
Abstract
Marjolin's ulcers (MU) are skin malignancies that form over burn injuries. These very aggressive ulcers can result in functional and wound healing impairment, and require a well thought out treatment plan. Physiotherapy offers resources to help promote recovery of these patients, as described in this case report, in which the patient with a history of burn in the lower limbs evolved to malignancy 32 years later. This patient underwent tumor resection of the left foot, with recurrence and lymphadenectomy. Physical therapy included the application of high-frequency generator (HFG) for wound healing and exercises for functional recovery. The treatment lasted for many months and resulted in the improvement of the surgical wound areas, pain, swelling, sensitivity, strength muscle, and gait. It was observed that the use of HFG can be a tool in the tissue repair of surgical wound after the resection of MU; however, further studies need to be carried out to suit parameters and ensure safety of cancer patients.

Introduction
M
There is poor investigation on follow-up and the conditions under which the patients survives after the control of MU, especially because they may have delayed wound healing, infection, necrosis, pain, and functional impairment. 1 The use of physical agents can improve wound healing 4 and skin transplants viability 5 and it has been growing as a complementary method to topical and medication agents to treat some complicated wounds. 6
The High-Frequency Generator (HFG) operates on alternating current of high frequency (1.000–200.000 Hz), low intensity (60–100 mA) with a tension between 6 and 40 kV depends on the body resistance (about 10.000 Ohms). The passage of the current through the glass electrode, which has rarefied air or neon gas inside, promotes the ionization of these gas molecules, represented by sparking effects and then, produces ozone around the area. The ozone produced is very instable and during the application of the HFG over the skin surface, this molecule easily decomposes in oxygen (O2) and atomic oxygen (O). The formation of these atomic oxygen molecules influences the biochemical events of cellular metabolism and promotes antimicrobial, bactericide and fungicide effects. 4,6,7 These properties accelerate the tissue repair and can control the infection process as showed by some experimental 4,7 and clinical studies 6,8 described on Table 1.
Experimental and clinical investigations about high frequency/ozone effects
HFG, High-Frequency Generator; NaOCl, sodium hypochlorite; PSST, Pressure Score Status Tool; PUSH, Pressure Ulcer Scale for Healing.
Clinical Problem Addressed
The main effects of the physical agents are that they can stimulate cellular metabolism, cellular growth, and angiogenesis, 4 –7 but there is no consensus if they can stimulate tumor growth in humans, as well. 3,5,9 However, several benefits have been showed to cancer patients, as reduction of pain, mucositis, necrosis, hematoma, and lymphedema. 3,5,9 To the best our knowledge, there is no information about the treatment of chronic wound by HFG after MU resection. Therefore, the objective of this article is to present a case report of a man who developed a complicated wound after MU resection and which was treated by HFG.
Case Presentation
This case presentation was approved by Ethics Committee of Brazilian Institute of Cancer Control (IBCC) and, the patient authorized the use of his data and images through an informed consent. A 59 years-old male patient, swarthy, incomplete basic education level, worked as a watchman, smoker, sedentary, body mass index of 24.66 kg/m2, hypertensive, and Hepatitis C. He suffered second and third degree steam burns in the lower limb extremities in 1975 at age of 25, and a skin graft was performed on left foot. In 2007, 32 years later, he presented a SCC on left foot diagnosed as MU. In October 2008, a resection was performed followed by a reconstruction of flexor digitorum longus muscle, subcutaneous cell tissue, and skin using a myocutaneous flap. In December 2008, a new and wide excision followed by skin graft was performed due to tumor recurrence. It evolved to necrosis, resulting in a surgical debridement and the postoperative wound remained opened. In February 2009, he was submitted to lymphadenectomy, due to metastasis, of the paraaortic, iliac, inguinal, and obturator foramen lymph nodes with myocutaneous flap reconstruction of the tensor fasciae latae and it followed well. After 1 year being treated once a week by wound care, the nurse team referred him to the physiotherapy in February 2010, when he was evaluated for first time. He presented five surgical wounds in the medial region of the left foot and ankle, which were measured with transparent thin film adhesives and sterile and then traced for digitization and area calculation using the ImageJ® software (Fig. 1).

Tracing of the wounds for digitization and measurement using the ImageJ® software.
