
Abstract
Objective:
To compare the effectiveness of “semiocclusive dressing (SOD)” treatment using plastic wrap or low-adherent absorbent wound dressings with that of occlusive dressing (OD) treatment for National Pressure Injury Advisory Panel stage III/IV pressure injuries in the inflammatory phase.
Approach:
This 12-week, open-label, randomized controlled trial was conducted at one hospital and three care facilities. Seventy-seven participants were enrolled; 40 comprised the SOD group and 37 comprised the OD group. The primary outcome was the surface area reduction. Secondary outcomes included the Bates-Jensen Wound Assessment Tool (BWAT) score reductions, incidence of adverse events, and material cost. This trial met the recommendations of the CONSORT 2010 statement.
Results:
The surface area reduction of the SOD group was greater than that of the OD group throughout the study period. The significant interaction was revealed between treatment and time course (p < 0.0001). The 95% confidence interval of the difference at 12 weeks was 3.4 to 21.9. The median BWAT score reduction of the SOD group at 12 weeks was 23, and that of the OD group was 18.5 (p = 0.0077). The incidence of adverse events was comparable between groups. The OD treatment cost was 3.0 times higher than the SOD treatment cost (p = 0.0012).
Innovation:
Because the SOD does not completely occlude the wound, excess exudate drains from the wound. Therefore, SOD can treat the wound with abundant exudate effectively and safely.
Conclusion:
SOD treatment is more effective and less expensive than OD treatment for stage III/IV pressure injuries.
Clinical Trial Registration:
UMIN Clinical Trials Registry [UMIN000023412]. Registered on July 31, 2016.
Keywords
INTRODUCTION
Although not well-known worldwide, the use of food wrap as a dressing material to treat pressure injuries is widespread in several countries. The effectiveness of plastic wrap dressing (PWD) for National Pressure Injury/Ulcer Advisory Panel (NPIAP)1,2 stages II, III, and IV pressure injuries has been reported.3–8 Because PWD treatment involves only nonmedical and low-cost materials, some experts regard it as a strange folk remedy or cheap alternative to medical treatment and dismiss it. Whereas many medical professionals view that it is rational treatment3–5,9,10 based on the modern concepts of moist healing11–13 and wound bed preparation14–16 with the unique mechanism that differs from conventional treatments.
The most crucial feature of PWD treatment is that the dressing material does not tightly adhere to the wound. Thus, the part of the dressing detaches from the wound when abundant exudate is generated and excess exudate drains outside the wound. This mechanism that the dressing material does not completely occlude the wound prevents wound deterioration following increased intrawound pressure and maintains an adequately moist environment to facilitate wound healing. Because the wound was not sealed, the lack of air permeability of the PWD caused no clinical problems.
The frequent adverse event associated with PWD treatment is periwound skin maceration due to overflowing exudate. To prevent it, several modified methods of PWD treatment have been developed to manage the exudate more effectively. One such method involves to use a PWD punched with many small holes and place an absorbent pad over it. Another is to place an absorbent pad inside a polyethylene bag with many small holes (sold as food waste bags).17,18
In addition, medical materials have been used, such as low-adherent absorbent wound dressings (for burns and postoperative wounds). 18 These products consist of some different layers, including an inner layer of low-adherent perforated film that prevents sticking to the skin, an absorbent layer made of cotton, resin, or polyester fiber pad, and a hydrophobic backing layer. The mechanism of these modified methods that the dressing material incompletely occludes the wound and allows excess exudate to drain from the wound is identical to that of PWD treatment. We call the treatments based on this mechanism “semiocclusive dressing (SOD)” treatment.
CLINICAL PROBLEM ADDRESSED
We hypothesized that SOD treatment involving PWD treatment and its modified treatments would improve severe pressure injuries faster than standard occlusive dressing (OD) treatment because of the results of previous reports.5–7 These reports suggested that PWD treatment was superior to standard treatment for the management of stage III/IV pressure injuries in the acute inflammatory phase9,10 with much exudate and necrotic tissue, however, the level of evidence was inadequate. Furthermore, few articles are available on SOD treatment other than PWD treatment. Thus, we compared the effectiveness of SOD treatment with that of OD treatment for NPIAP stage III/IV pressure injuries in the inflammatory phase.
MATERIALS AND METHODS
Trial design and participants
This 12-week, prospective, randomized controlled trial involved 10 wards of a Japanese psychiatric/geriatric hospital and three care facilities between August 2016 and March 2019. This study had an open-label design because it was impossible to mask the intervention. The Minakuchi Hospital Clinical Review Board approved the study protocol. This trial was registered on UMIN Clinical Trials Registry [UMIN000023412], and performed in accordance with the Declaration of Helsinki and its amendments. Study design and reporting followed the recommendations of the CONSORT 2010 guidelines. 19 Written informed consent was obtained from all participants or their family members.
