
Abstract
Gender-based violence (GBV) is a major public health issue for street-based female sex workers (SBFSWs), particularly in low- and middle-income countries like Bangladesh. There is a vast knowledge gap regarding the underlying issue; therefore, the authors aimed to perform this study to contribute to the literature by exploring the prevalence and associated factors of the severity of GBV based on secondary data collected from SBFSWs by the United Nations Population Fund (UNFPA) in 2021. In Bangladesh, it was revealed that about 95% of the SBFSWs had experienced GBV of any form. The prevalence of physical and sexual violence was more than 81% and 78% among SBFSWs, respectively. It was worthwhile to note that more than 40% of SBFSWs experienced all forms of GBV. Results also revealed that age, education, monthly income, marital status, group sex, negotiation for fees, client load, and consistent condom use had a significant effect on the severity of GBV among SBFSWs. Policymakers are recommended to take proper actions considering the magnitude and direction of the effects of the associated factors to reduce the prevalence of GBV among SBFSWs and help to access other jobs, which will contribute to improving several Sustainable Development Goals.
Introduction
Despite being previously thought of as a legal, social, and private issue, gender-based violence (GBV) against women has evolved over time to become an overwhelming and most pervasive severe public health (physical and mental) and human rights issue worldwide, regardless of sociodemographic and economic background (Alemayehu et al., 2015; Fairbairn, 2020; Hossain et al., 2022; Rivera-Rivera et al., 2004). It is undoubtedly the most socially tolerated form of human rights violation. Over the past decade, researches revealed that GBV may have an impact on global health policies and initiatives (Heise and Ellsberg, 1999; IGWG of USAID, 2008). According to the United Nations, GBV is referred to as “any act of GBV that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life” (United Nations, 1993). The World Health Organization (WHO) describes GBV as a global epidemic that encompasses physical, psychological, sexual, financial, and verbal abuse (Alemayehu et al., 2015; Schwitters et al., 2015; Wellesley Centers for Research on Women and Development & Training Services, 2003). Worldwide, it is estimated that “one in three women will be beaten, coerced into sex, or otherwise abused in her lifetime” by an intimate partner or by others who are not romantically involved with her, whereas less than 10% of sexual assaults will ever be reported to the police (García-Moreno et al., 2005; Schwitters et al., 2015; United Nations, 2009). According to the WHO, one in four women (27.0%) experiences physical or sexual abuse in her lifetime, while the same is notably higher (50.0%) among the ever-married women aged 15–49 years (WHO, 2021). GBV is a sensitive and complicated subject that is incredibly underreported in Bangladesh. The majority of GBV victims are women and young girls. Sixty percent of all assaults in 2020–2021 were on girls, including young children. Women, girls, and children make up 88.2% of GBV cases when taken as a whole (United Nations Development Programme, 2022). In Bangladesh, spousal violence against women is one of the main causes of violence (Johnston and Naved, 2008). According to a study, there is a high prevalence of domestic violence and oppression against the wife and other household workers, such as the chef, cleaner, and housekeeper, and it takes the form of torture, carelessness, rape, forced rape, physical attack, and sexual assault. Women and girls also experience harassment while traveling and that the business environment is unfavorable for women entrepreneurs because of social and cultural restrictions, a lack of political commitment, and insufficient governmental provisions for creating a workplace that is welcoming to women (Shahen, 2021).
Female sex workers (FSWs) are a marginalized and socially stigmatized group of women who are particularly vulnerable to GBV throughout the world (Deering et al., 2014; Hendrickson et al., 2018; Ikuteyijo et al., 2022; Schwitters et al., 2015; Shannon et al., 2014). Although data are lacking in many countries, global and regional studies show that GBV against FSW is prevalent, frequent, and often severe (Carroll and Mendos, 2017; Decker et al., 2015; Evens et al., 2019). FSWs are referred to as women who consensually exchange sexual intercourse for money or other goods, as a livelihood activity (Ikuteyijo et al., 2022; Overs, 2002; Standing, 1992; UNAIDS and UNDP, 2008). According to the International Labor Organization (ILO), FSWs are at a higher threat of experiencing GBV perpetrated by clients, brothel owners and other controllers, law enforcement personnel, police, nonpaying or intimate partners, families, neighbors, and peers (Cruz and Klinger, 2011; Deering et al., 2014; Hendrickson et al., 2021; Schwitters et al., 2015).