Four of the wounds were oval <10 cm2 in area and deeper than the fifth wound that was 40 cm2 in area and uniformly shallow. All of them presented pink color, pale, with a little quantity of fibrin around the borders, and there was no odor, secretion, or infection signs, neither necrosis. Around the wounds following was observed: dry skin and depigmented hypochromic stains; moderate edema with no pitting; estimate volume of lower limb (Disc Method): right side = 2,831.44 mL and left = 2,970.70 mL; anesthesia (tactile and thermal); hypoesthesia (pain) in lumbar vertebrae 5/sacral vertebrae 1 (L5/S1) showed by magenta monofilament of 300 gf (Semmes Weinstein Monofilaments); pain score 9 VAS (Visual Analog Scale); deficit of muscular strength for flexion and extension of hallucis; abduction; thigh flexion (grade 3); and dorsiflexion (grade 4) in the left side, limping gait compensated by the quadratus lumborum muscle.
The treatment consisted of the application of the HFG—Skinner® with a frequency of 1,700 Hz, tension of 8 kV in the air and 100% of amplitude (80 mA of maximal intensity). A sparking technique with a saturated electrode was used for 10 min in the larger wound and for 5 min in the other four smaller wounds, two times a week, as seen in Supplementary Video S1 (Supplementary Data are available online at
After the HFG, a simple dressing with oil-based essential fatty acids (Dersani®) was applied by a nurse. Following, the patient was instructed to perform resistance exercises with the left lower limb and gait training. A total of 48 sessions were held in 2010 and improvement was observed in the edema volume (left = 2,863.46 mL), sensitivity (orange monofilament of 10 gf), pain (VAS score 0), muscle strength (grade 4 and 5), gait (reduced compensation), and in the wounds. All of them were more colored, without fibrin, with a good aspect and the wounds 4 and 5 closed. The treatment continued in 2011 with 36 sessions, when the wound 2 closed, the wound 3 reduced and