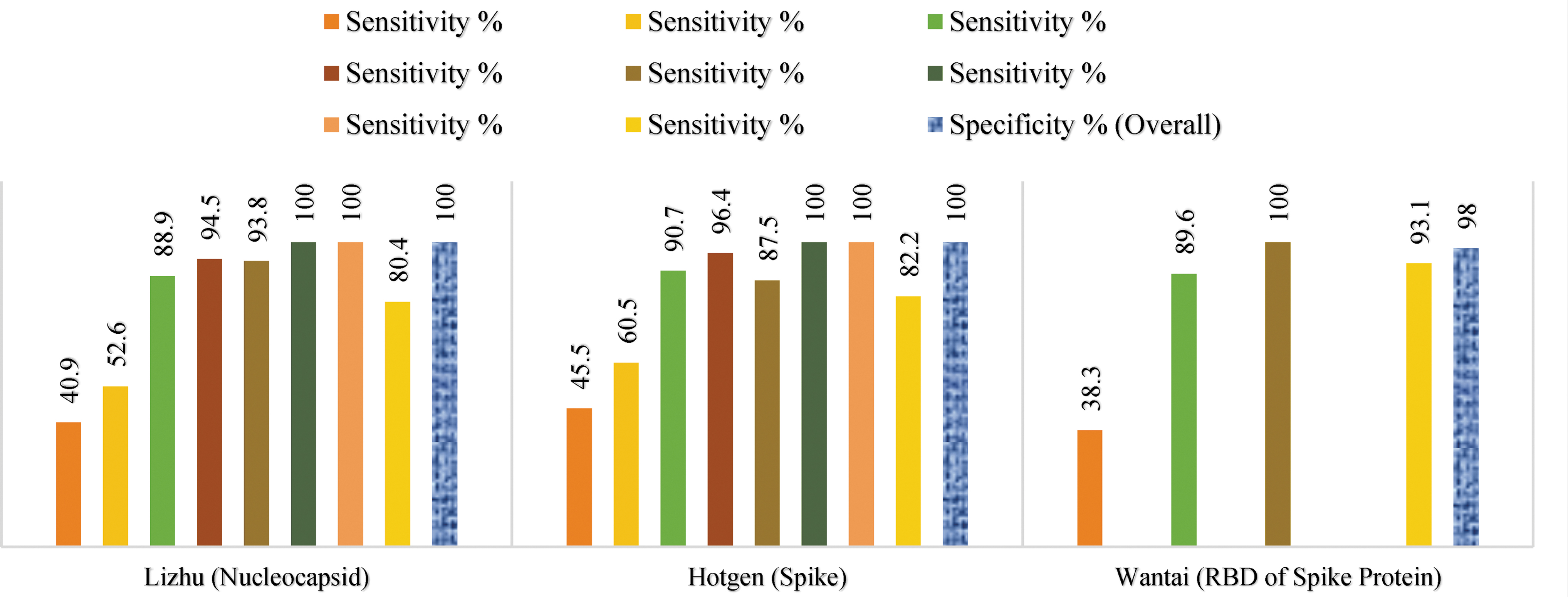
Comparative performances of three kits of ELISA for IgM and IgG detection from 0 to >35 days. Color images are available online.
The reason for the observed increased sensitivity while detecting total antibody compared with the detection of single isotype antibodies could be due to the kinetics of the antibody development in response to SARS-CoV-2, which varies from individual to individual. As total antibodies detect any type of antibodies, including IgM, IgG, and IgA in principle, this could be the other reason behind increased sensitivity.
Therefore, the inclusion of all crucial antibodies involved in the immune response gives this test an upper hand compared to individual antibody tests. Incorporating IgM, as well as IgG, drastically boosted the diagnostic sensitivity of the ELISA test. The variations between assay sensitivities may also partially depend on which SARS-CoV-2 antigen is targeted and which ELISA format is chosen (40). Double antigen ELISA was used for the total antibody assay, which requires two Fab arms of the same antibody to bind with the coated antigen and the enzyme-conjugated detecting antigen. This guarantees the specificity of the test. By increasing the concentration of antigens used for coating and detecting, sensitivity can be improved.
If sensitivity is the top priority, then the total antibody test outperforms individual IgM and IgG tests and has often been used for screening of blood donations for various infections caused by virus such as HIV and hepatitis virus (44). On comparing total antibody (RBD of S1), IgM, and IgG ELISA results of Wantai tests, it was observed that total antibody ELISA test has superior sensitivity and specificity compared to individual Wantai IgM, IgG ELISA, and Euroimmun IgG ELISA tests (S1 domain of spike protein of SARS-CoV-2).
In addition to lower sensitivities, Euroimmun IgA and IgG ELISA are prone to cross-reaction with negative sera. Euroimmun ELISA and Hotgen total antibody test target S1 subunit of spike protein; however, RBD domain of S1 subunit is targeted by Wantai total antibody. RBD constitutes just 33% of the S1 subunit. Thus, cross-reacting epitopes outside this domain are absent. The high variability of the RBD domain of SARS-CoV-2 compared to other coronaviruses reduces the likelihood of any cross-reaction.
The ELISA format Ag-Ab-Ag(peroxidase) is used by Wantai total antibody, whereas Euroimmun uses Ag-Ab-Ab(peroxidase) format. The significance of these formats being that the former is determined by the specificity of a single antibody and the latter has a secondary antibody which may introduce additional specificity (40). The seroconversion of Wantai total antibody (double antigen sandwich) was quicker than IgM (capture assay) and IgG (indirect ELISA) (100). ELISA targeting IgG antibodies against nucleocapsid protein delivered better sensitivity and specificity than IgA against the S1 domain of spike protein (Table 1).
Quantitative PCR (qPCR) has a higher detection rate than IgM ELISA before 5.5 days of postsymptom onset, while the detection efficiency of IgM ELISA was higher compared with the PCR method after 5.5 days of symptom onset. In a single PCR test, the positive detection rate was only 51.9% but drastically increased to 98.6% when IgM ELISA was applied to PCR-negative patients. This indicates that supplementary IgM tests along with qPCR can provide better sensitivity (28). ELISA is a long-established method for antibody detection. However, its drawbacks include longer turnaround time, need for laboratory equipment, and higher labor costs required for a result (86).
