
Abstract
Significance:
Burns are debilitating, life threatening, and difficult to assess and manage. Recent advances in assessment and management have occurred since a comprehensive review of the care of patients with severe burns was last published, which may influence research and clinical practice.
Recent Advances:
Recent advances have occurred in the understanding of burn pathophysiology, which has led to the identification of potential biomarkers of burn severity, such as protein C. There is new evidence about the potential superiority of natural colloids over crystalloids during fluid resuscitation, and new evidence about components of initial and perioperative management, including an improved understanding of pain following burns.
Critical Issues:
The limitations of the clinical examination highlight the need for imaging and biomarkers to assist in estimations of burn severity. Fluid resuscitation reduces mortality, although there is conjecture over the ideal method. The subsequent perioperative period is associated with significant morbidity and the evidence for preventing and treating pain, infection, and fluid overload while maximizing wound healing potential is described.
Future Directions:
Promising developments are ongoing in imaging technology, histopathology, biomarkers, and wound healing adjuncts such as hyperbaric oxygen therapy, topical negative pressure therapy, stem cell treatments, and skin substitutes. The greatest benefit from further research on management of patients with burns would most likely be derived from the elucidation of optimal fluid resuscitation protocols, pain management protocols, and surgical techniques from randomized controlled trials.
Thomas Charles Lang, MBBS, BAppSc (Phty)

Scope and Significance
Translational Relevance
This work is relevant to scientists involved in immunology, inflammation, circulation or coagulation, medical imaging, as well as researchers involved in the identification of biomarkers or the development of randomized controlled trials (RCTs).
Clinical Relevance
The diagnostic value of current assessment methods and the safety and efficacy of current treatments are critically appraised in light of recent advances. This is directly relevant to clinicians caring for patients with severe burns. In particular, this includes surgeons caring for patients throughout admission, but also is directly relevant to emergency medicine physicians, intensive care physicians, anesthesiologists, pain specialists, internal medicine physicians, pathologists, nurses, and allied health staff.
Background
Burns have been studied for centuries. 7 In 1905, a pioneer of burn management, Haldor Sneve, remarked, “there is no more frightful accident than a severe burn of large area. The intense suffering of the patient, and, in case of recovery, the hideous deformity left, render these accidents peculiarly distressing.” 8 A severe burn is an acute wound caused by local thermal exposures that leads to life-threatening systemic effects. 9 The management of acute wounds resulting from radiation, friction, electrical currents, and caustic chemicals are dealt with elsewhere. The destruction of healthy skin (as shown in Figs. 1 –3) is characterized by coagulation and denaturing of proteins. 10 A severe burn wound differs from other acute wounds by the nature of its size, heterogeneity of depth, its dynamic nature, and systemic effects.

Severe burns. The patient is a 52-year-old male with 33% TBSA flame burns to the back, chest, abdomen, lower limbs, and hands, which were predominantly partial thickness. These photos were taken on admission to hospital. He received a mean daily intravenous fluid volume of 3.3 L over the first 72 h, underwent three procedures for excision and grafting, and remained in hospital for 14 days with a length of stay in ICU of 6 days. ICU, intensive care unit; TBSA, total body surface area.

Severe burns. The patient is a 61-year-old female with 12% TBSA flame burns to the back and upper arm, which were predominantly partial thickness. The upper two photos were taken on admission. The burns on the upper arm were excised and grafted the day after admission and again a week later. The lower two photos were taken 2 weeks after admission. She underwent three excision and grafting procedures, and remained in hospital for 21 days, two of which were spent in ICU.

Severe burns. The patient is a 20-year-old male with 18% TBSA superficial partial-thickness burns, primarily to the lower limbs. The circumferential burns were initially managed with fasciotomies and this photograph was taken on day 3 of admission. He underwent three excision and grafting procedures and remained in hospital for 10 days.
To illustrate the issue of size of the wound, a burn affecting 80% of the total body surface area (TBSA) means loss of ∼1.5 m2 of healthy epidermis and dermis. A given burn will be heterogenous with regard to the depth of the burn, and the depth of a burn can progress over time even after the initial insult has occurred. This process is called burn conversion. 11 Human epidermis is 0.1–1 mm thick and the dermis is 1–4 mm thick, depending on the region involved. 12 Loss of both dermis and epidermis leads to poor healing outcomes, and determines management. 11 Therefore, there is interest in determining burn depth with great accuracy. 12 Burns can be conceptualized by concentric zones 10 : coagulation is at the center, where skin tissue is destroyed, the zone of stasis surrounds this (where skin perfusion is reduced) and the zone of hyperemia surrounds this (where skin perfusion is increased). A burn may theoretically progress bidirectionally through these zones. 10 Finally, a burn causes widespread systemic effects. These effects will be discussed in detail in this review. Recent reviews on burns have focused on intensive care-related wound management, 13 the metabolic response, 14 hypertrophic scarring, 15 smoke inhalation, 16 anesthetic and hemodynamic considerations, 17 and developments in surgical techniques 18 ; however, to our knowledge, this is the first review in recent years encompassing surgical, perioperative, anesthetic, and intensive care management.
Discussion: Critical Updates
Burn Pathophysiology
Excessive inflammation
Patients with severe burns enter a state of “burn shock,” which is characterized by poor tissue perfusion from profound capillary leakage, insidious coagulopathy, and widespread release of inflammatory mediators. 19 Excessive inflammation is now well described following a burn injury, 20 and this process is outlined in Fig. 4.
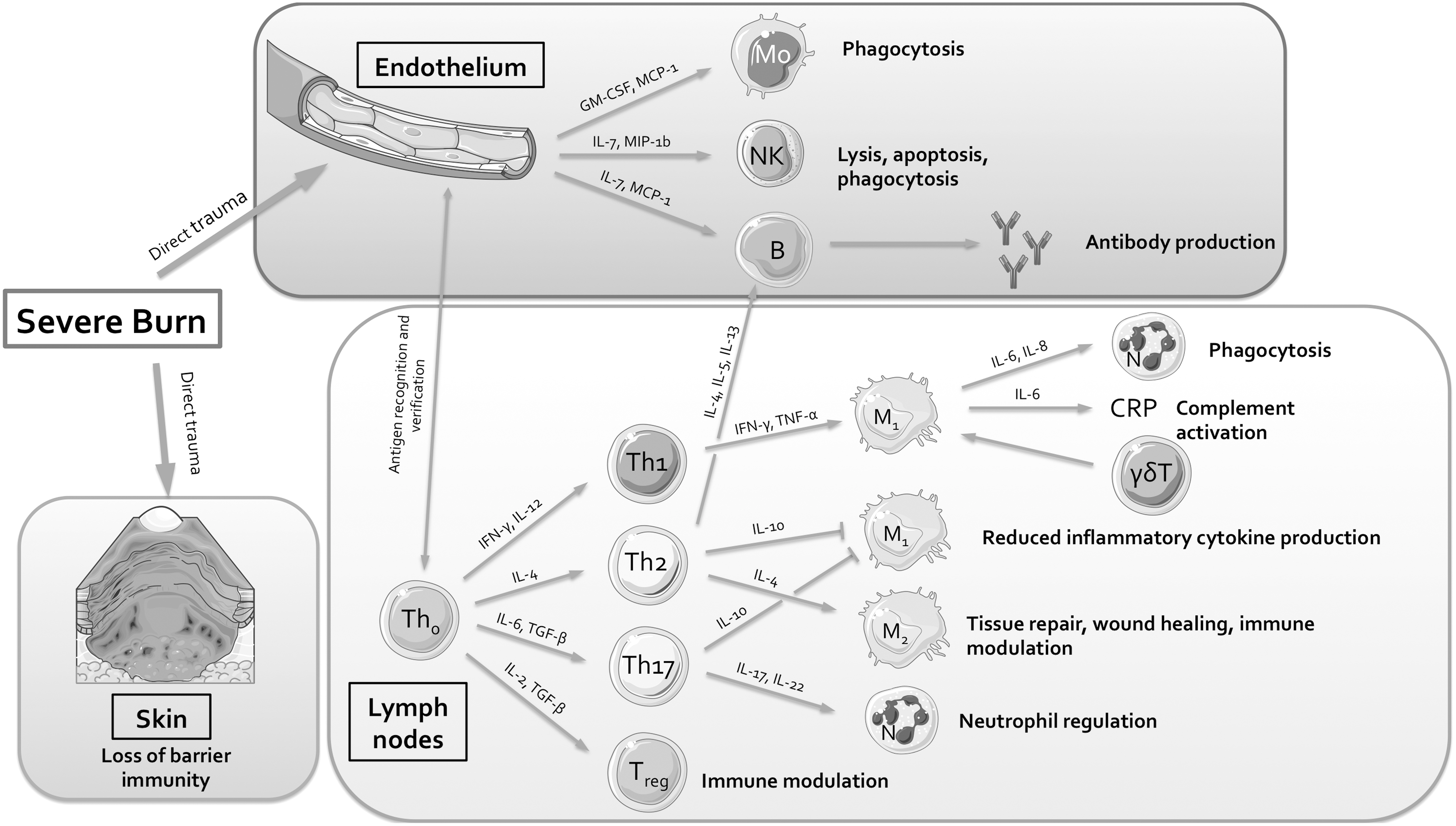
The immune response in severe burns. The immune response to a severe burn is widespread, poorly regulated, and prolonged. It is affected by massive fluid shifts due to increased vascular permeability as well as hemoconcentration and dysfunction of the coagulation system (not shown), which is closely linked to inflammatory dysfunction. Significant tissue injury causes the release of cytokines and chemokines from the endothelium, which activates proinflammatory effector cells to the site of injury. There is also upregulation and differentiation of T cells in the thymus, lymph nodes, and other locations, such as the skin. These T cells release a variety of chemokines and cytokines to draw effector cells to the site of injury, some of which are proinflammatory, and some of which are anti-inflammatory. All of the components in the diagram have been measured in animals or patients with severe burns or systemic inflammation, and excessive or suppressed activity levels of some of these components are associated with poor outcomes following a burn injury (please see Excessive inflammation for more details). γδ T cells, gamma delta T cells; B, B cell; CRP, C-reactive protein; GM-CSF, granulocyte–macrophage colony-stimulating factor; IFN-γ, interferon gamma; IL, interleukin; M, macrophage (M1 and M2 are subtypes of macrophage); MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1 beta (also known as chemokine [C-C motif] ligand 4); Mo, monocyte; N, neutrophil; NK cell, natural killer cell; TGFβ, transforming growth factor beta; Th, T-helper cell (Th0, Th1, Th2, and Th17 are T-helper cell subtypes); TNF-α, tumor necrosis factor alpha; Treg, regulatory T cell. Figure was produced using Servier Medical Art.