divided itself in two, the wound 1 reduced a little more and all of them maintained good aspects without complications. In 2012–2013, 32 sessions were carried out (only 16 per year) and the wound 3 almost closed in 2012, but in 2013 grew up again, as the wound 1, that grew up in 2012 and reduced again in 2013. The percentage reduction in wound area (cm2) is shown in Table 2 and Fig. 2.
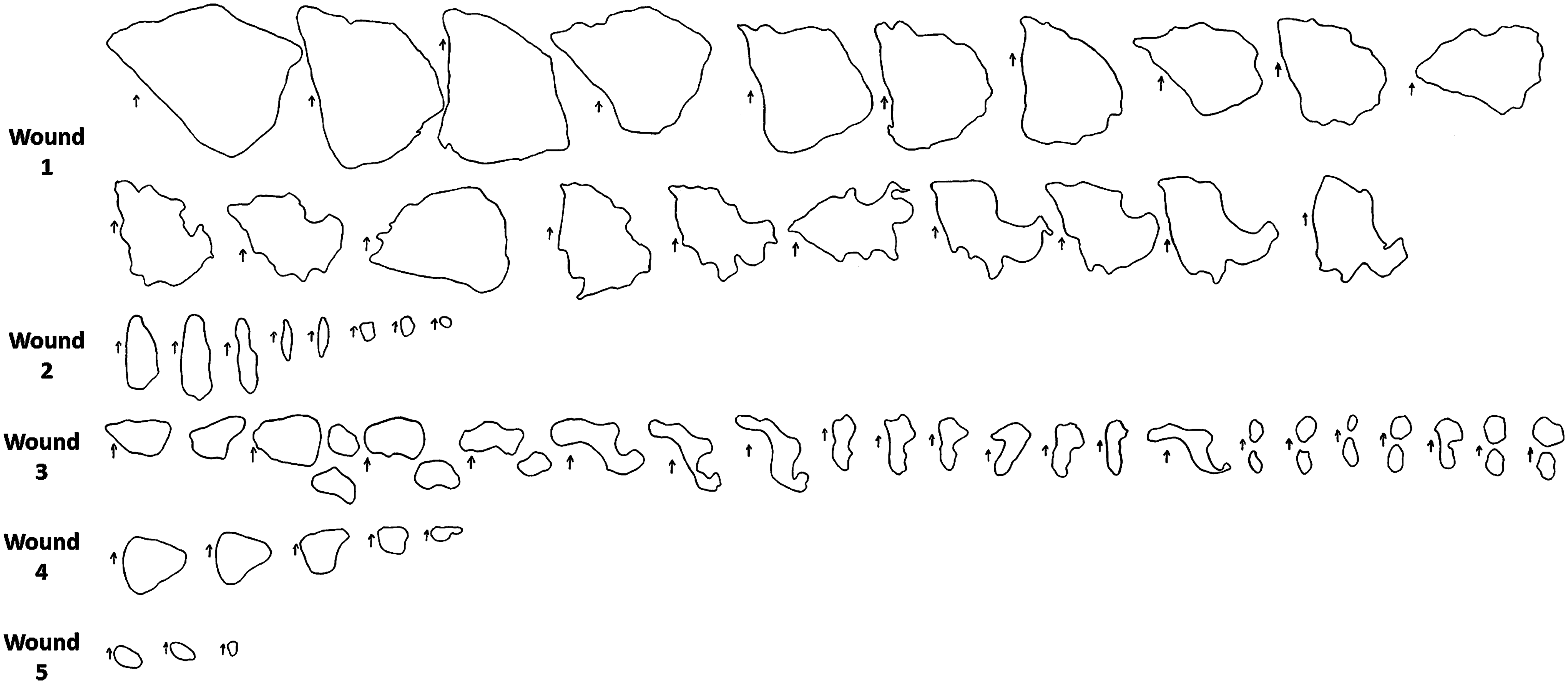
Evolution of the wound areas during the treatment. Wound 5 closed in August 2010; wound 4 in November 2010; and wound 2 in December 2011.
Reduction in the wound area during treatment expressed as percentage (%), year and general mean
The images were obtained only from August 2011, when wounds 4 and 5 had already closed. The conditions of skin and wounds are illustrated in Fig. 3. In December 2013, the patient was discharged from physiotherapy and was referred to being assisted by a wound care team in a public health service near his home. Until this time (December 2013), there was no sign of tumor recurrence or infection.
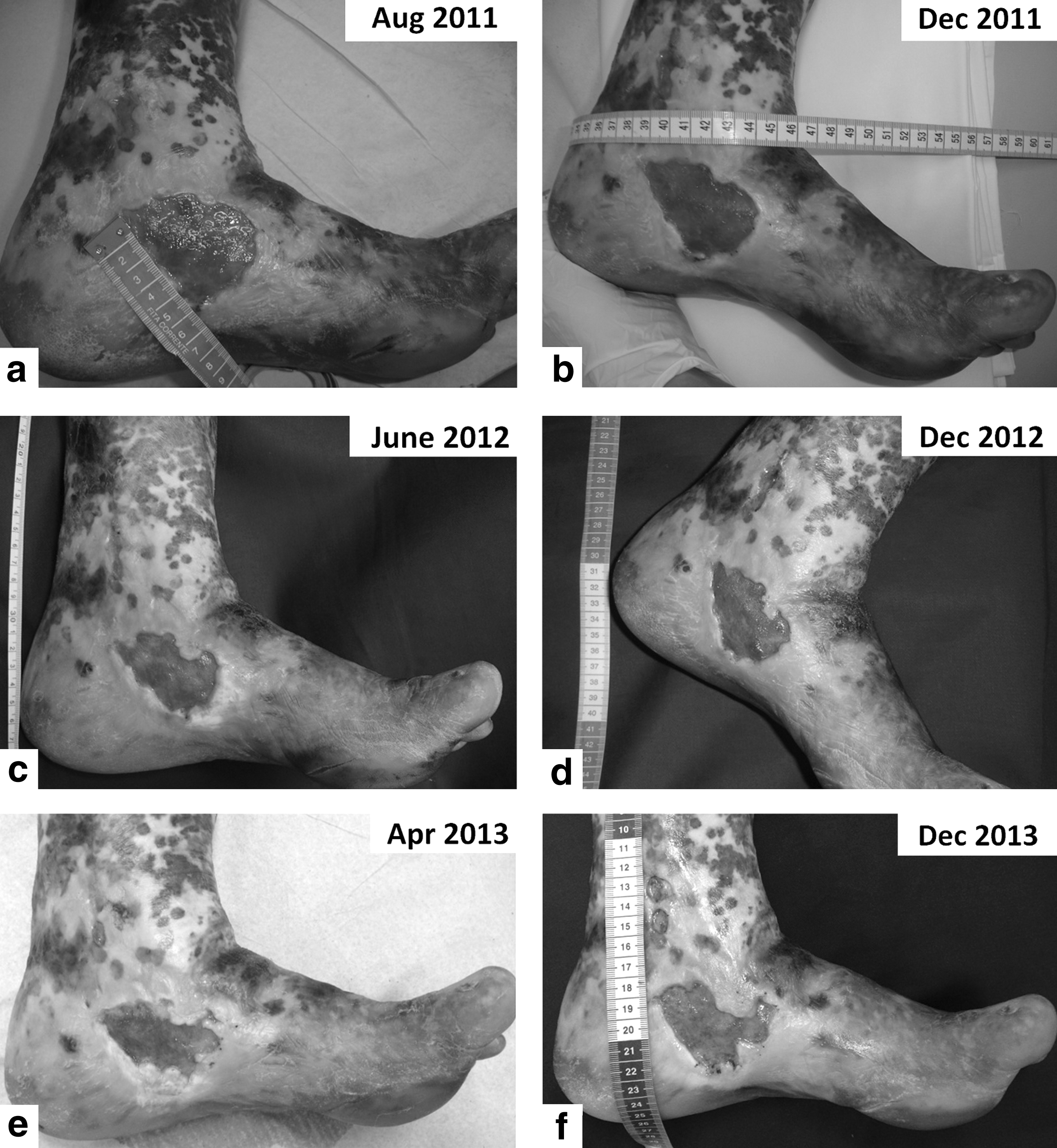
Images show the wounds in
Discussion
MU represents a great challenge due to the impact caused by the complications in postoperative scarring, as described in the case presented. Moreover, a chronic wound may be evolved to recurrence, because of its association with MU. 1,2 With these characteristics wound management is hard and may require more resources such as physiotherapy to manage the patient and wound. 6
HFG uses ozone as mechanism of action, which has germicide, bactericide, and antiseptic properties by stimulating the oxygen metabolism and activating the immune system. 4,6 –8 These effects were considered on the choice of a safe physical agent to apply over the wounds that once already had cancer, 7,9 and furthermore, it helped in tissue repair, wound closure/reduction, and prevention of infections. 4,6 –8