Chemiluminescent immunoassay
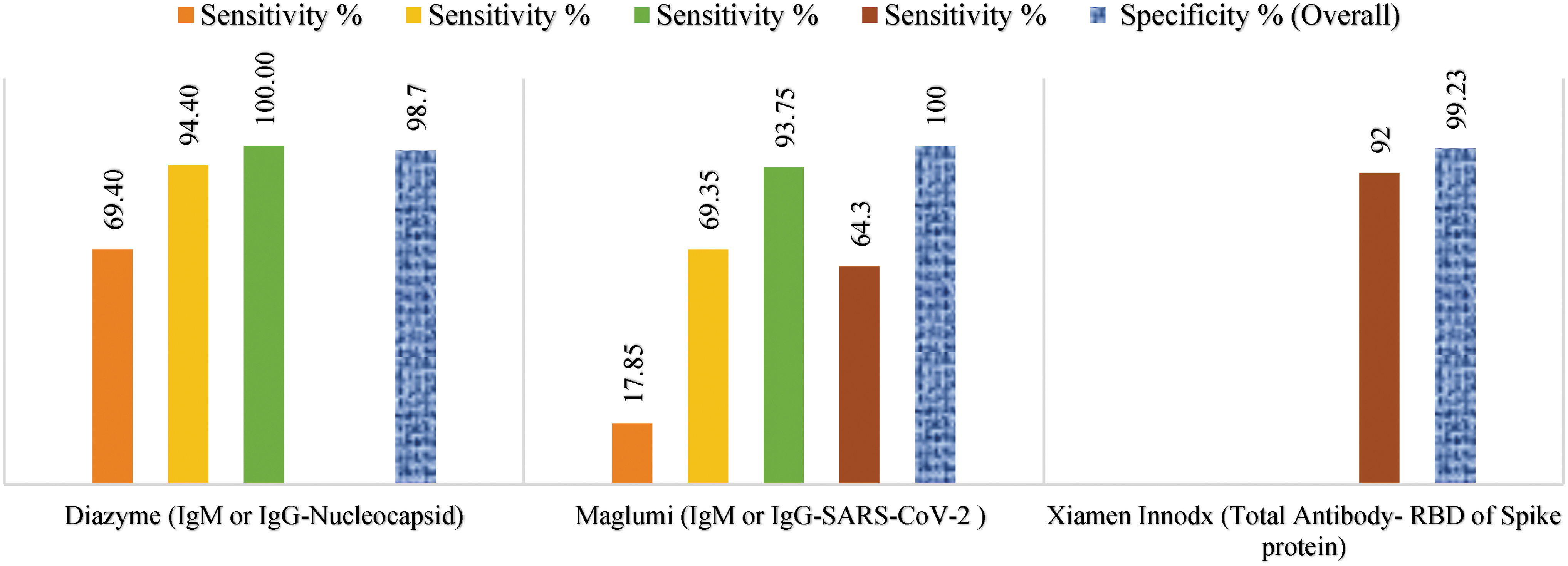
Among the tested 9 CLIA kits (Table 1), the highest sensitivity was observed in IgG/IgM kits by Diazyme laboratories and IgM alone and IgG alone kit by Shenzhen YHLO, which targets both N and S protein of SARS-CoV-2. For the kit by Diazyme laboratories, combining antibody results drastically elevated detecting sensitivity and it reached 100% after 15 days of symptom onset. It also displayed high sensitivity compared to other CLIA Kits in the initial days of symptom onset. The assay marketed by Xiamen, which targets RBD of S protein with an overall sensitivity of 92.0%, comes a close second. Among the CLIA Kits considered here, the one from Abbott Laboratories has been used extensively for the evaluation of seroprevalence in communities in different countries. DiaSorin and Shenzhen CLIA Kits were also used for the same (a–c in Table 3).
Overall Diagnostic Performance of the Chemiluminescent Immunoassay Kits for IgM Alone, IgG Alone, IgM or IgG, and IgM and IgG
Within the CLIA Kits compared here, the Ortho-clinical CLIA Kit exhibited the least sensitivity of 6.1% in the initial days of symptom onset, although it achieved 84.8% sensitivity after 7 days of symptom onset.
While comparing tests that targeted S protein, it was observed that the CLIA Kits that target RBD of S protein have greater diagnostic parameter values compared to those targeting full-length S protein. Although the S1 subunit of SARS-CoV S protein is a peripheral fragment of the viral envelope and is significantly exposed to the immune system, the S2 subunit is a membrane-spanning fragment buried within viral envelope protein in the native state, which results in its lower immunogenicity. Thus, the S1 subunit of S protein not only has a receptor-binding motif (RBM) but also confers antigenicity to induce a strong immune response (29) (Figs. 7–9).
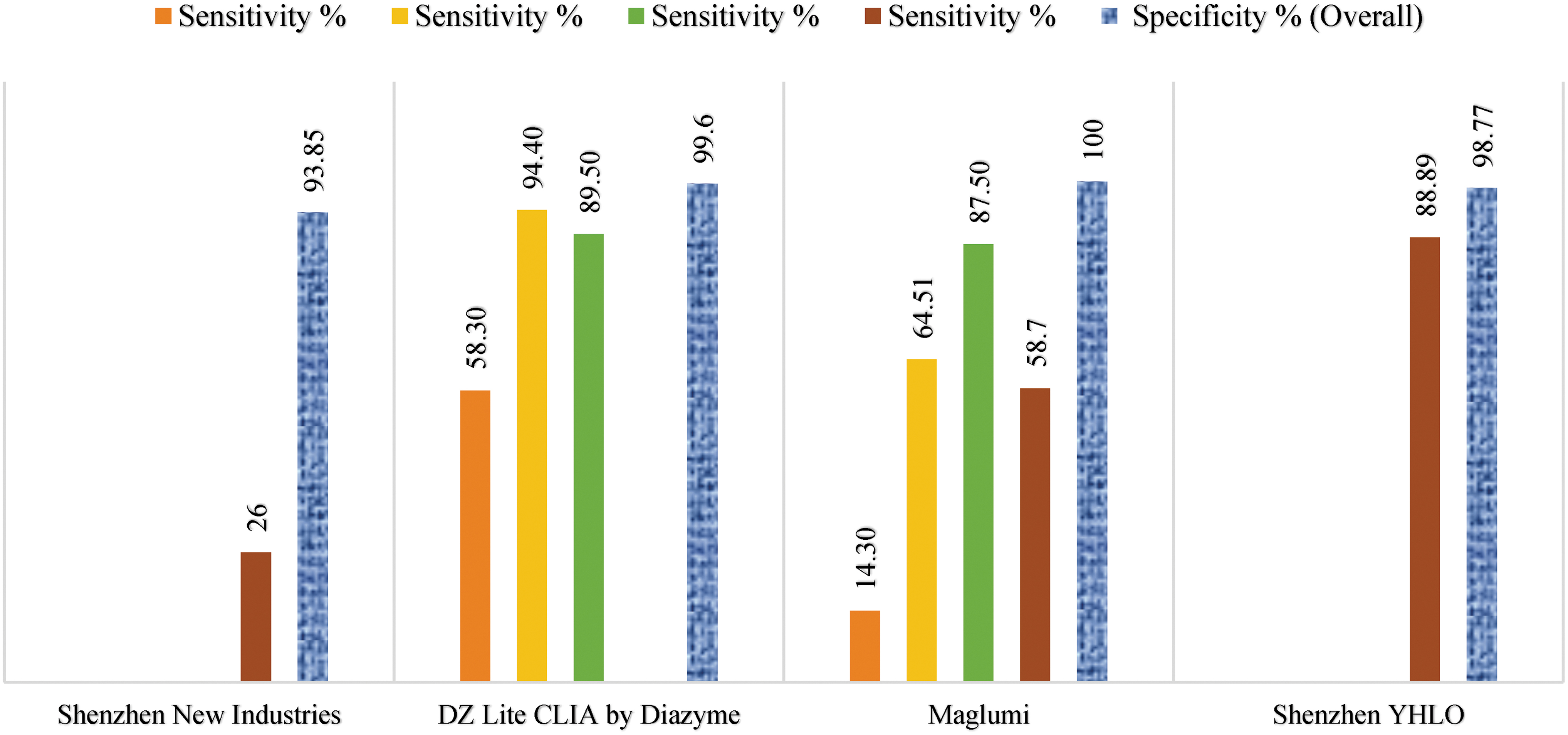
Comparative performances of four kits of CLIA for IgM detection from 0 to ≥15 days. CLIA, chemiluminescent immunoassay. Color images are available online.
