
Abstract
Abstract
Globally, transgender women (TGW) experience multiple forms of victimization such as violence and discrimination that can place them at risk for poor sexual health. To date, research overlooks the heterogeneity in experiences of victimization among TGW. Furthermore, few studies have examined the association between victimization and sexual risk among TGW in India, despite the high burden of HIV and victimization in this community. Latent profile analysis was performed to identify patterns of victimization in a convenience sample of 299 TGW recruited from nongovernmental organizations across four states in India. Analysis of covariance was performed to examine differences in sexual risk (i.e., alcohol use before sex; inconsistent condom use with a male regular partner, a male causal partner, and a male paying partner; and having multiple sexual partners) between latent profiles. Five distinct profiles of Indian TGW were identified based on the type and severity of victimization: (1) Low victimization, (2) High verbal police victimization, (3) High verbal and physical police victimization, (4) Moderate victimization, and (5) High victimization. While controlling for age, education, income, HIV status, and marital status, results revealed that TGW in the moderate victimization and high victimization profiles had higher sexual risk than TGW in the low victimization and high verbal police victimization profiles. In addition, TGW in high verbal and physical police victimization profile had higher sexual risk than TGW in low victimization profile. These findings underscore the importance of tailoring sexual risk reduction interventions to the specific needs of TGW based on patterns of victimization.
Introduction
I
Despite calls for antiviolence and antidiscrimination by the United Nations (UN 2015), globally, TGW experience high levels of victimization (Bockting et al. 2013; Logie et al. 2012; Molina and Ramirez-Valles 2013), which can contribute to poor health. In India, TGW experience victimization in the form of police-perpetrated harassment (Shaw et al. 2012) and discrimination (Chakrapani et al. 2004). Among U.S. transgender populations, victimization is strongly associated with sexual risk (Emlet et al. 2015; Reisner et al. 2016; Sevelius 2013; White Hughto et al. 2015) and contributes to the global burden of HIV among TGW (Baral et al. 2013).
In India, the HIV prevalence among TGW is 7.5% (national average), which is nearly 19 times higher than the general population and three times higher than cisgender (i.e., non-transgender) female sex workers (NACO 2015); yet few studies have examined the impact of victimization on sexual risk among Indian TGW (Chakrapani et al. 2017a; Ganju and Saggurti 2017). Moreover, research demonstrates variation in the severity of stigmatizing experiences reported by Indian TGW (Chakrapani et al. 2017b), but no study has sought to simultaneously examine multiple forms of victimization experienced by Indian TGW. Therefore, this study sought to (1) identify patterns of victimization experienced by TGW and (2) examine between-group differences in sexual risk.
Patterns of victimization have yet to be linked to sexual risk among TGW specifically, but research suggests a relationship between victimization and sexual risk in this population. Victimization can lead to feelings of low self-esteem, which can impact the negotiation and adoption of safer sex practices (Kosenko 2011a). Some TGW use substances to cope with victimization (Nemoto et al. 2006; Reback et al. 2005), which can heighten sexual risk. Socially oppressed TGW of color engage in condomless sex and transactional sex to affirm their gender (Sevelius 2013). Furthermore, TGW who experience housing and employment discrimination may use transactional sex for financial support (Hwahng and Nuttbrock 2007), and negotiating sexual safety can be difficult (Kosenko 2011a).
While TGW who experience victimization may be at greater risk for engaging in sexual risk, current research has not accounted for the potential heterogeneity in victimization among this population. Limited research on the diversity of victimization experienced by TGW is problematic as recent evidence found that subgroups of cisgender women experiencing high victimization severity engage in more sexual risk than subgroups with low victimization severity (Walsh et al. 2012; Wilson et al. 2012). Conducting subgroup analyses for violence-informed interventions is needed (Nurius and Macy 2008), and investigating the relationship between patterns of victimization and sexual risk among TGW could inform sexual risk reduction interventions for TGW.