Important components of the immune response have been elucidated. Immune cells, such as antigen-presenting cells, and components of adaptive immunity, such as T-helper (Th)-1, Th-2, Th-17, and cytotoxic T cells are activated and release cytokines to attract effector cells, such as granulocytes, to the burn. 21 –24 Immediately following major trauma and burns, the Th-1 response is attenuated, and the Th-2 and Th-17 responses are dramatically enhanced 25,26 and this leads initially to a state of immunosuppression. 27 Granulocytes need to differentiate into neutrophils after suitable signaling to induce phagocytosis and to release web-like neutrophil extracellular traps (NETs). In a process called NETosis, NETs pick up cell debris with cell-free DNA 28 and place cell-free DNA between cells to amplify inflammatory signals and localize chemokines to the site of injury. 29 Highlighting the clinical relevance of NETosis, one recent study showed that neutrophil dysfunction, immature granulocyte count, and cell-free DNA levels strongly predict sepsis in burns. 28 Along with necrosis and apoptosis, NETosis is an important process in the acute wound healing response. 30
Gamma delta T cells (γδ T cells) also play an important role in the immune response to burn injury. 31 γδ T cells modulate the inflammatory response, so their presence is likely to be beneficial following a burn, although it is unclear precisely how this process occurs. 32 These cells are a unique innate immune system surveillance cell that exist within the skin and gut. 33 They display increased toll-like receptor (TLR) reactivity following a burn. 34 TLRs recognize pathogen-associated molecular patterns (PAMPs) from bacteria and damage-associated molecular patterns (DAMPs) from dead cells. They prime macrophages to produce proinflammatory cytokines, such as tumor necrosis factor alpha (TNF-α) and interleukin (IL)-6. 31
TNF-α, which is secreted primarily by macrophages and Th-1 cells, is a proinflammatory cytokine central to the systemic inflammatory response syndrome and sepsis and is elevated in patients with burn injuries, 22 with higher levels associated with the development of sepsis 35 and lower levels associated with improved survival. 36 IL-6 is also a proinflammatory cytokine that modulates the acute phase of inflammation and is elevated in patients with burns particularly in the first week after a burn. 37 C-reactive protein (CRP) is activated by IL-6 and has been used clinically as a marker of inflammation but fails to predict both severe infection and sepsis in severe burns. 38
IL-8 is a chemokine that attracts neutrophils and granulocytes to the burn site. It peaks shortly after a burn injury. 39 Among burns patients who are mechanically ventilated, an elevated IL-8 level on days 0, 3, and 7 predicts death and ventilator-associated pneumonia 23 and among patients with large, severe burns requiring surgical intervention, IL-8 levels are significantly higher in nonsurvivors. 40 Similarly, levels of granulocyte/macrophage colony-stimulating factor (GM-CSF), and monocyte chemoattractant protein (MCP)-1 are higher among nonsurvivors of severe burns. 40 Levels of other inflammatory cytokines that are elevated in the first week after a severe burn include: IL-4, 40 IL-2, IL-5, IL-7, IL-12 and its active form p70, IL-13, IL-17, interferon-γ (IFN-γ), macrophage inflammatory protein 1β, 37 and the inhibitory cytokine receptor IL-1 receptor antagonist. 41
Enzymes, such as matrix metalloproteinase (MMP)-8 and MMP-9, are released from neutrophils in early inflammation in response to increased levels of GM-CSF, IL-8, and TNF-α. 42 MMPs break down the extracellular matrix and basement membrane in acute inflammation to contribute to vascular permeability 43 and are inhibited by tissue inhibitor of metalloproteinases (TIMP)-1. 44 Circulating levels of TIMP-1 are maximal 2 days after a severe burn, 45 are significantly higher in burns of >20% TBSA compared with burns <20% TBSA, and are significantly higher in patients who do not survive to 90 days after severe burn. 46 Levels of plasma gelsolin, an intracellular actin-severing protein that stabilizes mitochondria to inhibit apoptosis, predict mortality at 28 days to a similar extent to the acute physiology and chronic health evaluation (APACHE) II score. 47
Hypermetabolism
Patients with large burns have a significantly increased metabolic rate. This increase occurs in conjunction with the acute inflammatory response to injury, contributes to mortality, and persists for up to 3 years. 48 Metabolic changes are seen primarily in the mitochondria in adipose tissue. After a severe burn, adipose tissue turns from white to beige and has increased amounts of mitochondria that are positive for uncoupling protein-1 (UCP-1). UCP-1 causes uncoupled mitochondrial respiration. This is characterized by inner mitochondrial membrane proton conductance that proceeds without the presence of adenosine triphosphate (ATP) synthase. Uncoupling is identified by mitochondrial heat production and alters the metabolic function of adipose tissue from the storage of energy to the expenditure of energy. 49,50
Skeletal muscle also undergoes changes. Skeletal muscle oxygen consumption increases from 64 to 130 mL/min after a burn of 50% TBSA. 51 This is thought to be explained by increased ATP production 52 and mitochondrial dysfunction characterized by the presence of UCP-2 (which acts similarly to UCP-1). 53 Increases are also seen in ATP-consuming reactions required for protein synthesis, gluconeogenesis, and cycling of fatty acids. 54
A burn injury also leads to central (hepatic) and peripheral (skeletal muscle) insulin resistance 55 probably due to a postreceptor defect involving the glycogen synthesis pathways. 56 Insulin resistance elevates circulating glucose levels. High glucose levels promote an aggressive hyperinflammatory phenotype of macrophages 57 and natural killer cells 58 and the mean amplitude of glycemic excursion over the first 72 h is an independent predictor of mortality. 59
Coagulopathy
There is evidence of a link between inflammation and coagulation following burn injury. Using proteomic methods in patients with severe burns, investigators showed that a broad range of proteins involved in both inflammation and coagulation were significantly different between survivors and matched nonsurvivors (mortality in this study was defined as death from any cause and the mean time to mortality was 32 ± 19 days). For example, coagulation factor XIII, B polypeptide, and an antithrombin III variant (IPI00032179.2) were lower in nonsurvivors. This study also highlighted the relationship between nonsurvival and coagulation proteins, adhesion molecules (such as VCAM-1), inflammatory markers (such as TIMP-1, GM-CSF, IL-4, IL-8, and MCP-1), metabolic markers (such as retinol-binding protein 4, sex hormone-binding globulin, CD-14, glycosylphosphatidylinositol-specific phospholipase D1, and proplatelet basic protein), and acute-phase reactants (such as IL-4, IL-8, and CCL2) following a severe burn. 40
Low levels of the anticoagulant antithrombin III negatively correlate with increasing age and burn size, 60 and reduced levels of the anticoagulants protein C (PC), protein S, and antithrombin are associated with an increased risk of mortality. 61 PC is a protease synthesized by the liver, 62 vascular endothelial cells, and epidermal keratinocytes, 63 which circulates in plasma as a zymogen of activated protein C (APC). 62 In addition to its well-described anticoagulant function, which is to inhibit factor VIIIa and Va, 62 APC exerts potent anti-inflammatory and cytoprotective functions. 62 Following tissue injury, APC modulates the inflammatory response through intracellular signaling mechanisms, 62,64,65 and in wounds it promotes controlled angiogenesis, 66 –69 and stimulates re-epithelialization. 70 –72 This assists with the natural growth of well-vascularized granulation tissue from the base of the wound. It also facilitates cytoprotection through prevention of apoptosis and reduced inflammatory cell migration, which stabilizes the local cellular environment thus allowing and promoting the subsequent rapid growth of healthy new epithelium. 69,73
PC levels are an independent predictor of the presence of a chronic wound in diabetic patients, to a greater extent than percentage of glycated circulating hemoglobin (HbA1c%) or CRP levels. 66 PC levels are low in burns patients, ranging from 34% to 130% compared with the normal range of 70–180%. 74 In sheep, PC levels decrease over the first 24 h after a burn 75 and in an observational cohort study, we have recently shown that after a severe burn, PC levels are low and increase steadily over 6 days and then remain steady. This study showed that low PC levels are associated with large burns, deep burns, and poor outcomes, such as mortality, length of stay (LOS) in intensive care unit, number of surgeries, and a high volume of fluid resuscitation. 76 This may be explained by excessive inflammation, as TNF-α suppresses PC activation, 77 whereas IL-1 suppresses PC expression, 78 and because both cytokines are increased immediately after a burn 79 the PC system is shut off.
A detailed study of nine patients, including four nonsurvivors, who presented to hospital with severe burns with TBSA 25–95%, was recently published. Investigators measured coagulation factors II, V, VII, VIII, IX, X, and XI; the anticoagulant proteins antithrombin III; PC; and tissue factor pathway inhibitor; the clot formation and fibrinolytic markers plasmin–antiplasmin complex; D-dimer and fibrin monomer; as well as the inflammatory cytokines IL-1β, IL-6, IL-10, IL-12p.70, and TNF-α at regular intervals over the first 96 h of a hospital admission. The only markers with a significant difference between nonsurvivors and survivors on admission were PC activity levels (56% ± 18% for nonsurvivors vs. 82% ± 9% for survivors, p = 0.04) and factor VIII activity levels (518% ± 182% for nonsurvivors vs. 305% ± 148% for survivors, p < 0.05). 79 The proposed functions of the PC system in patients with burns are outlined in Fig. 5.
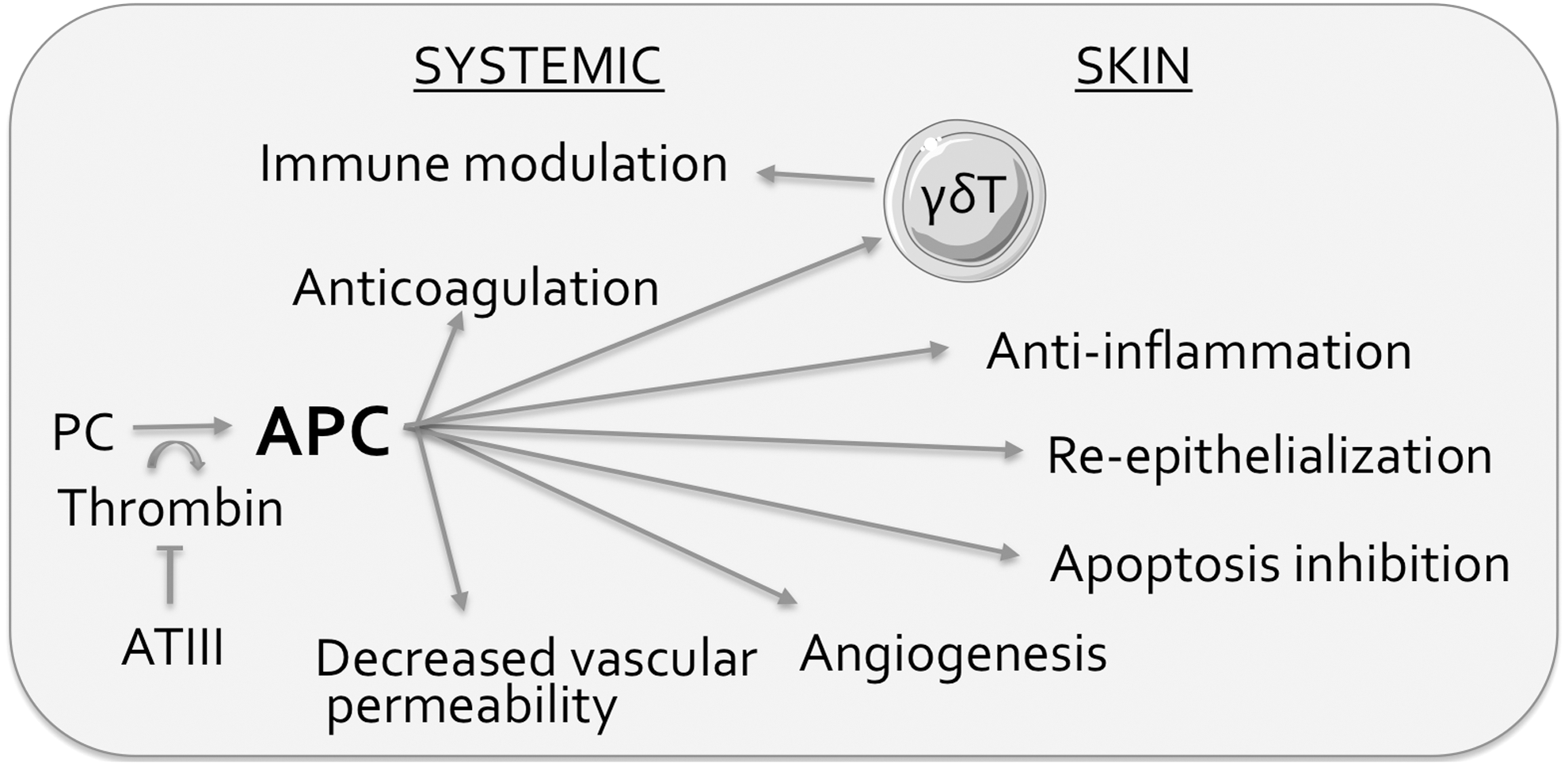
Proposed functions of the PC system in severe burns. PC is attached to the endothelial surface by endothelial PC receptor (not shown) and is cleaved by thrombin in response to tissue injury to produce APC. APC acts at the site of injury to manage the consequences of tissue damage and also has systemic effects on anticoagulation. APC is proposed to influence certain T cell subtypes such as the gamma delta T cell to influence modulation of the inflammatory response. APC, activated protein C; PC, protein C. Figure was produced using Servier Medical Art.