Patients who were 20 years or older and had stage III or IV pressure injuries according to the NPIAP Pressure Injury Staging System1,2 were considered for inclusion in this study. Eligible participants had pressure injuries within 3 weeks of onset, ranging from 4 to 80 cm2 (Bates-Jensen wound assessment tool [BWAT]20,21 score of 2–4 for size), and at least 50% of the surface area was covered by necrotic tissue (BWAT score of 4–5 for necrotic tissue amount). If patients had wounds covered with black hard eschars, we included them after surgically removing the eschars. When patients had multiple wounds, the largest wound was selected. Participants were excluded for the following reasons: the skin ulcer was attributable to other causes, such as peripheral arterial occlusive disease or skin cancer; poorly controlled diabetes (HbA1c >10.0% measured at the time of registration); or treatment with cytotoxic agents or immunosuppressants.
The baseline parameters included age, sex, mental disorders, systemic diseases (including infectious diseases, diabetes, and malignancy), hemoglobin level, body mass index, serum albumin level, Braden Scale22,23 score, location and surface area of the wound, and BWAT score. After obtaining these baseline characteristics, simple randomization was performed to allocate the consenting participants to SOD or OD treatment in a 1:1 ratio. For this randomization, a researcher affiliated with the registrar’s office who was not involved in the treatment or evaluation assigned treatments using a random number table created in Excel 2010 for Windows (Microsoft Japan Co., Ltd., Tokyo, Japan) and recorded the result on the registration form. An electronic laboratory notebook platform was not used.
Intervention
Procedure for SOD treatment
This study used unsterilized PWD or low-adherent absorbent wound dressing for SOD treatment. The low-adherent absorbent wound dressing was the first choice of treatment. The PWD was preferentially used when the wound was too large or when the wound with less exudate tended to dry out. 18 Unlike OD treatment, SOD treatment did not require the type of dressing material to be changed based on the wound condition and could be implemented in the same manner from wound development to healing.
After cleansing with saline solution, the wound was covered with the dressing material. To allow loose adherence to the wound, nonwoven or plastic tape with weak adhesive strength was used5,6; this is one of the most critical points of SOD treatment. After treatment initiation, a foul odor or copious yellow exudate might be observed. These signs indicated good performance of autolysis of devitalized tissue promoted by a moist environment, rather than wound infection or deterioration in most cases.5,6 Changing the dressing materials, removing the autolyzed necrotic tissue, and cleansing the wound two to four times daily resulted in translucent and odorless exudate after one to two weeks without antibiotic use. Subsequently, the amount of exudate decreased. Thereafter, changing the dressings once or twice daily was sufficient.
Procedure for OD treatment
After cleansing with saline solution, the polyurethane foam dressing was applied to the wound with extensive exudate, whereas the hydrocolloid dressing was applied to the wound with less exudate.24–27 Infected wounds were treated with the silver-impregnated dressing or calcium sodium alginate dressing.24,25 One physician decided which dressing to use depending on the depth of the wound, nature and volume of exudate, and presence of wound infection. The frequency of dressing changes was determined based on the amount of exudate. If the exudate was controlled, then the dressing was changed several times per week. For wounds with excess exudate or infection, the dressing was changed once or twice daily.
Common procedures
No disinfectants such as iodine or topical antibiotics were used.5–8 Debridement of necrotic tissue was primarily performed by autolysis. Surgical debridement and/or skin incision were performed for wounds with extensive necrosis, advanced cellulitis, and large abscesses.26,27 Calcium sodium alginate dressings were occasionally used to manage bleeding after surgical procedures. 28 Systemic antibiotics were administered to treat cellulitis or bacteremia/sepsis.
Depending on the risk level indicated by the Braden Scale, prevention protocols were implemented29–32 by a trial-independent pressure injury prevention and management committee. An alternating air pressure mattress, high-specification reactive foam mattress, nonpowered pressure redistribution support surface, seat cushions, and overlays were applied to enhance pressure redistribution, shear reduction, and proper posture.33–38
Outcome measures
The primary outcome measure was the difference in absolute surface area reduction (SAR) of both treatment groups throughout the study period observed when the baseline surface area was compared with the surface area after treatment (SAR = baseline surface area − actual surface area). Surface area measurements were performed as follows; after cleansing the wound and debridement, a ruler was placed vertically on the wound and photographed using a digital camera. Using these images and Leaf Area Counter Plus software (Vector Inc., Tokyo, Japan), the same investigator who was unaware of treatment allocation measured the surface area at baseline and every week.
The secondary outcomes included SAR value and BWAT score reduction comparison at 4, 8, and 12 weeks resulting from both treatments (BWAT score reduction = baseline BWAT score − actual BWAT score). A physician and nurse who were aware of treatment allocation examined the wound together and recorded BWAT scores for all wounds at baseline and every week. In addition, the incidence of adverse events, including wound infection and maceration, the frequency of wound deterioration as assessed by SAR values or BWAT score, material cost, and frequency of dressing changes were compared. The material cost was calculated by the number of each used item and unit price at which the hospital purchased the item. Nurses recorded the number of dressings, gauze, absorbent pads, gloves, and amount of saline used for each procedure.
Statistical analyses
Based on the results of previous studies,5,6 59 patients were needed in each arm of the study to detect a mean difference of 6.0 cm2 (standard deviation [SD], ±10.0 cm2) in the SAR between groups at 12 weeks and ensure an alpha risk of 0.0167 (to maintain an overall alpha level of 0.05 based on the Bonferroni adjustment) and study power of 0.80. Allowing for 10% loss to follow-up and unbalanced allocation, a minimum sample size of 150 (75 per group) was determined. We used EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) 39 for sample size planning.
