
Abstract
Introduction:
Currently, a sleeve gastrectomy is the most common bariatric procedure and resolves reflux symptoms in approximately 50% of patients. However, a sleeve gastrectomy is associated with new-onset reflux in 8–15% of patients postoperatively. This video depicts the surgical management of a patient who underwent a sleeve gastrectomy and developed refractory GERD. Ultimately, the patient underwent a hiatal hernia repair with resection of retained fundus.
Methods:
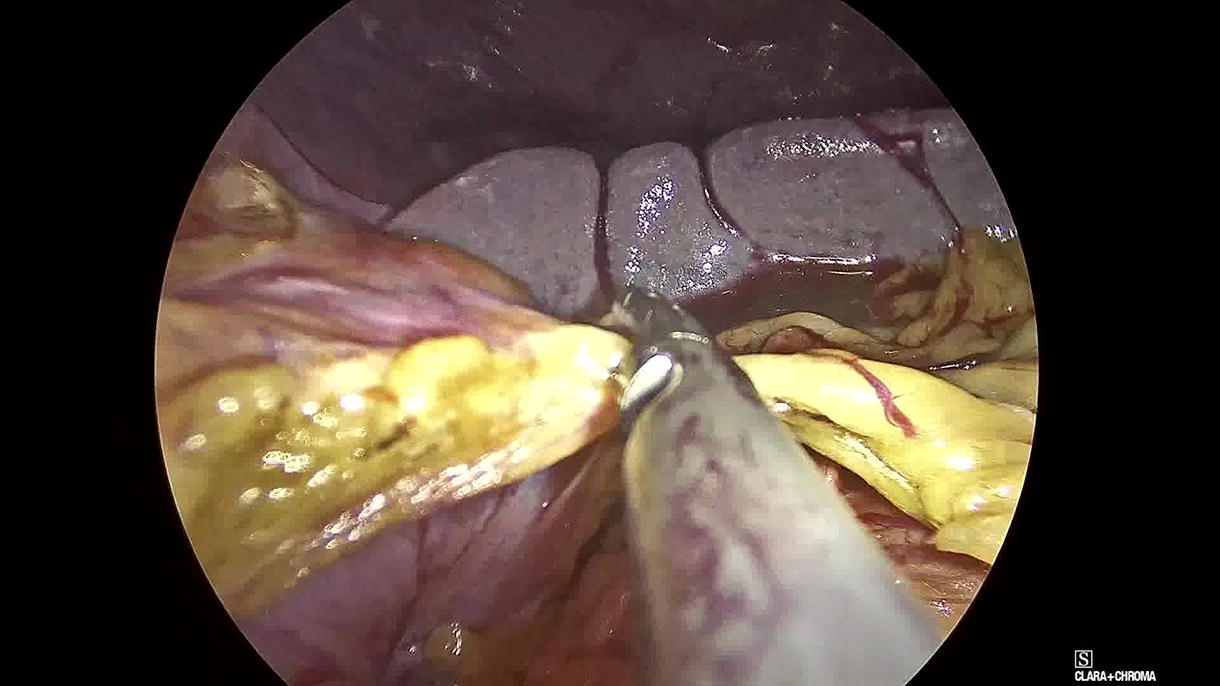
A 46-year-old female presented with reflux and regurgitation. She had undergone a sleeve gastrectomy 7 years prior to presentation. She underwent an upper gastrointestinal series that documented reflux with a sliding hiatal hernia. An upper endoscopy identified the hiatal hernia and a gastric diverticulum just below the Z line. The reported diverticulum was actually consistent with a retained fundus as opposed to a gastric diverticulum. Based on the patient’s symptoms and anatomical findings, a laparoscopic hiatal hernia repair and resection of the retained fundus was scheduled. The procedure began medially to open the lesser sac overlying the caudate lobe. The procedure then proceeded laterally to release the adhesions along the staple line of the sleeve gastrectomy. Next, the right crus was dissected, and the esophageal hiatus was circumferentially dissected. The esophagus was mobilized into the abdominal cavity to obtain 5 cm of intra-abdominal esophagus. Once the hiatus was dissected and the adhesions were divided, the retained fundus was evident along the posterior aspect of the stomach. This portion of the stomach was released from the pancreas, and the retained fundus was divided with a stapler. The hiatus was then repaired in a tension-free manner with several 0 silk sutures for a tension-free repair.
Results:
The patient was advanced to a clear liquid diet on postoperative day one and then discharged to home on postoperative day 1. She advanced to a regular diet by postoperative day 5 at home. She was asymptomatic in terms of GERD and she had discontinued PPIs after 2 weeks. Her follow-up esophagram did not show any evidence of a recurrent hiatal hernia or retained fundus.
Conclusion:
Reflux after a sleeve gastrectomy is not uncommon. If GERD occurs postoperatively, patients should be evaluated for anatomical defects or surgical complications. Hiatal hernias, obstruction at the angularis incisura, and a retained fundus may be addressed surgically. Alternatively, conversion to a gastric bypass may be the best option.
Conflicts of interest:
There are no conflicts of interest.
Author Disclosure Statement:
There are no commercial associations during the last three years that might create a conflict of interest in connection with this video.
Patient Consent:
Authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Runtime of video:
8 mins 37 secs.