
Abstract
Violent injury is known to be a chronic, recurrent issue, with high rates of recidivism in the 5 years following initial injury. Much of the strategy behind violence intervention programs, who are tasked with reducing recidivism, is directed toward young men, while there has been little research into the unique risk factors or long-term outcomes for female victims of violence. The aim of this study was to examine the risk of violent injury and long-term adverse outcomes by gender. This retrospective study was performed using a cohort of 4337 patients presenting to the Boston Medical Center emergency department for a violent penetrating injury between 2006 and 2016. Cox proportional hazards regression models were used to estimate hazard ratios (HR) and 95% confidence intervals (95% CI) for the risk of all-cause mortality and violent reinjury at 1 and 3 years after surviving a penetrating injury. There were 88 deaths (2.1%) and 568 violent reinjuries (13.2%) within 3 years after surviving the initial penetrating injury. At initial injury presentation, women were more likely to have a preexisting mental health diagnosis and to have been injured as a result of domestic violence. While men had greater than six times the risk of 3-year mortality compared to women (HR = 6.36, 95% CI = 1.56–25.83), both genders were equally at risk for violent reinjury (HR = 1.23, 95% CI = 0.95–1.59). Men were more likely to have a stab wound (HR = 2.68, 95% CI = 1.41–5.10) or gunshot wound (HR = 7.96, 95% CI = 2.95–21.48) reinjury, while women were more likely to have an assault (HR = 1.52, 95% CI = 1.13–2.04) or domestic violence (HR = 2.96, 95% CI = 1.43–6.12) reinjury. Compared to men, the risk of violent reinjury was significantly increased for women with a history of substance use disorders (p-interaction = 0.009). These results suggest a unique trifecta of risks for women—substance use, mental illness, and domestic violence—and underscore the critical role of violence intervention programs in addressing these risks to mitigate violent injury recidivism.
Introduction
In the United States, from 2001 to 2018, homicide was the second leading cause of death among people aged 15 to 24 years, with firearm and stabbing deaths accounting for 84% and 8% of homicides, respectively. Among Black youths over the same time period in the United States, homicide was the leading cause of death with 91.0% due to firearm injuries. During this time, violent penetrating assaultive injuries caused 261,154 deaths and an estimated 3,441,710 nonfatal injuries, with 56% of nonfatal firearm injuries and 18% of nonfatal stabbing injuries requiring hospitalization following acute care in the emergency room. Survivors of violent injury are often faced with life-long mental, physical, and financial difficulties (Centers for Disease Control and Prevention 2020).
Men account for more than 80% of homicides and nonfatal penetrating injuries, while women are at greater risk of domestic and intimate partner violence despite men accounting for significantly more assaultive injuries overall (Feltner et al. 2018; Miller et al. 2019; Ranney et al. 2011). Intimate partner violence has received more research attention than any other aspect of women's victimization, but it only constitutes 30% of violent injuries (Heimer 2008). Female victims are also more likely than men to report their assaults to law enforcement (Heimer 2008).
Violent injury is known to be a chronic, recurrent issue, with recidivism rates between 5% and 45% in the 5 years following initial injury (Goins et al. 1992; Gomez et al. 2012; Nygaard et al. 2018; Sims et al. 1989). Risk factors for violent reinjury include substance use, mental illness, school failure, weapon possession, poverty, neighborhood disorganization, male gender, Black race, and gang involvement (Cooper et al. 2000; Laytin et al. 2018; Rich et al. 2005). The clinical presentations seen in the emergency department are often consequences of complex upstream systemic and structural barriers to health, reflecting long-standing racial disparities that contribute to violent injury (Beard et al. 2017; James 2019).
Hospital emergency departments are presented with a unique opportunity for interventions aimed at reducing recidivism among victims of violence at high risk for reinjury (James 2019). Several urban trauma centers have responded by establishing effective, peer-model, hospital-based violence intervention programs intended to reduce violent reinjury or escalation of violence (Bell et al. 2018; Cooper et al. 2006; Corbin et al. 2011; James et al. 2014; Juillard et al. 2016; Pino et al. 2021b; Purtle et al. 2013, 2015; Shibru et al. 2007). Seizing upon what is referred to as a “teachable moment,” these intervention programs establish a connection with the victim as soon as practical after a violent injury when the patient may be more receptive to interventions and more likely to adopt changes in risky behaviors (Pino et al. 2021a).
While much of the strategy behind hospital-based violence intervention programs is directed toward young, Black men involved in gang violence, there has been little research into the unique risk factors or long-term outcomes for female victims of community and interpersonal violence (Grisso et al. 1999; Karraker et al. 2011; Rich et al. 2005). An accurate understanding of these risks is essential for targeted and effective interventions, as the prevailing methods of violence intervention may not be as applicable for women's distinct life circumstances and risks for adverse outcomes.
In this study, we examined the demographics, injury characteristics, and long-term adverse outcomes for victims of violent penetrating injury by gender, with the objective of determining which types of interventions may be necessary for violence intervention programs to engage and alter the life course for female victims of violence. The goals of this study were to test the primary hypotheses that female victims of violence are at decreased risk for mortality and all-cause reinjury, but at increased risk for domestic violence reinjury. Secondarily, we hypothesized that female victims of violence would trend significantly older and more likely to have an existing substance use disorder diagnosis, as has been shown among rural trauma recidivists (Toschlog et al. 2007).