Statistical analyses were performed on an intention-to-treat basis. All statistical tests were two sided, with an alpha level of 0.05. All analyses were performed using Stat View version 5.0 (SAS Institute Inc., Cary, NC, USA) and EZR. The difference in SAR for both treatment groups during the study period was evaluated by a linear mixed-model. The SAR value and BWAT score reduction comparison at 4, 8, and 12 weeks were analyzed using the unpaired Student’s t-test and the Mann–Whitney U test, respectively; for multiple comparisons, the Bonferroni adjustment was applied. For patients lost to follow-up but who were observed at least once after randomization, the last data observed were carried forward. Fisher’s exact test was used to analyze the incidence of adverse events and the frequency of wound deterioration. The material cost and frequency of dressing changes of both treatment groups were compared using unpaired Student’s t-test.
RESULTS
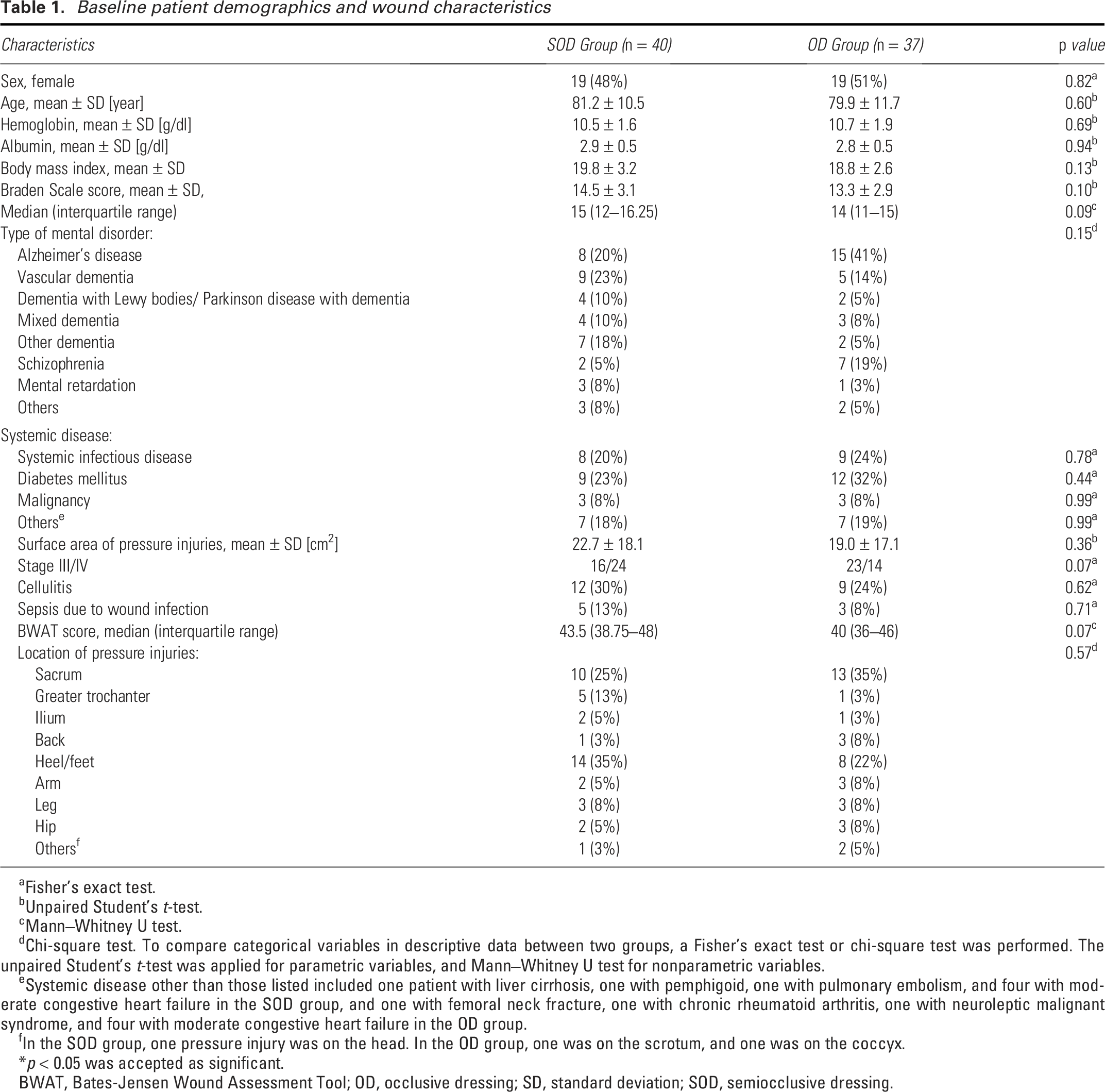
Eighty-six patients with deep skin ulcers were screened. Of those patients, 77 were enrolled and randomized to the SOD group (n = 40) or OD group (n = 37). Although the estimated number of necessary participants was not achieved, patient recruitment was terminated because changes in the practice structure of the research facility caused difficulties in the acceptance of more patients with pressure injuries. Figure 1 summarizes the flow of participants through the trial. Their baseline demographics and wound characteristics are shown in Table 1. The two groups were well-balanced.