GBV can have detrimental effects on FSWs' physical and mental health (Hendrickson et al., 2021; Hendrickson et al., 2018). In addition, due to GBV, FSWs are more likely to contract Human Immunodeficiency Virus (HIV) and other Sexually Transmitted Diseases (STDs)/Sexually Transmitted Infections (STIs) through forced sex without a condom, inconsistent condom use, and condom misuse (Alam et al., 2013; Hendrickson et al., 2018, 2021; Hussain and Saha, 2022; Ikuteyijo et al., 2022; Sultana, 2015). According to modeling on population-based data from Central Asia and East Africa, reducing GBV might help in decreasing HIV incidence among FSWs (Decker et al., 2013; Hendrickson et al., 2018; Shannon et al., 2015). Existing evidence revealed that a reduction in physical or sexual violence among sex workers may help in achieving ∼25% reduction in HIV infections among them (Decker et al., 2013).
According to the literature, GBV-exposed FSWs have a very high propensity for suicidal thoughts, suicide attempts, depression, and posttraumatic stress disorder (Ikuteyijo et al., 2022; Millan-Alanis et al., 2021). Furthermore, FSWs can suffer from sexual and reproductive health consequences, including forced and unwanted pregnancies, unsafe abortions, and traumatic fistula.
The likelihood of experiencing GBV among street-based female sex workers (SBFSWs) is shaped by the sociostructural setting in which they live and work (Beyrer et al., 2015; Decker et al., 2016; Hendrickson et al., 2021; Hendrickson et al., 2018). The severity of GBV among SBFSWs' is influenced by different structural factors such as the criminalization of sex work, inequitable gender norms and stigma, and discrimination toward SBFSWs (Beyrer et al., 2015; Deering et al., 2014; Hendrickson et al., 2018; Shannon et al., 2014). In addition, the effect of political conflict may worsen the GBV among SBFSWs (Ouma et al., 2021). Sex workers are more vulnerable to violence through their working conditions or by compromised access to services. Many of them have little control over the conditions of sexual transactions, for example, negotiating fees, deciding clients, and types of sexual services, etc.
SBFSWs in Bangladesh face daily threats to their personal and collective safety. A study among the FSW in Chittagong revealed that sexual, physical, and emotional violence were very common among the FSWs, leading toward substance use disorders (SUD), and FSWs who experienced emotional violence were more vulnerable to use drugs (Hengartner et al., 2015). But legal policies to protect sex workers' rights are still inadequate. Although sex work is legal in Bangladesh (Karim, 2020), the related activities (e.g., soliciting in public places) are still criminalized and thus make the sex workers more vulnerable toward all forms of violence.
However, while the authors know that the experience of GBV among SBFSWs is common, relatively little is known regarding the prevalence, perpetrators, associated factors, and severity of GBV in low-resource setting like Bangladesh. Therefore, GBV is an emerging concern for SBFSWs within this context. With this backdrop, the objective of this study was to explore the nature of GBV, including prevalence, perpetrators, and severity, and associated factors of the severity of GBV among SBFSWs in Bangladesh. The associated factors of severity of GBV were identified using ordinal logistic regression model.
Methods and Materials
Data
This study was carried out based on secondary data, which were collected by the United Nations Population Fund (UNFPA) and the Joint United Nations Programme on HIV/AIDS (UNAIDS) under a cross-sectional study on GBV among FSWs and transgenders (hijra) in 2021 in the context of Bangladesh. Data were collected on several characteristics, including sociodemographic, economic, sexual behavior, and GBV from 368 SBFSWs in Dhaka district.
The sample size of SBFSWs was determined using the formula for proportions considering 95% confidence interval (CI), 5% level of precision with prevalence of 38%, and 5% nonresponse rate. A semistructured questionnaire was used, and face-to-face interview was conducted with the sampled SBFSWs.
Institutional Review Board (IRB) approval
This study does not require Institutional Review Board (IRB) approval because it was conducted based on the secondary data.
