
Abstract
Significance:
Recent reports recognize transepidermal water loss (TEWL) as a critical objective parameter measuring clinical wound healing endpoint. At the site of wound repair, TEWL measures functional wound closure as marked by re-establishment of barrier function at the wound site. This review article addresses recent developments in clinical TEWL measurement in the context of human skin health and wound care. To that end, emphasis is placed on the review of registered clinical studies reported in ClinicalTrials.gov for which TEWL results have been posted or published.
Recent Advances:
The U.S. Food and Drug Administration (FDA) defines complete wound closure as the achievement of 100% re-epithelialization of the wound surface, with no detectable exudate, drainage, or need for wound dressing, as verified during two sequential clinical assessments conducted at least 14 days apart. Clinically, wounds may meet this current FDA-recommended clinical criteria for wound closure, yet not achieve functional wound closure which requires the re-establishment of barrier function at the site of repair. Such wounds are likely to recur. High TEWL posthealing predicts wound recurrence. Thus, TEWL measurement at the site of repair posthealing is emerging as a significant measurement of wound healing endpoint.
Critical Issues:
Appropriate clinical measurement of TEWL requires a basic understanding of the related technologies and their appropriate use. Such understanding will help achieve the necessary rigor and reproducibility in clinical measurement.
Future Directions:
Recent reports on the critical significance of TEWL in wound care open new horizons wherein TEWL is likely to have broader applications involving altered skin barrier functions, such as during aging and other factors that determine skin health. Evidence to support revisiting the FDA definition of wound closure to include restoration of barrier function at the site of closure is strong. Widespread adoption of TEWL in wound care practices to determine functional wound closure is anticipated.
Chandan K. Sen, PhD, FNAI
SCOPE AND SIGNIFICANCE
The U.S. Food and Drug Administration (FDA) defines complete wound closure as 100% wound surface re-epithelialization without discernible exudate, drainage, or dressing requirements, confirmed at two consecutive study visits two weeks apart. However, this definition does not account for the functional aspect of the closure or the restoration of barrier function. 1 Two independent studies,2,3 including the transepidermal water loss (TEWL) trial of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Diabetic Foot Consortium underscore the clinical significance of the re-establishment of barrier function at the site of wound closure. The earlier mentioned current FDA criteria for wound closure taken together with the requirement of re-establishment of barrier function at the wound site is referred to as functional wound closure.2,4–6 A wound site that is structurally closed, per FDA definition, but functionally open because of compromised re-establishment of barrier function may be viewed as an invisible wound. 7 Such invisible wounds will fail to retain body moisture and may allow pathogens and allergens to enter the body because of deficient skin barrier function. These invisible wounds can be detected by high TEWL.2,3,7 In addition to such clinical application, TEWL is used to understand numerous skin-related conditions.8–14 TEWL is the quantity of water vapor that diffuses across a fixed area of stratum corneum (SC) to the skin surface per unit time. 15 A probe is placed in contact with the skin surface to detect such water vapor density under controlled conditions. In this work, we review evidence on clinical measurement of TEWL with an emphasis on registered studies posted in ClinicalTrials.gov.
TRANSLATIONAL RELEVANCE
The notion of functional wound healing or closure originated from pre-clinical porcine studies wherein wounds subjected to biofilm infection were observed to fail to re-establish barrier function at the site of repair although structural closure was not affected. 16 Such preclinical observation was reproduced in follow-up clinical studies.2,3
CLINICAL RELEVANCE
Clinical evidence upholds the critical significance of functional wound closure. In patients failing to achieve functional wound closure, TEWL readings are higher at the site of closure. Such closed wounds are likely to recur.2,3 Wound recurrence is a major public health burden. TEWL measurements at the site of wound repair will help detect incomplete functional wound closure, justifying additional care toward wounds that close and remain closed.