The Clinical Assessment of Patients with Severe Burns
The initial resuscitation of a patient with burns allows rapid identification (and simultaneous treatment) of life-threatening injuries. Protocols vary in terms of resuscitation methodology, but a commonly used method is the Advanced Trauma Life Support algorithm. It is based on hierarchical and sequential management of the airway and cervical spine, ventilation, circulation and prevention of hemorrhage, assessment of neurological status, then identification of other injuries (including the burn) while maintaining normothermia. 80 Following this, the patient undergoes a thorough head-to-toe clinical assessment, the primary purpose of which is to rapidly determine burn severity by visually estimating burn depth and burn size. Burn size is estimated as a proportion of the TBSA affected by the burn and is important in early assessment as it guides the initial intravenous fluid resuscitation rate. Several methods assist this estimation. They include the rule of nines, 81 the rule of palms, 81 the Lund and Browder chart, 82 and other visual aids such as mobile apps. 83
The means of categorizing burn depth varies between centers, but a generally accepted convention is to separate burns into one of three general categories of superficial, partial, or deep burns, with partial-thickness burns further subcategorized into superficial partial and deep partial thickness. 84 Figures 1 –3 show photographs of adults with predominantly superficial partial-thickness burns. Another purpose of the history and physical examination is to identify an inhalational injury. Patients who are suspected of having sustained an inhalational injury to the infraglottic airway or lung parenchyma may then undergo bronchoscopy for visual confirmation of damage to the respiratory epithelium.
Burns surgeons use clinical examination by visual estimation of burn size and depth as the primary method of evaluation in a patient with severe burns, and as the method that determines expected outcomes and therefore management. 85 Although some surgeons consider clinical examination the gold-standard of patient assessment, 86 there is evidence that visual estimations of depth are often inaccurate when compared with histologically determined depth, with expert surgeons unable to determine depth in up to 35% of burns. 87 –89 These methods have been validated but have limitations in reliability and as a result lead to inaccurate estimations, with recent research showing that nonhealth care-trained people are better at estimating burn size than expert surgeons. 90 The primary implication of an unreliable estimation of burn size and depth is that the initial management (which is determined by the clinical examination) may be inappropriate.
Predicting inhalational injury with a purely clinical assessment is also difficult and error prone. Features, such as the presence of carbonaceous sputum, singed hairs, facial burns, and a burn in an enclosed space, were previously thought to provide evidence of an inhalational injury. However, each of these components of the history and physical examination are unreliable markers of inhalational injury when compared with findings on bronchoscopy. 91 Clinicians have therefore labeled the history and physical examination as inappropriate for the diagnosis of inhalational injury. 92 The implications of the history and physical examination as poor markers of inhalational injury include a limited ability to choose which patients require bronchoscopy and therefore detect true inhalational injury. This is important because inhalational injury confirmed by bronchoscopy and stratified by severity according to the Abbreviated Injury Score has been shown to predict inpatient mortality after a burn. 93
Regression models derived from data based on the clinical examination are used to predict clinical outcomes following a burn. Examples of scores derived from these models include the Baux score, 94 the Zawacki score, 95 the Abbreviated Burn Severity Index, 96 Roi's model, 97 and the Unit Burn Standard Index. 97 Among even the best regression models, however, none is properly validated, none provides odds ratios, and none is able to quantify the risk of a given outcome. 98 For example, burn size and patient age are the best predictors of LOS, but even the best models cannot predict this outcome with a high degree of certainty, with the R2 statistic ranging from 0.15 to 0.75 for these models, meaning that between 15% and 75% of the variance in LOS can be predicted using the clinical examination. 98
The visual inspection of the skin and upper airway after a burn has a limited capacity to detect the true nature of a burn injury. Tissue perfusion and necrosis cannot be identified by visual inspection. Therefore, adjuncts are required to accurately assess burn severity.
Adjuncts to the clinical asses sment of patients with burns
Imaging
Laser Doppler imaging (LDI) provides information about regional tissue perfusion. When laser light is directed at perfused skin, circulating red blood cells scatter the light leading to a detectable Doppler shift, and a calculated estimation of blood flow follows. A systematic review and meta-analysis concluded that LDI has good diagnostic abilities (sensitivity 89%, specificity 93%) but that careful clinical assessment should be used alongside LDI for patients with full-thickness burns. A recent RCT showed LDI led to faster decision making about excision and grafting, and had a cost-saving benefit, 99 and a recent study showed that LDI had superior specificity, sensitivity, positive predictive value, and negative predictive value than the clinical examination for estimating burn depth. 100
There is some evidence to support the use of laser speckle imaging (LSI) in very small burns 101 and although it has high specificity to detect deep dermal burns, it has limitations in sensitivity and accuracy. Spatial frequency domain imaging (SFDI) is noninferior to the physical examination in animal studies. 102 Photoacoustic imaging was shown to be superior to LDI in detecting burn depth in animals, 103 although a systematic review recently concluded that LDI is superior to other imaging modalities. 104 Other imaging modalities to assess burn depth include near-infrared spectroscopy, 105 ultrasound, 106 skin quality probes, 107 nuclear magnetic resonance imaging 108 capillary microscopy, orthogonal polarization spectral imaging, reflectance mode confocal microscopy, and polarization-sensitive optical coherence. 109 These modalities require further testing before they are used routinely in the clinical setting.
The use of radiopaque contrast dyes and angiography remains in use but may be superseded by noninvasive imaging. The most commonly used dye is indocyanide green, which emits and absorbs energy within the near-infrared spectrum. The dye is injected intravenously before an imaging device is applied over the affected area of skin. The imaging device detects the presence of the dye within the affected area of skin using videoangiography. An image representing the amount of dye detected by the device can be mapped to create an image similar to that of the LDI to provide a representation of blood flow as a surrogate marker of burn depth. It is a highly accurate method of determining burn depth 110,111 but it is associated with headache, pruritis, urticaria, and diaphoresis. It can only measure very small areas of blood flow (less than that of LDI) and it takes time and skill to set up the apparatus. 109
Skin biopsies
In the setting of laboratory analysis and research, punch biopsies are considered the gold standard of measuring burn depth. A punch biopsy sample is typically stained with Hematoxylin and Eosin (H&E). 112 Other stains are also used. These include Masson's Trichrome stain (which is designed to detect the depth of burn and tissue necrosis), 113 Verhoeff–Van Gieson's stain for elastic fibers, 114 and an anti-vimentin antibody stain (which delineates a zone of necrosis). 115 New evidence suggests that the lactate dehydrogenase (LDH) stain may be a superior alternative to the H&E stain. 112 However, reporting takes several days and fixation causes contraction of some portions of the skin sample and inaccurate estimations of depth. 106 So while remaining useful for research, skin biopsies are not yet clinically useful. 112
Biomarkers
Biomarkers have been defined as “any substance, structure, or process that can be measured in the body or its products and influence or predict the incidence of outcome or disease.” 116 In recent years, significant advances have been made in biomarkers that may be clinically useful in the care of patients with severe burns. Several candidates are listed in Table 1.
Potential biomarkers in severe burns
γδ T cells, gamma delta T cells; CRP, C-reactive protein; GM-CSF, granulocyte–macrophage colony-stimulating factor; IFN-γ, interferon gamma; IL, interleukin; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1 beta (also known as chemokine [C-C motif] ligand 4); MMP, matrix metalloproteinase; Th, T-helper cell (Th0, Th1, Th2, and Th17 are T-helper cell subtypes); TIMP, tissue inhibitor of metalloproteinase; TNF-α, tumor necrosis factor alpha.