Response variable
According to the United Nations (United Nations, 2014) and to WHO (Ellsberg and Heise, 2005), there are five forms of GBV which include physical, sexual, emotional, and economic violence and controlling behavior. The measuring indicators of all forms of GBV are listed in Table 1. A dichotomous variable corresponding to each of the forms of GBV was defined and categorized as “1” if SBFSW experienced it and “0” if SBFSW did not experience it. Finally, the target response variable of this study, called “severity of GBV,” was defined from the dichotomous variables corresponding to the forms of GBV and was scored as below:
Indicators Used for Measuring Different Forms of Gender-Based Violence
Predictor variable
The sociodemographic and economic characteristics, such as age (10–19, 20–24, ≥25 years), education (no formal education, primary, secondary, or higher), monthly income in Bangladeshi Taka (<10,000, 10,000–14,999, ≥15,000), and marital status (unmarried, currently married, separated), as well as sexual behavior, including living with a sex partner/spouse (yes, no), group sex (yes, no), time of selling sex (<5, 5–9, ≥10), use of condom (yes, no), penetrative sex (0–7, 8–14, 15–21, >21), decision maker of a type of sex (either client or FSW, both), negotiation for condom (Yes, no), negotiation for fee (yes, no), client load (0–1, 2–3, ≥4), change of income during coronavirus disease 2019 (COVID-19; same or increased, reduced), and consistent condom use (yes, no) were considered as predictor variables of the severity of GBV in this study. The categories of each predictor variable are presented in Table 2.
Significance of Bivariate Association Between the Severity of Gender-Based Violence Among Street-Based Female Sex Worker and Their Different Sociodemographic and Sexual Behavior Characteristics
BDT, Bangladesh Taka; COVID-19, coronavirus disease 2019; FSW, female sex worker; GBV, gender-based violence; SBFSW, street-based female sex worker.
Statistical analyses