This work compares different types of TEWL measuring devices: open chamber (e.g., Tewameter, DermaLab), closed chamber (e.g., Vapometer), and condenser chamber (e.g., AquaFlux). Understanding such technologies and their optimal use will improve the rigor and reproducibility of clinical TEWL measurements. Current wound-recurrence-related TEWL data are from open chamber DermaLab equipment.2,3
BACKGROUND
Human skin is the largest organ intended to serve as a barrier against abiotic and biotic insults, including allergens and pathogens. 15 Comprising of four key components—physical, chemical, microbiological, and immunological—the skin barrier operates synergistically to regulate moisture levels, prevent dehydration, and protect against harmful pathogens. 17 Skin hydration plays a pivotal role, reflecting the water content within the SC—the outermost layer of the skin. Proper hydration is essential for maintaining skin barrier integrity and function. 13 A variety of methods are used to assess skin health in both clinical and research settings, each offering different levels of invasiveness and insight into skin properties. However, despite the availability of multiple assessment techniques, TEWL emerges as a widely adopted noninvasive tool in evaluating skin barrier function because of its ability to directly quantify the skin’s barrier function at the point of care.
TEWL is a vital parameter measuring the flux of water vapor through the SC before being released into the surrounding environment. 15 Unlike assessments of SC hydration, which focus on intrinsic skin moisture levels, TEWL offers insights into the skin’s capacity to retain moisture and uphold barrier function. This distinction is pivotal in comprehending the pathophysiology of dermatological conditions such as pressure ulcers and atopic dermatitis (AD), where disruptions in skin barrier function play a central role in condition progression.13,17 TEWL measurement typically expresses the release of water vapor in units of grams per square meter per hour (g·m−2·h−1).
TEWL devices measure skin barrier function by assessing time- and surface-dependent water evaporation, with different designs influencing accuracy, usability, and environmental sensitivity. Measuring devices can be characterized by three primary device architectures: open chamber, closed chamber, and condenser chamber configurations.18–20
Open-chamber devices feature a probe with unidirectional airflow, allowing ambient air to flow freely over the skin. They offer faster measurements, are less prone to occlusion effects, and are suitable for dynamic or uneven surfaces (e.g., wounds). However, they are also limited by their sensitivity to environmental factors such as air currents, humidity, and temperature fluctuations, requiring controlled conditions. The DermaLab TEWL probe (Cortex Technology) is an example of an open-chamber TEWL device.
Closed-chamber devices use a sealed chamber that traps vapor near the skin, measuring humidity changes over time. They are less affected by external air movement and more stable in variable environments. However, they also have a slower equilibration time and potential for occlusion artifacts if left too long on the skin. The VapoMeter (Delfin Technologies, Kuopio, Finland) is an example of a closed-chamber TEWL device.
Condenser-chamber devices incorporate a cooling element (Peltier condenser) to create a controlled microclimate, separating water vapor from air for precise measurement. These systems offer high accuracy and minimize environmental interference. On the contrary, they are more expensive, involve complex operations, and are slower than open-chamber systems. The AquaFlux (Biox Systems, London, England) is an example of a condenser-chamber TEWL device.