Methods
Study design
This retrospective study was performed using a cohort of patients presenting to the Boston Medical Center (BMC) emergency department for a violent penetrating injury between 2006 and 2016. Data were obtained from the Boston Violence Intervention Advocacy Program (VIAP) data repository, a database of all penetrating injuries (gunshot and stab wounds) due to community and interpersonal violence that have been treated in the BMC emergency department from the founding of VIAP in June 2006 through the year 2018. BMC, the region's largest safety-net hospital, is a level 1 trauma center that treats ∼70% of the gunshot and stab wound victims in the city of Boston (Boston Medical Center 2017). A detailed account of the data sources is presented in Supplementary Appendix SA1.
Ethical aspects
The Boston University/BMC Institutional Review Board approved the creation of the VIAP data repository (Study H-38631) with a waiver of the requirement of informed consent. The institutional review board deemed this study (H-39962) exempt from federal regulations for the protection of human research participants.
Study setting and population
Victims of violent penetrating injury from 2006 to 2016 were used in this analysis, allowing a minimum of 2 years follow-up for violent reinjury and a minimum of 1 year follow-up for all-cause mortality. Criteria for inclusion in this analysis required complete data for name and date of birth, which allowed for determination of follow-up outcomes. A flow chart of inclusion and exclusion criteria for the analysis is presented in Figure 1. Five transgender females and one transgender male were grouped with their self-identified gender for all analyses.
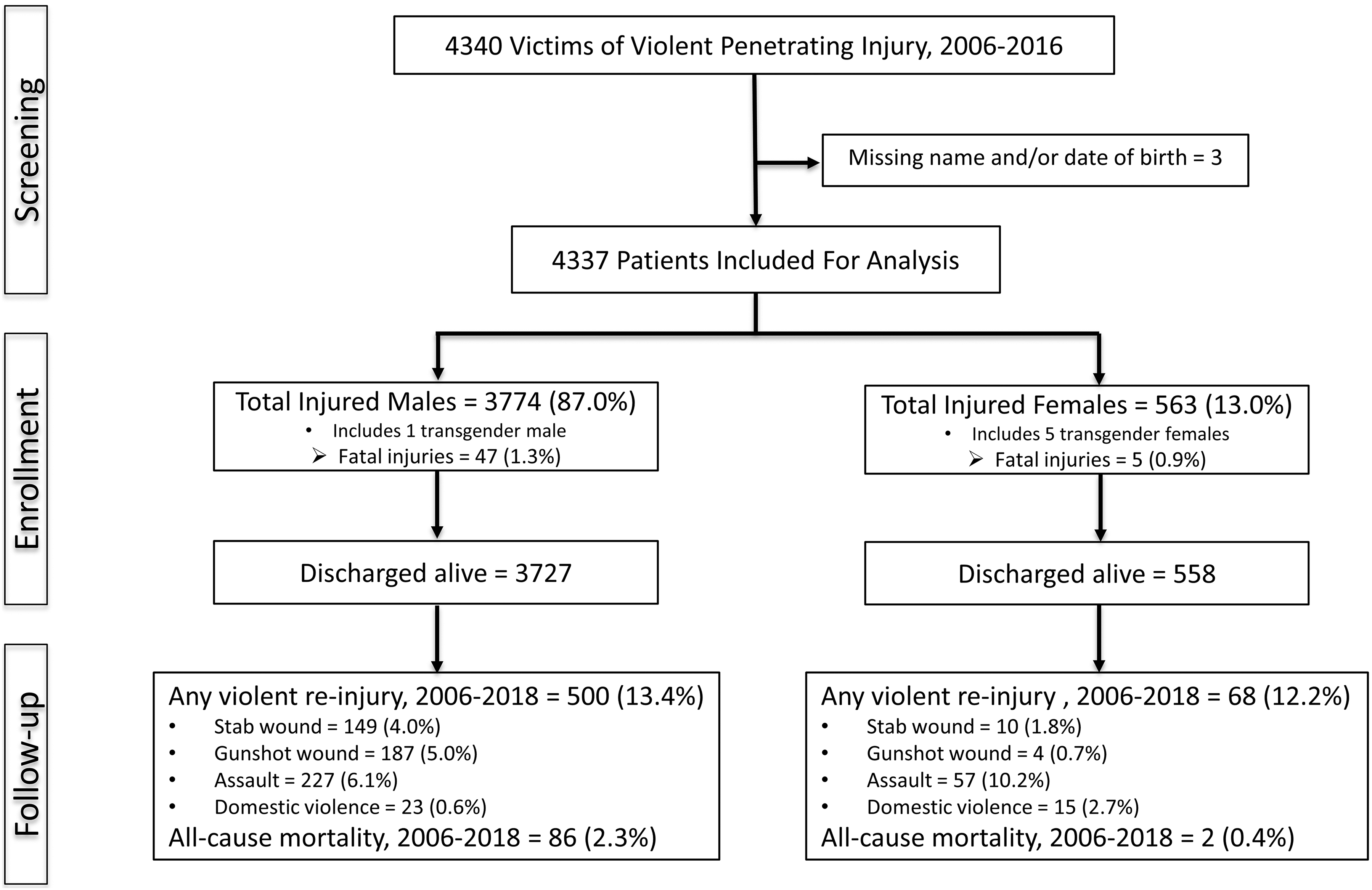
Flow chart of analysis.