Application of person-centered approaches such as latent profile analysis to examine the differential health impacts of patterns of victimization is key. Unlike variable-centered approaches, person-centered approaches can identify profiles of individuals within a population who are similar to each other based on specific indicators (e.g., victimization types) and use these profiles to determine subgroups at increased risk for poor health (e.g., sexual risk). This analysis aimed to identify patterns of victimization experienced by Indian TGW and examine differences in sexual risk across these profiles.
Extending research among U.S. sexual and gender minorities (Mustanski et al. 2016), we hypothesized that at least two profiles would emerge: one profile with low victimization and another profile with high victimization. Consistent with research on patterns of victimization and sexual risk among cisgender women (Walsh et al. 2012; Wilson et al. 2012), we hypothesized that TGW in profiles characterized by higher victimization would have greater sexual risk. Understanding patterns of victimization and sexual risk among Indian TGW can help to identify high-risk groups and tailor effective risk reduction interventions for this heterogeneous population.
Materials and Methods
Procedure
Data for the current analysis were collected as part of a larger cross-sectional study exploring the health implications of stigma among 300 TGW and 300 men who have sex with men in India. Participants were recruited from six nongovernmental organizations located across four Indian states from October 2011 to January 2012. These nongovernmental organizations provide services (e.g., support groups and HIV prevention outreach) to TGW.
Trained field research interviewers screened potential participants for eligibility. Eligible participants were asked to complete a survey. Inclusion criteria were as follows: (1) aged ≥18; (2) able to provide informed consent; and (3) self-identified as a TGW. Interviews were conducted by trained field research interviewers and administered in the interviewer's native language (Tamil, Hindi, Marathi, and Bengali) under the supervision of a research assistant. Interviews took place in private rooms located in the nongovernmental organization or a private, mutually convenient location. The institutional review board of the Humsafar Trust approved the study procedures.
Participants
This analysis was restricted to TGW with complete data (N = 299). On average, participants were 29.6 years old (standard deviation [SD] = 7.8) and had an average monthly income of 8064.8 INR (SD = 6262.4) (M = $126.2 USD, SD = $98.0 USD). The majority of participants had up to a secondary education (62.2%), reported being HIV negative (77.0%); and were not married to a woman (85.0%). About three-fourths (77.0%) reported being HIV negative, and 9.5% as HIV positive. The self-identities reported were as follows: hijra = 66.7%, “transgender” (English term) = 24.7%, and jogta = 8.3%.
Measures
Latent profile victimization indicators were as follows: (1) Family nonacceptance, (2) Police-perpetrated verbal harassment, (3) Police-perpetrated physical harassment, (4) Police-perpetrated sexual assault, (5) Housing discrimination, and (6) Employment discrimination.
Indicators were assessed using six items from the 14-item Transgender Identity Stigma scale (Chakrapani et al. 2017b). This scale measures the frequency of past-year transgender-identity stigma, is validated among Indian TGW, and demonstrates construct validity with depression and social support (Chakrapani et al. 2017b). This scale was adapted from a standardized scale on exposure to transphobia (Sugano et al. 2006). An example item is “How often have you been verbally harassed by the police for being transgender (or hijra or jogta)?” Participants responded on a scale ranging from Never (1) to Many Times (4). For the latent indicators, only the violence, discrimination, and nonacceptance items from the stigma scale were used.
Sexual risk score included five variables: (1) alcohol use before sex, (2) inconsistent condom use with a male regular partner, (3) inconsistent condom use with a male casual partner, (4) inconsistent condom use with a male paying partner, and (5) multiple sexual partners.
