
Abstract
Objective:
A dihydropyridine-type calcium channel blocker, benidipine (BD), is extensively used in hypertension therapy. In vitro study reported BD promoting bone metabolism. We evaluated the effect of sustained release of BD-loaded poly(lactic-co-glycolic acid) (PLGA) microcarriers on the promotion of bone and gingival healing at an extraction socket in vivo. In addition, the effect of BD on osteoblasts, osteocytes, fibroblasts, and epithelial cells was evaluated in vitro.
Approach:
The maxillary first molar of rats was extracted. Next, PLGA microcarriers containing BD were directly injected into the gingivobuccal fold as a single dose. After injection, bone and soft-tissue healing was histologically evaluated. Effect of BD on proliferation, migration, and gene expression of gingival and bone cell was also examined in vitro.
Results:
After tooth extraction, BD significantly augmented bone volume and density, and also epithelial wound healing. During in vitro studies, BD promoted significant proliferation and migration of fibroblasts and epithelial cells. Real-time RT-PCR revealed that BD upregulated messenger RNA expression of Ahsg (alpha 2-HS glycoprotein) and Csf2 (colony-stimulating factor 2) in osteoblasts.
Innovation:
The prevention of bone and soft-tissue reduction associated with tooth extraction has been eagerly anticipated in the field of dentistry. This study first reported the effect of BD on extraction socket healing.
Conclusion:
A single dose of topically administered BD-loaded PLGA microcarriers promoted bone and soft-tissue healing at the extraction site of tooth.
Yasunori Ayukawa, DDS, PhD

Introduction
A
In this study, we focused on these properties of BD and explored the possibility of accelerating the healing of the extraction socket soft and hard tissues. Accordingly, we introduced newly developed sustained-releasable BD-loaded microcarriers and evaluated the effect of single transmucosal injection of BD-loaded microcarriers.
Clinical Problem Addressed
A sufficient volume of alveolar bone is one of the most important factors that determine favorable results in the fields of prosthetic dentistry and dental implantology. In addition, an appropriate volume of soft tissue is essential for dental esthetics. 9 –11 However, alveolar bone volume always decreases to a certain extent after tooth extraction. The consequences of these physical soft- and hard-tissue changes greatly affect clinical outcomes.
A variety of materials, such as autografts, allografts, xenografts, and alloplastic materials, have been applied to extraction sockets to avoid a decrease of bone volume. 12 –17 However, these materials have several disadvantages, and there are currently no gold standard treatment modalities to preserve bone volume.
Platelet-rich plasma or similar blood concentrate has also been used for this purpose without any risk of infection because it can be harvested from the patient's own blood. This concentrate is believed to include several types of growth factors, but it is still insufficient to preserve bone at the extraction socket. 18 –21 Consequently, to eliminate the possibility of extraction socket volume reduction, the development of a novel method to enhance bone regeneration is anticipated.
When using certain drugs and growth factors, an appropriate drug-delivery system (DDS) is important to obtain a clinically successful outcome. For bone formation, a DDS must feature a long-lasting and steady release of the drug.
Materials and Methods
In vivo study
Materials and animals
A total of 100 five-week-old male rats (130–150 g; 80 rats for histomorphometry, 20 for micro-computed tomography [CT]) were used for two experimental (15 or 45 μg/kg of BD) and two control (no administration or poly(lactic-co-glycolic acid) [PLGA] without BD) groups. Each group comprised four subgroups based on the experimental period. Consequently, each subgroup comprised five animals for histomorphometry. Throughout this study, we complied with the ARRIVE guidelines and experiments were carried out in accordance with the National Institutes of Health guide for the care and use of laboratory animals, and the rats were treated according to the guidelines for animal care established by Kyushu University under the approval of the institution's ethical committee (approval no.: A26-223-0).