The case report presented had percentage of reduction about 84% considering all wounds, 68% to wound 3 and 56.41% to wound 1, which was similar to Korelo et al. 6 with 68.27%, but in our case a long-term treatment was necessary. This was probably because our patient had a chronic wound even more complicated by previous burn, surgeries, scar tissue, and lymphostatic fibrosis, hindering the development of an appropriate wound healing cascade. Moreover, the best results were seen during the first 18 months of treatment corroborating with Sousa et al. 4 who observed better effects of HFG in all phases of tissue repair when compared to the control group, and only in the initial phase when compared with low-level laser therapy (LLLT). Maybe it would be interesting to apply the HFG during the initial steps of wound healing and then LLLT, but the use of HFG was preferred to avoid tumor growth, as shown with LLLT in the literature. 9
HFG can be used as a promise tool in the tissue repair of surgical wound after MU resection. However, further studies need to be carried out as a double blind randomized controlled trials, using a sham treatment with identical supporting physical therapy and associated treatments, to determine HFG effects and dose response to improve the outcome.
Key Findings
HFG contributes for the healing process of chronic wounds.
A long-term treatment was required and best results were found during the first 18 months.
It is necessary to know more about the HFG on tissues harboring tumor, but in the case presented there was neither tumor recurrence nor infections.
Innovation
HFG contributes on the tissue repair with reductions between 40% and 100% of chronic wounds after MU resection.
Footnotes
Acknowledgments and Funding Sources
The authors would like to acknowledge the nurses and physiotherapy students who worked with us on IBCC between 2010 and 2013. All authors declare that there were no funding sources for this study and they approved the final article.
Author Disclosure and Ghostwriting
The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.