
Abstract
Objective:
Hard-to-heal diabetic foot ulcers (DFUs) are associated with higher mortality rates and an increased medical burden for patients. ON101, a new topical cream, exhibited better healing efficacy than the control dressing in a Phase III trial. In this post hoc analysis, we further identify whether ON101 can improve the healing of ulcers with hard-to-heal risk factors in this cohort of DFU patients.
Approach:
To compare the efficacy of ON101 with absorbent dressing among various hard-to-heal wounds in patients with DFU, a post hoc analysis of a randomized Phase III trial that included 276 DFU patients was performed by subgrouping those patients based on ulcer depth, location, size, duration, and patients’ glycated hemoglobin (HbA1c) levels and body mass index (BMI).
Results:
In the full analysis set, the proportion of patients achieving healing was 61.7% in the ON101 group and 37.0% in the comparator (p = 0.0001). In subgroup analysis according to risk factors, ON101 demonstrated superior healing capacity on Wagner grade 2 ulcers (p < 0.0001); plantar ulcers (p = 0.0016), ulcer size ≥5 cm2 (p = 0.0122), ulcer duration ≥3 months (p = 0.0043); for patients with HbA1c ≥9% (p = 0.0285); and patients with BMI ≥25 (p = 0.0005).
Innovation:
ON101, a novel therapeutic drug, can modulate the functions of macrophages and demonstrate superior healing rates to conventional absorbent dressing in patients with hard-to-heal DFUs.
Conclusions:
The results of this post hoc study suggest that ON101 is a better therapeutic option than conventional dressing used in treatment for DFU patients with higher HbA1c, BMI, or ulcers with complex conditions such as longer duration, deeper wounds, larger size, and plantar location.
Guang Ning, MD, PhD

David G. Armstrong, DPM, MD, PhD
INTRODUCTION
Diabetic foot ulcers (DFUs) are one of the most prevalent complications of diabetes mellitus, whereby one-third of people with diabetes will develop an ulcer in their lifetime. 1,2 The 5-year mortality and care costs for people with diabetic foot complications, including peripheral neuropathy and peripheral vascular disease, are comparable with those for cancer treatment. 3 Such costly and severe complications are a leading contributor to the global burden of disability. 4,5 Thus, effective disease management strategies are urgently needed for DFUs.
Regarding DFU being a multifactorial clinical problem, various studies have extensively investigated the underlying possible and measurable risk factors associated with complicated and hard-to-heal DFUs to decide on wound management approaches. 6 –8 Patient-related systemic factors such as hyperglycemia and higher body mass index (BMI) are associated with the poor healing efficacy of DFUs and increased DFU-related lower-extremity amputation and mortality. 9,10 Furthermore, some risk factors such as longer wound duration, large wound size (depth and circumference), and ulcer locations under higher pressure of the ulcers themselves directly involve the healing rate. 6,7,9,11 –13 Patients with DFUs and the risk factors described above are frequently associated with longer healing time or even unhealed, which leads to poor prognoses. 8,14 This warrants a better approach to treating hard-to-heal diabetic ulcers.
A Phase III randomized controlled trial (RCT) with 236 patient participants completed in 2020 demonstrated that topically applied ON101 cream improved the overall healing rate of DFU compared with a conventional absorbent dressing during the 16 weeks of treatment period. 15 In this study, hard-to-healing risk factors, including HbA1c level higher than 9% at baseline demography, ulcer duration more than 6 months, and ulcer size more than 5 cm2, had been investigated. The result demonstrated that patients with poor glycemic control, longer ulcer duration, or larger ulcer-size wounds would have a lower wound healing rate in the dressing group than those without these risk factors. 15 However, in the ON101 cream treatment group, patients with poor glycemic control or larger ulcer size displayed similar healing efficacy compared with those without risk factors, suggesting that ON101 exerts macrophage regulating functions by which bypass the obstacles’ risk factors arise. 16 To further elucidate the effect of ON101 on more risk factors associated with hard to heal, we included an extended sample with 40 patients with DFUs to produce a cohort of 276 participants and analyze more risk factors, including BMI and ulcer depth. By dividing patients according to the severity of the investigated risk factors, we conclude that ON101 was a better choice than conventional dressing when DFU patients underwent poor glycemic control, were overweight, had longer ulcer duration, and had more significant deeper ulcers (Fig. 1).