The microcarriers were prepared using an oil phase consisting of BD (Wako Pure Chemical Industries, Osaka, Japan) in a mixture of PLGA (PLGA-7510; Wako Pure Chemical Industries) dissolved in dichloromethane. The oil phase was cooled and subsequently poured into an aqueous solution of 0.25% polyvinyl alcohol. The oil-in-water emulsion was stirred to aid dichloromethane evaporation. The hardened microcarriers were then filtered using sieves with apertures of 70 μm, rinsed with water, and lyophilized into powder, which was dried under reduced pressure. As a result, 1 mg microcarrier contained 15 μg BD. To observe the microcarriers, they were coated with gold (JEC-550 Twin Coater; JEOL, Tokyo, Japan) and observed with a scanning electron microscope (S-3100; Hitachi High-Technologies, Tokyo, Japan) at 15 kV (Fig. 1a). To confirm sustained-release characteristic, the microcarriers (1 mg) were suspended in 2 mL of simulated body fluid (SBF) 22 at 37°C. An aliquot (70 mL) of SBF supernatant was sampled every 2 days and analyzed by spectrophotometry at 237 nm (Fig. 1b).

Tooth extraction and injection of microcarriers
The maxillary right first molars of the rats were extracted under a combination anesthetic (0.3 mg/kg of medetomidine, 4.0 mg/kg of midazolam, and 5.0 mg/kg of butorphanol). The animals were randomly categorized into the abovementioned four groups. After extraction, 0.1 mL of 150 or 450 μg/mL microcarrier-suspended saline (the final dose of BD was 15 or 45 μg/kg, respectively) was immediately injected into the gingivobuccal fold near the extraction socket. The concentration of BD was defined as follows: according to interview form of Coniel® tablet (bland name of BD), peroral administration of 8 mg of BD (maximum dose of BD for hypertension) resulted in the concentration of a maximum of 4 ng/mL in blood. One milligram of microcarrier released ∼120 ng/mL SBF per month (Fig. 1b) and it was equivalent to 4 ng/mL SBF per day. Thus we decided to use this concentration. In addition, threefold concentration was also used for the test purpose.
On 1, 3, 7, and 28 days after the treatment, the animals were killed by an overdose of pentobarbital sodium and perfusion fixed through the ascending aorta with a 0.9% saline and 4% paraformaldehyde solution (pH 7.4).
Micro-CT
The maxillae were further immersed in the same fixative for 24 h. Next, bone biopsies were examined using a micro-CT scanner (SkyScan 1076; SkyScan, Aartselaar, Belgium). Scanning was performed with an in-lane pixel size and slice thickness of 9 μm. Reconstruction was conducted using built-in SkyScan NRecon program.
Tissue preparation
Specimens were decalcified in 20% tetrasodium ethylenediaminetetraacetate (pH 7.4), dehydrated, and embedded in paraffin. Sectioning was performed parallel to the coronal plane and the tissues were stained with hematoxylin and eosin.
Analysis of epithelial wound healing, connective tissue area, and bone density
Sections representing the central portion of each extraction socket were selected, and images were obtained using a microscope (BZ-9000; Keyence, Osaka, Japan). Epithelial wound healing was evaluated by measuring the distance between the both epithelial edges on days 1, 3, and 7. The connective tissue area and bone density were evaluated on day 28 after tooth extraction (Fig. 1c–e).
Vertical bone height and bone volume
Using micro-CT images, vertical bone height was measured. Among frontal plane slices, a slice that included mesiodistally median slice of corresponding tooth of opposite site was used for the measurement of bone height. Bone height was measured at the buccolingually median position of alveolus. Bone volume was measured at the extraction socket using a built-in numerical analysis software (CTAn; SkyScan) (Fig. 1f, g).
In vitro study
Cell culture
Mouse osteoblast cell line MC3T3-E1 cells (RIKEN BRC Tsukuba, Ibaraki, Japan) were cultured in α-minimum essential medium (α-MEM) containing 100 U/mL penicillin, 100 U/mL streptomycin, and 10% fetal bovine serum (FBS) in a humidified incubator at 37°C and 5% carbon dioxide (CO2). Mouse osteocyte cell line MLO-Y4 cells were cultured on type I collagen-coated plates (0.15 mg/mL, rat tail collagen type I; BD Biosciences, Bedford, MA) with α-MEM (Gibco BRL, Paisley, United Kingdom) supplemented with 2.5% FBS (Gibco BRL), 2.5% iron-supplemented calf serum (HyClone Laboratories, Logan, UT), and antibiotics (100 IU/mL penicillin and 100 g/mL streptomycin; Gibco BRL). 23 The cells were subcultured every 3 days in the presence of 0.25% trypsin.