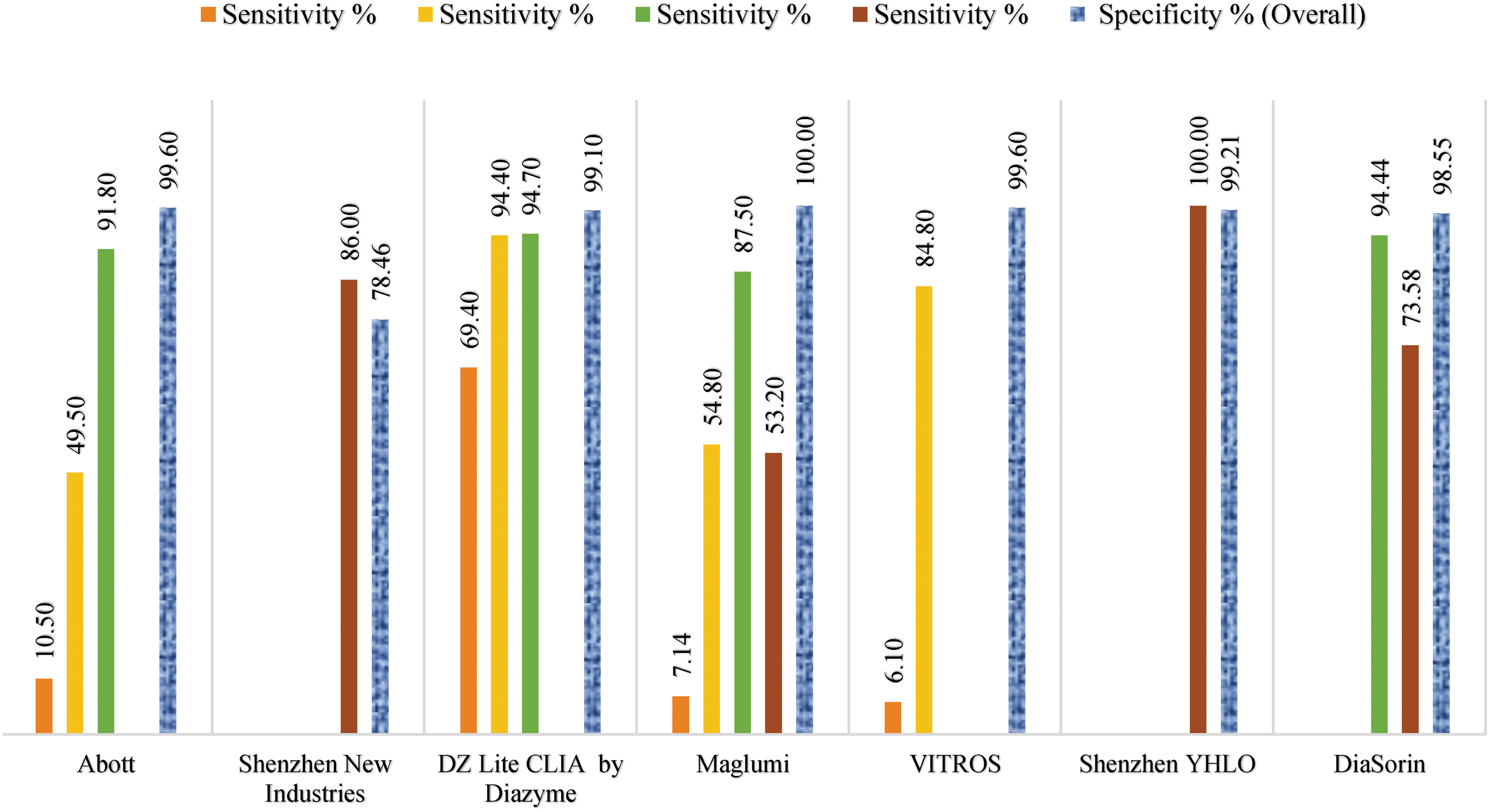
Comparative performances of seven kits of CLIA for IgG detection from 0 to ≥15 days. Color images are available online.
Comparative performances of three kits of CLIA for IgM or IgG detection with the targeted components of SARS-CoV-2 virus from 0 to ≥15 days. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2. Color images are available online.
The diagnostic accuracy of CLIA based on RBD of S protein outperformed those based on nucleocapsid protein (NP). On adding IgA to a conventional serological test that had IgM and IgG, the SARS-CoV-2 diagnostic sensitivity at an early stage of infection improved significantly. The kinetics of IgA, as well as its antiviral immunity, is unexplored. On the evaluation of individual IgA, IgM, and IgG CLIA Kits, the IgA Kit gave more false positives than IgG but less than IgM. CLIA Kits of RBD base were found to be highly specific to SARS-CoV-2. The highest sensitivity of IgA was found during 4–25 days after illness onset. Although the RBD-specific IgA was observed to have a peak median concentration of 8.8 μg/mL during 16–20 days after illness onset, its concentration declined and remained at 3.6 μg/mL until 31–41 days.
In the early stage of the disease, the median concentration of RBD-specific IgG was less and reached its peak of 16.5 μg/mL after day 21 through day 25 after illness onset and stayed at a comparatively higher concentration of 11.4 μg/mL until 31–41 days. This suggests that at later stages of infection, IgG is much more significant in diagnostics. However, IgM concentration reached its peak of 7.25 μg/mL at early stages but was lower compared with IgA or IgG.