Measures
The primary outcomes of this study were violent reinjury and all-cause mortality. Time to event was calculated for each event from the date of the initial nonfatal penetrating injury treated at BMC to the date of violent reinjury or death. The follow-up time for each patient was determined by the date of the initial nonfatal penetrating injury to the death date or to the last day of the year 2018 for patients surviving the study period. Covariates are described in Supplementary Appendix SA2.
Data analysis
Cox proportional hazards regression models were used to estimate hazard ratios (HR) and 95% confidence intervals (95% CI). The final multivariable Cox regression model for all-cause mortality was adjusted for significant covariates from the full model: age and race/ethnicity (c-statistic = 0.66). The final multivariable Cox regression model for all-cause victim of violence was adjusted for significant covariates from the full model: age, race/ethnicity, housing status, history of substance use/abuse, and history of mental health diagnosis (c-statistic = 0.66). The detailed steps in statistical analysis are presented in Supplementary Appendix SA3 (Shapiro et al. 1972). All analyses were conducted using STATA 16 (StataCorp 2019).
Results
Patient demographics, baseline comorbidities, and injury characteristics are presented in Table 1. Of the 4337 victims of violent penetrating injury treated in the BMC ED between 2006 and 2016, 3774 (87%) were male and 563 (13%) were female. Women were more likely to be covered by Medicare/Medicaid, while men were more likely to have no health insurance coverage (p < 0.0001). More than a quarter of female patients (26.8%) had a preexisting mental health diagnosis compared to 13.8% of male patients (p < 0.0001). While there were no differences in overall substance use disorders by gender (p = 0.22), female patients were more likely to have a disorder involving cocaine (p = 0.009) or heroin (p = 0.05). No significant differences were observed by age, race/ethnicity, or housing status.
Baseline Patient and Injury Characteristics of Victims of Penetrating Injury Treated at Boston Medical Center, 2006–2016
All values are frequencies and column percentages except age, ISS, and length of stay that are mean and standard errors. Categorical variables were compared using χ2 tests except for hospital disposition, discharge placement, disability, and AIS extremities score, which were compared using Fisher's exact test. Continuous variables were compared using the Wilcoxon rank sum test for nonparametric data. Homeless housing status includes clients living on the street, in a shelter, at friends' houses, or unknown homeless location.
p-value excluding unknown category.
AIS, abbreviated injury scale; ISS, injury severity score.
More than half of penetrating injuries were stab wounds (57.9%) when compared to gunshot wounds (42.1%). Female patients were significantly more likely than male patients to be treated for a stab wound compared to a gunshot wound (66.8% vs. 56.5%, p < 0.0001), and to be victims of domestic violence (5.3% vs. 1.1%, p < 0.0001). Compared to women, men were more likely to have injuries of the torso (p < 0.0001). More than half (61.8%) of all penetrating injuries were severe enough to require hospital admission, and male patients were more likely to be admitted to the hospital for treatment of their injuries (63.5% vs. 50.5%, p < 0.0001). Men admitted to hospital also had more severe injuries than women, as evidenced by higher injury severity scores (p = 0.0005) and longer lengths of stay in hospital (p = 0.0006).
The risk of death and violent reinjury at 1 and 3 years after surviving a violent penetrating injury are presented in Tables 2–4. Between 2006 and 2018, a total of 42 (1.0%) patients died within 1 year after surviving the initial penetrating injury and 88 (2.1%) died within 3 years. Men were more than six times more likely than women to die within 3 years (HR = 6.36, 95% CI [1.56–25.83], p = 0.01). During the same time period, a total of 280 (6.5%) patients had a violent reinjury within 1 year after surviving the initial penetrating injury and 568 (13.2%) were reinjured within 3 years. No significant differences were observed in the risk of all-cause violent reinjury by gender (HR = 1.23, 95% CI [0.95–1.59], p = 0.11). However, men were at significantly greater risk of stabbing (HR = 2.68, 95% CI [1.41–5.10], p = 0.003) and gunshot wound (HR = 7.96, 95% CI [2.95–21.48], p < 0.0001) reinjuries, while women were at greater risk of assault (HR = 0.65, 95% CI [0.49–0.88], p = 0.005) and domestic violence (HR = 0.34, 95% CI [0.16–0.70], p = 0.003). The cumulative incidences of all-cause mortality and violent reinjuries are shown in Figures 2–4.