Descriptive statistics such as proportion were used to analyze the sociodemographic characteristics of the respondents, perpetrators, and prevalence of GBV. The chi-square test was used to select initial set of predictors of the severity of GBV to be included in the model and later by assessing the bivariate association with the cutoff p-value of 0.2. In this study, this cutoff value was selected for possible inclusion of all relevant variables in the multivariable logistic regression model. The similar approach was used in several previous studies (Austin and Tu, 2004; Hosmer and Lemeshow, 1989). The ordinal logistic regression model was used to measure the effect through adjusted odds ratio (AOR), and the Wald test was used to test the significance of the effects of the selected predictors on the severity of GBV with p-value up to 0.1. The statistical analyses were carried out using the IBM SPSS V25.
Results
The sociodemographic characteristics of the study participants are demonstrated in Figure 1. Among the respondents, almost three-fourths (76%) were aged 25 years or older. About 43% of the SBFSWs were found as illiterate followed by primary education (42%). More than half of SBFSWs (52%) were currently separated followed by 37% being currently married. About 37% of SBFSWs said that their monthly income was less than 10,000 Bangladesh Taka (BDT), and one-third (34%) had a monthly income of 15,000 BDT or more (Fig. 1).
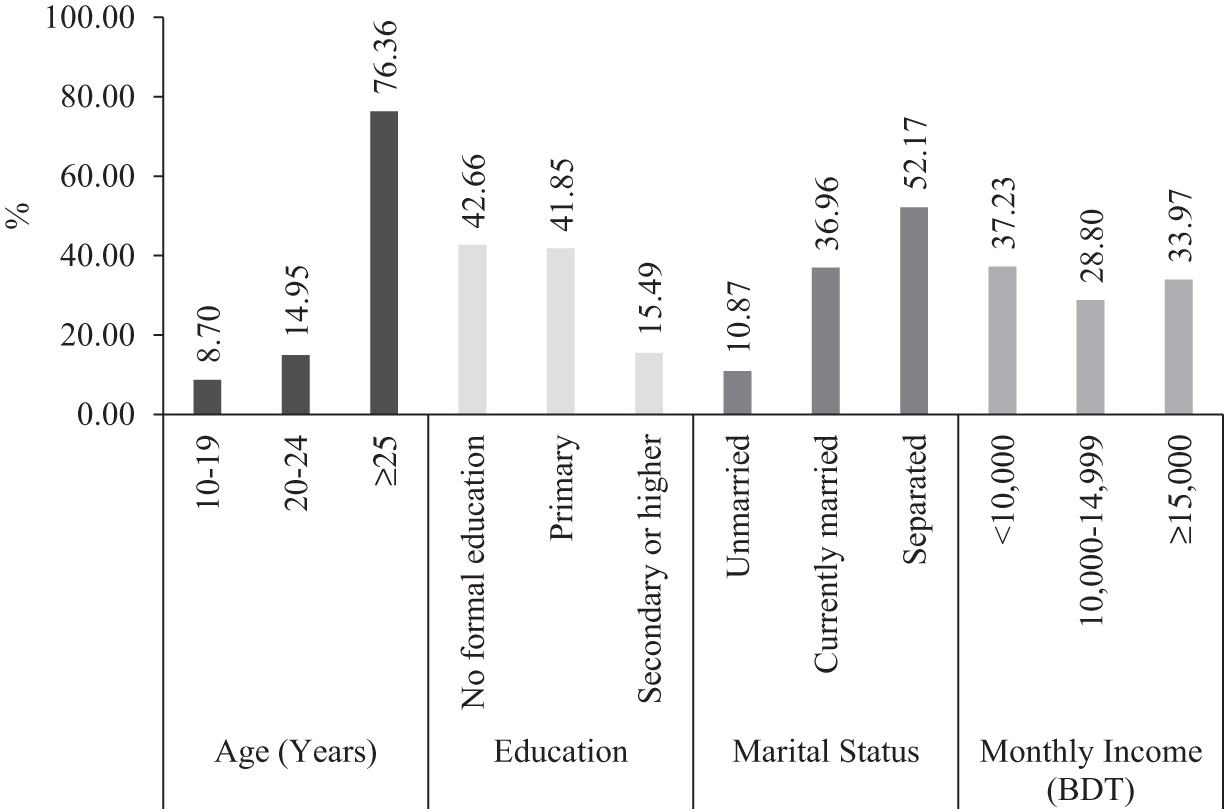
Sociodemographic characteristics of the respondents.
The prevalence of each form of GBV among SBFSWs at any time and during COVID-19 is illustrated in Figure 2. In case of those on the streets, the prevalence of all forms of GBV was observed at around 80%. During COVID-19, the prevalence of all forms of GBV was decreased (Fig. 2).
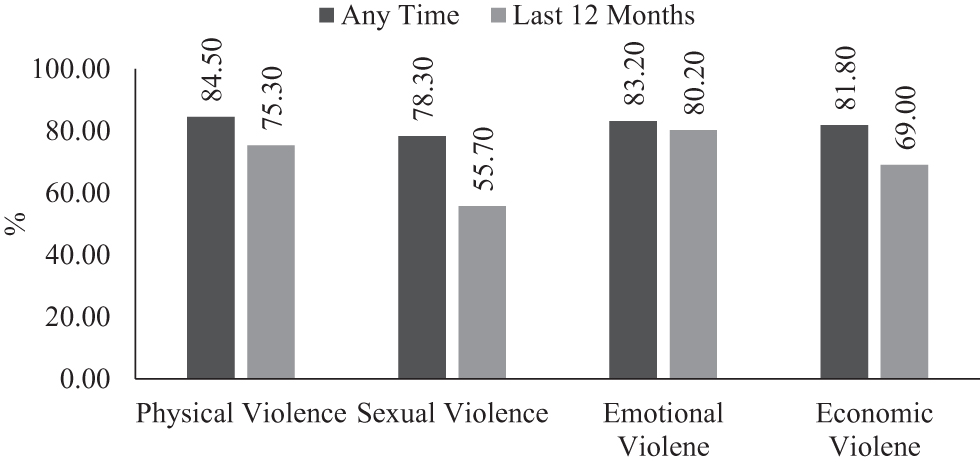
Prevalence of different forms of GBV at any time and during COVID-19. COVID-19, coronavirus disease 2019; GBV, gender-based violence.
Figure 3 illustrated the distribution of perpetrators of different forms of GBV among SBFSWs. The client was reported as highest frequent perpetrator followed by police, local mastan, community people, and regular live-in partner/husband for all forms of GBV (Fig. 3).