Summarizing the effect of ON101 on the healing efficacy of DFUs with risk factors associated with hard-to-heal wounds compared with absorbent dressing. DFU, diabetic foot ulcer.
CLINICAL PROBLEM ADDRESSED
Hard-to-heal DFUs impose a substantial medical and economic burden on patients and society. Effective approaches to dealing with them urgently need to be developed. Thus, the current study enrolled 276 DFU patients treated with either ON101 or a control dressing. The primary outcome is assessing the two groups’ complete healing rate. A post hoc analysis is conducted by subgrouping the 276 patients with risk factors associated with hard-to-heal wounds.
MATERIALS AND METHODS
This study extended a randomized Phase III trial, 276 patients (including 236 eligible patients from the original study and 40 patient participants from the extended study) with DFU patients at Wagner 1 and 2 severity, following the same study protocol as established between November 23, 2012 and 17 June 2022, which aimed to compare the healing efficacy of ON101 with a control dressing (absorbent dressing; Aquacel Hydrofiber, ConvaTec, USA) in patients with Wagner Grade 1 or 2 DFUs (ClinicalTrials.gov identifier: NCT01898923). 15 The detailed clinical protocol had been shown in the previous study. 15 Electronic laboratory notebook was not used.
For the post hoc analysis, efficacy variables for subgroups were stratified by the HbA1c level (<9% vs. ≥9%), BMI (<25 kg/m2 vs. ≥25 kg/m2), ulcer depth (Wagner grade 1 vs. 2), ulcer size (<5 cm2 vs. ≥5 cm2), ulcer location (nonplantar vs. plantar), and ulcer duration (<3 months vs. ≥3 months). 6,7,9,11 –13 All analyses were conducted using SAS software (version 9.4; SAS Institute). The number and percentage of patients achieving the efficacy endpoints were calculated, and those in the ON101 group were compared with the absorbent dressing group using a chi-square test. The logistic regression model in terms of the odds ratio (OR), with p values and associated 95% confidence intervals (CIs) for treatment/intervention as fixed factors, and baseline wound size and Wagner grade evaluated as covariates, was applied to analyze the complete healing rate. Some outcomes are expressed as the hazard ratio (HR). The time to complete ulcer healing was calculated using a Kaplan–Meier method with a log-rank test. The HRs and 95% CIs were estimated using a Cox proportional hazards regression model. For safety outcomes, the incidence of infection of target ulcers and recurrence were evaluated using a Fisher exact test. For the safety parameters, numerical comparisons between treatment groups in adverse events, vital signs, and safety laboratory results were based on changes from the baseline.
RESULTS
The study population consisted of 276 patients with diabetic foot ulcer (204 males [73.9%]; 72 females [26.1%]; mean [SD; range] age, 56.8 [10.9; 23–79] years), including 141 patients in the ON101group and 135 patients in the absorbent dressing group. The demographic data, combining the previous 236 participants with the 40 newly recruited patients, were established to analyze various subgroup studies (Supplementary Tables S1 and S2). The baseline distribution of the newly recruited cohort was similar to the previous cohort of 236 participants. 15
In the newly recruited cohort, a healing rate of 68.4% was observed in the ON101 treatment group (13/19 participants). In contrast, the healing rate in the absorbent dressing group was only 47.62% (10/21 participants) (Table 1), confirming the superior healing efficacy of ON101 during the 16-week treatment period for promoting DFU healing. 15 The safety outcomes showed no treatment-related adverse effects (Table 1).
Healing efficacy in 40 patient participants
The absorbent dressing used was Aquacel Hydrofiber (ConvaTec Ltd).
Calculated using a logistic regression model. Treatment was the main exposure variable; the baseline wound size in cm2 and Wagner grade were covariates.
Ulcer recurrence was recorded once the ulcer had healed completely and was observed during the follow-up period.
