
Abstract
Introduction:
Parastomal hernia is the most common long-term complication after stoma creation, with an estimated incidence of 5%−60%. 1 Parastomal hernias can be a source of chronic pain and discomfort, as well as impaired quality of life from issues with stoma function and ostomy appliance application. 2 Small bowel obstruction and strangulation necessitating emergent surgical intervention can also result. 3 Several surgical options have been described for the repair of parastomal hernias, with the most common being keyhole and Sugarbaker repair. Pauli’s repair, first described in 2016 by Eric Pauli, is a modified Sugarbaker parastomal hernia repair that utilizes the retrorectus space to lateralize the bowel and place a mesh in a sublay fashion. 4
Case:
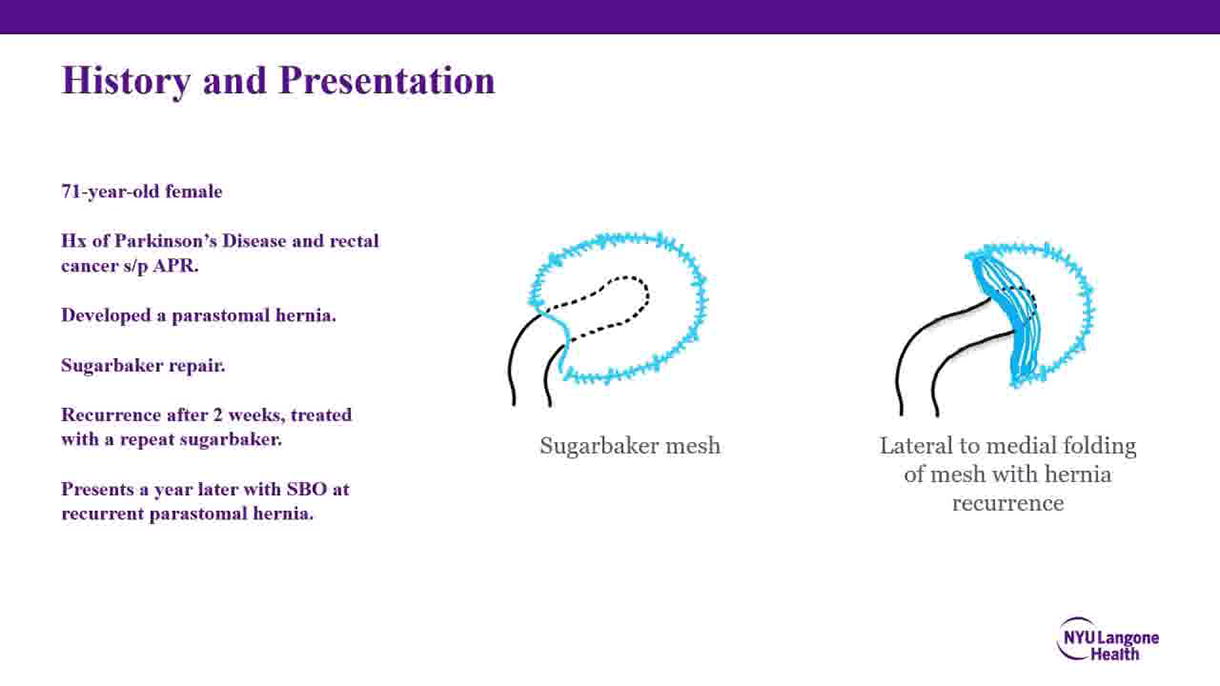
We present the case of a 71-year-old female with a past medical history of Parkinson’s disease and rectal cancer. The patient underwent abdominoperineal resection and subsequently developed a parastomal hernia, which recurred after two failed attempts at repair using the Sugarbaker procedure. The patient presented with small bowel obstruction resulting from the parastomal hernia. Small bowel obstruction was successfully relieved by manually reducing the parastomal hernia contents.