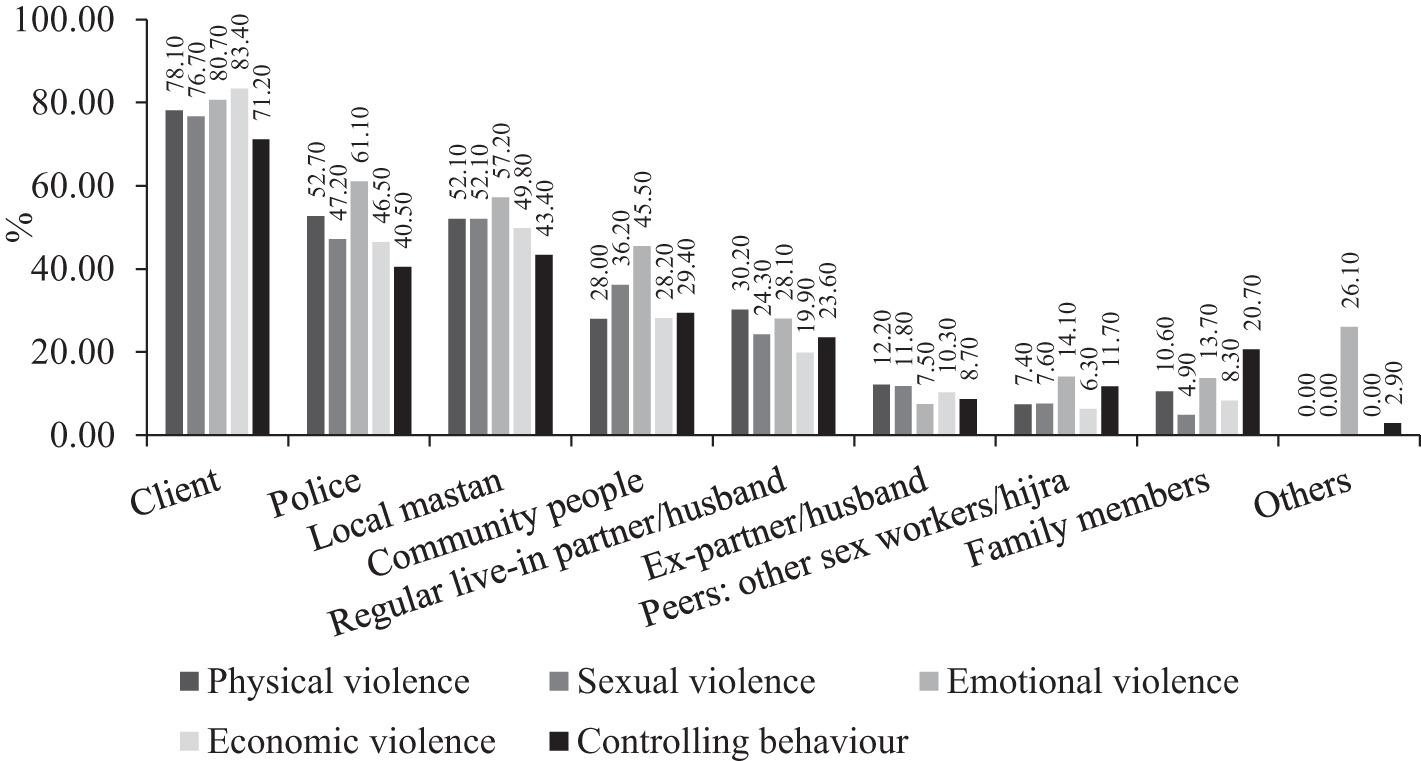
Distribution of perpetrators for all forms of GBV among SBFSWs. SBFSWs, street-based female sex workers.
The severity to GBV among SBFSWs is shown in Figure 4. It was observed that more than 40% of SBFSWs experienced all five forms of GBV, and around 15% of FSWs experienced any four forms of violence in streets (Fig. 4).
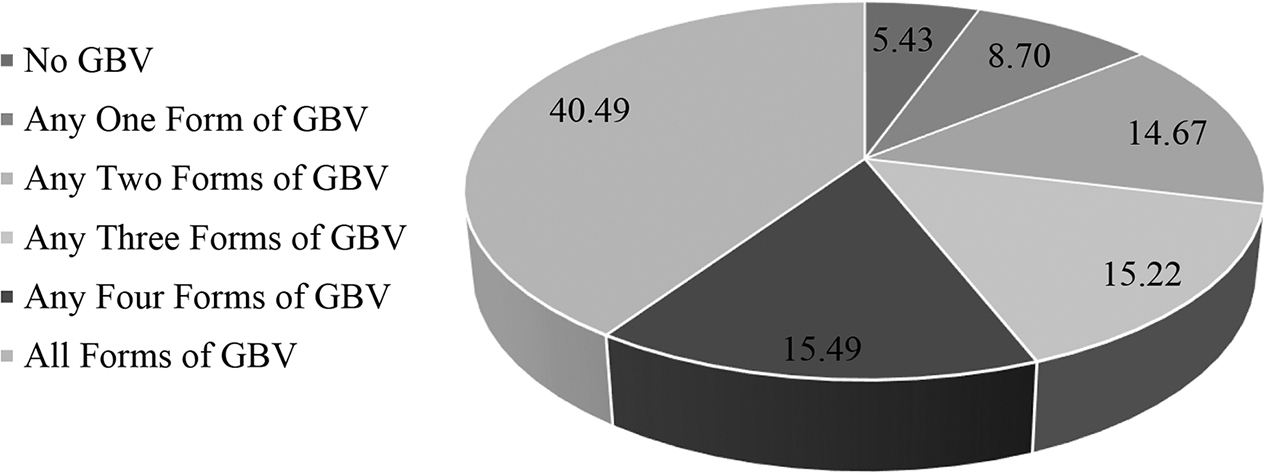
The severity of GBV among SBFSWs.