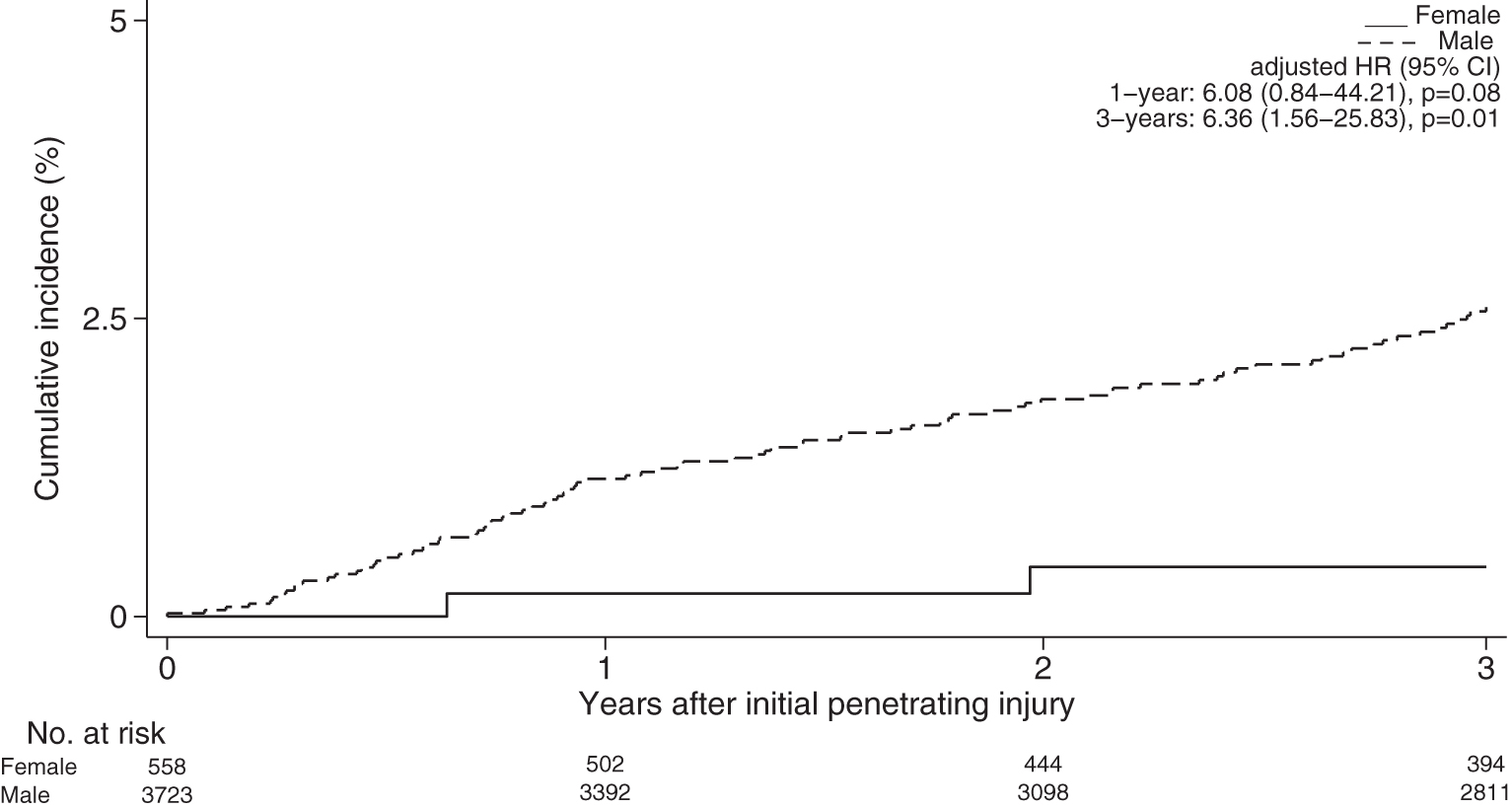
Cumulative incidence of all-cause mortality at 3 years after surviving a penetrating injury treated at BMC, 2006–2018. BMC, Boston Medical Center.
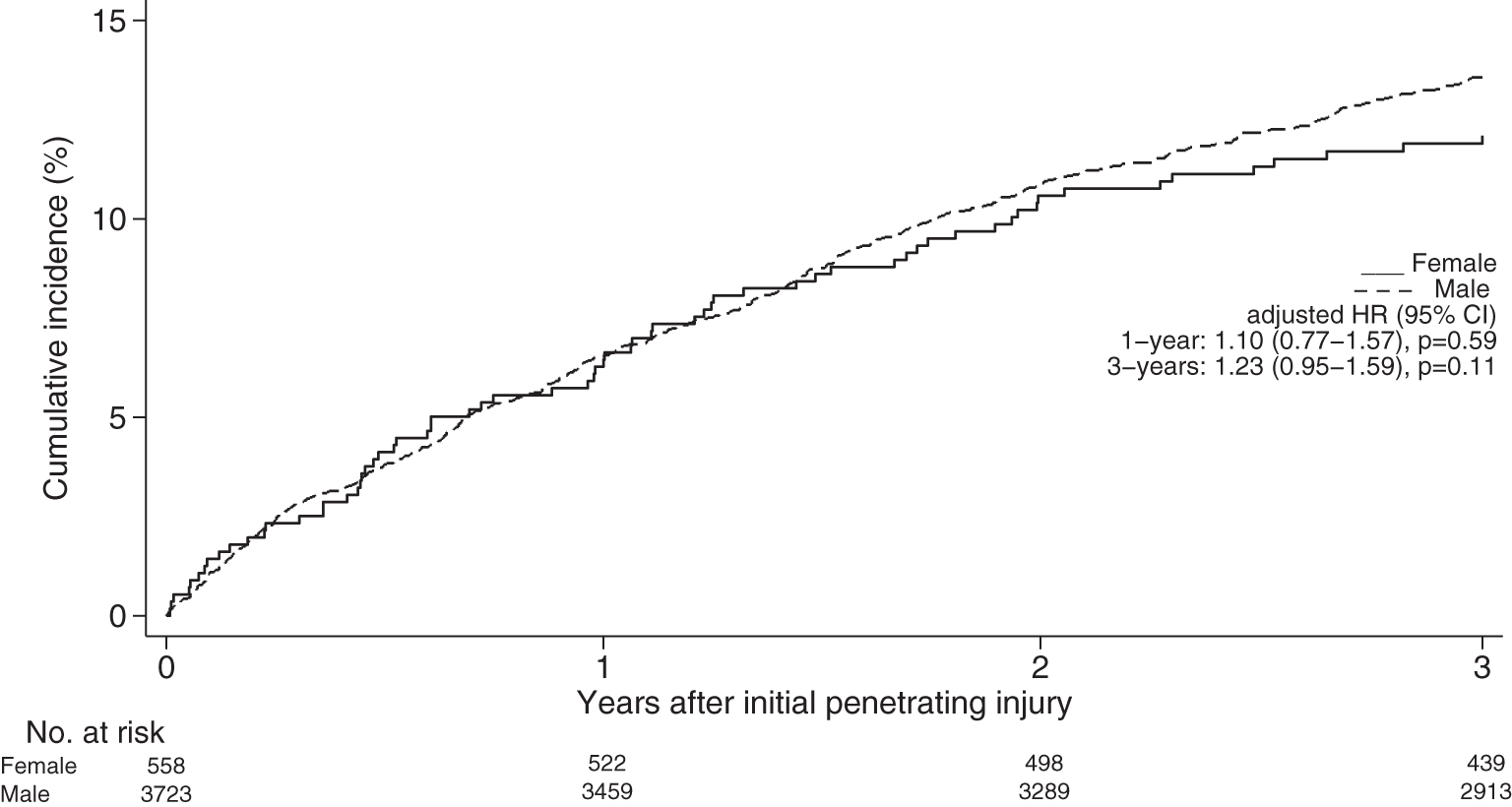