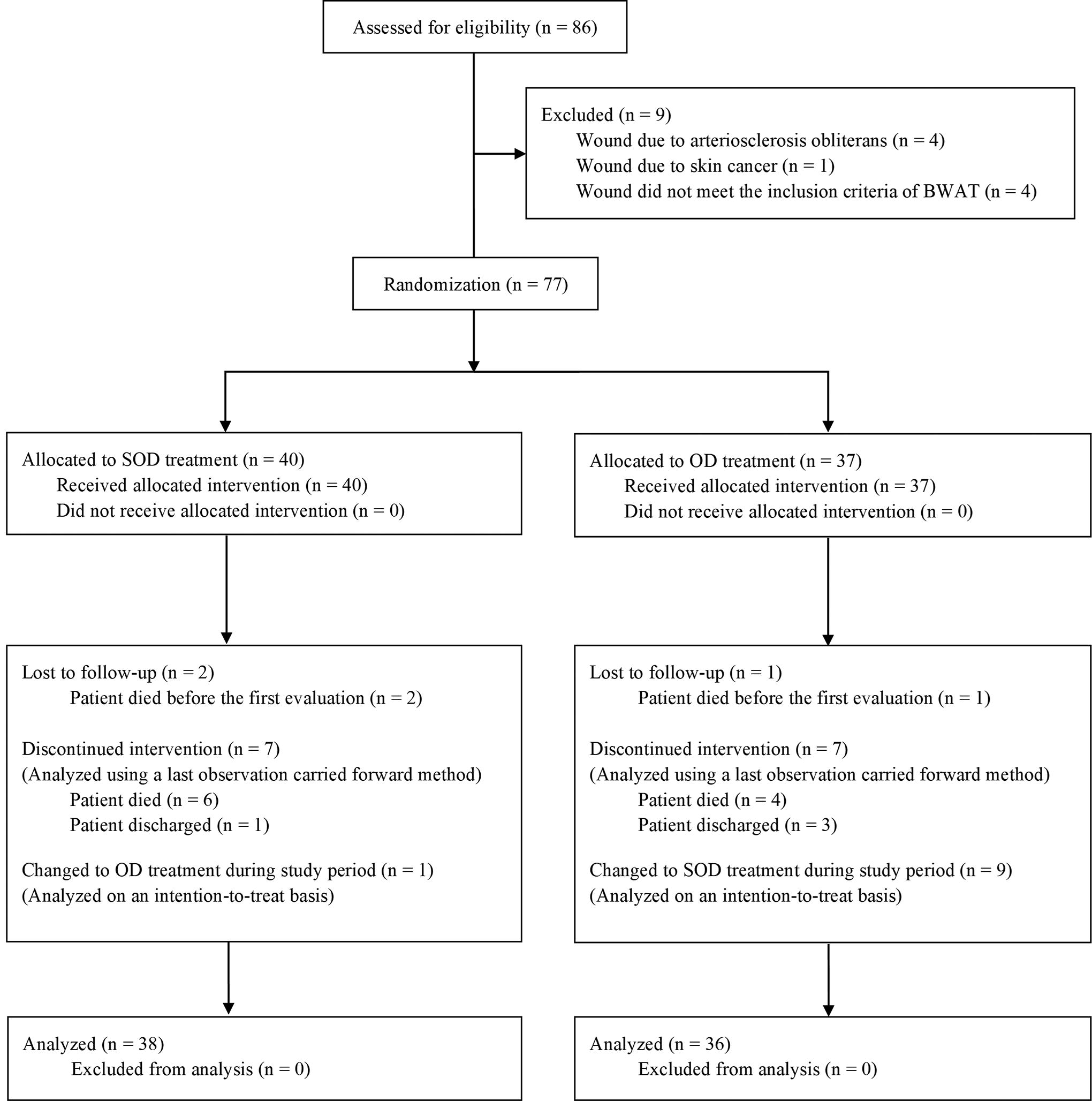
Flow of participants during the trial. BWAT, Bates-Jensen Wound Assessment Tool; OD, occlusive dressing; SOD, semiocclusive dressing.
Baseline patient demographics and wound characteristics
Fisher’s exact test.
Unpaired Student’s t-test.
Mann–Whitney U test.
Chi-square test. To compare categorical variables in descriptive data between two groups, a Fisher’s exact test or chi-square test was performed. The unpaired Student’s t-test was applied for parametric variables, and Mann–Whitney U test for nonparametric variables.
Systemic disease other than those listed included one patient with liver cirrhosis, one with pemphigoid, one with pulmonary embolism, and four with moderate congestive heart failure in the SOD group, and one with femoral neck fracture, one with chronic rheumatoid arthritis, one with neuroleptic malignant syndrome, and four with moderate congestive heart failure in the OD group.
In the SOD group, one pressure injury was on the head. In the OD group, one was on the scrotum, and one was on the coccyx.
p < 0.05 was accepted as significant.