Results obtained from the bivariate analysis of the severity of GBV with different sociodemographic and behavioral characteristics are presented in Table 2. When p-value of 0.2 was considered as the cutoff point, the severity of GBV among SBFSWs was significantly associated with age, education, monthly income, marital status, penetrative sex, decision of type of sex, negotiation of fees, client load, consistent condom use, group sex, and change of income during COVID-19 (Table 2).
The SBFSWs who were aged 25 years or older had a lower likelihood (AOR: 0.63, 95% CI: 0.40–0.98) of experiencing multiple forms of GBV compared to those aged 10–19 years. Interestingly, the SBFSWs with formal education had a higher likelihood (primary educated: 33% and secondary or higher educated: 35%) of being more susceptible to GBV than those who had no formal education. The likelihood of GBV observed declined by 45% among the SBFSWs who had a monthly income of 15,000 BDT or more compared to those who had a monthly income of less than 15,000 BDT. Compared to the unmarried SBFSWs, the currently married and separated SBFSWs had 41% and 34% lower chances to experience GBV, respectively.
The SBFSWs reported that group sex had higher odds (AOR: 1.63, 95% CI: 1.26–2.12) of being more susceptible to GBV compared to those who did not perform group sex. The SBFSWs who negotiated for the fees with clients were less likely (AOR: 0.56, 95% CI: 0.44–0.72) to experience GBV than those who did not negotiate for the fee. Moreover, the SBFSWs with client load of more than one were more likely (AOR: 1.20, 95% CI: 0.82–1.75 for client load of 2–3 and AOR: 1.57, 95% CI: 0.97–2.54 for client load of ≥4) to experience multiple forms of GBV than those who had an average client load of one or less. Higher odds (AOR: 1.36, 95% CI: 1.06–1.75) of GBV were observed among the SBFSWs who reported using condoms consistently than those who did not.
To get more insights, a separate multivariable ordinal logistic regression model for SBFSW with the significant associated factors was also carried out, and the results are presented in Table 3. It was revealed that sociodemographic characteristics such as age, education, monthly income, and marital status, as well as sexual behavior, including group sex, negotiation of fees, client load, and consistent condom use, had a significant effect with a p-value of ≤0.1 on the severity of GBV among SBFSWs.
Adjusted Effect of the Significantly Different Sociodemographic and Sexual Behavior Characteristics on the Severity of Gender-Based Violence Among Street-Based Female Sex Worker
AOR, adjusted odds ratio.
Discussion
The prevalence of GBV has an increasing trend in Bangladesh (UNFPA, 2016). SBFSWs are more vulnerable to GBV because they are perceived to be easy prey and cannot report violence to the police or seek help due to well-established fears of being arrested, criminalized, or evicted, and their testimonies are often undermined or dismissed (Capraro, 2018). The GBV experienced by SBFSWs is an essential component of the overall GBV of a country. Therefore, it is quite impossible to prevent GBV of a country without preventing the GBV against SBFSWs (Capraro, 2018).
Identifying different strategies to prevent GBV is crucial not only for the lives and well-being of girls and women but also for the accomplishment of the Sustainable Development Goals (SDGs; UNFPA, 2016). Consequently, appropriate policies or strategies to address GBV among SBFSWs should be undertaken. Lacking knowledge of the factors that increase the severity of GBV among SBFSWs creates an obstacle to develop an appropriate strategy for lessening the GBV among them. Therefore, this study aimed to explore the prevalence, perpetrators, and associated factors of GBV's severity among street based FSWs in Bangladesh.