FAS, full analysis set; WSA, wound (ulcer) surface area; TEAEs, treatment emergent adverse events; OR, odds ratio; CI, confidence interval; NA, not applicable.
The average baseline levels between the groups were similar in the 276 cohorts (Supplementary Table S2). The overall healing rate after 16 weeks of treatment in the ON101 group was 61.7% (87/141 patients) versus 37.0% (50/135 patients) in the comparator group (OR, 2.75; 95% CI, 1.68-4.50; p = 0.0001). The cumulative incidence of complete healing after each week also reflected the continual higher probability in the ON101 group of reaching complete wound closure (HR, 1.82; 95% CI, 1.28–2.57; p = 0.001, Fig. 2A). Moreover, the time for half of the ulcers of patients in the ON101 treated group to heal was 95.9 days. In contrast, it was not determinable in the control dressing group because only 37% of these participants had their DFU healed during the treatment period (Fig. 2A).
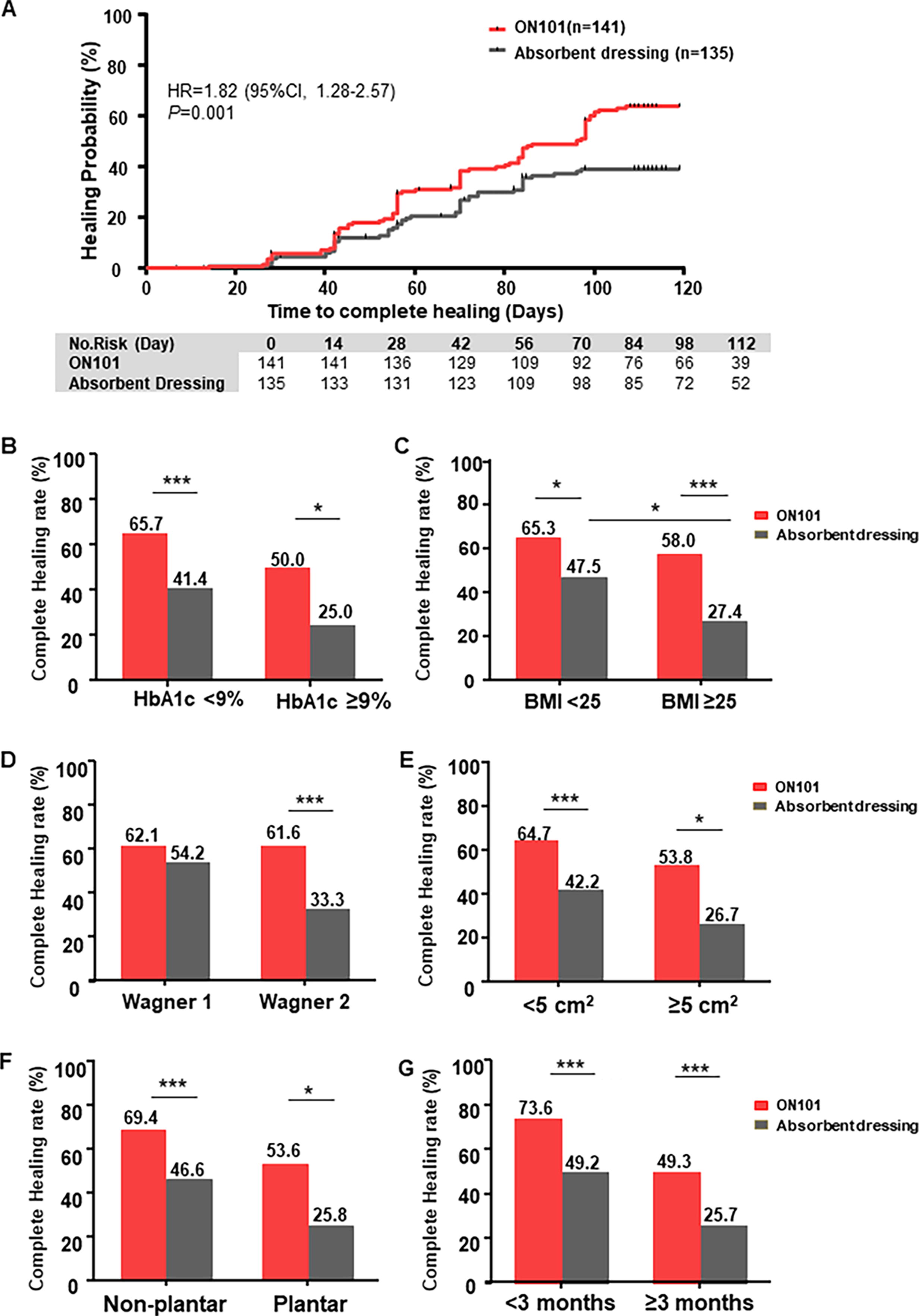
Healing efficacy in 276 patient participants and subgroups.