Participants were asked, “Last time you had sex, did you drink alcohol before sex?” Participants were asked the frequency of past-month condom use with three types of partners: male regular partner (i.e., a committed partner like a spouse), male paying partner (i.e., a partner who paid the participant to have sex), and male casual partner (i.e., partner with whom the participant has a casual acquaintance and did not pay for sex). Participants who used condoms most of the time, sometimes, or never were coded as inconsistent condom users. Participants were asked the number of male sexual partners in the past month. Participants with more than 10 partners were coded as having multiple sexual partners, which is consistent with previous studies among transgender populations across cultural contexts (Clements-Nolle et al. 2001; Fernandes et al. 2015; Kellogg et al. 2001; Koh and Yong 2014; Weissman et al. 2016). Each sexual risk variable was coded as dichotomous (Yes = 1; No = 0). Responses were summed with higher scores meaning higher sexual risk. This sum score approach is consistent with previous research (De Santis et al. 2017).
Demographics included age (in years), highest level of education (i.e., illiterate, completed primary education, elementary education, high school, higher secondary education, college degree, or diploma course), average monthly income (in rupees or INR), HIV status (i.e., HIV positive, HIV negative, Never tested, or Unknown), and marital status (i.e., not married, married, separated, or divorced).
Analyses
Descriptive statistics (frequencies, means, and SDs) were conducted for participant characteristics. We conducted latent profile models using six indicators. Models were selected with the smallest values for Akaike information criterion (AIC) (Akaike 1987) and Bayesian information criterion (BIC) (Hu and Bentler 1999), bootstrapped parametric likelihood ratio test p-value <0.01 (Nylund et al. 2007), and entropy >0.80 (Ramaswamy et al. 1993). Analyses of variance were performed to examine between-group differences in demographics, victimization, and sexual risk score. Tukey was performed to determine significant pairwise comparisons. Analysis of covariance was performed to determine the effect of profile membership on sexual risk score, while controlling for age, education, income, HIV status, and marital status.