This study found that about 95% of SBFSWs were reported to experience at least one form of GBV at any time in their past life; however, the prevalence of each form of GBV was around 80%. It is important to note that there is a gap in the literature on this issue in the context of Bangladesh. The review of available literature from the out context of Bangladesh reveals that around 61.0% of the FSWs experienced at least one occurrence of client-perpetrated GBV in Northern Uganda (Ouma et al., 2021).
In addition, economic (58.7%) and emotional (52.0%) violence were the most prevalent forms of GBV, whereas sexual violence (21.0%) was the least prevalent in the context of Northern Uganda (Ouma et al., 2021). The prevalence of client-perpetrated GBV among FSWs was 82% in Kampala, Uganda (Schwitters et al., 2015). Another study conducted in Latin America and Caribbean reported that almost all of the FSWs had an experience of emotional violence and controlling behavior and more than 75% had an experience of economic, physical, and sexual violence (Evens et al., 2019). Moreover, the prevalence of sexual or physical violence among FSWs was 60% in Cameroon (Decker et al., 2016). More than a half (57%) of FSWs experienced GBV in Vancouver, Canada (Shannon et al., 2009). However, GBV against SBFSW was found as low during COVID-19; it may be due to lockdown, financial crisis of the clients, and fear of COVID-19.
In their study, more than 40% of SBFSWs experienced all considered forms of GBV. There is a gap of knowledge on the severity of GBV. However, a previous study reported that 32.7% of the FSWs experienced two or three forms of client-perpetrated violence, followed by 19.0% of four forms (Ouma et al., 2021). The authors found that clients were the most frequent perpetrators followed by police, local mastan, community people, and regular live-in partner/husband. These findings are in line with the findings of previous studies (African Sex Worker Alliance, 2019; Bakh and Ibisevic, 2010; Cruz and Klinger, 2011; Deering et al., 2014; Evens et al., 2019; Hendrickson et al., 2021; Schwitters et al., 2015).
The younger SBFSWs and/or those with lower income had a higher chance of experiencing more severe GBV. There are some studies conducted on the relationship of age and income level with GBV among FSWs (Alemayehu et al., 2015; Ayamah et al., 2022; Hendrickson et al., 2018; Shannon et al., 2009). Previous studies also showed that the younger FSWs had a higher chance of GBV (Ayamah et al., 2022; Shannon et al., 2009). Another study reported that younger aged FSWs had a higher likelihood of severe GBV (Hendrickson et al., 2018). The reason behind this may be their lower ability to protect themselves from riskier sexual activity such as condom less sex, rough sex style, more client load, etc. compared to the older aged FSWs.
Moreover, it was reported in a previous study that the FSWs having low income had a two-fold higher likelihood of client-perpetrated GBV in Uganda (Ouma et al., 2021). Another study conducted in Ethiopia reported similar findings (Alemayehu et al., 2015). In contrast, the FSWs with higher monthly income were more likely to experience severe GBV in Tanzania (Hendrickson et al., 2018). This may be due to the fact that FSWs with low income are intended to increase their income; therefore, they may have a lower tendency of negotiating with the client for a fee; riskier sexual behaviors; safer sex, sex places, and style of sex (Ouma et al., 2021).
Formal educated SBFSWs were more likely to experience more severe GBV. Most likely, because they are more aware of the hazards to their health, strive to negotiate with clients, and report suspicious behavior to the authorities to avoid riskier sexual behavior. However, there is a scarcity of the evidence on the relationship between education and GBV among FSWs; therefore, the authors think that a separate study is needed to understand this relationship clearly. The likelihood of more severe GBV was higher among married and separated SBFSWs. This finding is in contradiction to the existing literature (Ayamah et al., 2022).
Higher client load and penetrative sex increased the likelihood of experiencing multiple forms of GBV among SBFSWs. The result of the earlier research is consistent with this finding (Hendrickson et al., 2018). Comparatively, street-based FSWs are more likely to have more clients, which could raise their risk of more severe GBV (Hendrickson et al., 2018). A higher client load also increases the risk of HIV for both clients and SBFSWs (Evens et al., 2019). Moreover, negotiation for fees reduced the likelihood of experiencing multiple forms of GBV among SBFSWs. There is a lack of evidence, in the existing literature, on the relationship between negotiation for the fee with clients and the severity of GBV among SBFSWs. The author's perception is that if SBFSWs demand their expected fee from the client after performing sex, the client may act more violently and may likely use physical violence—such as slapping and beating—as well as economic violence and/or controlling behavior.