The healing rates for the different treatment approaches were further classified according to risk factors that may affect ulcer healing rate, including HbA1c level, BMI, and ulcer conditions, that is, ulcer depth, area, location, and duration (Fig. 2B–G). When patients encountered risk factors, such as poor glycemic control, overweight, or severe ulcer conditions, the healing rate of ulcers in patients in the control dressing treatment group decreased (Fig. 2B–G), suggesting that these factors impede healing efficacy. However, sustained healing efficacy was observed in patients in the ON101 treatment group (Fig. 2B–G), indicating that ON101 was effective regardless of ulcer conditions.
Furthermore, the average healing time was compared to the investigated factors affecting different treatment groups, and the time to reach half of the population to heal was calculated (Table 2). In the hard-to-heal group, an average 2–3 weeks delay was observed in the ON101 treatment group. In addition, most of the dressing treatment groups did not reach half of the healed population (Table 2).
Healing efficacy in the subgroup of risk factors
Calculated using a logistic regression model. Treatment was the main exposure variable; the baseline wound size in cm2 and Wagner grade were covariates.
HbA1c, glycated hemoglobin; BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); OR, odds ratio; CI, confidence interval; NA, not applicable.
Accordingly, all participants were classified as those with hyperglycemia with HbA1c <9% versus those with HbA1c ≥9%. A Kaplan–Meier plot demonstrated that in patients with HbA1c <9%, the cumulative healing curve with ON101 treatment tended to be significantly higher from the control dressing cohort (HR, 1.67; 95% CI, 1.13–2.46; p = 0.008; Fig. 3A). In patients with HbA1c ≥9%, ON101 treatment had superior healing efficacy than absorbent dressing treatment (HR, 2.35; 95% CI, 1.05–5.23; p = 0.029; Fig. 3B).
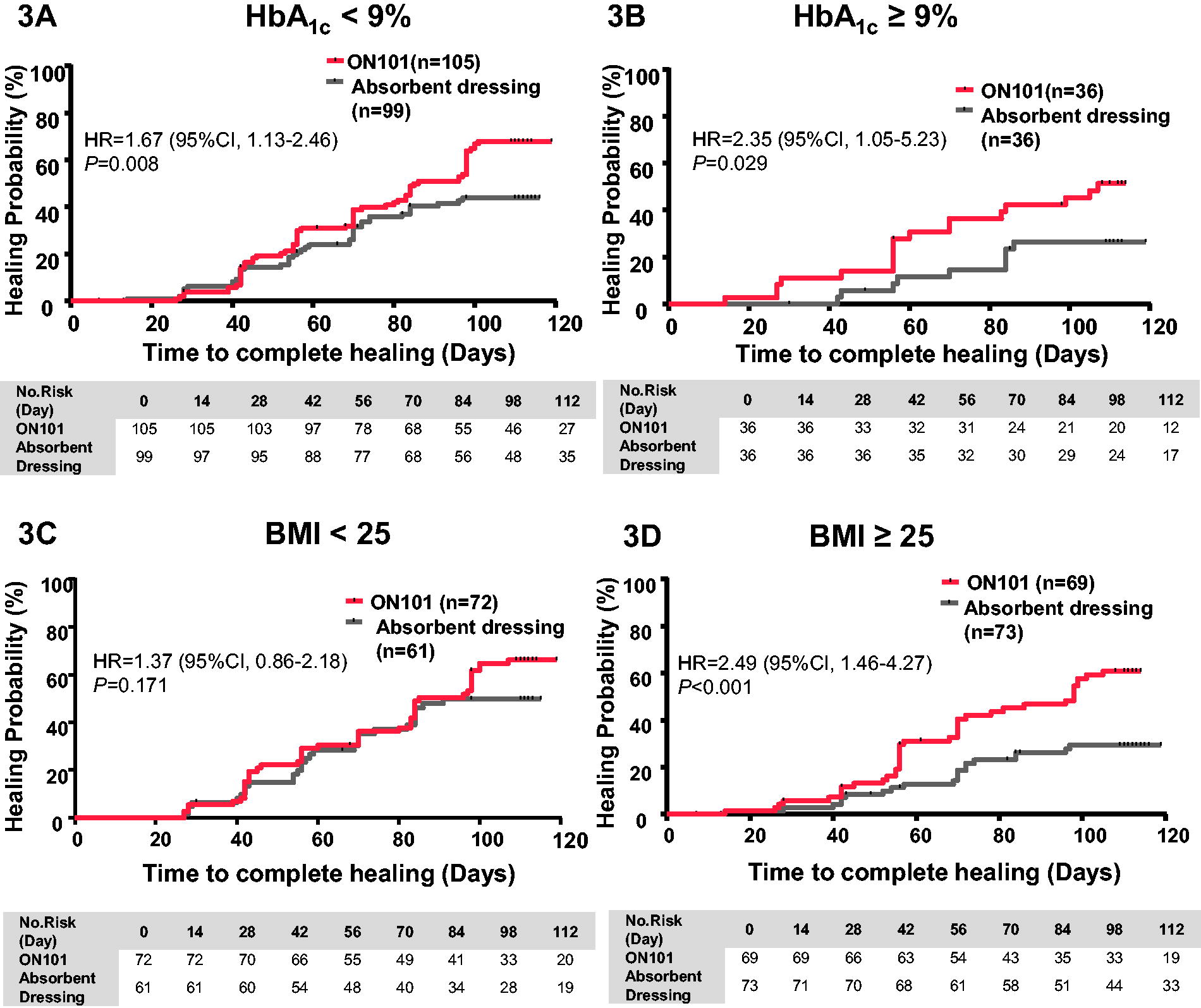
Kaplan–Meier plot for patients classified according to glycemic condition and BMI