These observations suggest that out of the three antibody isotypes, IgM has the lowest diagnostic power in detecting SARS-CoV-2. Serological testing power can be improved by combining IgA into a diagnostic assay that contains IgG and IgM. A direct correlation was found between IgA/IgG concentration and the severity of COVID-19. The reason for SARS-CoV-2 specific IgA detection being highly sensitive in the early stage of infection is because of the low basal level of IgA in blood serum (45).
Lateral flow immunoassay
For the rapid detection of SARS-CoV-2 antibodies, many point-of-care (POC) immunoassays have been developed, including the lateral flow assay. Theoretically, rapid antigen lateral flow assay is advantageous by giving a faster result, its user-friendliness, and its low-cost detection. However, its sensitivity in early infection is poor. Antigen detection may give false-negative results due to low viral load or sampling variability.
Lateral flow assays of IgM and IgG antibodies have played an important role in the COVID-19 outbreak. However, the response of IgM is blatantly nonspecific, and given the weeks required to develop specific IgG responses, serology detection involving these two antibodies is not likely to play an active role in case management. Nonetheless, these would be helpful in diagnosing/confirming late-stage COVID-19 cases and in determining the immunity of health care workers as the outbreak progresses (81) (a–d in Table 4).
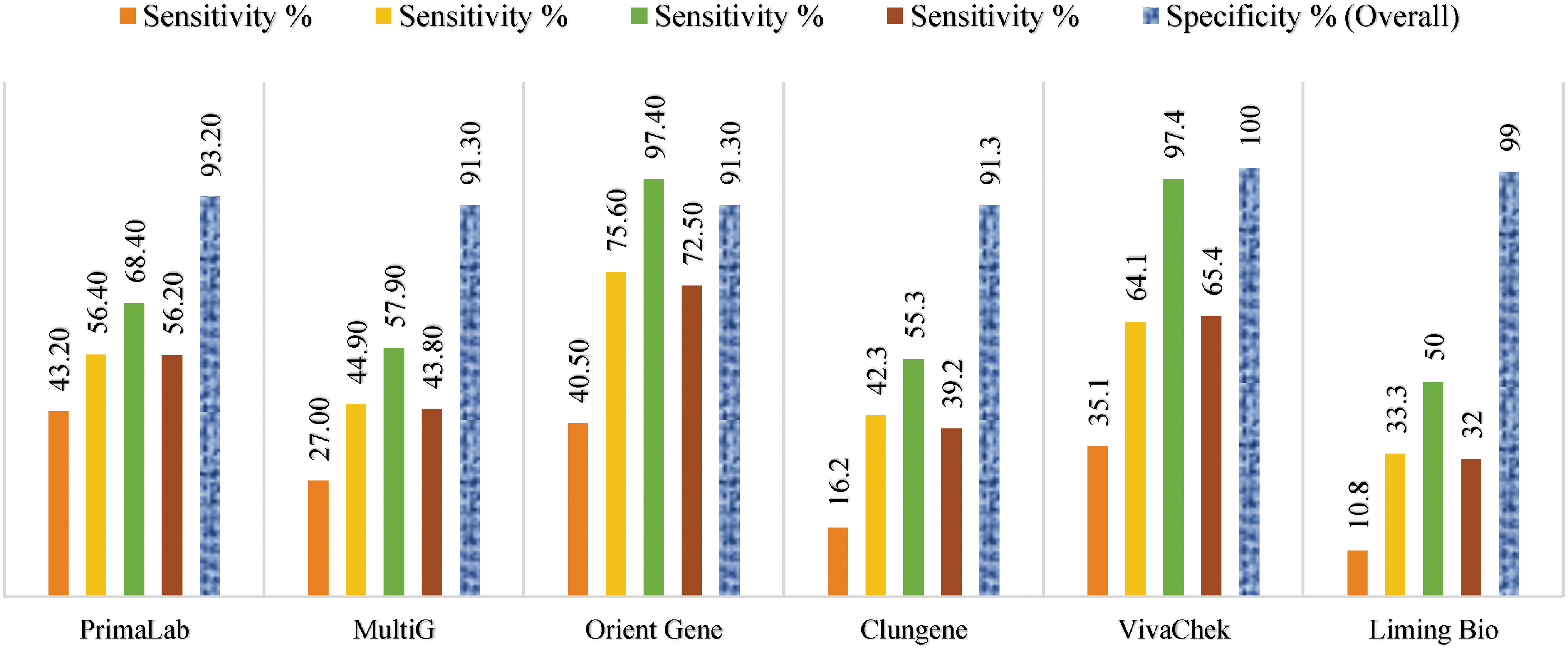
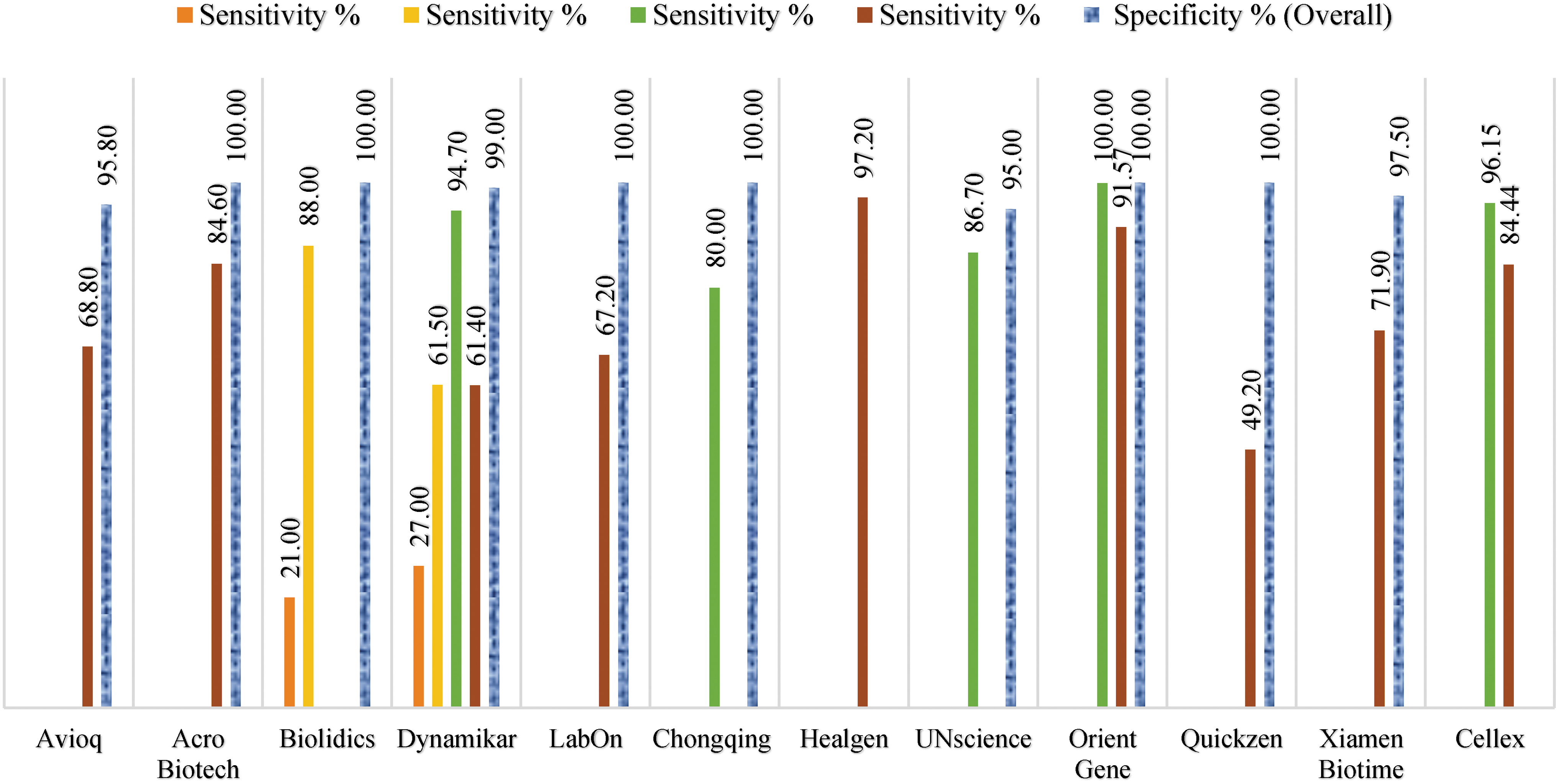
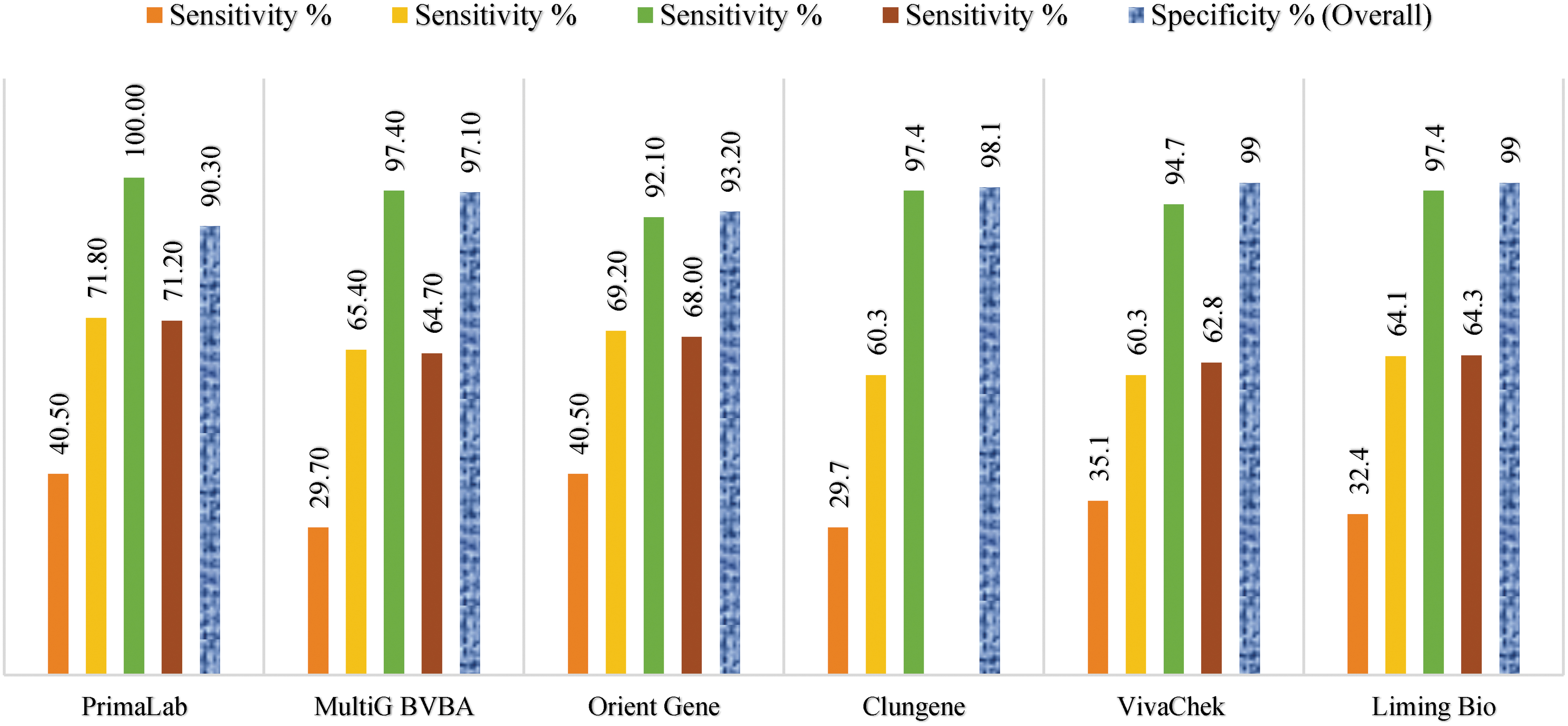
Overall Diagnostic Performance of the Lateral Flow Immunoassay Kits for IgM Alone, IgG Alone, IgM or IgG, and IgM and IgG
Average sensitivity of <10 days (76.32%) and 10–15 days (88.89%).