Mouse fibroblast cell line NIH3T3 cells (RIKEN BRC Tsukuba) were cultured in α-MEM containing 10% FBS. The cells were maintained at 37°C in a humidified atmosphere of 5% CO2 in air. Mouse oral epithelium cell line GE1 cells (RIKEN BRC Tsukuba) were cultured in serum-free medium (SFM-101; Nissui, Tokyo, Japan) supplemented with 1% FBS and epidermal growth factor. The cells were incubated in a humidified atmosphere of 5% CO2 in air at 33°C. The cells were subcultured every 3 days in the presence of 0.25% trypsin.
Cell proliferation assay
MC3T3-E1, MLO-Y4, NIH3T3, and GE1 cells were seeded in 96-well plates (5,000 cells per well) and incubated overnight. BD was dissolved in 0.1% dimethyl sulfoxide (DMSO) at different concentrations (final concentrations of 0.1–10,000 nM) and added to the cell cultures. Cells without BD but with DMSO were used as negative control, and wells without cells were used as blanks. Further incubation for 12 h (NIH3T3 and GE1) or 24 h (MC3T3-E1 and MLO-Y4) was performed. Next, 10 μL of WST-8 reagent (Cell Count Reagent SF; Nacalai Tesque, Kyoto, Japan) was added, and the cells were further incubated for 2 h. Subsequently, the optical density at 450 nm was measured on a microplate spectrophotometer (Infinite M200; Tecan, Salzburg, Austria). The cell proliferation rate was calculated according to the following formula: (ODsample − ODblank)/(ODcontrol − ODblank).
Cell migration assay
Cell migration was measured using a scratch assay. NIH3T3 and GE1 cells were grown to a semiconfluent monolayer in a 35 mm dish. Next, the surface of the dish was scratched using a pipette tip (∼300 μm in diameter of apex). Thus, a cell-free band ∼300 μm in width was created. The cells were incubated and images were captured every 1 h for 12 h using a time-lapsed microscope (BioStation IM; Nikon, Tokyo, Japan) in the presence of BD at doses of 0 and 100 nM. The number of cells migrating into the cell-free band and the distance from the edge were measured.
Real-time PCR assay
MC3T3-E1 cells were seeded at a concentration of 2.5 × 10 4 cells/mL in a 35 mm dish containing α-MEM, 10% FBS, and osteogenic induction supplement containing 10 mmol/L β-glycerophosphate disodium and 0.15 mmol/L ascorbic acid (Sigma, St. Louis, MO). A series of dilutions of BD (final concentration, 100 nM) were added to the culture medium in the 35 mm dish for 7 days. MC3T3-E1 cells treated solely with osteogenic induction supplement were used as a control group.
Quantitative Reverse transcriptase PCR assays were performed using the RT 2 Profiler™ PCR array: mouse osteogenesis (catalogue no.: PAMM-026; Super-Array, Frederick, MD), according to the manufacturer's instructions. The array contained primer sets for 84 osteogenesis-related genes and five housekeeping genes. The starting amount of RNA was 1 μg. PCR was performed using a LightCycler® 96 System (Roche Molecular Systems, Pleasanton, CA) using the following parameters: 1 cycle for 10 min at 95°C, 45 cycles for 15 s at 95°C, and 1 min at 60°C. Data were analyzed using the PCR Array Data Analysis Web Portal.
All quality control parameters, that is, genomic DNA control, reverse transcription control, and positive PCR control, were within the manufacturer's recommended limits for each assay. Results for each assay were normalized to the average of all five housekeeping genes. The average thresholds were compared, and a gene expression change was reported if statistically significant difference between control and BD groups was present.