When the healing efficacy was assessed in patients classified according to BMI, the cumulative healing curves were not significantly different between groups (HR, 1.37; 95% CI, 0.86–2.18; p = 0.171; Fig. 3C). In addition, in the overweight group (BMI ≥25), patients treated with ON101 had significantly better healing than patients treated with absorbent dressing (HR, 2.49; 95% CI, 1.46–4.27; p < 0.001; Fig. 3D). In overweight patients, we found a significantly lower healing rate in those treated with the absorbent dressing (p = 0.02; Fig. 2C), but there was no significant delay in healing in those treated with ON101 (p = 0.391; Fig. 2C).
We performed a Kaplan–Meier analysis to verify the healing time curve for the divided groups with Wagner grade 1 (Fig. 4A) and grade 2 (Fig. 4B) DFUs. The healing time curve with ON101 treatment or dressing for superficial wounds (Wagner grade 1) was similar (HR, 1.15; 95% CI, 0.56–2.34; p = 0.705; Fig. 4A), but the cumulative curve for patients treated with ON101 showed a significantly faster healing trend in the Wagner grade 2 group than in the control dressing group (HR, 2.05; 95% CI, 1.38–3.06; p < 0.001; Fig. 4B). A Kaplan–Meier plot showed that compared with those treated with the standard dressing, there was faster healing of ulcers <5 cm2 (HR, 1.64; 95% CI, 1.10–2.45; p = 0.012; Fig. 4C) and ulcers ≥5 cm2 (HR, 2.19; 95% CI, 1.08–4.46; p = 0.025; Fig. 4D) in patients treated with ON101. The cumulative healing curve showed that ulcers healed faster in patients treated with ON101 than in those treated with standard dressing, regardless of ulcer location (Fig. 4E and F). The plantar region can be further classified into different pressure sites, and we found that ON101 significantly improves the healing efficacy in ulcers on the dorsal and metatarsal (Supplementary Fig. S2). We further used an ulcer duration of 3 months as a cutoff to classify the 276 patients into a group with an ulcer duration of <3 months (n = 137) and group with an ulcer duration of ≥3 months (n = 139). A Kaplan–Meier plot showed that ulcers in patients treated with ON101 healed significantly faster than those in the standard dressing group at both with ulcer duration of <3 months (HR, 1.67; 95% CI, 1.07–2.59; p = 0.018; Fig. 4G) and with ulcer duration of ≥3 months (HR, 2.03; 95% CI, 1.14–3.59; p = 0.012; Fig. 4H).