Logistic regressions were performed to examine the effect of profile membership on each sexual risk variable, separately. Adjusted models controlled for age, education, income, HIV status, and marital status. Odds ratios, 95% confidence intervals (CI), and p-values <0.05 were used to assess the significance. Descriptive, analysis of variances, analysis of covariance, and logistic regression analyses were conducted using SAS 9.4 (SAS Institute 1990). Latent profile analyses were conducted using Mplus 7.0 (Muthén and Muthén 2012).
Results
A five-profile solution was considered optimal (Fig. 1) based on small values for the AIC and BIC, higher entropy compared to the other models (excluding the one-profile solution), and meaningful profiles based on indicators (Table 1).
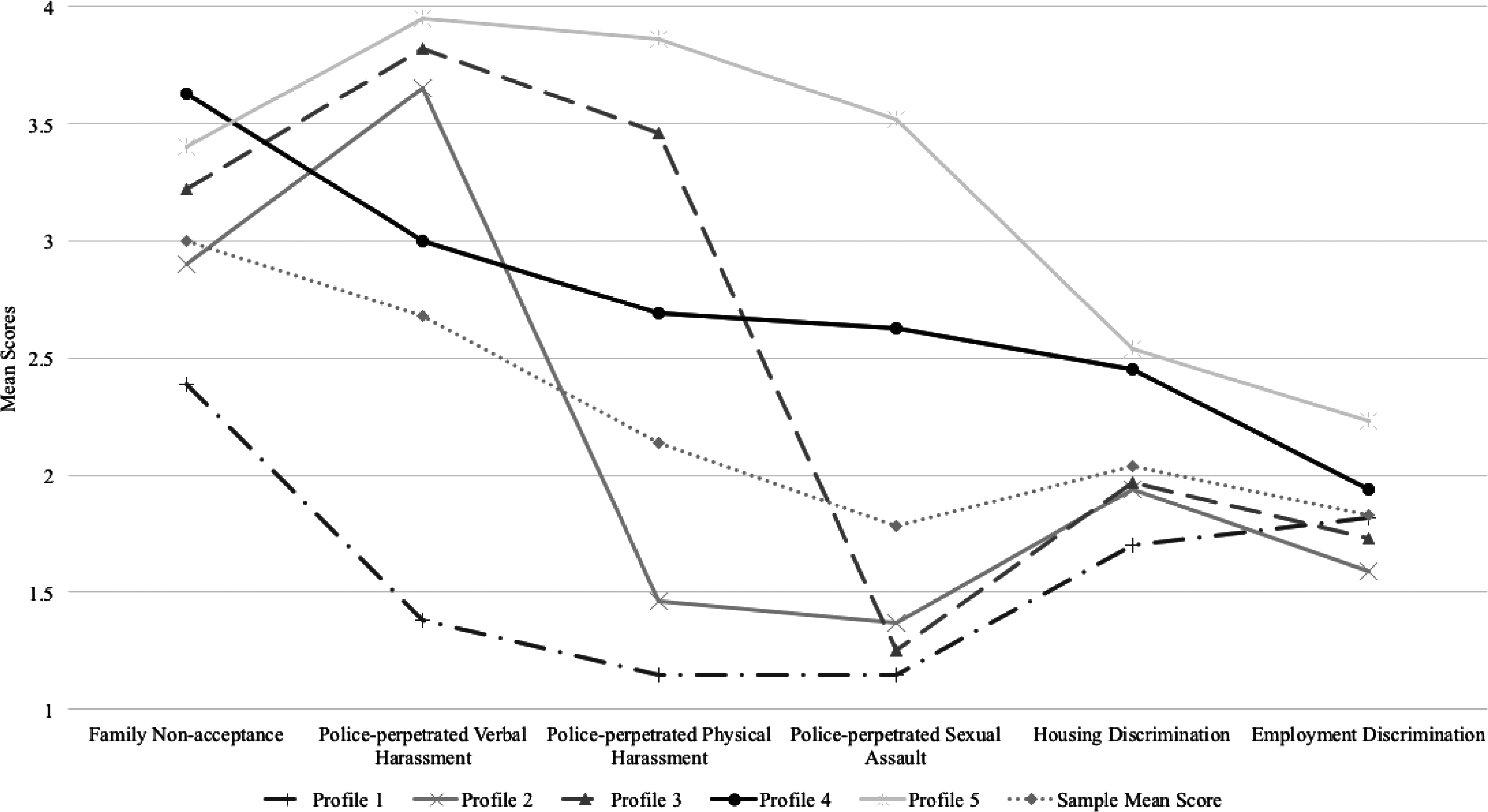
Patterns of victimization among transgender women (N = 299).
AIC, Akaike information criterion; BIC, Bayesian information criterion; BLRT, bootstrapped parametric likelihood ratio p-value.
Mean victimization scores for each profile were compared with the total mean scores to describe severity (e.g., high > sample mean, low < sample mean; Table 2). Profile 1, low victimization (35.8%) was described by low levels of all forms of victimization. Profile 2, high verbal police victimization (14%) was described by high police-perpetrated verbal harassment. Profile 3, high physical and verbal police victimization (28.8%) were described by high police-perpetrated physical and verbal harassment. Profile 4, moderate victimization (13.7%) was described by high family nonacceptance and moderate levels of other forms of victimization. Profile 5, high victimization (7.7%) was described by systematically high levels of all forms of victimization. Mean victimization scores were statistically different across the profiles (ps < 0.05).
Means (standard deviations) are shown for each profile. Total represents means (standard deviations) for the overall sample.
p < 0.05. p-values derived from Tukey's test.
Profile membership was significantly associated with demographics (Table 3). Income was higher for TGW in the moderate victimization profile compared to TGW in the low victimization, high verbal police victimization, and high physical and verbal police victimization profiles (F = 10.29, p < 0.01). Profile membership was significantly associated with HIV status (χ2 = 26.78, p < 0.01), of which the high victimization (18.2%) and high physical and verbal police victimization (14.6%) profiles had the highest proportions of TGW living with HIV. Profile membership was associated with marital status (χ2 = 30.60, p < 0.01), of which moderate victimization had the highest proportion of TGW who were separated/divorced (17.7%) and high physical and verbal police victimization had the highest proportion of TGW currently married (14.3%).