Statistical analysis
The statistical significance of differences with respect to migration assay, cell proliferation assay, and other data were determined by a one-tailed Student's t-test, one-way analysis of variance with post hoc Dunnett or Tukey test, respectively. Differences were considered significant if p-values were <0.05.
Results
Epithelial wound healing
There were no significant differences in epithelial wound healing among the groups on day 1 (data not given). On day 3, wound closure significantly progressed in the PLGA with BD (PL-BD) 1.0 and 3.0 groups (each administered 1 or 3 mg/kg microcarriers that contained 15 or 45 μg/mL, respectively) compared with the control group (Fig. 2a). On day 7, complete wound closure of the epithelium was observed in all groups (data not given).

Connective tissue area
No significant differences between the groups were observed on day 28 (Fig. 3a).
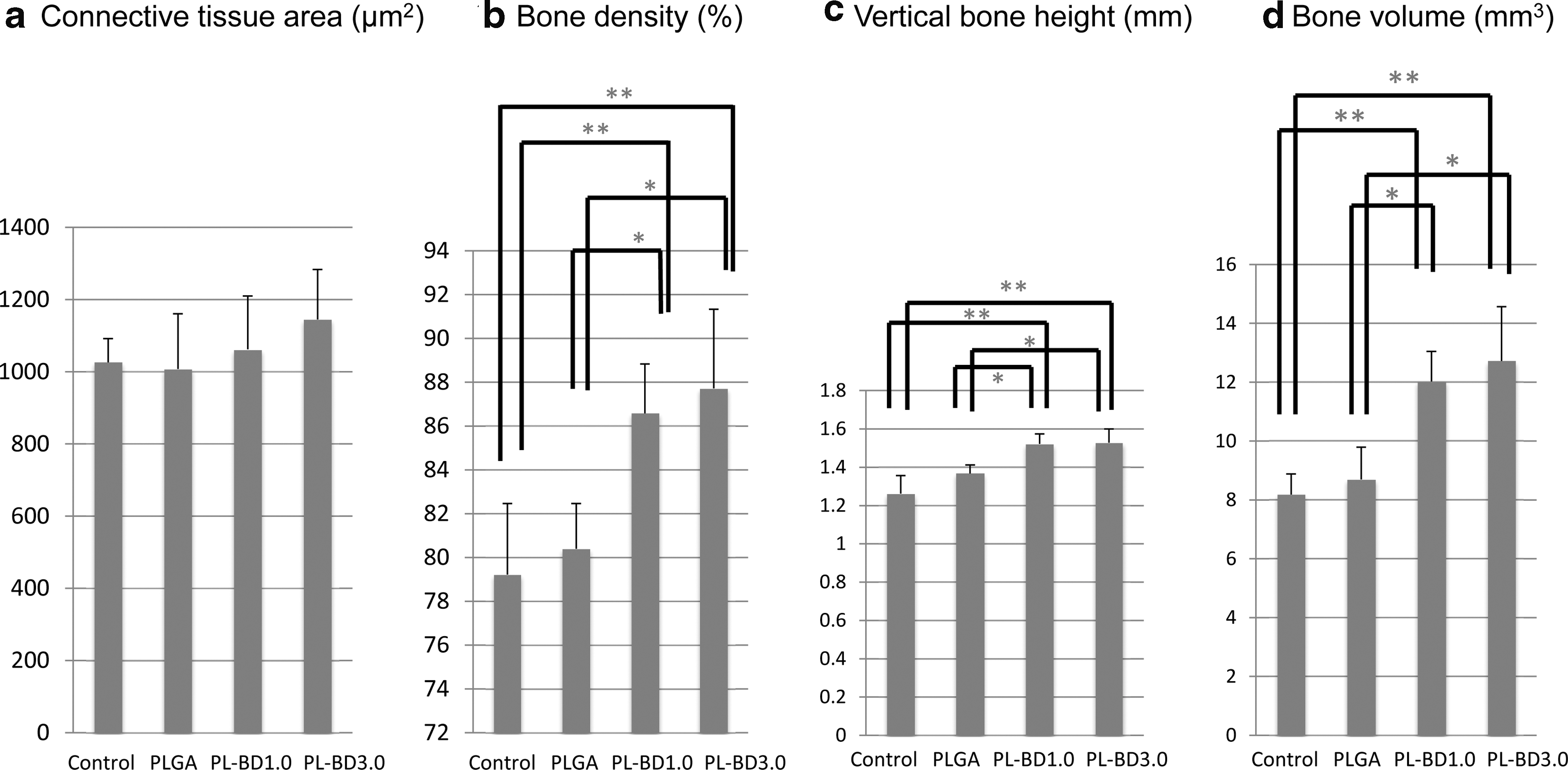
Bone density
On day 28, bone density was significantly larger in both the PL-BD groups than in the control and PLGA groups (Figs. 2b and 3b).