The Acute Management of Patients with Severe Burns
Management of inhalational injury
Once confirmed by bronchoscopy, several management options exist to reduce the likelihood of adverse outcomes associated with inhalational injury. There is evidence to support the early and ongoing use of chest physiotherapy, encouragement of coughing, and early ambulation. 16,117 In intubated patients, continuous mechanical ventilation is associated with increased mortality and pneumonia incidence compared with ventilator modes with interrupted flow. These modes can incorporate different frequencies of flow interruption from the ventilator to the patient while maintaining positive airway pressure and are discussed in detail elsewhere. 118,119
Pharmacological management options are better studied. There is evidence to support the use of the mucolytic agent nebulized N-acetylcysteine (NAC), the bronchodilator salbutamol and the anticoagulant nebulized heparin to reduce the duration of mechanical ventilation after inhalational injury. 120 A dosing study showed that 10,000 IU of nebulized heparin per dose improved lung injury scores without influencing coagulation parameters. 121 There is some evidence emerging to suggest that nebulized antithrombin is effective in reducing the incidence of pneumonia after inhalational injury. 122
Intravenous fluid resuscitation
For over 100 years, it has been observed that the early provision of fluid after a burn is associated with reduced mortality. 123 For 40 years the mineral composition and volume of intravascular and interstitial fluid compartments after a burn has been understood. Figure 6 outlines important concepts related to fluid compartments and intravenous fluid resuscitation. Hartmann's solution (a crystalloid solution) mimics the mineral composition of physiological extracellular fluid. A seminal publication by Baxter and Shires described the administration of Hartmann's solution to a series of patients with severe burns and a subsequent reduction in the typical mortality rate. 124 These findings were then adapted to create a formula (the Parkland formula) to guide initial fluid resuscitation volume in the first 24 h. It is typically defined as 4 mL/TBSA burn %/kg body weight. 125,126 Most burn centers utilize the Parkland formula, 125,126 but its use is associated with significant adverse events related to “fluid creep” such as abdominal compartment syndrome and pulmonary edema. 127 –129
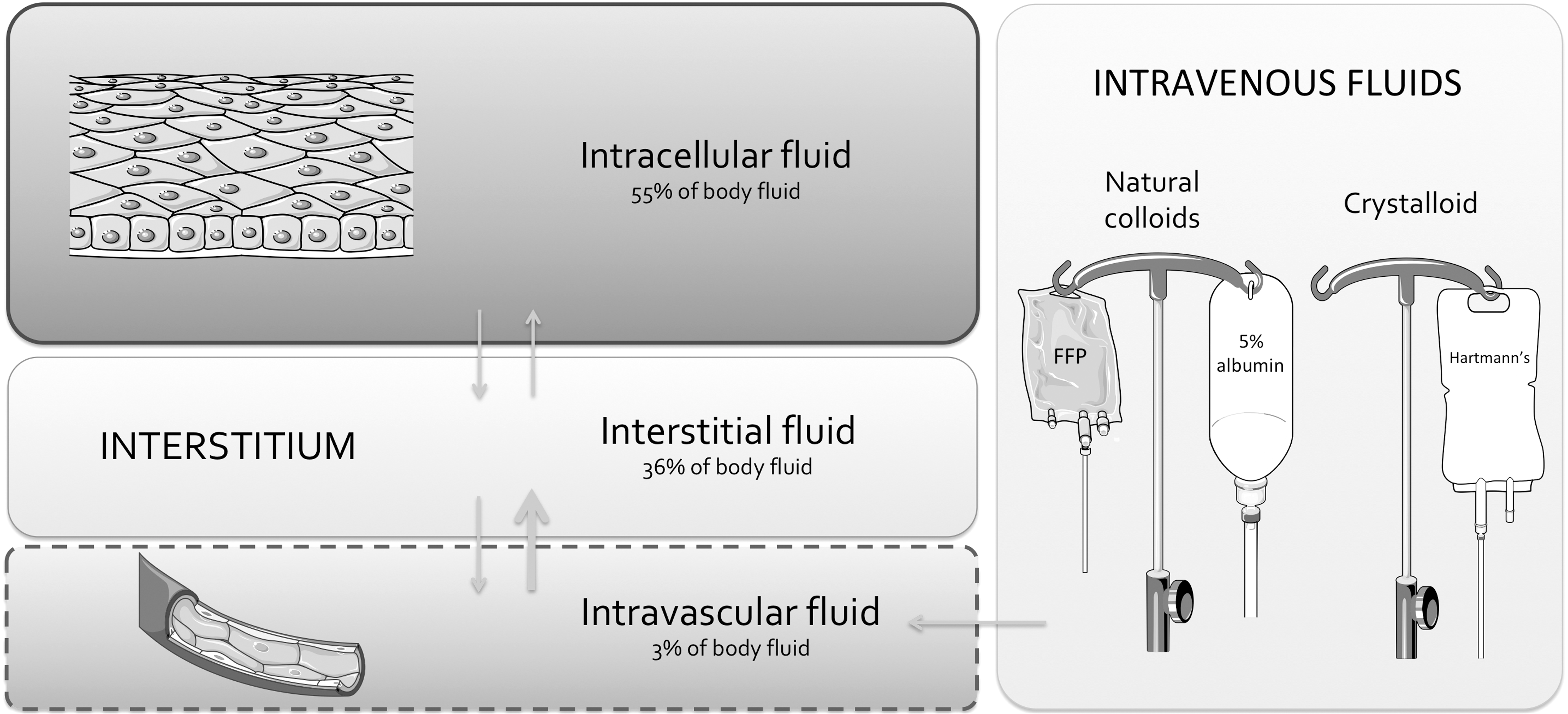
Fluid compartments and intravenous fluid resuscitation in severe burns. The human body is 60% water by weight and contains two virtual fluid compartments: the intracellular compartment and the extracellular compartment. The intracellular compartment holds 55% of body fluid and exists within all 1014 human cells, which make up tissues contained within muscle, skin, and solid organs. Fluid movement between the intracellular compartment and the extracellular compartment is tightly regulated by the semipermeable cell membrane and its ion channels and pumps. The extracellular compartment holds 45% of body fluid and is comprised of the interstitial compartment, and the intravascular compartment, as well as the water of dense connective tissue, bone, and transcellular fluid. Fluid resuscitation of a patient with burns directly affects the volume of the intravascuar, interstitial and the intracellular compartments. The interstitial compartment makes up 80% of the extracellular fluid and exists solely within the space between cells, while the intravascular compartment holds 7.5% of the extracellular fluid and exists solely within the vascular system. Fluid movement between the intravascular and interstitial space occurs through the capillary wall, which has increased permeability after a burn. The main goal of intravenous fluid resuscitation after a burn is to maintain tissue perfusion and this is thought to be achieved by maintaining a full intravascular compartment while avoiding overfilling of the interstitial compartment. Figure was produced using Servier Medical Art.
Other formulae exist, such as the Modified Brooke formula and the Rule of Tens, and they also utilize body weight and burn size to determine the initial volume and rate of Hartmann's solution for resuscitation. 130 The Modified Brooke formula suggests an initial intravenous fluid volume of 2 mL/kg/TBSA burn percent using Hartmann's solution over the first 24 h, followed by a colloid solution at 0.3–0.5 mL/kg/TBSA burn percent over the subsequent 24 h, with glucose in water added to maintain adequate urine output. 131 The Rule of Tens is followed accordingly 132 : burn size in TBSA perccent is estimated to the nearest 10%. To determine the initial fluid rate in mL/h, this number is multiplied by 10, for patients weighing 40–80 kg.
Two U.S. Army publications suggest the use of non-Parkland fluid administration protocols following severe burn in a military casualty. One uses Hartmann's solution according to the Rule of Tens protocol in the first 24 h then 5% albumin in the second 24 h, 133 and another uses the Modified Brooke formula to determine the initial resuscitation volume, and then suggests a switch to 5% albumin after 12 h of Hartmann's solution administration for large burns and after 24 h for small burns. 134 Protocols in hospitals vary similarly. 125 –129
One of the most striking and reproducible findings from recent studies of crystalloid fluid resuscitation in patients with burns, is a clear association between the volume of intravenous crystalloid administered and the incidence of adverse events related to interstitial fluid accumulation. There is a threshold volume of risk, somewhere between 250 135,136 and 300 mL 137 of intravenous crystalloid fluid administration per kg of body weight, particularly over the first 72 h 137,138 that is associated with an increased risk of death, acute respiratory distress syndrome, pneumonia, intra-abdominal hypertension, and abdominal compartment syndrome. 135 –138
The alternative to a crystalloid solution is a colloid solution, and recent evidence shows that some colloids have a lower risk profile than that of crystalloids. Colloids contain macromolecules. In healthy patients, colloids remain within the intravascular compartment to a greater degree and for longer than crystalloids, due to their greater oncotic pressure. 139 The macromolecules in solution can be either natural or synthetic. The natural colloids available to use are albumin and fresh frozen plasma (FFP), while the synthetic macromolecules available are hydroxyethyl starch (HES) and gelatine. HES use is associated with acute kidney injury in critically unwell patients, and although there is no data on its efficacy or safety in patients with burns, it is scarcely used and generally avoided. 140 Similarly, there is no data on the safety and efficacy of gelatine in patients with severe burns. 19
Natural colloids, particularly 5% albumin, have been better studied in patients with burns. In a randomized trial of 42 patients with severe burns, there was no difference in the incidence of multiorgan dysfunction syndrome (MODS) at any time point from days 0 to 14 postburn when comparing the use of Hartmann's solution to the use of Hartmann's solution plus 5% albumin. 141 However, in a retrospective study of 202 patients with severe burns, the use of 5% albumin during resuscitation significantly decreased the risk of mortality. 142 Furthermore, a retrospective study of 159 patients with severe burns showed that, among patients who required high resuscitation volumes (>6 mL/kg/h at 12 h after the burn), the use of 5% albumin was associated with lower mortality, less mechanical ventilation days, lower incidence of ventilator-associated pneumonia and open laparotomy for abdominal compartment syndrome, and better arterial partial pressure of O2:fractional inspired O2 ratios at 24 h when compared with the use of Hartmann's. 143
FFP is used in several resuscitation protocols. One trial compared FFP (administered according to the Slater formula) to Hartmann's solution (administered according to the Parkland formula). Patients who received FFP maintained an ideal urine output with significantly less fluid than patients who received Hartmann's (140 mL/kg/day vs. 260 mL/kg/day, p = 0.005). Significant improvement was seen in patients who received FFP: patients had less weight gain, lower peak intra-abdominal pressures, lower peak inspiratory pressures, and faster and greater base deficit clearance. 144 Another study compared FFP resuscitation to resuscitation with hypertonic saline and Hartmann's solution and found that the FFP group required less fluid in the first 24 h and still maintained the desired urine output yet gained less weight at both 24 and 48 h when compared with the other groups. 145 Another study analyzed FFP-based resuscitation in patients with severe burns and showed decreased overall crystalloid fluid requirements when using FFP. 146 Although there are rare reports of lung injury following FFP transfusion, 147 and FFP is typically more expensive than crystalloids and albumin, 148 a retrospective review of 5 years' experience with FFP-based resuscitation described FFP as safe and effective for fluid resuscitation. 149 Overall, these comparison studies suggest a trend toward a lower risk profile with initial natural colloid use compared with crystalloid use. There is however a lack of data from RCTs of fluid administration in patients with burns. RCTs would be invaluable to help determine best practice in fluid resuscitation following severe burns. 19
Targeted fluid resuscitation
Adequate tissue perfusion is the goal of fluid resuscitation. It can be estimated by measuring cardiac output and blood oxygenation. These measurements can be used as targets to aim for during resuscitation. Patients with severe burns have had improved outcomes since the implementation of physiological targets during fluid resuscitation, 150 but there does not seem to be a clearly superior method of measurement.