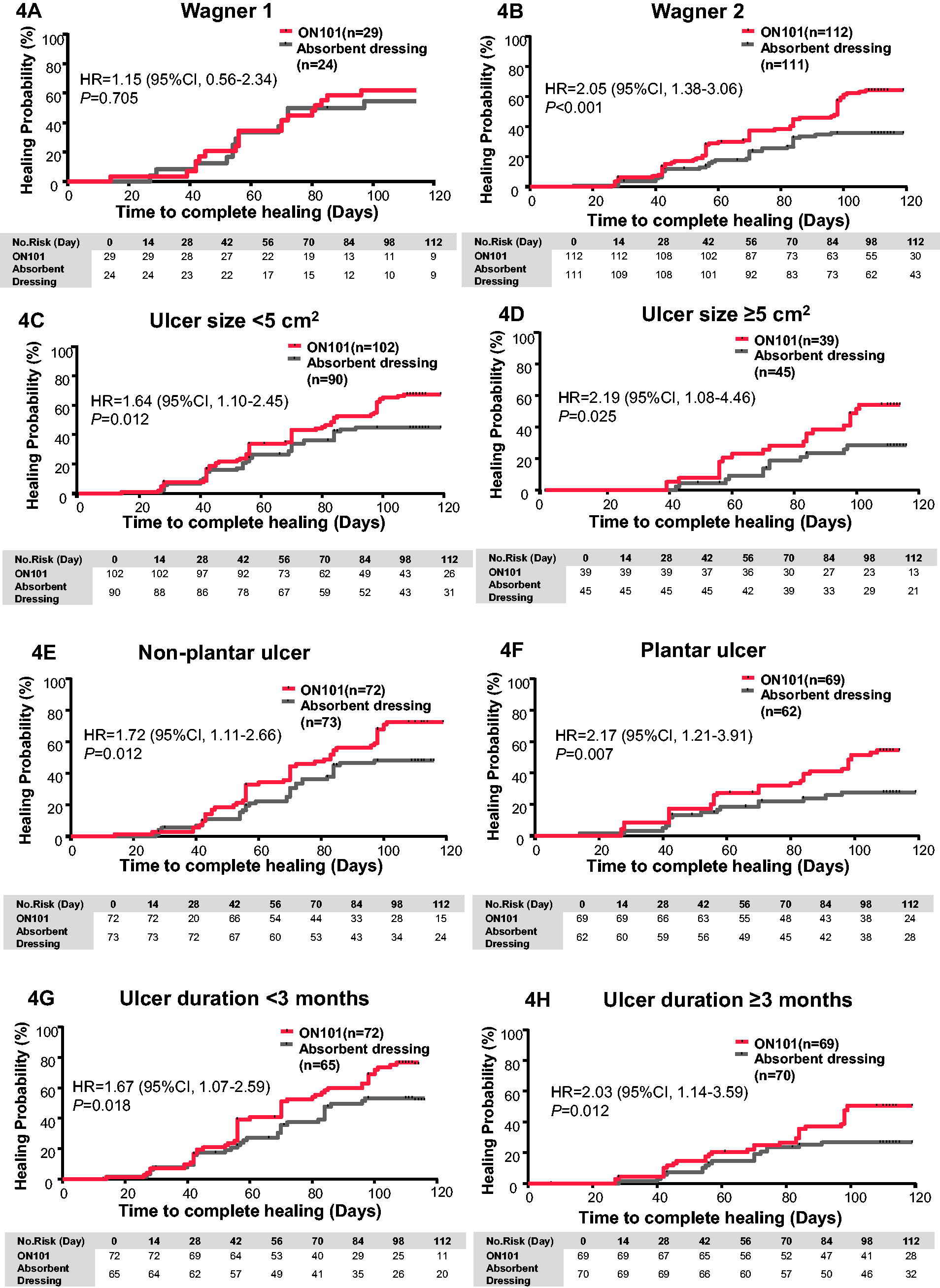
Kaplan–Meier plot for patients classified according to ulcer depth
Considering that most of the patients with DFUs (80%) enrolled in the present study had Wagner grade 2 ulcers, we combined this risk with other factors to determine whether the efficacy of treatment with ON101 was still superior to that for the standard dressing in those with more likely to have hard-to-heal ulcers with multiple risk factors. As expected, when Wagner grade 2 combined other risk factors, including hyperglycemia, obesity, large ulcer size, longer duration, and plantar location, we found that ON101 produced around a twofold greater healing rate than the standard dressing control (Supplementary Fig. S3), suggesting that ON101 has a robust healing ability in complicated and hard-to-heal DFUs in patients with other risk factors.
DISCUSSION
Recurrent ulceration and deterioration of DFUs involve multiple factors, including systemic metabolic disorders and extrinsic stress that persists in diabetic patients after the wound occurs. 6,13,17 These factors impede wound healing and increase the risk of amputation and even mortality in people with DFUs. 6,13,17 In the 276 DFU patients’ study, we found that ON101 has superior healing efficacy compared with a standard absorbent dressing. We observed robust healing effectiveness of ON101 for severe ulcers with risk factors classified as ulcer severity, depth, size, duration, and location or in patients with systemic risk factors such as high HbA1c level and BMI. Although Wagner grade 2 itself, compared with grade 1, is recognized as a risk factor for hard-to-heal DFU, 18 when Wagner grade 2 DFU patients who had other risk factors such as hyperglycemia, high BMI, large ulcer size, long ulcer duration, and plantar location, we still found that ON101 retained a greater efficacy than the control dressing in such complicated wound conditions. Studies of several real-world cases of hard-to-heal ulcers, such as those of UT/Wagner grade 3 or more complex in patients with diabetic comorbidities, found that topical ON101 treatment greatly improved diabetic wound healing. 