Values are given as number (column percentages) or mean (standard deviation).
Percentages may not equal 100 due to rounding.
p-Values are derived from analysis of variance or Fisher's test.
There was a main effect of latent profile membership on sexual risk controlling for age, education, income, marital status, and HIV status (F = 12.81, p < 0.001; Table 4). Greater sexual risk was found in the moderate victimization and high victimization profiles compared to the low victimization and high physical and verbal police victimization profiles (ps < 0.05). High physical and verbal police victimization also had greater sexual risk than low victimization (p < 0.05).
p-values based on Tukey-Kramer Adjustment.
SD, standard deviation.
Posthoc analyses revealed that latent profile membership was strongly associated with each sexual risk outcome (Table 5). TGW in the high verbal police victimization profile had greater odds of multiple sexual partners (adjusted odds ratio [AOR] = 3.28, 95% CI = 1.36, 8.42, p = 0.009) than TGW in the low victimization profile. TGW in high physical and verbal police victimization profile had greater odds of alcohol use before sex (AOR = 3.03, 95% CI = 1.35, 6.80, p = 0.007) and multiple sexual partners (AOR = 6.62, 95% CI = 2.60, 16.86, p < 0.001) than TGW in the low victimization profile.
Row percentages may not sum to 100% due to rounding.
AOR, adjusted odds ratio; OR, odds ratios, CI, confidence intervals.
TGW in the moderate victimization profile had greater odds of alcohol use before sex (AOR = 4.05, 95% CI = 2.04, 8.06, p < 0.001), inconsistent condom use with a male regular (AOR = 4.72, 95% CI = 2.33, 9.59, p < 0.001), inconsistent condom use with a male casual partner (AOR = 3.67, 95% CI = 1.60, 8.40, p = 0.002), inconsistent condom use with a male paying partner (AOR = 4.88, 95% CI = 2.08, 11.44, p < 0.001), and multiple sexual partners (AOR = 4.07, 95% CI = 1.78, 9.27, p < 0.001) than TGW in low victimization profile. TGW in the high victimization profile had greater odds of alcohol use before sex (AOR = 9.88, 95% CI = 3.26, 30.03, p < 0.001), inconsistent condom use with a male paying partner (AOR = 3.44, 95% CI = 1.04, 11.36, p = 0.04), and multiple sexual partners (AOR = 9.11, 95% CI = 3.01, 27.60, p < 0.001) than TGW in low victimization profile.
Discussion
This is the first study to identify latent profiles based on victimization among Indian TGW and examine associations between victimization profiles and sexual risk. Consistent with our hypothesis, our findings illustrate heterogeneity in victimization as five profiles emerged: (1) Low victimization, (2) High verbal police victimization, (3) High physical and verbal police victimization, (4) Moderate victimization, and (5) High victimization. Also aligned with our hypotheses, Indian TGW in subgroups described by higher severities of victimization tended to engage in more sexual risk than TGW in the lower victimization severity subgroups. These findings have important implications for sexual risk reduction interventions among this heterogeneous at-risk population.
Expanding current research, our findings suggest that Indian TGW have diverse victimization experiences. For example, police victimization experienced by Indian TGW can vary by type (e.g., verbal vs. verbal and physical) and level (e.g., high vs. low). Discriminatory laws that criminalize sex with cisgender men can expose TGW to police violence (UNFE 2017). Furthermore, TGW transactional sex workers may be more vulnerable to police victimization due to policies that criminalize transactional sex (WHO et al. 2013). These points are particularly salient for TGW who have sex with cisgender men as they can be punished under the Indian Penal Code—Section 377. Moreover, police use violence against Indian TGW sex workers to assert authority and obtain free sexual services (Ganju and Saggurti 2017).