Blood oxygenation is measured directly and easily, whereas cardiac output measurement is more complex and indirect. The best and most reliable methods to measure cardiac output are transpulmonary thermodilution (TTD), intrathoracic blood volume index (ITBVI), and lithium dilution cardiac output (LiDCO). 151 –154 Pulmonary arterial catheter (PAC) measurements do not provide superior estimates of cardiac output to these less-invasive methods, 151,152 therefore, PAC is not commonly used. Conversely, TTD, ITBVI, and LiDCO each require a peripheral arterial catheter. TTD and ITBVI involve analysis of a thermodilution curve recorded at the tip of an arterial line after the injection of a cold bolus in the circulation 155,156 and LiDCO involves analysis of the arterial pressure waveform. 154
Urine output (generally targeted at 0.5–1 mL/kg/h) 157 has been used for decades to monitor the response to fluid resuscitation and is a good marker of organ perfusion. It is also not inferior to invasive hemodynamic monitoring methods with respect to patient outcomes, despite its inability to estimate cardiac output. TTD-guided resuscitation is associated with improved survival when compared with the use of hemodynamic parameters, 158 but is not superior to urine output-guided resuscitation: there is no difference seen in mortality, hospital LOS, or central venous pressure. 159 LiDCO-guided resuscitation is associated with lower crystalloid solution administration when compared with urine output-guided resuscitation, 154 but there are no studies of clinical outcomes following LiDCO-guided resuscitation. ITBVI-guided resuscitation is also not superior to urine output-guided resuscitation, with no difference seen in the incidence of MODS at 48 or 72 h postburn. 160
Ascorbic acid
Studies of animal burn models show that intravenous ascorbic acid (vitamin C) infusion decreases capilliary permeability and fluid administration volumes 161,162 and given the morbidity associated with overresuscitation, its use has recently become popular during fluid resuscitation. 163 However, the only blinded RCT on ascorbic acid showed no differences in fluid intake at 24, 48, or 72 h when comparing patients who received ascorbic acid to patients who received the placebo, normal saline. 164 There are also several safety concerns with ascorbic acid. First, it is a potent osmotic diuretic 163,165 and cases of profound hypovolemia have been reported with ascorbic acid infusion. 166 Second, there are cases of nephrotoxicity following high-dose infusions, possibly related to calcium oxalate production. 167 Third, ascorbic acid falsely elevates blood glucose levels. A false hyperglycemia may be erroneously treated and may lead to hypoglycemia. 168
Wound cooling and hypothermia
The skin plays an important role in thermoregulation by regulating blood flow (which leads to modification of radiative and convective heat loss) and by regulating sweat production (which leads to modification of evaporative heat loss). 169 Loss of dermal and epidermal tissue leads directly to impaired thermoregulation after a severe burn 170 and this is highlighted by the positive association between burn size and the incidence of hypothermia. 171,172 Most patients with severe burns arrive to hospital hypothermic (<36.0°C). 171 In nonburn trauma patients, hypothermia is considered part of the “lethal triad” along with coagulopathy and acidosis, 173 and although no such “lethal triad” concept exists in burns management, hypothermia certainly appears to be harmful in burn patients. 171 There is data to suggest that following a burn, hypothermic patients with severe burns have a shorter time to mortality 171 and hypothermic patients with severe burns have a dramatically higher incidence of mortality (60% vs. 3%) when hypothermia is defined as <35°C and normothermia is defined as ≥36°C. 174
One animal study did show a prolongation of survival after inducing hypothermia in 36 rats with 40% TBSA full-thickness burns, 175 but another study of 40 rats with 40% TBSA full-thickness burns did not show an effect on survival after inducing hypothermia. 176 Another study of 28 rats with 20% TBSA burns showed a mortality benefit and wound-healing benefit from directly cooling burn wounds with water 177 and among dogs with burns, cool compresses applied directly to the burned area reduces edema formation, with the optimum temperature of the compress estimated to be 5–17°C. Therefore, in animals, local cooling provides a wound healing benefit, however, targeted hypothermia in humans with severe burns does not seem to show a benefit and may indeed be harmful. Studies of local cooling in humans would be useful to determine any potential risk–benefit profile.
Surgical management
Burn excision
Following resuscitation, patients typically undergo early excision and grafting. Burn excision is the immediate removal of necrotic tissue in the area of the burn to a depth where viable bleeding tissue is identified. Excision is classically performed with a skin graft knife called a dermatome. Tangential excision is excision in repeated parallel slices with a dermatome, in contrast to the use of a scalpel to cut down to subcutaneous tissue. Early excision refers to the timing of tangential excision, which typically occurs within 2 days of injury. 178 Several other methods of excision are in use. The most prominent alternatives to tangential excision are chemical debridement and hydrosurgery. Chemical debridement is performed with a bromelain-based debriding enzyme that is derived from the pineapple plant stem (Nexobrid®; MediWound Ltd.). It is prepared as a powder to be mixed with a gel for direct application to eschar. It removes necrotic tissue without damaging healthy tissue. It is associated with a reduced time to complete debridement, reduced need for surgery, reduced area of burns excised, and reduced need for autografting. 179 Chemical debridement is far less painful than sharp debridement, so a general anesthetic is usually avoided. However, its use is associated with procedural pain therefore local or regional anesthesia and/or pre-emptive analgesia are required. Furthermore, bromelain is inhibited by topical products containing copper and silver so concurrent use of these products should be avoided. 180
Hydrosurgery involves debridement with high-velocity, high-pressure saline directed at necrotic tissues. The best-studied hydrosurgery system is Versajet® (Smith & Nephew) and this has been superseded by a newer model (Versajet II®; Smith & Nephew). Hydrosurgery has become popular for debridement and there is evidence to suggest that in most circumstances, it is as safe and efficacious as sharp debridement for devitalized, soft, necrotic tissue. 181 Drawbacks include poor efficacy in removal of firm leathery tissue and a concern over potential contamination if infectious material is forced into deeper tissues, as well as concern over potential contamination of the operating room environment if infectious material is aerosolized. Hydrosurgery is initially far more costly than traditional sharp excision, although there is some evidence it is more cost effective in the long term. 181
Grafting
Grafting is the harvesting of healthy skin from the patient (autografting) or a cadaver or living donor (allografting). Allografts are usually cadaveric. Animal grafts (xenografts) are typically porcine and often demonstrate acute rejection reactions and therefore are rarely used. 182 The purpose of grafting is to achieve early closure of the burn wound, to provide a cover for the excised wound, and to supply it with epidermal cells to facilitate healing. Harvested skin is most commonly split thickness, although dermatomes can be adjusted to harvest full-thickness skin samples. The graft may be pressed and expanded to cover a large area. For most burns, adequate coverage is achieved with a meshing device that produces mesh-like grafts from the split-thickness skin graft (STSG). This is commonly referred to as the Tanner technique. These devices produce grafts with an expansion ratio between 1:1 and 9:1 of the initial harvested sample. Use of expansion ratios of ≥3:1 are typically used for burns >50% TBSA. 183
Early tangential excision and autografting has been the mainstay of surgical management of patients with severe burns. 184 Early excision and grafting is associated with shorter hospital LOS and less blood loss than patients who undergo delayed excision and grafting. 185 For burns of TBSA <20%, it is associated with shorter LOS and lower hospital costs than silver sulfadiazine (SSD) cream 186 and for burns of TBSA between 20% and 40%, it is associated with a smaller number of wound debridements, less wound infections, and shorter hospital LOS when compared with no early excision and grafting. 187 From animal studies, there does not appear to be a healing benefit from early excision within 2 days of injury compared with delayed excision within 7 days of injury, 188 although scarring is increased with delayed excision 14 days after injury. 189
Very large full-thickness burns (>70–80% TBSA) with limited donor sites may not be suited to traditional STSG and may require the Meek technique to ensure adequate autograft coverage. 190 The Meek technique involves cutting multiple squares of STSG (42 × 42 mm each) into 196 micrografts (3 × 3 mm each). Micrografts are placed on a pleated card that is unfolded to separate the micrografts. These grafts are then placed onto the excised area as individual “islands” that epithelialize and expand, and using this method, large areas of excised skin can be covered with STSG. The Meek technique appears to be a satisfactory method for autografting very large burns. 191 A modification of the Meek technique also uses micrografts but the micrografts are covered by larger ready-to-use allografts. This is sometimes called the micrograft sandwich technique. After 2–3 weeks the allografts are carefully peeled away, leaving the micrografts to continue epithelialization. 192 A modification to the micrograft sandwich technique has been described: after the removal of the allografts, cultured epithelial autografts (CEA) are placed at sites where the micrografts have not fully epithelialized. 193 Retrospective data suggest similar clinical outcomes following the combined use of the micrograft sandwich technique and additional cultured epithelial autografts (M/CEA) when compared with traditional STSG, however, the M/CEA method was superior with regard to a smaller overall donor site and a lower cost of surgery. 193
Autografting, particularly for facial burns, can lead to dissatisfaction about cosmetic results. 194 Patients with very large burns may not be able to provide their own grafts, and therefore require allografts. Improved surgical techniques show promise to improve the issues of both cosmetic dissatisfaction and acute rejection that have been associated with allografting in the past. Vascularized composite allotransplantation (VCA) techniques have led to at least 30 successful hand and face transplants in patients with severe burns. Most patients remain on long-term immunosuppressive drugs after VCA. 195 Although chronic immunosuppression is associated with the risk of infection, no VCA patients have had chronic graft rejection. 194 Newer immunomodulation 196 and immunosuppressive therapies show positive preliminary results. 182,197
Dehydrated human amnion/chorion membrane (dHACM) allografts (EpiFix, AmnioFix, EpiBurn; MiMedx Group, Inc.) have become popular in recent years. These allografts contain natural growth factors, cytokines, and chemokines. They are terminally sterilized and packaged as ready-to-use mesh or sheet dressings, or as a powder that can be mixed in saline for injection. Case reports show evidence that dHACM is a safe and effective graft option for partial- and full-thickness burns to the hands, face, and genitalia, although comparative trials would be useful. 198
Skin substitutes
If early autografting is not feasible, for example if sufficient autograft is not available or not desirable due to the physiological condition of the patient, then temporary covers can be used (e.g., Integra® Dermal Regeneration Template; Integra Life Sciences Corporation, and Matriderm®; MedSkin Solutions Dr. Suwelack AG). Temporary covers are engineered to incorporate the growth of a neodermis and vascular network. They are widely used and allow temporary wound closure to facilitate healing. Integra is used commonly in the United States, and contains inert bovine tendon collagen and glycosaminoglycan scaffolding. The Integra Bilayer Matrix Wound Dressing has an additional removable semipermeable silicone layer. 199 Matriderm is not available in the United States and consists of native collagen scaffolding and elastin and has shown to be useful in facial burns. 200
Other covers are improving in quality and may become methods of permanent skin replacement, potentially avoiding temporary skin replacement and grafting altogether. 201,202 Examples include allogeneic engineered skin substitutes (ESSs), autologous composite cultured skin (CCS) and three-dimensional (3D) bioprinting.