19 –21 These observations suggest that ON101 cream has great potential for treating various hard-to-heal DFUs in complicated real-world wounds.
Defects in the M1-to-M2 macrophage transition during the inflammation-to-proliferation phase transition, a critical feature characterized by persistent chronic inflammation, are considered to be affected by systemic problems in patients with DFUs. 22,23 Diabetes-associated factors, including hyperglycemia, hypoxia, ischemia, and hyperinflammation, are known to impair macrophage polarization and monocyte recruitment to the injury site. 24 –28 It has also been shown that hyperlipidemia and hyperglycemia alter the genetic profile of macrophages at the epigenetic level, which results in the expression of pro-inflammatory cytokines. 25,29 Hard-to-heal wounds have exacerbated persistent chronic inflammation triggered by various inflammatory mediators and M1/M2 ratio imbalance, making it challenging to heal these wounds.
A number of factors modulate the presence and persistence of ulcers. Deeper, larger, and older ulcers, as well as those in high-pressure areas, require more time to heal. 11,30 –33 We found sustained healing efficacy in patients treated with ON101 even when the ulcers were persistent or did not heal, especially in patients with complicated wounds, such as Wagner/UT grade 2 DFU, who had other risk factors simultaneously. These findings suggest that ON101 can proactively overcome systemic or difficult ulcer conditions to increase wound healing rates, unlike standard absorbent dressings, which passively prevent ulcer exacerbation. ON101 is a novel therapeutic modality for reducing M1 macrophages and elevating M2 macrophages, the central mechanism by which ON101 counteracts hard-to-heal DFUs.