BWAT, Bates-Jensen Wound Assessment Tool; OD, occlusive dressing; SD, standard deviation; SOD, semiocclusive dressing.
Initially, 29 patients and 11 patients in the SOD group were treated with the low-adherent absorbent wound dressing and PWD, respectively. In the OD group, 10 patients and 27 patients were initially treated with the hydrocolloid dressing and polyurethane foam dressing, respectively. During the trial, the treatment of nine patients was changed from the OD to SOD because of excessive exudate. The treatment of one patient was switched from the SOD to OD because SOD treatment could not be performed at the facility where he would be transferred.
Outcome measures
Figure 2 shows the SAR of both groups. The SAR of the SOD group was greater than that of the OD group during the study period. The significant interaction was revealed between treatment and time course (p < 0.0001). The mean SAR values of the SOD group at 4, 8, and 12 weeks were 7.4 cm2 (SD, ±16.6 cm2), 12.1 cm2 (SD, ±19.2 cm2), and 14.0 cm2 (SD, ±19.9 cm2), respectively, whereas those of the OD group were −0.4 cm2 (SD, ±18.6 cm2), −0.1 cm2 (SD, ±22.2 cm2), and 1.3 cm2 (SD, ±20.0 cm2), respectively. The differences between groups were statistically significant at 8 and 12 weeks. The 95% confidence intervals of the differences at 4, 8, and 12 weeks were −0.3 to 16.0, 2.6 to 21.8, and 3.4 to 21.9, respectively.
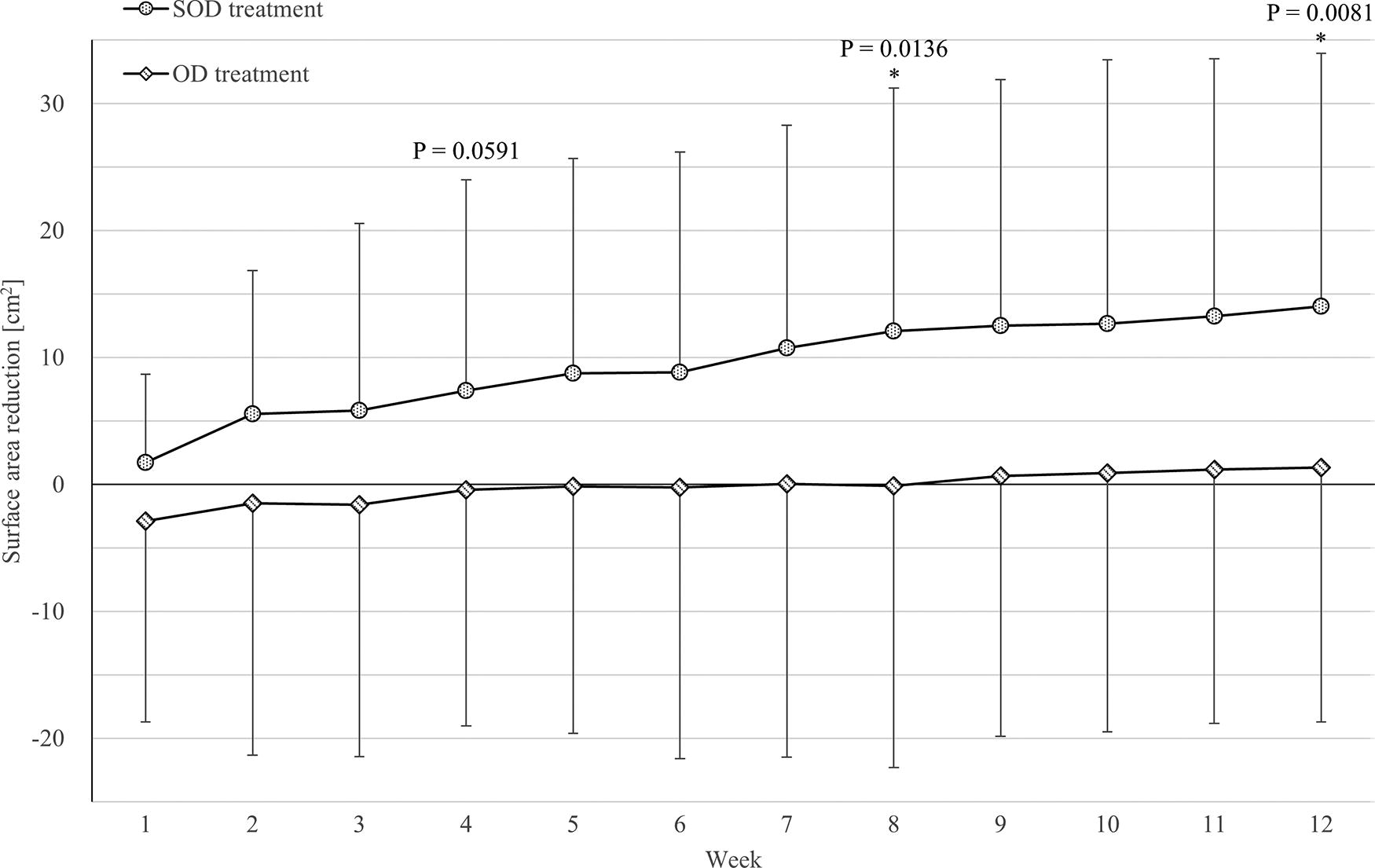
SAR of the SOD and OD treatment groups. The linear mixed model revealed a significant interaction between treatment and time course (p < 0.0001*). The comparisons of SAR values at 4, 8, and 12 weeks resulting from both treatments were performed using the unpaired Student’s t-test and Bonferroni adjustment for multiple comparisons. *Statistically significant. SAR, surface area reduction.