ESSs are premade wound coverings that are made from allogeneic epidermal keratinocytes and dermal fibroblasts attached to collagen–glycosaminoglycan scaffolds. They offer the option of the immediate placement of healthy skin cells onto the wound bed without the need for a general anesthetic but carry a theoretical risk of rejection. Case reports describe excellent wound coverage and incorporation of ESSs by the host as functional skin, with cosmetic and functional results comparable to STSG and no cases of rejection. 203
CCS incorporates autologous cells and is undergoing testing in clinical trials of patients with burns. In this technique, skin biopsies are taken during initial excision to harvest fibroblasts and keratinocytes. Biodegradable polyurethane foam attached to an inert nonbiodegradable membrane is then immediately placed over the excised wound for temporary wound coverage and neodermis growth. The harvested cells are cultured in a bioreactor for 28 days to produce CCS. After 28 days, the membrane is removed and the CCS transplants are placed onto the neodermis. Preliminary results show complete healing with satisfactory cosmetic outcomes. 202 A retrospective analysis showed no significant differences in hospitalization length for patients receiving allogeneic cells from ESS compared with patients with autologous cell techniques. 204
Three-dimensional bioprinting is currently undergoing development for use in humans. One research group has successfully developed an in situ skin bioprinter that can print skin substrates directly to a wound. In one technique, fibroblasts are incorporated into a hydrogel of collagen and fibrinogen. This hydrogel is printed onto the wounds. Then a layer of keratinocytes is printed onto the hydrogel. These layers mimic the dermis and epidermis. Using this technique, full-thickness wounds in mice and pigs achieved complete re-epithelialization in 8 weeks. 205 In another technique, amniotic fluid-derived stem cells and bone marrow-derived mesenchymal stem cells are suspended in a gel containing collagen, fibrin, and thrombin and are printed directly onto the wound. Then a second layer of the same gel is applied. 205 Other groups have developed similar techniques mimicking the two-layer structure of skin, and have been able to print functional sweat glands in mice by using a composite hydrogel based on gelatin and sodium alginate. 206
Perioperative management
Acute pain management
Pain is rated by patients, relatives, and staff as the most distressing part of critical illness. 207 Effective acute pain management not only prevents unnecessary suffering acutely but also reduces the risk of the development of chronic and neuropathic pain 208 primarily by damping the catecholamine-mediated stress response. 209 After a burn, nociceptive Aδ and C neurons within the skin are activated. 210,211 New evidence has shown that following a burn, the transient receptor potential channels transient receptor potential cation channel subfamily V member 1 (TRPV1) and transient receptor potential cation channel subfamily A member 1 (TRPA1; which are on the surface of nociceptive neurons) are activated by lipid agonists to cause nociception and allodynia. 212 The stimulated Aδ and C neurons then synapse in the dorsal horn of the spinal cord to activate cortical pain pathways and this results in conscious perception of pain. 211 This process of nociception is shown in Fig. 7.
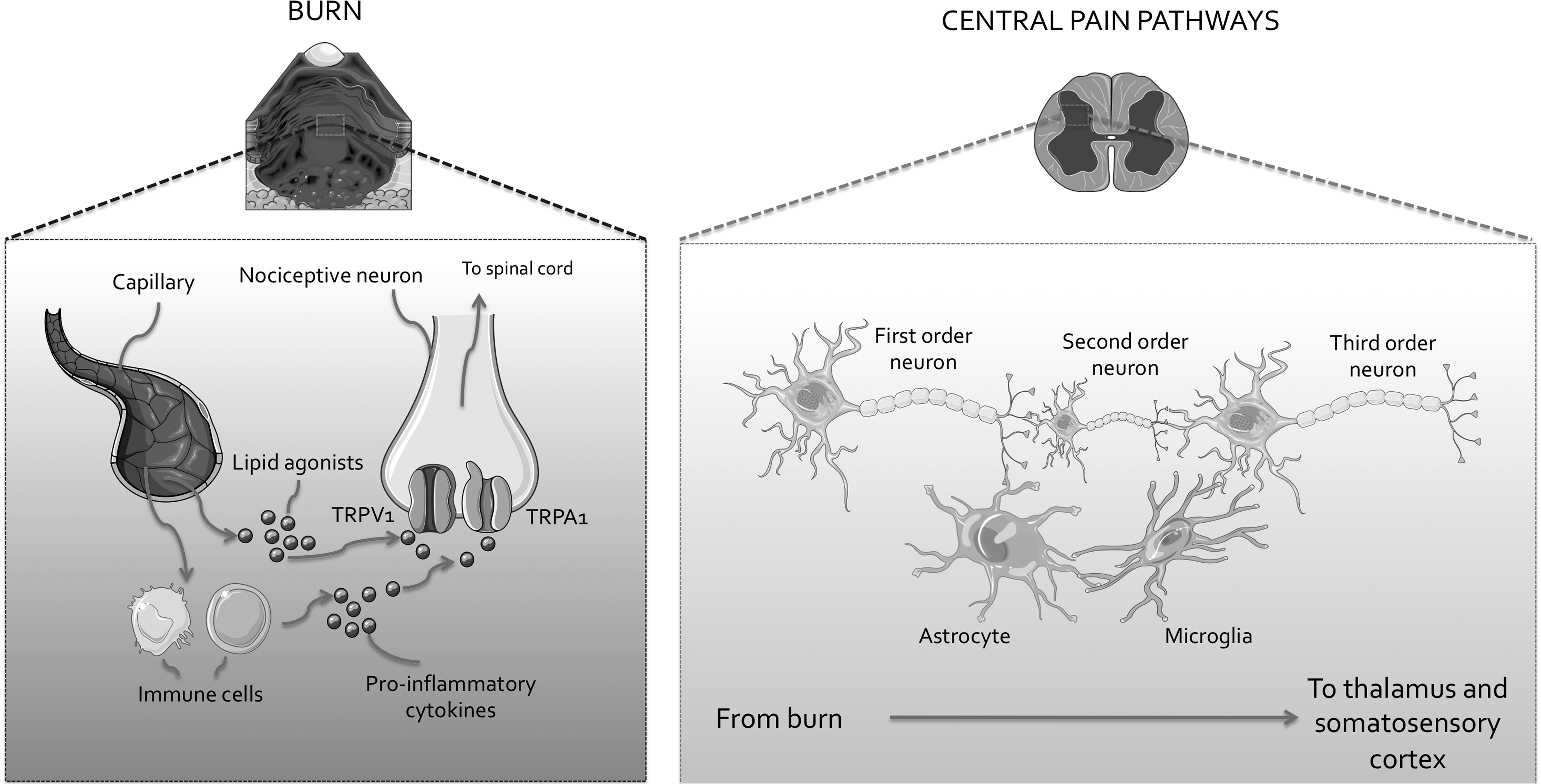
Nociception in severe burns. Local and systemic inflammation characterized by vascular release of lipid agonists and release of cytokines by immune cells cells is associated with activation of TRPV1 and TRPA1 in peripheral nociceptive neurons. These first-order neurons synapse with second-order neurons in the dorsal horn of the spinal cord, which synapse with ascending neurons within the spinothalamic tract. These neurons are sensitized by astrocytes and microglia. The spinothalamic neurons terminate in the thalamus then synapse to neurons which travel to the somatosensory cortex. The transmission of nociceptive stimuli to the cortex is modulated by descending inhibitory neurons (not shown). TRPA1, transient receptor potential cation channel subfamily A member 1; TRPV1, transient receptor potential cation channel subfamily V member 1. Figure was produced using Servier Medical Art.
Assessment of pain severity enables observation of quantifiable changes in pain in response to management. The most well-validated tools for pain quantification in burns are the visual assessment scale (VAS), 213 the burn-specific pain anxiety scale (BSPAS), 214 and if the patient is on a ventilator, the critical care pain observation tool (CPOT). 215 Acute pain severity does not correlate well with burn size or depth, 216 therefore, pain severity should be considered separately from burn severity. Burn pain management should aim to provide background analgesia, and should allow for additional analgesia as required if pain worsens, for dressing changes or after surgical procedures. 217
Opioids are now used far more in burns than previously, and this is independent of patient factors. 218 They provide effective analgesia for severe pain. 219 They should be used with caution as they are associated with side effects, such as sedation (which may be desirable), nausea, constipation, and dependence. 220 Another consideration with their use is that critical illness induces opioid tolerance through multiple proinflammatory mechanisms, including tightening of the P-glycoprotein-controlled blood–brain barrier, increased circulating levels of opioid-binding α-1 glycoprotein, induction of opioid-metabolizing cytochrome P450, increased hyperalgesic opioid metabolite concentrations, increased intraneuronal protein kinase and N-methyl-D-aspartate (NMDA) concentrations, 221 and persistent immune activation of the dorsal horn of the spinal cord by PAMPs and DAMPs released after tissue damage. Some key intracellular changes in opioid tolerance in burns are shown in Fig. 8. These changes lead to significant dose escalation to achieve adequate analgesia. 222 Animal models show that burns directly reduce the antinociceptive effects of opiates 223 and there are reports of increases in pain associated with opioid use in patients with burns, termed hyperalgesia. 224 Some strategies to avoid opioid tolerance and hyperalgesia include limiting sedative infusions, considering neuraxial and non-neuraxial analgesia, rotating opioids, and utilizing multimodal analgesia 222 with evidence to support adding clonidine and ketamine 225 as well as methadone 226 and dexmedetomidine. 157 However, clonidine and dexmedetomidine can precipitate hypotension in the hypovolemic patient, so should be avoided if the patient is hypovolemic. 157
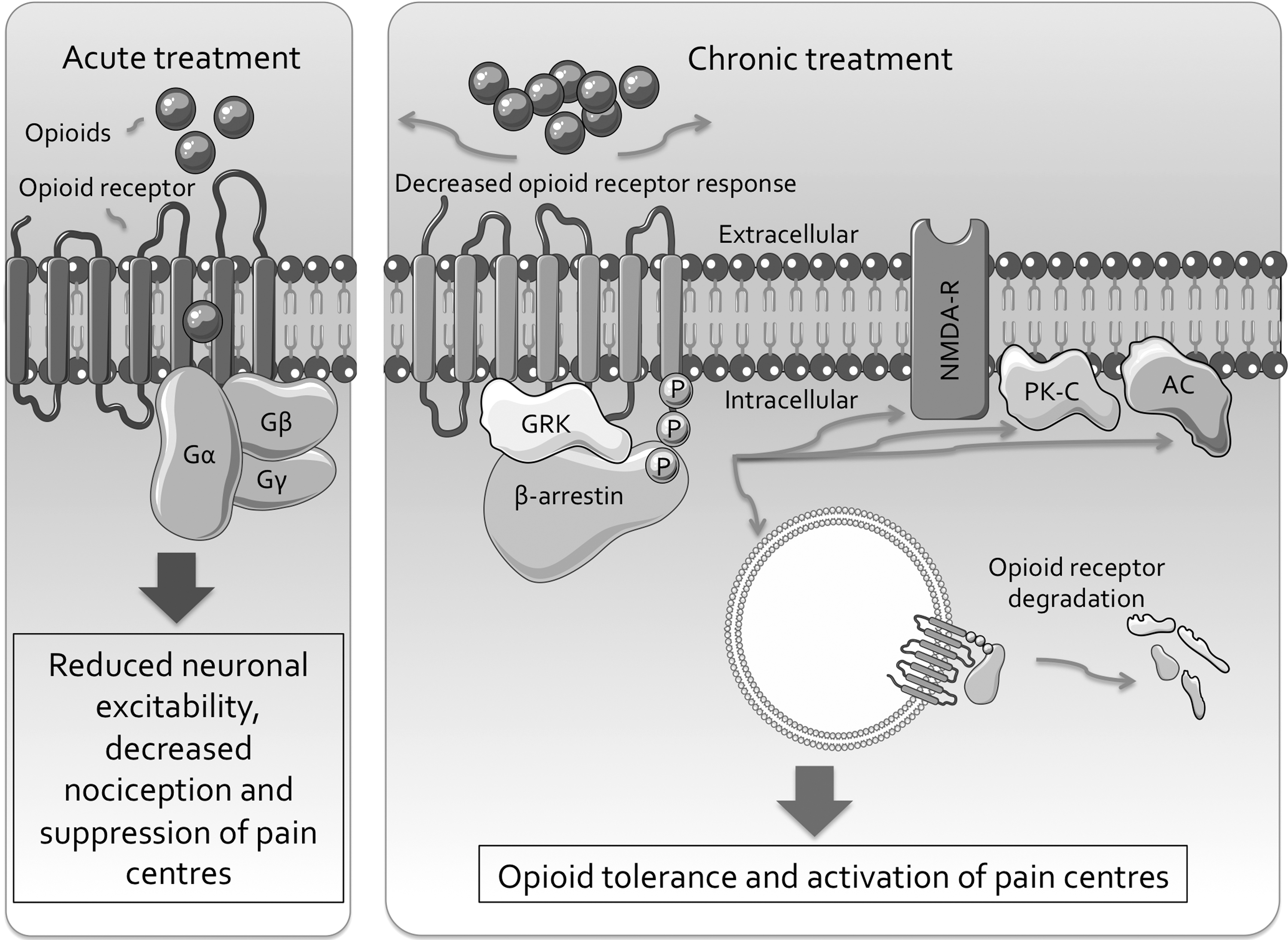
Opioid analgesia, tolerance, and hyperalgesia. During early treatment, opioids such as fentanyl and morphine bind to their opioid receptors in the cell wall of peripheral and central neurons. The opioid receptor is coupled with G proteins, which are composed of Gαβγ subunits. These subunits inhibit calcium channels and activate potassium channels leading to hyperpolarization of the neuronal membrane. The subunits also inhibit downstream AC enzymes, which decreases cyclic adenosine monophosphate levels. In the short term, these events reduce excitability and nociception and result in analgesic effects through decreased activation of the higher pain centers. However, after repeated exposure, particularly to morphine, opioid receptors become a substrate for G-protein–coupled receptor kinase (GRK), which leads to recruitment and binding of β-arrestin protein to the receptor. The opioid receptors are then less responsive to opioids and are degraded, leading to lower numbers of less-responsive opioid receptors, therefore increased doses are required to achieve the same effect on pain. Important intracellular events associated with this phenomenon in patients with burns include increased activity of AC (which increases cyclic adenosine monophosphate levels), increased phosphorylation by protein kinases (PK) and upregulation of N-methyl-D-aspartate (NMDA) receptors. AC, adenylate cyclase. Figure based on an illustration from Martyn et al. 222 Figure produced using Servier Medical Art.