Vertical bone height
On day 28, the vertical bone height value at the extraction socket was significantly larger in the PL-BD 1.0 and 3.0 groups than in the control and PLGA groups (Fig. 3c).
Bone volume
On day 28, bone volume was significantly higher in the PL-BD 1.0 and 3.0 groups than in the control and PLGA groups (Fig. 3d).
Cell proliferation assay
After incubation for 24 h, the proliferation of MC3T3-E1 was significantly promoted by BD at doses of 10, 100, and 1,000 nM. The proliferation of MLO-Y4 was significantly promoted by BD at doses of 0.1, 1, 10, 100, 1,000, and 10,000 nM. After incubation for 12 h, the proliferation of NIH3T3 was significantly promoted by BD at doses of 1, 10, 100, and 1,000 nM. The proliferation of GE1 was significantly promoted by BD at doses of 1, 10, 100, 1,000, and 10,000 nM (Fig. 4a–d).
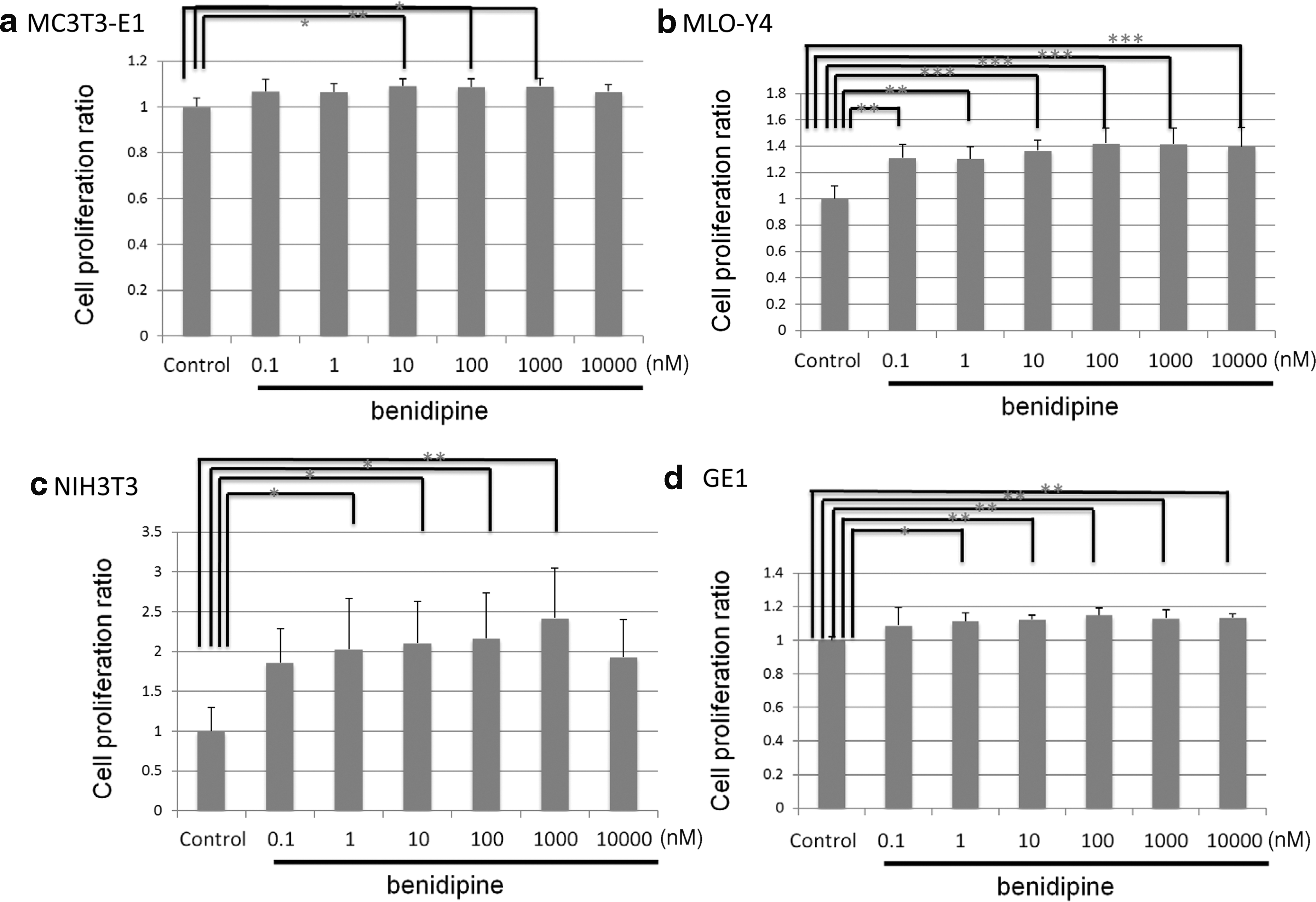
Cell proliferation ratios after incubation for 24 h (MC3T3-E1 and MLO-Y4) or 12 h (NIH3T3 and GE1).
Cell migration assay
The number of NIH3T3 and GE1 cells that migrated into scratch was increased by BD at a dose of 100 nM (Fig. 5a, b).
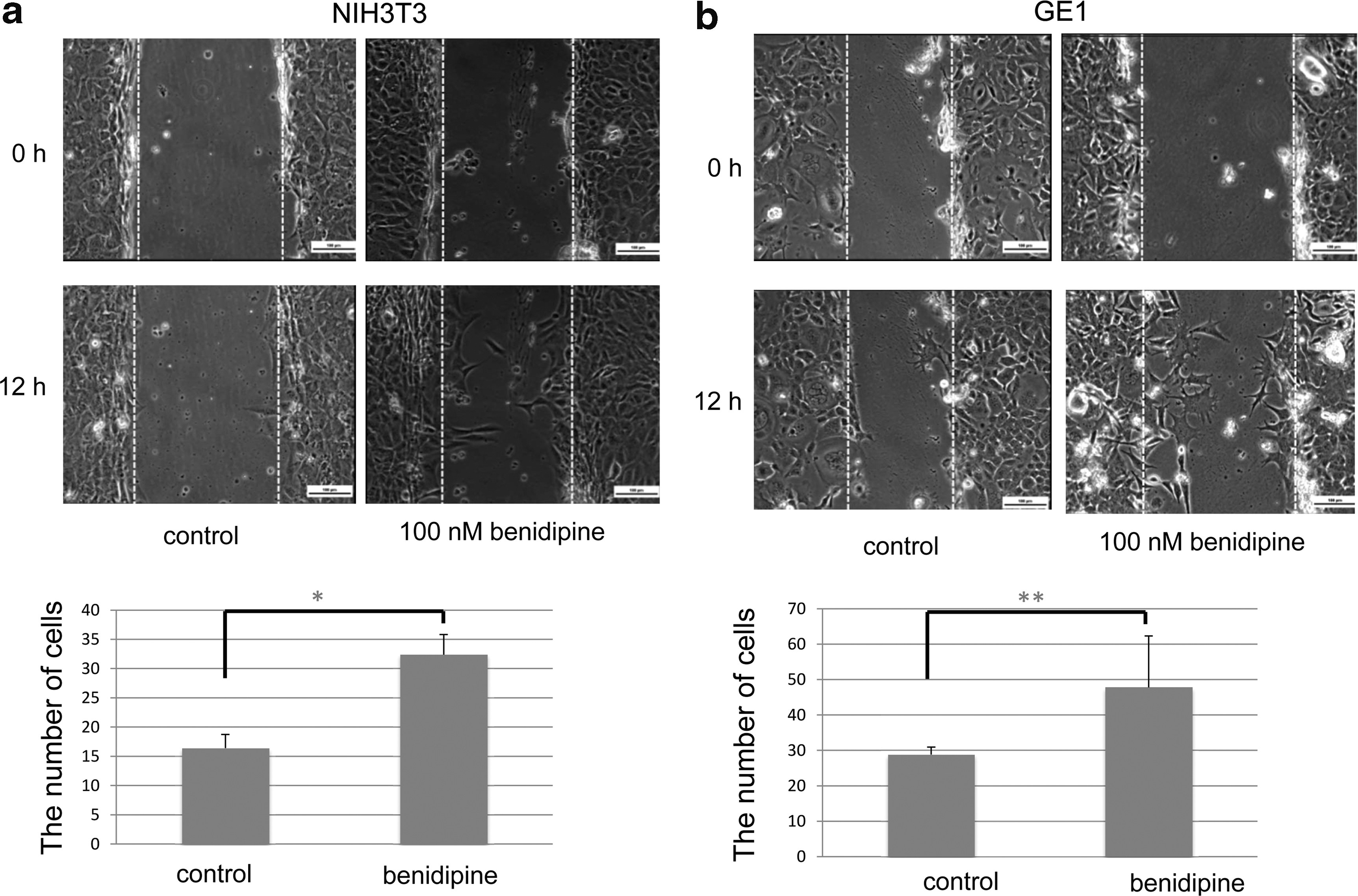
Scratch assay after incubation for 12 h. Both NIH3T3
Real-time PCR
Relative to control, six genes in MC3T3-E1 were significantly upregulated by BD (Table 1).
Expressions of 84 osteogenesis-associated genes
The gene expressions of benidipine-administered MC3T3-E1 were compared with those of the control. Genes whose expression statistically significantly changed are shown. No downregulated genes were indicated (n = 3).
Discussion
The antihypertensive mechanism of BD involves blocking of three kinds of calcium channels. Particularly, blocking of the T-type calcium channel reportedly inhibits the activity of Rho kinase. 24 This study demonstrates that the local administration of BD facilitates epithelial wound healing as early as 3 days after tooth extraction. These findings are persistent with our in vitro findings that the migration and proliferation of NIH3T3 and GE1 cells are accelerated by BD. Cell migration is promoted by inhibiting the Rho-ROCK(rho-associated kinase)-myosin signaling. 25 These findings prove that BD affects the activation of epithelial proliferation and migration and subsequent wound healing after tooth extraction.