Figure 3 shows the BWAT score reductions of both groups. The median BWAT score reductions of the SOD group at 4, 8, and 12 weeks were 14 (interquartile range [IQR], 10.25–20), 18 (IQR, 13.25–26.75), and 23 (IQR, 14.25–29.75), respectively. The corresponding values of the OD group were 12 (IQR, 0–21), 16 (IQR, 8.5–22), and 18.5 (IQR, 9.75–22). At every assessment point, the BWAT score reduction of the SOD group was greater than that of the OD group, with a statistically significant difference observed at 12 weeks.
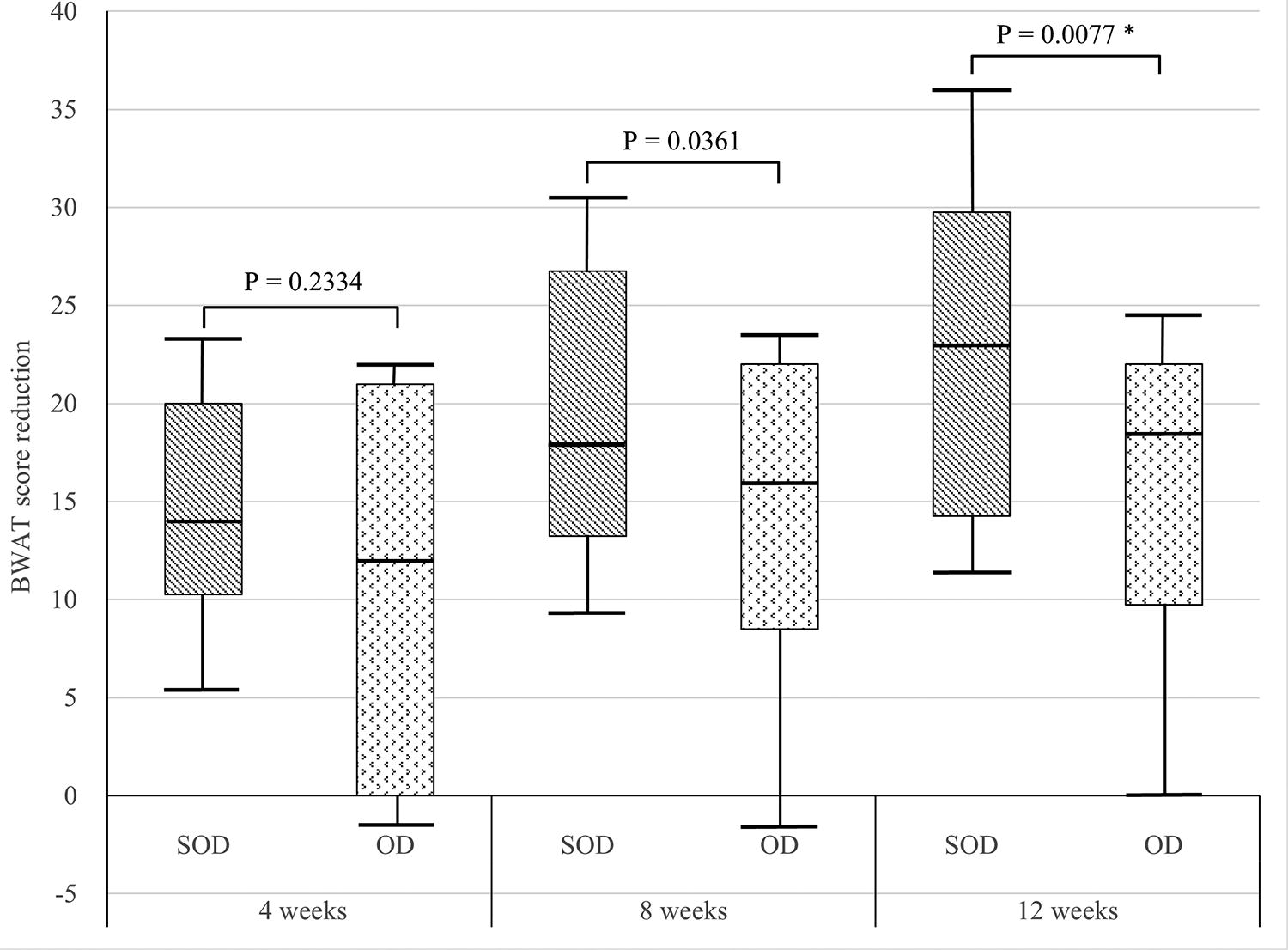
BWAT score reduction of the SOD and OD treatment groups. The horizontal bar in each box represents the median. Horizontal boundaries of the boxes represent the first and third quartiles. Vertical bars indicate the values of the 10th and 90th percentiles. p Values were based on the Mann–Whitney U test, and the Bonferroni adjustment was used for multiple comparisons. *Statistically significant.