Current standard wound care, such as debridement, off-loading, and antibacterial dressing, which passively manage wounds by avoiding reinfection, providing pressure relief, and maintaining the wound under a moist environment, is not intended to specifically deal with chronic inflammation. 34 Adjuvant therapies, such as oxygen therapy, negative pressure wound therapy, and biologics, barely involve macrophage regulation. 34,35 However, our subgroup results, classified by ulcer conditions, showed that macrophage regulation approaches such as ON101 treatment could reduce the proportion of M1 macrophages and reduce the production of pro-inflammatory cytokines, providing the therapeutic potential to promote the healing of diabetic wounds associated with confounding metabolic risks.
KEY FINDINGS
ON101 effectively improved DFU healing in a cohort of 276 subjects compared to standard dressings. ON101 displayed robust efficacy in ulcers with concomitant risk factors that may delay wound healing, including hyperglycemia, high BMI, difficult wounds (large size, depth, and stressed sites), and long ulcer duration. ON101 has the potential to change the treatment paradigm of DFU in clinical practice.
The limitation of this study is that the type I error rate was not controlled in the post hoc analysis. However, given that it was focused on exploring the consistency of treatment effects across subgroups, this limitation may be of marginal concern. An appropriate approach to controlling type I error is required for future studies intending to implement confirmatory subgroup analysis to corroborate this study’s findings.
INNOVATION
ON101, a novel drug, can reorchestrate the DFU microenvironment by rebalancing the proportion of M1 and M2 macrophages. Compared with standard absorbent dressing, the approach using ON101 appears to significantly improve the healing of DFUs in patients with various conditions, including HbA1c levels ≥9%, BMI ≥25, Wagner grade 2 ulcers, ulcer sizes ≥5 cm2, plantar ulcers, and ulcers persisting ≥3 months. ON101 cream is a potentially effective and beneficial treatment option for hard-to-heal DFUs.
Footnotes
ACKNOWLEDGMENTS AND FUNDING SOURCES
This study was supported by Oneness Biotech Company Limited, Microbio Company Limited, and Haihe Biopharma Company Limited.
AUTHORS’ CONTRIBUTIONS
S.-C.C., G.N., and D.G.A. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: S.-G.C., C.-W.L., J.-C.C., and Y.-H.W. Acquisition, analysis, or interpretation of data: S.-C.C., G.Ning., D.G.A., S.-G.C., Y.-Y.H., N.-C.C., S.M.C., H.-H.C., K.-F.H., K.-Y.T., K.-Y.T., H.-L.H., C.-K.P., B.S., C.L., Y.M., Y.C., Y.L., Y.X., L.Y., and Q.L. Drafting of the article: D.G.A., C.-W.L., J.-C.C., and Y.-H.W. Critical revision of the article for important intellectual content: S.-C.C., D.G.A., G.N., C.-W.L., J.-C.C., and Y.-H.W. Statistical analysis: Y.-H.W. Administrative, technical, or material support: C.-W.L., J.-C.C., and Y.-H.W. Supervision: G.N. and D.G.A.
ROLE OF THE FUNDER/SPONSOR
Sponsors were responsible for designing the study and preparing the article. The sponsors had no role in the conduct of the study; collection, management, analysis, and interpretation of the data; review or approval of the article; or decision to submit the article for publication.
ADDITIONAL CONTRIBUTIONS
We thank all the staff and participants at the sites involved in the study. Ya-Yuan Lu, MS (Bestat Pharmaservices Corporation), was responsible for statistical analysis and data interpretation. The sponsors paid Bestat Pharmaservices Corporation for their services. OnLine English editors assisted with revision, for which they were compensated.
AUTHOR DISCLOSURE AND GHOSTWRITING
C.-W.L., J.-C.C., and Y.-H.W. were the employees of Oneness Biotech. The rest of the authors have no competing financial interests. The content of this article was expressly written by the authors listed. No ghostwriting was used to write this article.
ABOUT THE AUTHORS
SUPPLEMENTARY MATERIAL
Supplementary Data S1
Supplementary Data S2
Supplementary Figures
Supplementary Tables
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.