Coupled with our findings, it is possible that the variation in police victimization is related to the intersection of multiple co-occurring stigmatized identities among Indian TGW (e.g., gender, perceived or actual HIV status, and transactional sex status). Consistent with research among U.S. transgender populations (Kattari et al. 2016), variations in housing and employment discrimination emerged across profiles. Our findings found that high housing and employment discrimination co-occur with high levels of all other forms of victimization, which could indicate secondary victimization. Secondary victimization occurs when subsequent victimization is enacted in response to victimization that is legal and widely condoned, such as societal rejection, and can result in denial of housing and jobs (Lombardi et al. 2002; Silva-Santisteban et al. 2012). Violence-informed structural interventions for Indian TGW are needed, including the enforcement of antidiscriminatory laws to protect sexual and gender minorities as well as police accountability.
There were significant differences in sexual risk between latent profiles. Generally, our findings are consistent with literature among cisgender women (Walsh et al. 2012; Wilson et al. 2012), suggesting that more victimization relates to more sexual risk. For example, TGW in the high physical and verbal police victimization profile engaged in greater sexual risk than TGW in the low victimization profile. Given the research on alcohol as a coping mechanism (Nemoto et al. 2006; Reback et al. 2005), Indian TGW may use alcohol to deal with victimization, heightening sexual risk.
Likewise, TGW in the high and moderate victimization profiles engaged in greater sexual risk than TGW in the high verbal police and low victimization profiles. In addition to higher severities of police victimization, these profiles also experienced discrimination. Discrimination in employment and other necessary resources can force TGW into transactional sex for income and survival (Hwahng and Nuttbrock 2007), and condom negotiation is difficult in this context (Kosenko 2011a). Extending previous research, these findings show that victimization severity and type differentially impact sexual risk among TGW.
While greater sexual risk tended to emerge among TGW in profiles with higher severities across victimization types, TGW in the moderate victimization profile were the only subgroup to have greater odds of engaging in all five sexual risk behaviors, including inconsistent condom use with male regular and casual partners. Our posthoc analyses suggest that TGW in the moderate victimization profile may be particularly vulnerable to sexual risk, and TGW in this profile may be experiencing multiple, co- occurring pathways to sexual risk. For example, Indian TGW in the moderate victimization profile may be engaging in condomless sex with regular, casual, and paying partners as a way to affirm their gender, which is consistent with past research (Sevelius 2013).
Furthermore, Indian TGW engage in condomless sex with male regular partners to show love, trust, and intimacy (Chakrapani et al. 2007), and also because of fear of being rejected (Chakrapani et al. 2015). This context may be unique to the moderate victimization profile and is consistent with research on the difficulty of negotiating safer sex between TGW and their partners (Kosenko 2011b). It might have been anticipated that TGW in the high victimization profile would have a heightened likelihood of all five sexual risk outcomes, but this was not supported in our findings. The high victimization profile had the highest prevalence of TGW living with HIV and previous research finds that people living with HIV, who are aware of their HIV status, are more willing to adapt safer sex behaviors (Chakrapani et al. 2015). Moreover, these findings may be indicative of desensitization theories. Desensitization theories suggest that individuals who experience high levels of violence may “adapt” to violence by suppressing emotional and physiological reactions and sometimes, normalizing violence (Gaylord-Harden et al. 2016). Unlike TGW in the high victimization profile, it is possible that TGW in the moderate victimization profile are not desensitized to their victimization experiences.
While this explanation is speculative, future research is needed to understand how coping behaviors vary by victimization profiles to develop effective psychosocial interventions that mitigate sexual risk. Further additional research is needed to understand mechanisms by which patterns of victimization lead to sexual risk among Indian TGW to inform sexual risk reduction interventions.
Given the high earning potential for TGW engaged in sex work as well as the risk for victimization, it is possible that profiles with higher forms of victimization had a higher proportion of TGW engaging in transactional sex work relative to those in the lower victimization profiles. It might be useful for future research to further examine the relationship between income and victimization among TGW in India.