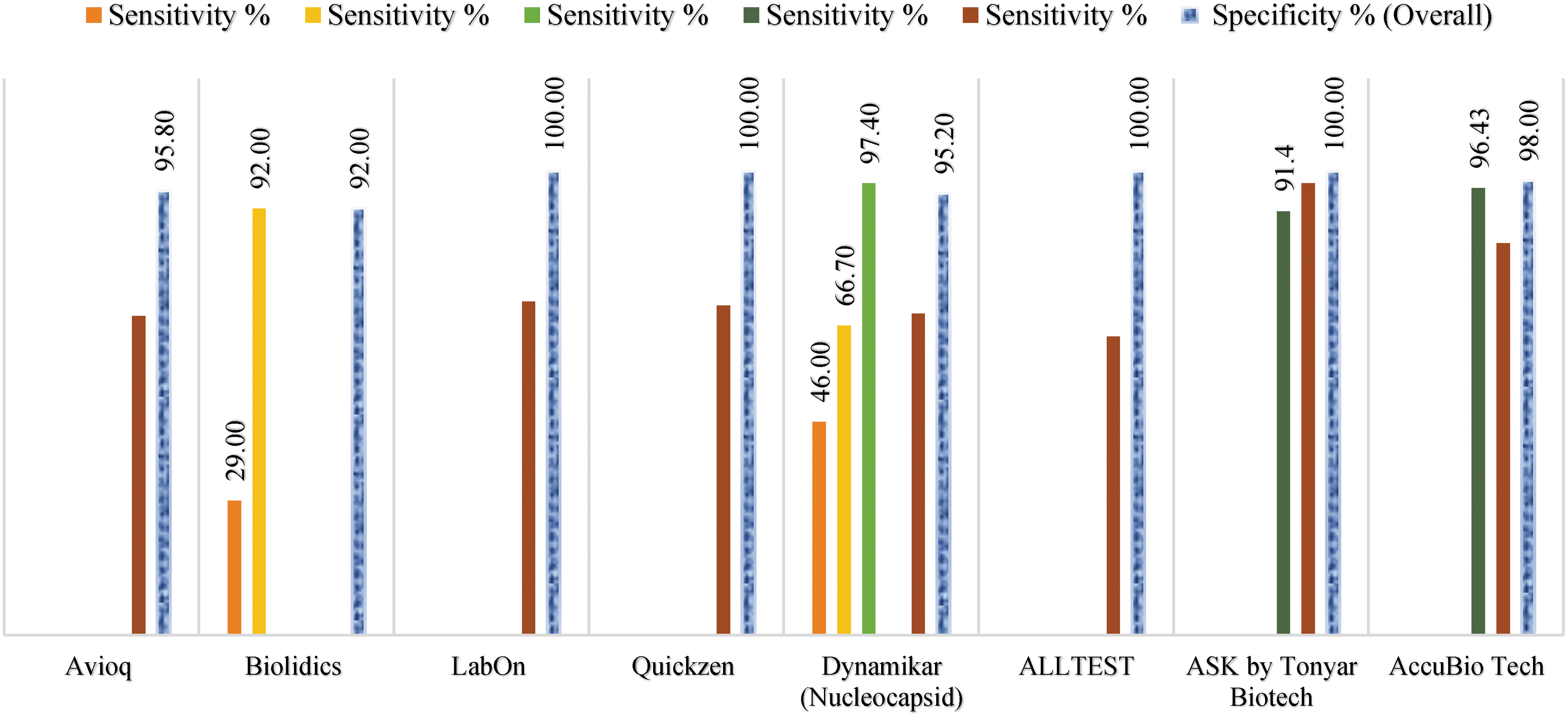
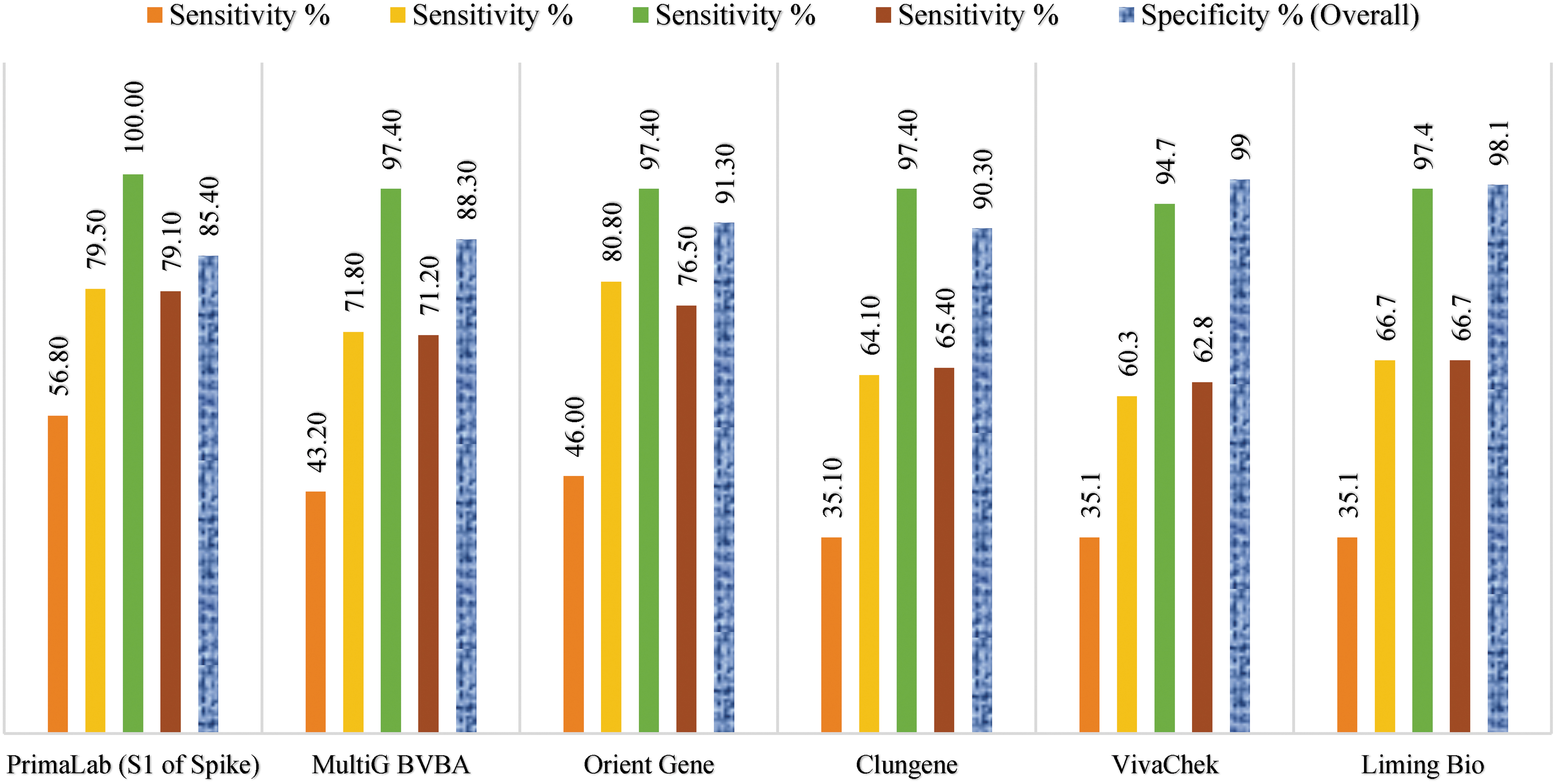
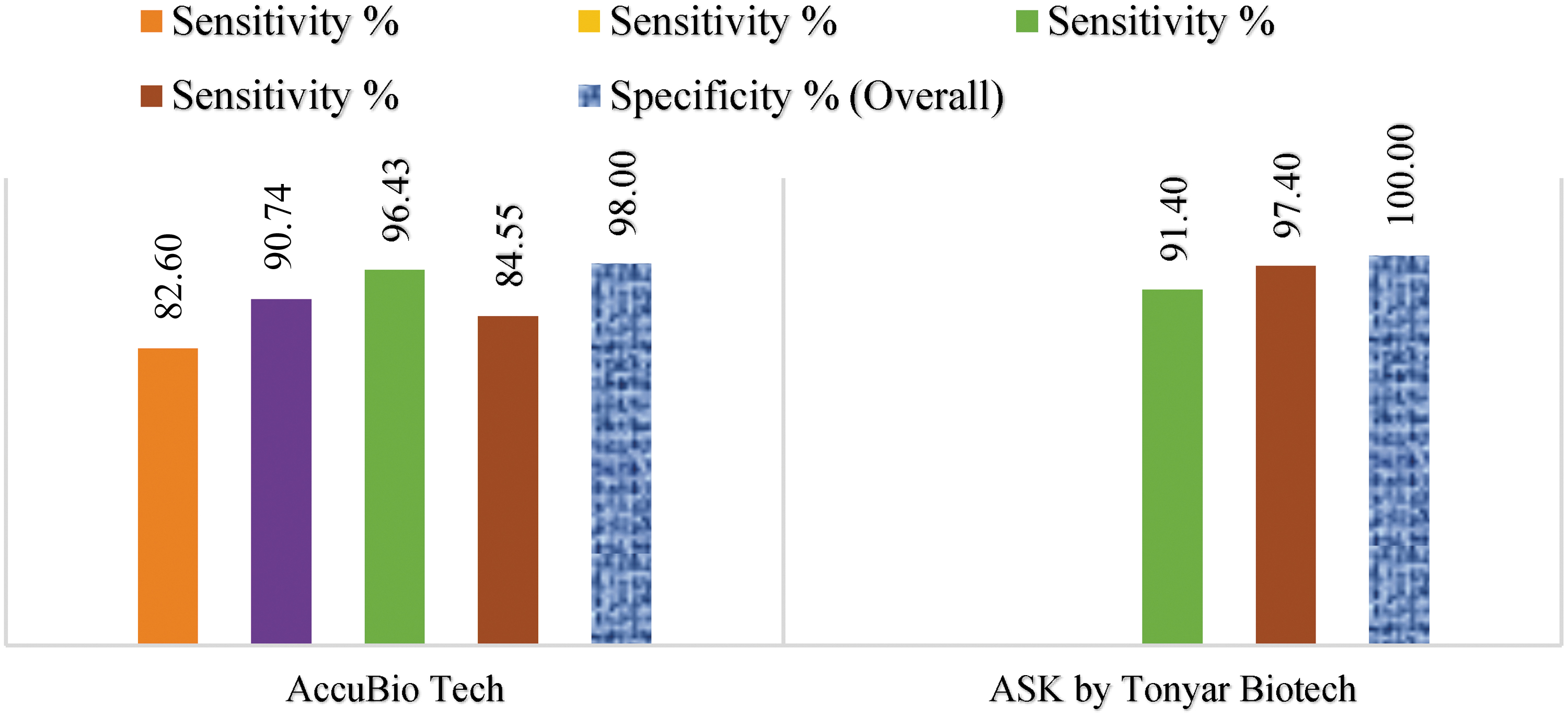
Out of the 19 LFIA Kits considered here, 2 kits exhibited a sensitivity of or above 80%, 8 kits showed more than 90% sensitivity, and a kit from PrimaLab which detects S1 of S protein showed 100% sensitivity for IgG detection. Healgen IgM/IgG Kit, which also targets the S1 domain of S protein, showed the highest overall sensitivity for IgM (87.9%) and IgG (97.2%) detection. VivaDiag™ and Dynamiker Kit, which detects antibodies against RBD of S protein and N protein, respectively, exhibited excellent sensitivity when tested either alone for IgM (97.4%), IgG (94.7%), or combined (94.70%) antibodies after 15 days postsymptoms. These results were almost nearer to Cellex IgM/IgG Kit detecting IgM and IgG antibodies against S and N protein (96.15%). The aforementioned three kits showed comparable sensitivity between IgG and IgM.
Thus, the sensitivity was unchanged in any combination mentioned above. One of the kits, ASK by TONYAR, which detects antibodies against S protein showed 100% sensitivity for IgG and IgM antibodies even after the third week of symptom onset. Independent of which proteins the kit targeted (N or S), a combination of IgG and IgM reduced diagnostic sensitivity compared with the individual antibody tests. But greater sensitivity was observed when either IgM or IgG positive results were considered. This stark difference is seen as the LFIA results of IgM vary drastically (20). It was observed that the detection of IgM is more susceptible to false-positive results by both ELISA and LFIA (7).