Cumulative incidence of any violent reinjury at 3 years after surviving a penetrating injury treated at BMC, 2006–2018.
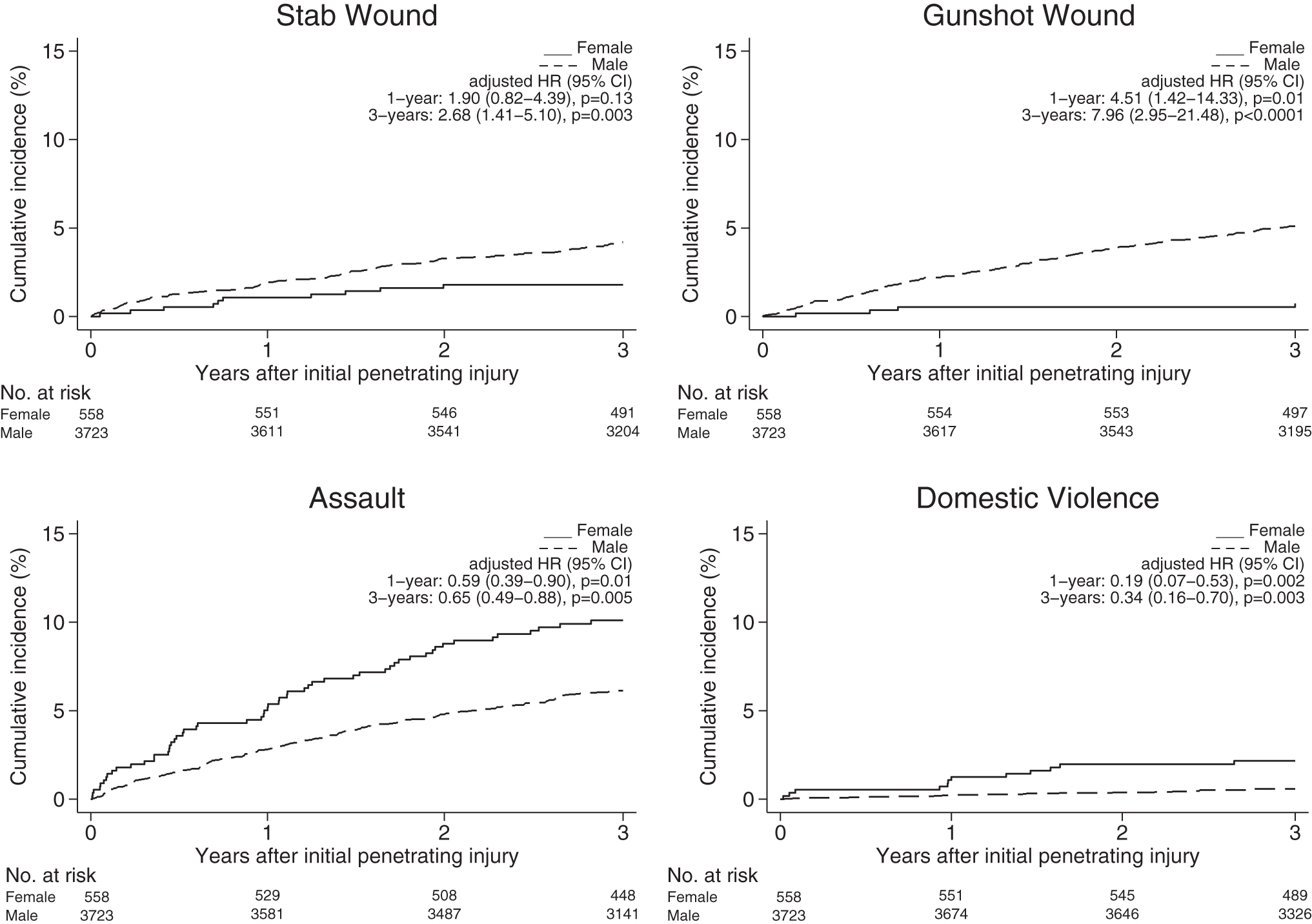
Cumulative incidence of violent reinjuries at 3 years after surviving a penetrating injury treated at BMC, 2006–2018.