The incidence of adverse events and the frequency of wound deterioration with both treatments were approximately equal (Table 2). Table 3 shows the material cost and frequency of dressing changes. The cost associated with OD treatment was significantly higher (3.0 times higher) than that associated with SOD treatment. Conversely, the frequency of dressing changes of the SOD group was significantly higher (2.4 times higher) than that of the OD group.
Incidence of adverse events and frequency of wound deterioration
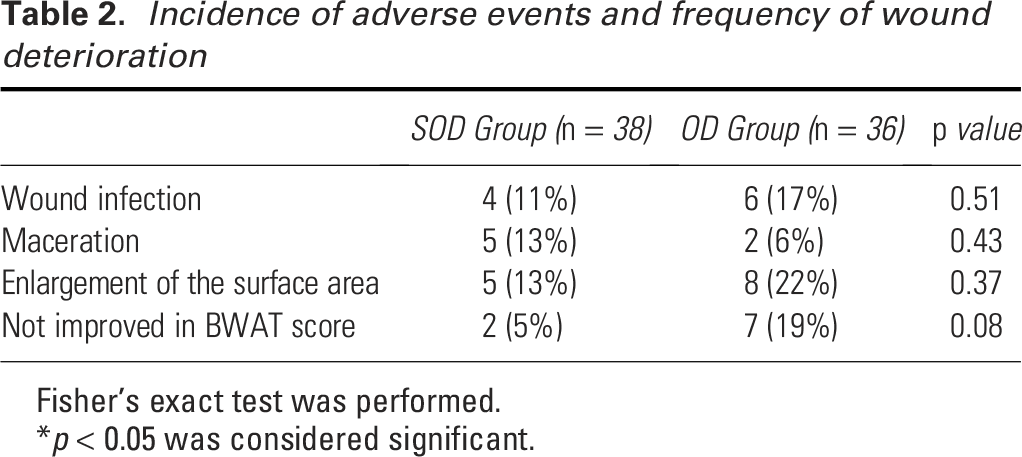
Fisher’s exact test was performed.
p < 0.05 was considered significant.
Material costs and frequency of dressing changes
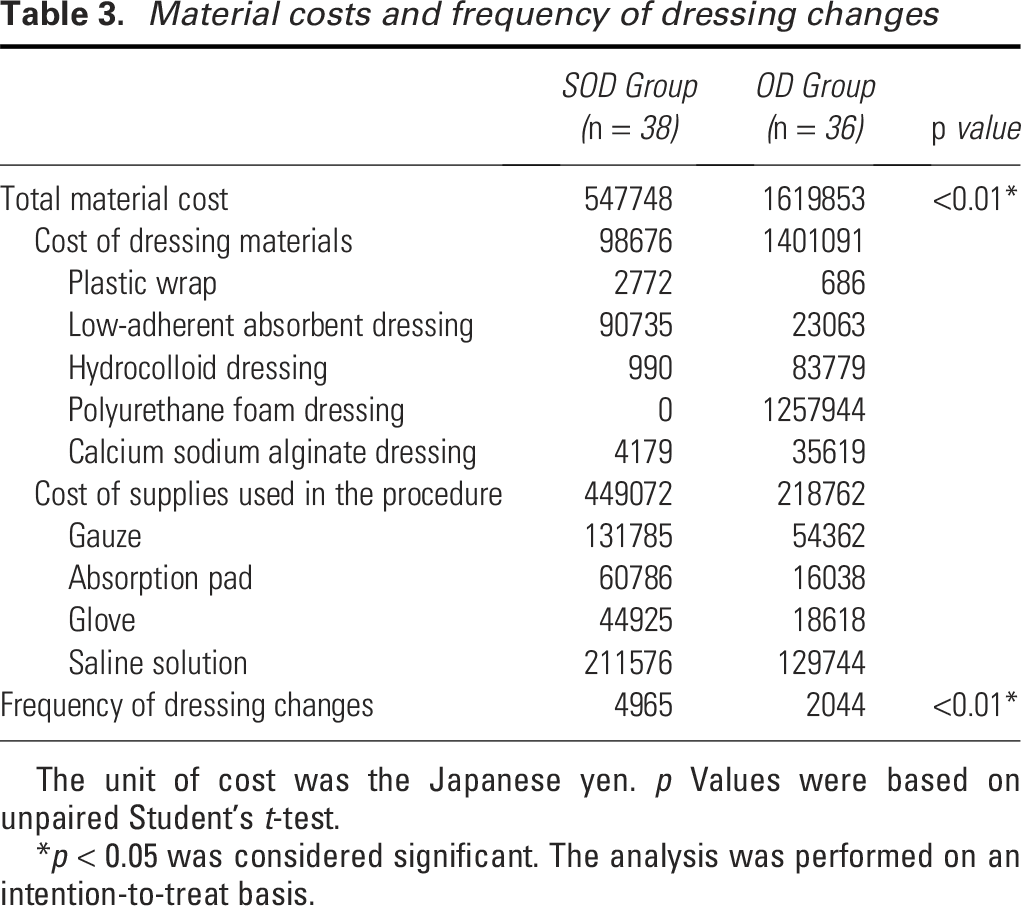
The unit of cost was the Japanese yen. p Values were based on unpaired Student’s t-test.
p < 0.05 was considered significant. The analysis was performed on an intention-to-treat basis.