Overall results of all the kits reviewed here show that the test sensitivity increases considerably after 2 weeks of symptom onset giving better results with IgG detection than IgM antibodies. Among all the kits, only the Accu-Tell® Kit exhibited excellent sensitivity (IgM or IgG—76.2%) during the first 10 days of symptom onset. Clungene, MultiG, and StrongStep® by Liming Bio IgG/IgM Rapid Test exhibited the least IgM and IgG sensitivity, that is, <60% even after the third week of symptom onset (Figs. 10–18).

Comparative performances of 12 kits of LFIA for IgM detection from 0 to ≥15 days. Average taken (refer a in Table 4). LFIA, lateral flow immunoassay. Color images are available online
Comparative performances of six kits of LFIA for IgM detection from 0 to 25 days. Color images are available online.
Comparative performances of 11 kits of LFIA for IgG detection from 0 to ≥15 days. Color images are available online.
Comparative performances of six kits of LFIA for IgG detection from 0 to 25 days. Color images are available online.
Comparative performances of eight kits of LFIA for IgM or IgG detection from 0 to ≥15 days. Color images are available online.
Comparative performances of six kits of LFIA for IgM or IgG detection from 0 to 25 days. Color images are available online.
Comparative performances of two kits of LFIA for IgM or IgG detection from 0 to >21 days. Color images are available online.