Risk of Death and Violent Reinjury at 1 and 3 Years After Surviving a Penetrating Injury Treated at Boston Medical Center, 2006–2018
Cox proportional hazards regression models were used to estimate HR and 95% CI. Multivariable model for all-cause mortality is adjusted for age and race/ethnicity. Multivariable models for all-cause victim of violence and domestic violence are adjusted for age, race/ethnicity, housing status, history of substance use/abuse, and history of mental health diagnosis. All HRs are reported with women as the reference value.
95% CI, 95% confidence intervals; HR, hazard ratios.
Risk of All-Cause Mortality at 3 Years After Surviving a Penetrating Injury Treated at Boston Medical Center, 2006–2018
Cox proportional hazards regression model was used to estimate HR and 95% CI. Full multivariable model is adjusted for age, gender, race/ethnicity, insurance payer, housing status, history of substance use/abuse, history of mental health diagnosis, and injury type. Final multivariable model is adjusted for is adjusted for age, gender, and race/ethnicity.
p-value excluding unknown category.
Risk of All-Cause Violent Reinjury at 3 Years After Surviving a Penetrating Injury Treated at Boston Medical Center, 2006–2018
Cox proportional hazards regression model was used to estimate HR and 95% CI. Full Multivariable model is adjusted for age, gender, race/ethnicity, insurance payer, housing status, history of substance use/abuse, history of mental health diagnosis, and injury type. Final multivariable model is adjusted for age, race/ethnicity, housing status, history of substance use/abuse, and history of mental health diagnosis.
p-value excluding unknown category.
In a sensitivity analysis, the study population was further restricted to victims of violent penetrating injury from 2006 to 2014 to allow for a full 3 years of follow-up for death and reinjury outcomes for all included participants. After adjusting for significant covariates, the strength of the association between gender and adverse outcomes was similar to the results of the primary analysis for both all-cause mortality (HR = 10.44, 95% CI [1.44–75.10], p = 0.02), and violent reinjury (HR = 1.25, 95% CI [0.95–1.66], p = 0.11).
A comparison of risks for the six transgender patients versus both cisgender males and females are described in Supplementary Table S1. Although the sample size was small (n = 6), transgender patients were at greater risk of firearm reinjury than cisgender women (HR = 62.63, 95% CI [4.19–936.70], p = 0.003), and at greater risk of domestic violence assault than cisgender men (HR = 10.20, 95% CI [1.30–79.82], p = 0.03).
The stratified analysis of all-cause violent reinjury within 3 years is presented in Figure 5. We observed significant effect modification by age and by history of substance use disorder when comparing the risk of violent reinjury by gender. The risk of violent reinjury among children and young adults under 27 years of age was 73% greater for men compared to women; however, there were no significant differences by gender for adults aged 27 years or older (p-interaction = 0.005). Men were also at 55% greater risk of reinjury among patients with no history of substance use disorder, while the risk of reinjury was equivalent by gender among patients with a previous diagnosis of substance use disorder (p-interaction = 0.009).
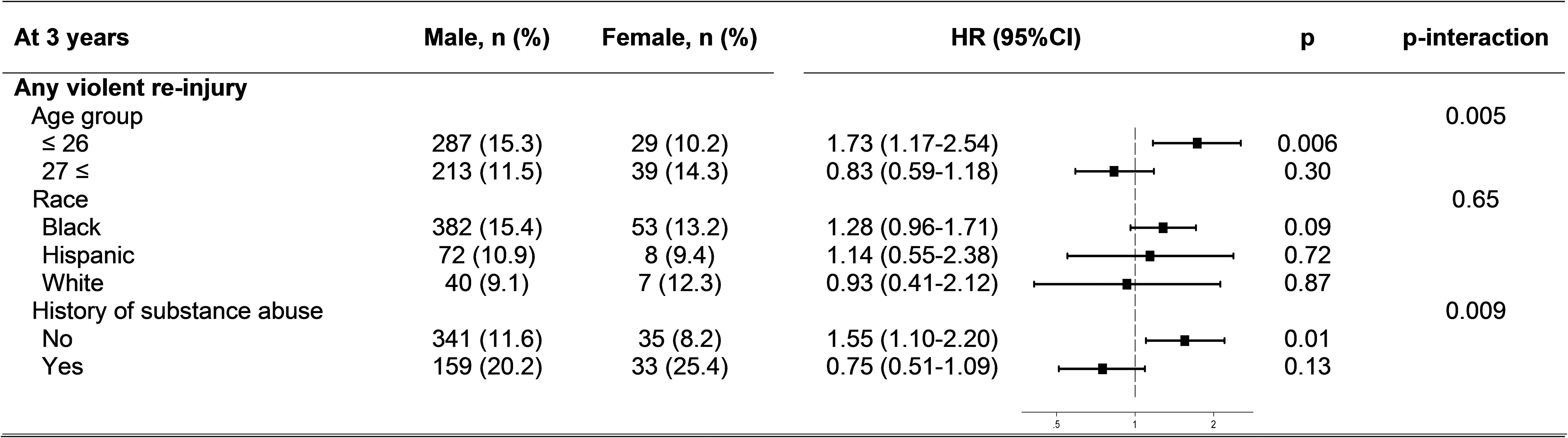
Stratified analysis at 3 years following a penetrating injury treated at BMC, 2006–2018.