Intravenous opioid patient-controlled analgesia (PCA) shows greater efficacy than intermittent opioid injections with no difference in side effects. 227 Fentanyl and morphine PCA protocols have recently been examined. The optimal fentanyl dose protocol involves a loading dose of 1 μg/kg followed by patient-demand boluses of 30 μg with a lockout time of 5 min. 228 An effective morphine regimen involves no loading dose, patient-demand doses of 1.5 mg with a lockout time of 7 min, and a 24-h maximum dose of 180 mg, with up to three additional 3 mg boluses every 4 h as required and other adjuncts such as midazolam and ketamine when required. 229
For brief breakthrough analgesia during procedures, inhaled methoxyflurane is effective 230 and it provides superior analgesia compared with a midazolam and ketamine PCA during dressing changes. 230 Lidocaine infusion has been used for breakthrough pain but there is minimal evidence to support its use. 231
Paracetamol (acetaminophen), nonsteroidal anti-inflammatory drugs, and cyclo-oxygenase (COX)-2 inhibitors are effective to treat mild pain in patients with burns and exhibit a ceiling effect. 232 However, they reduce opioid requirements and prevent opioid side effects such as nausea, vomiting, and sedation and thus should form part of the usual multimodal analgesia management. 233 They act peripherally by inhibiting COX-2-mediated inflammation and centrally by modulating inflammation through activation of microglia. 234 This is shown in Fig. 9. They are associated with gastrointestinal, and very rarely, renal and cardiovascular side effects 235 so should be used with care.
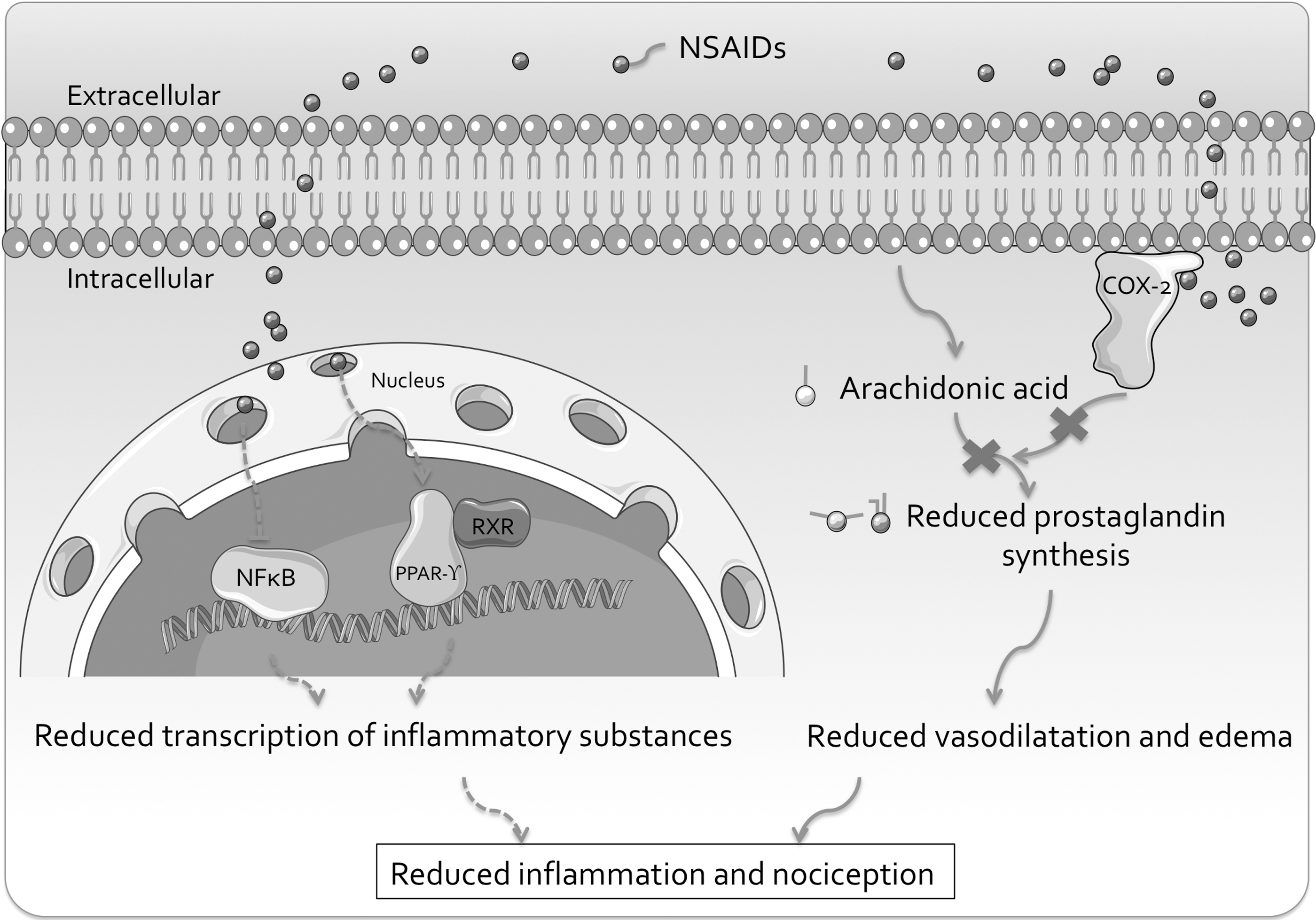
NSAID analgesia. NSAIDs bind to, and inhibit intracellular COX-2 and COX-1 (not shown). Their analgesic effect comes primarily from inhibition of COX-2. Inhibited COX-2 cannot convert arachidonic acid, which is derived from the cell membrane phospholipids, to prostaglandins such as prostacyclin. This leads to reduced vasodilatation and edema and reduced inflammation and activation of nociceptors, which is excessive in patients with severe burns. This is the primary mechanism of analgesia in NSAIDs, however, animal models have also shown non-COX-mediated analgesic mechanisms from NSAIDs within microglia. These include activation of PPAR-γ-RXR complex and inhibition of NFκB, which together lead to reduced transcription of proinflammatory intermediates. COX, cyclo-oxygenase; NFκB, nuclear factor kappa-light-chain-enhancer of activated B cells; NSAID, nonsteroidal anti-inflammatory drug; PPAR-γ, peroxisome proliferator-activated receptor-gamma; RXR, retinoid X receptor. Figure was produced using Servier Medical Art.
Anxiety also plays a role in the unpleasant emotional response to acute nociception and there is evidence to support the use of any of the following: a midazolam infusion, a dexmedetomidine infusion, antipsychotics, or a propofol infusion (for less than 48 h only) to manage acute anxiety associated with burn pain. 236 Of these agents, a midazolam infusion is the least preferred as it increases the risk of delirium 237 and dexmedetomidine the most preferred, as it has an additional analgesic effect and decreases opioid requirements. 238
Studies of nonpharmacological pain management strategies have also shown efficacy in patients with burns. Hypnosis reduces pain anxiety and improves pain quality, 239 virtual reality reduces pain scores and is most effective in patients with very severe pain, 240 and transcutaneous electrical nerve stimulation appears to safely reduce acute pain. 241
Dressings and topical therapies
Nonocclusive dressings provide an initial temporary barrier to reduce bacterial contamination, improve skin healing, and reduce pain from movement of air over skin, or from direct contact to the burned or grafted area. 242
Silver-containing dressings play an important role in the topical management of partial-thickness burns. 243 Silver is a potent antimicrobial 244 and can be used to treat (but not prevent) skin infections in burn wounds. Among silver-containing dressings, nanocrystalline silver, silver-impregnated foam, and silver-impregnated hydrofiber each appears to be superior to SSD in terms of infection control, LOS, time to healing, pain, and surgical intervention required. 243 Nanocrystalline silver dressings (Acticoat® and Acticoat 7®; Smith & Nephew) appear to be superior to silver-impregnated foam (Mepilex® Ag; Mölnlyke Health Care AB) and silver-impregnated hydrofiber (Aquacel® Ag Hydrofiber®; ConvaTec) in terms of LOS, healing time, infection control, and surgeries required. 243 SSD is consistently associated with significantly slower healing times. 245,246 Silver nylon dressings have been used in military casualties for decades, and a 10-year retrospective study of military casualties found no significant difference between patients treated with silver nylon dressings and several topical agents (mostly antimicrobial) immediately following a burn, with respect to the presence of a wound infection or the composite endpoint of wound infection, bacteremia, and/or mortality. These burns and trauma surgeons preferred silver nylon dressings due to ease of application and its light weight. 247 Newer biosynthetic dressings (e.g., Biobrane®; Smith & Nephew) that contain nylon, collagen, and silicone (and no silver) show faster wound healing times, ease of application, and patient comfort, when compared with SSD, 248 although more comparison studies between nanocrystalline silver dressings and biosynthetic dressings would be helpful.