Procedure:
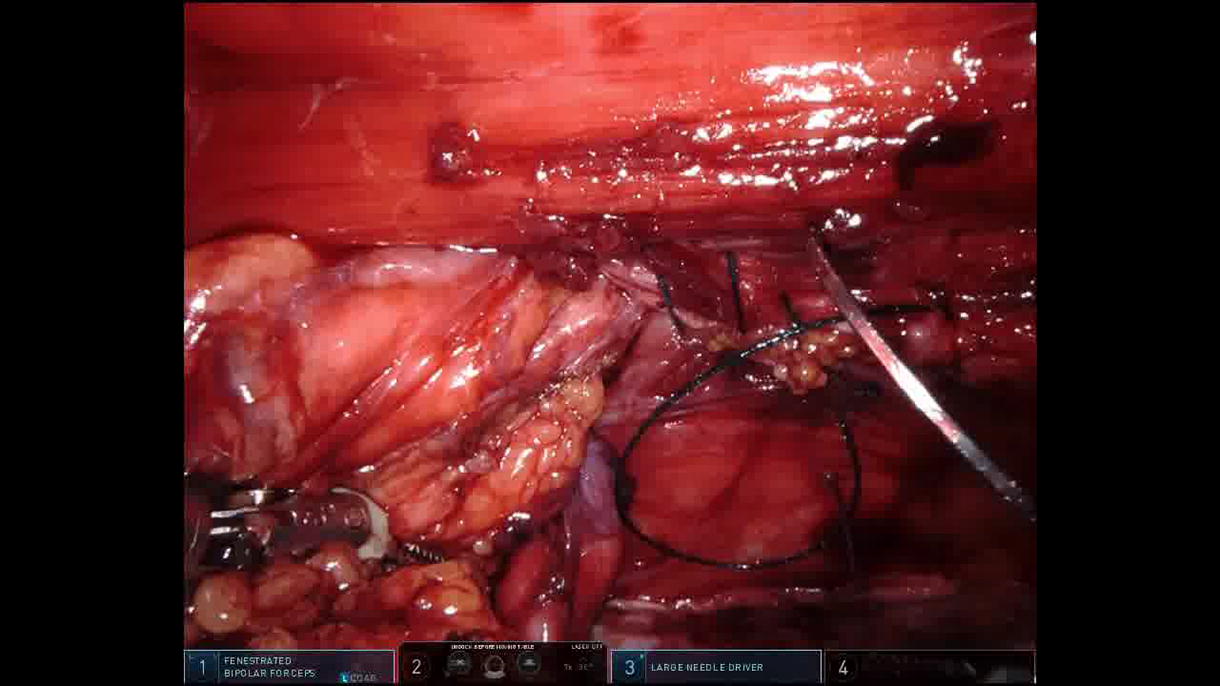
To perform the Pauli repair, we used a Da Vinci Xi robotic platform. The robot was docked on the right side, and three robotic trocars were placed on the right side of the abdomen. An assist port was placed in the left upper quadrant. The procedure required enterolysis and separation of the parietal peritoneum of all adhesions. The mesh was then removed off the peritoneal wall. The preperitoneal space was entered just lateral to the midline, and left-sided retrorectus dissection was performed, which was continued laterally with transversus abdominis release allowing for adequate sublay placement beneath the hernia repair. Fascia around the stoma was dissected to allow for bowel mobilization. The posterior sheath was divided laterally to allow bowel lateralization. The anterior fascial defect was then closed with a slowly absorbing unidirectional barbed monofilament suture. The colon is then sutured to the lateral side wall using an absorbing suture. A V-loc suture is used to close the posterior abdominal wall fascia, lateralizing the colon entry into the peritoneal cavity. The retrorectus space was then measured, and a 30 cm × 20 cm mesh was placed in the retromuscular space, securing it in an underlay fashion. The mesh should cover the sutured colon to the side wall for 5 cm. The peritoneal flap was then closed with an absorbable running V-loc suture.
Results:
The patient had an uneventful postoperative recovery and was discharged home on postoperative day 6. There was no evidence of recurrence at a 12-month follow-up.
Key points in performing a Pauli repair The anatomical planes of the Transversus Abdominis Muscle Release (TAR) dissection must be respected. When positioning the conduit, the exit site from the posterior elements should be as lateral from the stoma site as possible, and angulation should be minimal, creating a long, “lazy” intramuscular conduit. The natural lie of the bowel should be followed towards lateralization, and an oblique course from the stoma site is acceptable. The concept of lateralization allows for the forces that generate stomal hernia to be buttressed by the posterior elements of the abdominal wall and its accompanied mesh reinforcement. To minimize the risk of enteroprosthetic fistulation, the bowel is positioned such that the antimesenteric side is against the abdominal wall, and the mesenteric fat is abutting the surface of the mesh. In this video, the mesh is affixed to the “roof” of the retro muscular space, or underside of the abdominal wall musculature. With this approach, care must be taken during fixation of the mesh to avoid slinging the mesh too taught against to conduit, thereby causing an obstruction or promoting an area of friction between the bowel and the mesh. The procedure can be altered by placing the mesh on the “floor” of the operative space, or posterior sheath. With the latter approach, mesh fixation is minimized and may allow the mesh to lie in a more natural position.
All relevant data have been included in the article. Furthermore, information is available upon request to the authors.
The authors declare that they have no conflict of interest.
There are no commercial associations to be disclosed by the authors.
The authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Runtime of video:
5 mins 30 secs.