Discussion
In this analysis of victims of violent penetrating injury treated at an urban, level I trauma center emergency department between the years 2006 and 2016, we report three main findings. First, men were more than six times more likely than women to die within 3 years after surviving a violent penetrating injury. Second, while men and women were equally at risk for all-cause violent reinjury, men were more likely to suffer a penetrating violent reinjury, while women were more likely to sustain an assault reinjury and to be reinjured through domestic violence. These findings are strengthened by a sensitivity analysis confirming the robustness of the results. Third, in younger patients and those with no history of substance use disorder, men were at greater risk of all-cause violent reinjury, while the risk for women was increased to the levels of men when victims were over age 26 or had a history of substance use.
Our first finding, men are at a significantly increased risk of mortality within 3 years after surviving a violent penetrating injury, supported our hypothesis and is similar to numerous previous studies (Brooke et al. 2006; Cooper et al. 2000; Jacovides et al. 2013; Kao et al. 2019; Liebschutz et al. 2010; Nygaard et al. 2018; Rich et al. 2005). Research indicates a predictable environment in which violence perpetuates poverty, dangerous neighborhoods, illicit drug and alcohol abuse, unemployment, drug dealing, and prior incarceration (Cooper et al. 2000). Several qualitative studies have emphasized the role of perceived disrespect and the “code of the street” in violent injuries and escalation of violence among young men (Cooper et al. 2000; Rich et al. 2005). In these studies, an escalating argument or act of retaliation was the cause of the majority of violent injuries. The traumatic stress experienced by victims of violent injuries, coupled with an overwhelming lack of faith in the police among this population, prompts victims to protect themselves in ways that could increase their risk of reinjury. Fear of future victimization leads these victims to consider the option of carrying a weapon for self-protection. These studies and, thus, violence intervention strategies in general may be more reflective of the male experience of violent injury and potentially not applicable to female victims of violence.
We also observed that while men and women were equally at risk for all-cause violent reinjury, men were more likely to suffer a penetrating violent reinjury, while women were more likely to sustain a blunt assault reinjury and to be reinjured through domestic violence. These observations only partially support our hypothesis because women were indeed at higher risk of domestic violence, and they were also surprisingly just as likely to be reinjured as men. Our results are comparable to the very limited published data assessing gender differences in violent injury (Jacovides et al. 2013). This previous study similarly showed that women were at high risk of assault but decreased risk of penetrating injury compared to men. The average severity level of these differing injury types also likely reflects the increased mortality for male survivors of violent injury.
The increased risk of domestic violence for women has been well documented (Brookoff et al. 1997; Feltner et al. 2018; Henning et al. 2004; Miller et al. 2019). Among domestic assault incidents involving the police, almost 90% of victims had been previously assaulted by the same assailant, often daily, with the majority of assaults involving weapons (Brookoff et al. 1997). However, most of these victims of domestic violence rarely used medical or mental health facilities for problems related to family violence despite frequent assaults. Domestic violence resulting in an emergency room visit presents an opportunity, beyond treatment of their physical wounds, to provide the victim with social services support and connection to an advocacy agency. Importantly, mental illness, which afflicts women more than men in our population, has also been previously shown to be an independent predictor of violent reinjury (Cunningham et al. 2015; Laytin et al. 2018), and represents an additional opportunity for outreach and intervention that could uniquely benefit women.
Finally, we observed that for younger patients and those with no history of substance use disorder, men were at greater risk of all-cause violent reinjury, while the risk for women was increased to the levels of men when victims were over age 26 or had a history of substance use. In our data these groups are often one and the same, as almost 34% of patients over the median age of 26 had a preexisting substance use disorder, while less than 10% of those 26 and younger had a history of substance abuse (data not shown).