Our findings contribute to the research on victimization and sexual risk among TGW, but these findings should be interpreted under these limitations. First, these analyses were conducted using cross-sectional data, which limit causal inferences (i.e., sexual risk may have occurred before victimization). Future studies should use prospective study designs to strengthen our findings. Second, these analyses relied on self-reported data, which may lead to underreporting (i.e., social desirability), but our concern is attenuated since our victimization prevalence is similar to other TGW studies (Chakrapani et al. 2004; Molina and Ramirez-Valles 2013; Shaw et al. 2012). HIV status was self-reported and it might be useful for future research to use objectively verifiable measures of HIV status like rapid antibody and//or serologic HIV testing.
Third, this study assessed six forms of victimization for TGW; however, the study was not an exhaustive list of all types of violence (e.g., childhood abuse). Future research should examine the prevalence of other forms of interpersonal violence, including violence within trans communities (Prabhu and Pilot 2014). Last, a diverse sample of TGW connected to nongovernmental organizations was recruited using convenience sampling, which may limit generalizability to the larger population of Indian TGW.
Conclusions
Indian TGW may benefit from multilevel HIV prevention interventions (Chakrapani 2010), and our findings offer some important suggestions for these interventions. Fundamentally, structural-level changes are needed to protect the human rights of Indian TGW, including the decriminalization of sexual relationships between TGW and cisgender men, and antidiscriminatory laws against transgender identities. Structural factors can legitimize victimization against Indian TGW, and advocacy efforts must reform policies to safeguard the sexual health of Indian TGW. For example, the 2014 The National Legal Services Authority of India (NALSA) judgment provided legal recognition and access to necessary healthcare services for Indian TGW (Narrain et al. 2015), and the implementation of similar proactive policies can be beneficial.
Moreover, national campaigns can be implemented to change the societal attitudes, norms, and behaviors of individuals using violence and discrimination toward Indian TGW such as family, employers, landlords, and police. These campaigns should promote understanding of transgender communities and recognition of their human rights. These campaigns could manifest into programs on police sensitization and promoting family acceptance. Also, sexual risk interventions should focus on predictors of risk behavior (Sevelius et al. 2009), including differential experiences of victimization. Interventions should ensure that Indian TGW receive routine screening for victimization and are offered safety planning, counseling, and other services that may help reduce the impact of victimization.
Furthermore, if these five victimization subgroups are replicated in other samples of Indian TGW, then it may be useful to tailor risk reduction interventions to these specific victimization profiles. Interventionists working with subgroups with higher victimization severities may need to address safer sex strategies. Furthermore, unique psychosocial interventions can be designed to help TGW in specific latent profiles cope with victimization experiences. For example, TGW in the two profiles with the highest severities of all forms of victimization may benefit from an intervention that helps TGW cope with experiences of police violence and find housing and jobs in the wake of housing and employment discrimination. Emotional-regulation, cognitive-reframing, social-relational, and political-empowerment coping strategies have been integrated into clinical care with transgender individuals in the United States (Mizock and Mueser 2014) and should be considered in developing coping interventions for Indian TGW who have experienced violence.
Further research is needed to identify protective factors that buffer the effect of victimization on sexual risk among Indian TGW. Engaging in resilience and collective action can mitigate the effects of discrimination (Breslow et al. 2015; White Hughto et al. 2015), and this could be an important direction for future research. Comprehensive multipronged approaches that prevent violence against TGW and help TGW manage the health consequences of violence are future opportunities to improve the health of Indian TGW.
Footnotes
Acknowledgments
This research study was funded by Indian Council of Medical Research (RHN/Adhoc/21/2010–11). T.C.W. was supported, in part, by grants from the National Institute of Mental Health (T32MH02003118 and F31MH113508-01A1). J.M.W.H. was supported by the National Institute on Minority Health and Health Disparities (1F31MD011203-01).
Author Disclosure Statement
No competing financial interests exist.