Occlusive dressings are used postoperatively, particularly topical negative-pressure (TNP) therapy. TNP consists of a pump connected through tubing to an occlusive foam-based dressing covering the skin providing a constant negative pressure to the burn to draw moisture away from the burn while providing a temporary covering and promoting granulation tissue growth. One recent systematic review in burns did not find evidence to support its use and a systematic review in acute and chronic wounds concluded there was little evidence to support its use. 249 –251 However, a more recent literature review of a modified form of TNP found it to be a safe and effective temporary covering following early excision, particularly patients with large burns, with benefits of valuable quantification of wound exudate, reduction of opioid requirements, and lower risk of bacterial contamination. 252
Regarding other topical therapies, some of which remain in use, there is clear evidence of a lack of effect for various types of honey 253,254 and aloe vera 255,256 as well as platelet-rich plasma, 257,258 curcurmin, 259 fibroblast growth factor (FGF)-10, dermatan sulfate, 260 ultraviolet C irradiation, 261 and chitosan. 262
Antibiotics
Outside of the operating theater, antibiotics and other antimicrobial agents such as silver should be used only to treat established infection. 263 Established infection is important to diagnose, due to the risk of the development of sepsis. Sepsis has been recognized as a significant cause of death in patients with burns. 264 Sepsis criteria have been clearly defined by the American Burn Association (ABA) although these criteria correlate poorly with blood culture-proven bacteremia. 265 Newer markers of sepsis are being utilized. Procalcitonin is measured in clinical practice in patients with suspected infection. The site of production and physiological role in inflammation of procalcitonin are unclear. Although early studies assessing the prognostic utility of procalcitonin varied from supportive 266 to dismissive, 267 a recent meta-analysis and a subsequent study found that procalcitonin can clearly differentiate between a burned patient with sepsis and a burned patient without sepsis. 268,269 Once established infection has been identified, it should be treated with an antimicrobial agent. Antimicrobial selection varies according to local pathogen resistance and prevalence, and the development of infection is influenced by the use of personal protective equipment, hand hygiene, and hospital culture. 270
There is evidence from a systematic review and meta-analysis of studies of 2,117 participants to support not routinely using antibiotics to prevent infection in severe burns. Compared with control treatments, prophylactic topical antibiotics increase the risk of burn wound infection (relative risk [RR] 1.37, 95% confidence interval [CI] 1.02–1.82) and the use of silver sulfasalazine as a topical antibiotic increases infection rates by up to 80%. Prophylactic topical antibiotics also increase the risk of sepsis (RR 4.31, 95% CI 1.61–11.49), all-cause mortality (RR 5.95, 95% CI 1.1–32.33), and do not reduce the risk of bacteremia, pneumonia, urinary tract infection, adverse events, infection-related mortality, multiresistant Staphylococcus aureus (MRSA) colonization, or hospital LOS. Compared with control treatments, prophylactic systemic antibiotics increase the risk of any adverse outcome (RR 3.12, 95% CI 1.22–7.97), MRSA colonization (RR 2.22, 95% CI 1.21–4.07), hospital LOS (RR 7, 95% CI 3.28–10.72), and do not reduce the risk of burn wound infection, sepsis, bacteremia, urinary tract infection, infection-related mortality, or all-cause mortality. 271
The above data do not include the use of preoperative antibiotic use. A single preoperative dose of an appropriate antibiotic such as cefazolin (or other antibiotic as guided by local pathogen prevalence and resistance) 60 min before incision is important to prevent surgical site infection. 272 A second intraoperative dose may be required if the operation exceeds 4 h, and for prolonged major surgery, an infusion can maintain steady plasma antibiotic concentration. 273 A single dose of preoperative antibiotic reduces the risk of surgical site infection particularly for autografting procedures. 274 However, there is not yet clinical evidence to quantify the risks and benefits of preoperative antibiotics for newer minimally invasive debridement and grafting techniques.
Hyperbaric oxygen therapy
Hyperbaric oxygen therapy involves the use of 100% oxygen administered at pressures above 1 atmosphere. 275 Its use to improve healing after burns is emerging. A Cochrane systematic review of RCTs from 2013 concluded that while further evaluation was required to support its use in acute surgical wounds, the trials with patients with burns showed promising results. When compared with usual treatment, the addition of hyperbaric oxygen improved complete graft survival (RR 3.5, 95% CI 1.35–9.11) 276 and subsequent work has shown a potentially beneficial role in controlling sepsis among patients with severe burns as measured by time to normalization of procalcitonin levels (136 ± 23 days vs. 84 ± 7 days, p < 0.001). 277
Early nutrition, metabolic therapy, and exercise
Early consideration of nutrition is an important feature of modern burn management 278 although the ideal type, timing, and amount of macronutrients to be administered are not known. One consensus article suggests initially delivering enteric carbohydrates at a rate of 5–7 mg/kg body weight/min, providing a total protein quantity of 1.5–2 g/kg body weight/day and a total daily lipid quantity of <20% of nonprotein stores. However, optimal protocols are still being elucidated from animal models and high-quality evidence of improved outcomes in humans is yet to be established. 279
Catabolic processes lead to the loss of muscle mass, strength, and therefore body function. Oxandrolone and somatropin have been used to prevent this. 14 Oxandrolone is testosterone analog. In a systematic review and meta-analysis of RCTs, oxandrolone was shown to reduce body mass loss, nitrogen loss, and accelerate donor graft healing site time. 280 Recombinant human growth hormone (somatropin) provides a clinically significant beneficial effect on healing time and LOS with a side effect of increased incidence of hyperglycemia. 281
Hyperglycemia from insulin insensitivity is a well-established acute complication of severe burns and it should be avoided as it is associated with a risk of infection, catabolism, and excessive inflammation. 282 Insulin controls hyperglycemia effectively in patients with burns. 282 Its use is associated with hypoglycemia although this can be mitigated with target-guided protocols. 283 Metformin, exenatide, and fenofibrate have a role in control of hyperglycemic control beyond the acute stage of management and their use is discussed elsewhere. 14
Catecholamines drive the hypermetabolic response and can be suppressed by β-blockade. The β-blocker propranolol is well studied in burns and a systematic review and meta-analysis of RCTs shows it to be safe and effective to reduce resting energy expenditure, trunk fat, increase peripheral lean mass, and reduce the incidence of insulin resistance. 284 Exercise after hospital discharge has well-established benefits, and some evidence is emerging to support inpatient exercise. 14
Upper gastrointestinal ulcer prophylaxis
Upper gastrointestinal ulcers occur in patients after severe burn and can lead to hemorrhage. 285 They are also known as stress ulcers or Curling ulcers. Among patients with severe burns who undergo endoscopy, 38% of patients have either a gastric or duodenal ulcer, and the strongest predictors of ulcer presence are epigastric pain (OR 4.55, 95% CI 1.74–11.9) and burn size of >20% TBSA (OR 4.31, 95% CI 1.34–13.85). There is no data from studies of patients with burns to support the use of stress ulcer prophylaxis, 286 although guidelines based on findings from critically ill patients with stress ulcers support the use of stress ulcer prophylaxis for all patients with severe burns. 287 Proton pump inhibitors are more efficacious than histamine receptor antagonists among critically ill patients for the prevention of stress ulcers. 288
Summary
Several advances have been made in the field of assessing and treating patients with severe burns. Examples of advances in assessment include quantification of the limitations of the clinical examination, improvements in noninvasive imaging technology, as well as elucidation of the pathophysiology of inflammation, metabolism, and coagulation, which has led to analysis of the potential role of biomarkers.
Regarding resuscitation, there have been advances in explication of the safety and efficacy of different fluid resuscitation protocols and there is evidence to support the use of targeted fluid resuscitation particularly with natural colloids, while ascorbic acid infusion during fluid resuscitation does not seem to have a clear benefit. For surgical management, early excision and grafting is commonly performed and advanced techniques such as vascularized composite allografting for total face and hand transplants are becoming more common. Regarding perioperative management, advances have been made in the use of pharmacological and nonpharmacological analgesia. Hyperbaric oxygen therapy, TNP wound therapy and skin substitutes (which includes 3D bioprinting) are emerging burn treatments. Biosynthetic dressings and nanocrystalline silver dressings appear to be superior to dressings or creams containing SSD. There is clear evidence of harm from the use of prophylactic antibiotics, and evidence of a lack of effect from honey, aloe vera, platelet-rich plasma, curcurmin, FGF-10, dermatan sulfate, ultraviolet C irradiation, and chitosan. Benefits are apparent with hyperglycemic control and anabolic medication. Pharmacological stress ulcer prophylaxis is recommended. Ideal nutritional supplementation regimens are still to be elucidated. The greatest benefit from further research would be derived from elucidation of optimal fluid resuscitation protocols and surgical techniques based on findings from randomized trials.
Take-Home Mesages
Burn pathophysiology primarily involves excessive inflammation, hypermetabolism and coagulopathy. Evidence for the utility of potential biomarkers reflecting these processes, such as PC, is emerging.
The clinical assessment of patients with severe burns has significant limitations. Accurate assessment of burn size and depth is crucial for making decisions about treatment and although LDI is a useful adjunct to help clarify burn depth, improvements in this area will be helpful.
The crucial step in early treatment of severe burns is careful intravenous fluid resuscitation. This provides an overall mortality benefit, and the use of natural colloid solutions such as 5% albumin, and FFP appears to be associated with less morbidity than crystalloid solutions such as Hartmann's.
After resuscitation, surgical management with early burn excision and skin grafting provides a morbidity benefit. Evidence is emerging to support the perioperative use of skin substitutes, TNP wound therapy, hyperbaric oxygen therapy, anabolic medications, and nutritional supplementation to improve wound healing.
Pain after a burn is prolonged, severe, and distressing. During a hospital admission, multimodal analgesia using opioid PCA is effective for treating severe pain but patients can develop opioid tolerance. Limiting sedative infusions, considering neuraxial and non-neuraxial analgesia, rotating opioids and utilising multimodal analgesia may prevent this.
There is clear evidence of harm associated with routine use of prophylactic antibiotics and the topical administration of SSD or silver sulfasalazine, therefore these treatments should be avoided.
RCTs that quantify the safety and efficacy of different fluid administration protocols, pain management protocols, and surgical techniques would be useful.
Footnotes
Acknowledgments and Funding Sources
No funding was sought or obtained.
Ethics Approval
Ethics approval was obtained for the period of March 18, 2015 to March 18, 2020 by the Human Research Ethics Committee (HREC) of the Northern Sydney Local Health District (NSLHD). HREC Reference: HREC/13/HAWKE/417, which included review of the National Ethics Application form NEAF AU/1/F4EB112. NSLHD Reference: 1312-409M.
Author Disclosure and Ghostwriting
C.J.J., J.V., and A.W. are shareholders in a company undertaking a trial of a 3K3A-APC in diabetic ulcers. For T.C.L., R.Z., and A.K., no competing financial interests exist. The content of this article was expressly written by the authors listed. No ghostwriters were used to write this article.
About the Authors