The association of substance abuse with violent injury and injury recidivism has been firmly established (Bernstein et al. 2014; Cunningham et al. 2003; Pino et al. 2021b; Vitale et al. 2006). However, the interaction between substance abuse and gender in the risk of violent injury has not been fully explored (Grisso et al. 1999). Previous studies have grouped together binge drinking and casual use of marijuana, with use of hard drugs such as opioids, benzodiazepines, amphetamines, and cocaine, which are known to cause more severe physical and psychological addiction (Bernstein et al. 2014; Choo et al. 2014; Korcha et al. 2014; Ranney et al. 2011; Walton et al. 2007). This seemingly confuses the recreational use of alcohol and marijuana by younger victims of community violence, with violence stemming from the effects of drug addiction, often at the intersection of chronic homelessness and the opioid epidemic.
In our data, women were more likely than men to have a substance use disorder involving cocaine, and trended toward increased likelihood with opioids, while there were no gender differences in alcoholism diagnoses. Among both genders, those with a history of substance use disorder were twice as likely to die or have a violent reinjury within 3 years compared to patients with no substance use diagnosis. However, among only women, the risk of violent reinjury among those with substance use disorders increased to 3.5 times the risk of women with no diagnosis. While we cannot be certain of the causal relationship of substance use and violent injury in these data, of the patients who died within 3 years after a violent penetrating injury with a drug or alcohol overdose as the cause of death, more than 70% had a preexisting substance use diagnosis at the time of injury (data not shown).
These results give valuable insight into the root causes of violence among women compared to men, and what types of interventions are necessary to combat this epidemic. Trauma centers with similar patient populations should consider novel strategies to engage vulnerable populations not typically targeted by intervention programs, including expanded partnerships with drug treatment centers, and transitional housing programs.
Worthy of note, transgender individuals are not overrepresented in our sample (0.14%) compared to the general population (0.60%; Flores et al. 2017), despite previous findings that transgender people are at increased risk for violent injury (Mizock et al. 2008; Winter et al. 2016). It is likely, however, that transgender individuals were not captured in older data unless they chose to engage with a VIAP advocate, as the options to select transgender or nonbinary gender would not have existed on medical forms. While the sample size of transgender patients in our population is too small to make meaningful conclusions, we observed that transgender patients have a greater likelihood for gunshot reinjury than cisgender women, but also greater likelihood for domestic violence than cisgender men. The risk factors for violent injury and injury recidivism among transgender populations is likely distinct from both cisgender men and women and warrants further investigation in a larger population.
Limitations
The results of this study are subject to several limitations in study design and availability of longitudinal data. First, our cohort consisted of patients from a single medical center, which limits the generalization of our findings to other patient populations. Second, the analysis was limited to comorbidities recorded in the patients' medical records or self-reported at the time of injury. It is likely that an additional subset of the patient population has undiagnosed mental health and substance use disorder comorbidities. However, patients suffering from these comorbidities are disproportionately high health care utilizers (Ng et al. 2019; Vickery et al. 2018) and would likely have an extensive medical history at BMC, the city's safety-net hospital and a central depot for substance use disorder treatment services.
Third, information regarding patient reinjury was restricted to data from BMC medical records and Boston Police Department reports. Injuries not occurring in the Boson metro area, or injuries that did not involve the Boston police, or not treated at BMC will not be captured in this analysis, leading to an underestimation of the risk of reinjury. Fourth, there is likely an underreporting, and differential reporting by gender, of domestic violence as injuries categorized as such must be reported to an emergency department worker or VIAP staff member, or investigated by Boston Police Department, leading to an underestimation of the risk of domestic violence injury. Fifth, information regarding patient mortality was restricted to BMC medical records, the Massachusetts Death Files from 2006 to 2017, and the U.S. Social Security Administration Death Master File from 2006-May, 2013. Deaths occurring outside of Massachusetts after May, 2013 will not be captured in this analysis, leading to an underestimation of the risk of mortality.
Sixth, matching of patients to outcomes is performed, in order of priority, using social security numbers, dates of birth, and names. Missing social security number information increases the likelihood of mismatched outcomes or excluded adverse events. Seventh, while the use of time to event methodology does account for differential follow-up time, patients captured in 2015–2016 have not been followed for three full years for death and reinjury outcomes and are censored at heavier rates than patients captured from other years.
Conclusions
In conclusion, this study demonstrates that although women constitute a small proportion of the total victims of violent penetrating injury, they have unique risk factors for violent injury and adverse outcomes. While men were more than six times more likely than women to die within 3 years after surviving a violent penetrating injury, men and women were equally at risk for violent reinjury. Further, men were more likely to suffer a penetrating violent reinjury, while women were more likely to sustain an assault or domestic violence reinjury. Baseline substance use disorders and mental illness, established risk factors for violent injury, were more common in women compared to men. Moreover, a history of substance abuse greatly increased the risk of violent reinjury for female patients compared to male patients. These results suggest a distinctive trifecta of risks for women—substance use, mental illness, and domestic violence—and underscore the critical role of violence intervention programs in addressing these risks to mitigate violent injury recidivism among women.
Footnotes
Authors' Contributions
Study concept and design: E.C.P. and E.D.; Acquisition of the data: E.C.P., F.F., T.L.J., and E.D.; Analysis and interpretation of the data: E.C.P.; Drafting of the article: E.C.P.; Critical revision of the article for important intellectual content: E.C.P., F.F., T.L.J., E.F.R., and E.D.; Statistical expertise: E.C.P. and E.F.R.; and Acquisition of funding: E.D.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Supported by the Department of Emergency Medicine, Boston Medical Center.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.