The SBFSWs who used condoms consistently were more likely to experience more severe GBV. The clients are not interested to use condoms during sexual intercourse because of fear of losing sexual pleasure or better sexual sensation and embarrassment over buying condoms (Ghimire et al., 2011; Tamang et al., 2001). Therefore, when sex workers forced the clients to use a condom, the clients may behave more violently and coerce for unprotected sex by proposing more money or physical violence. The negotiation for condom use with clients or partners may be more difficult for mobile FSWs; therefore, the rate of inconsistent condom use is higher among them (Goldenberg et al., 2014; Rushing et al., 2005; Saggurti et al., 2012; Verma et al., 2010). In a previous study, it was reported that sexual violence is significantly associated with inconsistent condom use (Abelson et al., 2019). Unprotected sex and inconsistent condom use also increase the risk of HIV for both clients and sex workers (Evens et al., 2019).
Furthermore, the SBFSWs who had group sex were more likely to experience more severe GBV. In a riskier sexual environment like a street, clients often negotiate with the sex worker and take her to some residence, after which he may force the sex worker to have group sex—that is, intercourse with more than one person at once. Nonetheless, when the sex worker refuses to have group sex, the clients torture and coerce her to do group sex.
The United Nations' ongoing efforts to advance gender equality are reflected in SDGs 5 and 10(Leal Filho et al., 2022). Women tend to be more susceptible to assault, discrimination, and under-representation in the economic, business, and political realms (Milazzo and Goldstein, 2019). The significance of gender is in relation to health and well-being, education, as well as link between other relevant SDGs (Morgan et al., 2020). The authors believe that the findings of this study will make a strong foundation for further research aiming for establishing the relationship of severity of GBV among SBFSWs with the associated factors. The findings will also help the policymakers in articulating appropriate policies, which can accelerate achieving SDGs by reducing GBV among SBFSWs. In this regard, the appropriate policy measures may include developing a support system for the GBV survivors among SBFSWs by linking them with the health services and legal support. In addition, government can help sex workers to find employment and provide counseling so they can stop doing sex work and live in their community as regular people.
Strengths and Limitations
One of the major strengths of this study is attached in its novelty. Furthermore, the study adopts a robust methodology, which enhances trust on the estimates. However, this study has some limitations as it considers street based female sex workers from the capital city Dhaka and, thus, is not a country-representative study. Even though the authors anticipate that, due to adopting vigorous methodology, the study estimates will represent the overall situation of GBV among SBFSWs in Bangladesh. Second, as the data were collected using a cross-sectional study design, it is not possible to establish any causal relationship of the GBV among FSWs with the influential factors. Third, there may be some variables that are related to GBV but are not considered in this study due to availability of requisite data. A further study will be focused on the inclusion of other relevant variables, and the authors believe that qualitative findings along with quantitative results will enhance the quality of the future study.
Conclusion and Recommendation
This study explored that nearly a half of the SBFSWs experienced all forms of GBV by the clients, police, local mastan, community people, and regular live-in partner/husband. The sociodemographics such as age, education, monthly income, and marital status, as well as sexual behaviors, including group sex, negotiation of fees, client load, and consistent condom use, significantly influenced the GBV's severity among SBFSWs with the varying magnitudes and directions. It is therefore recommended that appropriate policies should be designed, in accordance with the outcomes of this study, for reducing the burden of GBV among SBFSWs, control the overall GBV in Bangladesh, and help to access other jobs, which will help to improve economic outcomes (SDG 1, 2, 8), health outcomes (SDG 3), educational outcomes (SDG 4), gender equality (SDG 5, 10), and peace and inclusion (SDG 16).
Footnotes
Acknowledgment
The authors express their appreciation to the UNFPA and the Joint United Nations Programme on HIV/AIDS (UNAIDS) for allowing to access their dataset. The authors are thankful to the editor and three reviewers for providing comments and feedback that help to improve the quality of the article.
Authors' Contributions
Conceptualization: M.N.H., F.A., M.M.H. Data Curation: M.N.H., S.K., R.A.N. Formal analysis: F.A., M.M.H. Methodology: M.N.H., F.A., M.M.H. Supervision: M.N.H. Visualization: F.A., M.M.H. Writing—Original Draft: M.N.H., F.A., M.M.H. Writing—Review and Editing: M.N.H., F.A., M.M.H., S.K., R.A.N.
Data Availability
This study is based on the secondary dataset that will be available upon reasonable request to the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.