In view of calcium channels other than T-type, the blocking of N-type calcium channels, which is also conducted by BD, is known to inhibit adrenergic receptors. 26,27 Both osteoblasts and osteoclasts possess adrenergic receptors, and adrenergic stimulation from sympathetic nerves enhances bone resorption. 28 –30
The region of connective tissue around the extraction socket showed no significant differences between the groups on day 28. Some calcium channel blockers are known to have a side effect of gingival overgrowth by fibroblastic collagen overproduction; however, this finding was not observed in this study. This is consistent with a previous study reporting that BD does not have the side effect of gingival overgrowth. 31
This study demonstrated that 1.0 or 3.0 mg/kg BD-impregnated PLGA microcarriers promote bone density, bone volume, and vertical bone height of the extraction socket. As mentioned previously, BD inhibits Rho-ROCK-myosin signaling. Another ROCK inhibitor, Y-27632, reportedly increases cell movement into bone formation sites, resulting in enhanced osteogenesis. 25 Furthermore, Y-27632 enhances BMP-4 production. 32 With regard to gene expression of MC3T3-E1, six genes were statistically significantly upregulated. Especially, the expression changes of two genes were greater than fourfold. Fetuin, a gene product of Ahsg that is enhanced by BD expression in this study reportedly combines with calcium phosphate to form calciprotein particles and promotes bone mineralization. 33 Similarly, BD upregulates colony-stimulating factor 2 (CSF-2) expression. CSF-2 is known to inhibit differentiation of osteoclast precursors into osteoclasts. 34
Cell proliferation is a key attribute of the bone healing process. In this study, the promotional effect of BD on MC3T3-E1 proliferation is observed. A previous study also demonstrated that BD promoted MC3T3-E1 proliferation at concentrations from 1 × 10−6 to 1 × 10−9 M 6 . The results in this study are consistent with this finding. Similarly, BD promoted MLO-Y4 proliferation. This finding has not been previously reported. Osteoblasts are known to possess L-type calcium channels, and T- type calcium channels are expressed on osteocytes but not osteoblasts. 28 However, other studies reported that T-type calcium channels were expressed in osteoblasts during skeletal development. 29,30 Our results indicate that BD may also act on osteocytes that are abundant in bone tissue.
In this study, a novel drug-delivery microcarrier for sustained release of BD has been developed using PLGA. This is expected to facilitate a long-lasting effect, even with the minimal dose (i.e., single transmucosal injection) at the socket. In our previous studies, an injectable fluvastatin-loaded PLGA microsphere suitable for local injection was developed, which had a long-term effect on bone formation. This DDS has been shown to release fluvastatin at a constant rate for >1 month. 35,36 The method of fabricating microcarriers in this study is referenced in these preceding studies with a modification in the impregnation procedure of drugs into PLGA. This is because fluvastatin is water soluble, but BD is water insoluble. BD in this DDS demonstrates release at an invariable rate for >1 month. Consequently, despite the single injection of BD-impregnated PLGA microcarriers near the extraction socket, accelerated epithelial healing and considerable improvements in bone volume, bone density, and vertical bone height are observed on day 28 in this study.
The limitation of this study is that the results are not necessarily extrapolatable to humans. In addition, some cell lines used for culture study are nongingival or alveolar bone origin that has a possibility to bring misinterpretation. Moreover, BD is usually prescribed for oral dosage. Thus, local injection of BD with a long-lasting effect may give rise to unexpected side effects.
At present, a variety of methods have been used to promote socket healing; however, these methods present problems such as infection, difficulty in surgical skill, or insufficient clinical outcome. Thus, the PLGA and BD microsphere is expected to be a novel potent modality to improve the outcome of socket preservation with its concurrent enhancement characteristics of soft- and hard-tissue healing at the extraction site.
Innovation
Alveolar bone volume always decreased after the teeth extraction. The consequences of these physical soft- and hard-tissue changes greatly affect the clinical outcomes. This animal study demonstrates that a single transmucosal application of PLGA-BD microcarriers promotes healing of both bone and gingiva at the extraction socket. Culture study demonstrates that BD promotes proliferation and migration of bone tissue and oral soft-tissue cells through the enhancement of expression of some genes in osteoblasts that have metabolic effects on bone.
BD promoted bone healing of extraction socket in vivo.
BD upregulated messenger RNA expression of Ahsg and Csf2 in osteoblasts.
BD promoted gingival healing at the extraction socket in vivo.
BD promoted the migration of epithelial cell and fibroblast.
Footnotes
Acknowledgments and Funding Sources
The authors thank Dr. Lynda Bonewald and Dr. Yoichi Kato for the kind gift of MLO-Y4 cells. This work was supported by a KAKENHI Grant (No. JP24249089) to K.K. from the Japan Society for the Promotion of Science.
Author Disclosure and Ghostwriting
All authors declare no competing financial interests exist. The authors listed expressly wrote the content of this article. No ghostwriters were used to write this article.
About the Authors