DISCUSSION
By performing SAR and BWAT score reduction comparisons, this trial demonstrated that SOD treatment improved stage III/IV pressure injuries in the inflammatory phase faster than OD treatment. No apparent difference in the incidence of adverse events was observed between groups. In addition, SOD treatment was significantly less expensive than OD treatment. Many participants were older with poor general conditions, and some were terminally ill. Some patients had systemic illnesses that impeded wound healing. Infected wounds were included in this study. SOD treatment was beneficial for such patients often encountered in the clinical setting of pressure injury treatment.
Our results are in agreement with those of prior studies, including one randomized controlled trial, 6 one nonrandomized controlled trial, 5 and one comparative study of the same patient, 7 suggesting that SOD treatment is more effective than conventional treatment for stage III/IV pressure injuries in the inflammatory phase. The superiority of SOD over conventional treatment can be attributed to the difference in their treatment mechanisms. Because excess exudate drains outside the wound, SOD treatment can manage abundant exudate. Whereas with conventional treatment, the wound is occluded and dressing materials or ointments absorb the exudate, resulting in a limited amount of exudate that can be managed even though modern polyurethane foam dressings, which can absorb much exudate, are used. Unabsorbed excess exudate increases the intrawound pressure and deteriorates the wound.
Conversely, regarding treatments of mild pressure injuries, two randomized controlled studies3,8 and one comparative study of the same patient 7 showed no significant difference in the efficacy of SOD and conventional treatments. Because mild wounds do not typically generate abundant exudate and can be managed with conventional treatment, the effectiveness of both treatments may be equivalent for such wounds. Therefore, when conducting studies, deep wounds and shallow wounds should be considered separately, or results may be confusing.
Regarding the burden of medical practitioners, OD treatment was more advantageous than SOD treatment because fewer dressing changes were required. However, the caregiver workload required for SOD treatment was not high because the treatment procedure was simple. Changing dressings could be performed easily while providing other care, such as diaper changes and bathing. Moreover, frequent dressing changes, although burdensome, were also beneficial because they allowed more opportunities to observe wound conditions. Conversely, OD treatment required skilled medical professionals to select the type of dressings depending on the wound condition, which was not necessary with SOD treatment. In this respect, SOD treatment had an advantage over OD treatment.
SOD treatment can be easily implemented; however, the correct therapeutic procedures must be followed.9,10 Wounds could worsen attributable to improper treatment by medical practitioners who were unskilled in wound care or nonmedical professionals. 40 For example, severe wound infection occurred when the dressing material was not changed for several days, the wound was sealed by a food wrap, or wound infection in the early stages was not appropriately managed.
This study had some limitations. First, the small sample size limited the strength of evidence. It may have also introduced some bias, affecting the equality of the underlying background characteristics between the two groups and the results. Moreover, the significance of the differences in some endpoints, including the incidence of adverse events, may have been underestimated because of insufficient statistical power. Second, the labor cost was not considered when calculating the treatment cost. Arguably, the labor cost associated with SOD treatment was higher than that associated with OD treatment because of the frequency of dressing changes. However, because the time and effort required to change dressings are not great, the difference in the labor cost between groups may be insignificant. Finally, long-term safety was not investigated. As this study does not provide sufficient findings to confirm the effectiveness and safety of SOD treatment, further studies of more patients over longer periods are required.
Key Findings
SOD treatment was more effective and less expensive than OD treatment for NPIAP stage III/IV pressure injuries in the inflammatory phase.
The incidence of adverse events associated with SOD and OD treatment was comparable.
The crucial feature of SOD treatment is that the low-adhesive dressing incompletely occludes the wound and allows excess exudate to drain from the wound while a moist environment is adequately maintained.
INNOVATION
The SOD does not completely occlude the wound and allows excess exudate to drain outside the wound; thus, wound deterioration following increased intrawound pressure is prevented while a moist environment is adequately maintained to facilitate wound healing. Due to this unique and rational mechanism, the SOD can treat severe pressure injuries with abundant exudate effectively and safely. In addition, SOD treatment is easy to implement and inexpensive. Therefore, SOD treatment can be a useful option at medical facilities and patients’ homes.
ACKNOWLEDGMENTS AND FUNDING SOURCES
This work was partially supported by a research grant from Minakuchi Hospital (RGM2406 to JT) and Minamikusatsu Keyaki Clinic (MK2-2300011).
AUTHORS’ CONTRIBUTIONS
J.T., K.N., R.N., and H.H. collected the data; R.N. carried out the randomization; J.T., K.N., and R.N. analyzed the data; J.T. drafted the article; O.Y. and M.M. provided edits to the article; J.T., O.Y., and M.M. designed the study.
Footnotes
AUTHOR DISCLOSURE AND GHOSTWRITING
The authors declare no financial interests or no conflict of interest to disclose. No ghostwriters were employed.