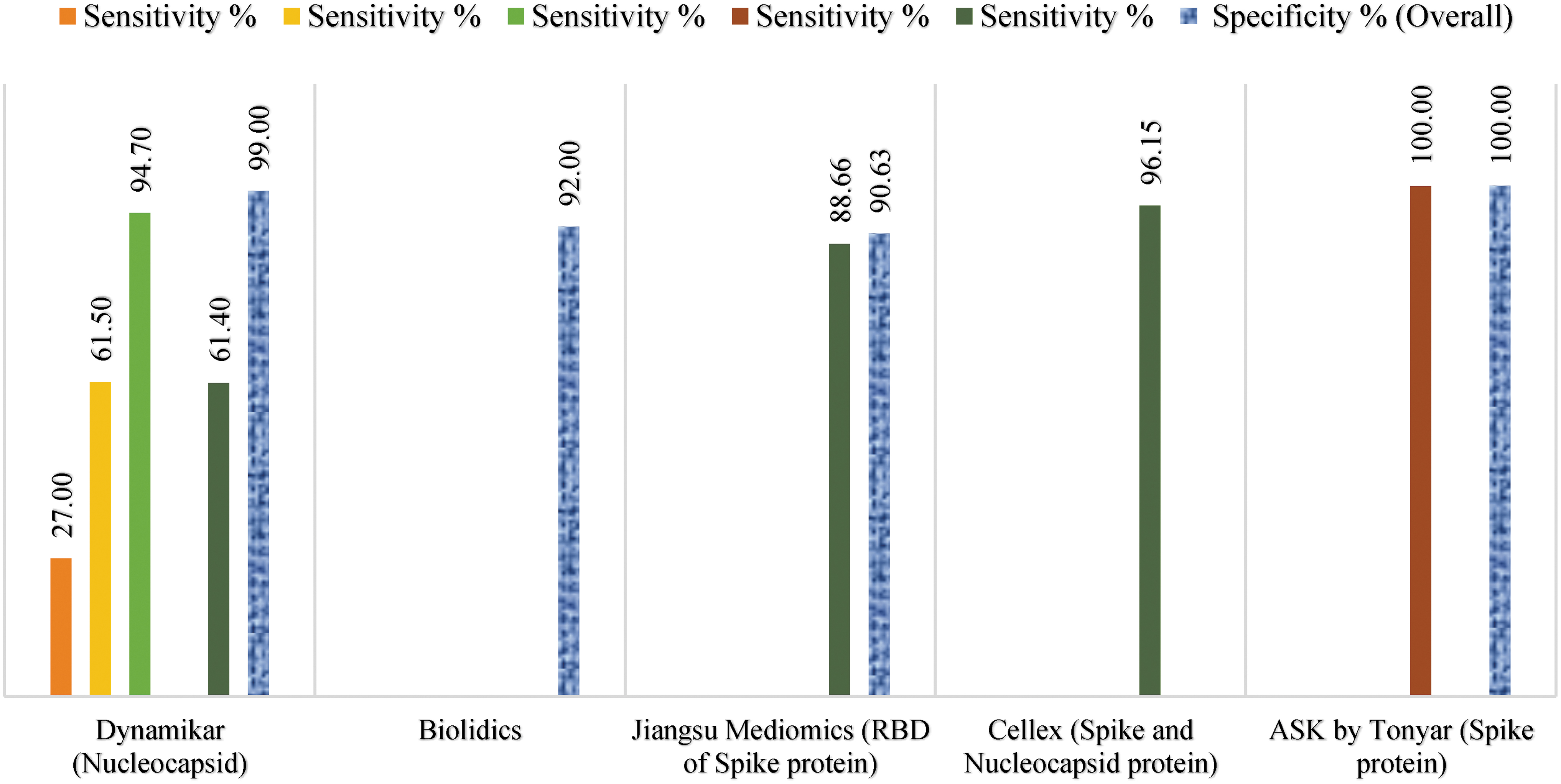
Comparative performances of five kits of LFIA for IgM and IgG detection from 0 to >21 days with targeted components of SARS-CoV-2 virus. Color images are available online.

Comparative performances of seven kits of LFIA for IgM and IgG detection from 0 to 25 days. Average taken for 6–15 days (refer c in Table 4). Color images are available online.
ELISA and POC LFIA tests may overcome some of the challenges posed by the gold-standard PCR (40). However, LFIA based POC test is far from a perfect diagnostic tool. Rheumatoid factors and Human anti-mouse antibodies can interfere in the evaluation, which can give false-positive results for some of the kits. The accuracy of the kits is highly dependent on the storage conditions. Humidity and temperature above 30°C can have a detrimental effect on their diagnostic efficiency.
Conclusion
The importance of serology testing stems from its ability to detect infection or disease in a time effective manner. Evaluating disease prevalence in a population gives insight on how to strengthen the health system. Emerging evidence suggests that transmission of SARS-CoV-2 is through aerosols. Thus, in densely populated regions, serology testing and evaluation plays a crucial role in understanding infection at the community level. As studies suggest, the serological test which evaluates virus-induced antibody has unique advantages in clinical diagnosis, specifically for identifying people who are asymptomatic.
Therefore, there is an urgent need for the development of serological assays with high sensitivity and specificity. Molecular-based RT-PCR testing demands skilled technicians, a relatively invasive collection of samples, and high complexity laboratories. In addition, it is important to note that during the acute phase of infection nucleic acid detection is superior to antibody testing; however, beyond 8 days of illness the sensitivity of serological assays outpaces nucleic acid detection.
Serological evaluations and observations that have been made earlier revealed that abundant antibodies are produced against N protein. Although the antibody titer against N protein is high, it displays strong cross-reactivity. In contrast, antibodies against S protein are comparatively more specific. Therefore, we expect that detecting antibodies against both antigens would result in a reliable performance. Considering these, N protein can be used as a diagnostic marker, and S protein could be the main target for neutralization antibodies.
Like RT-PCR, gold standard for antibody detection and quantification, ELISA requires trained technicians and complex laboratory procedures. LFIA can address some of the above limitations and with great diagnostic efficiency allows excellent tracking methods for asymptomatic carriers. Due to their high demand, there has been a massive flow of newly developed LFIA Kits in the market.
Soon, reports from multiple parts of the world emerged on their inaccuracy compared to the RT-PCR. This large variability of LFIA tests demanded each test to be validated in-house. Antibody screening on a large scale will provide an understanding of the rate of human-to-human transmission, the incidence of infection, and infection prevalence, which remain uncertain in the rapidly evolving global landscape. Thus, independently validated serological tests are crucial to obtain such information. We acknowledge that what we know is just a drop in the ocean but here we have compiled data of clinically validated kits to help the decision-making while procuring antibody kits and to be mindful of their shortcomings.
Footnotes
Authors' Contributions
First author contributed to the conception, design of work, interpretation of data, and critical revision of the article. Second author contributed to the acquisition, analysis, and interpretation of data for the work and drafted the article. Third and fourth authors contributed to the collection of data, interpretation, and literature survey of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for the work.