The open chamber provides faster measurements compared to the condenser chamber, which requires a longer equilibration time. These are most affected by airflow, whereas condenser-chamber devices are the least. Condenser chamber offers the highest precision, whereas closed chamber balances stability, ease of use, and practicality. Considering the effect size expected, the use of open-chamber devices may provide practical advantages for routine use in the clinical environment where rapid measurements are likely to be more widely adopted. TEWL measurement is noninvasive, making it practical and suitable for clinical and research settings. 20
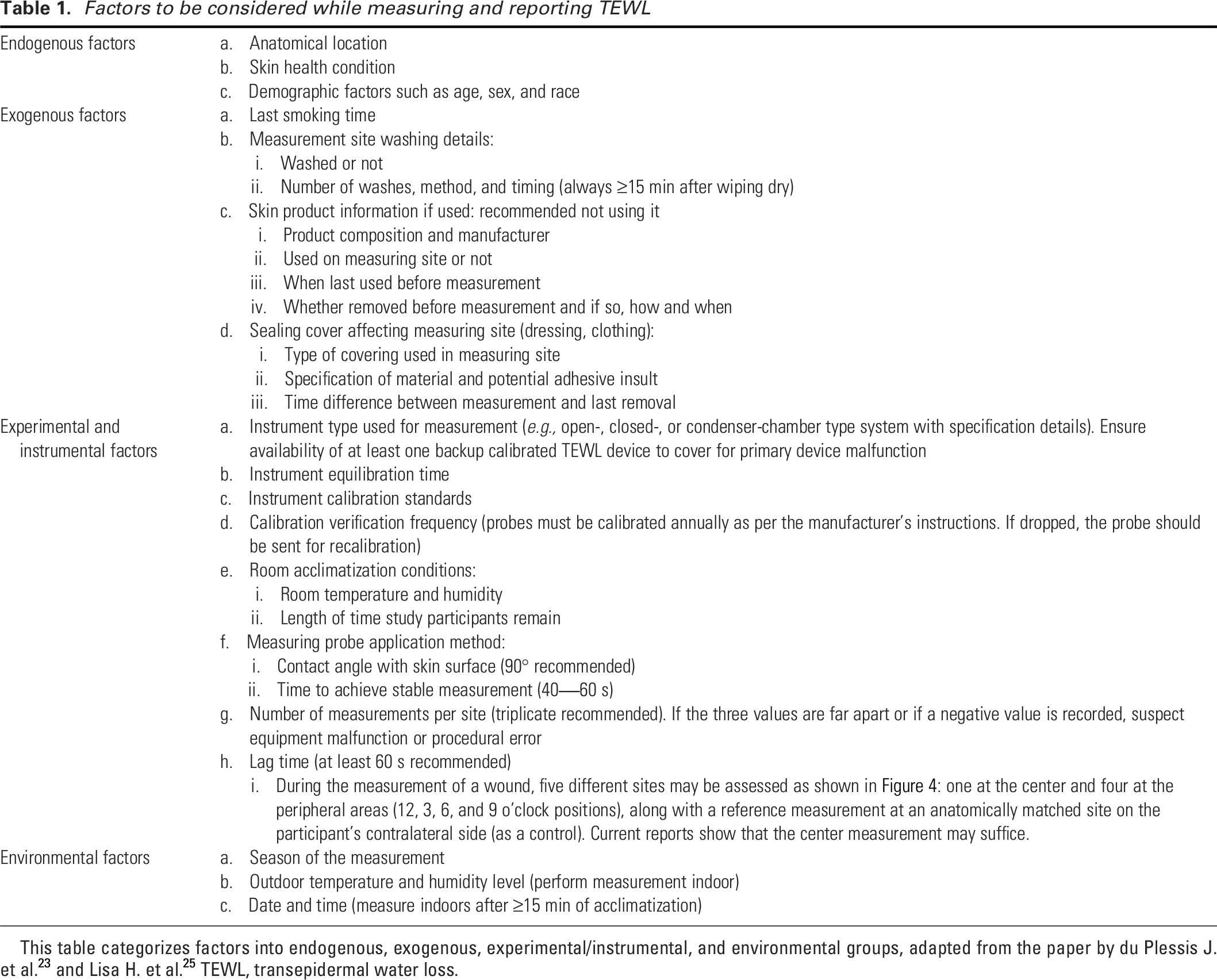
Absolute TEWL values may vary depending on the measurement system used thus, it is essential to report the specific type of device (e.g., open, closed, or condenser chamber) when presenting results.21,22 Compliance with the manufacturer’s standardized calibration protocols ensures accuracy and consistency across measurements. Standardization of variables such as room temperature, humidity, equilibration time, and measurement frequency enhances rigor and reproducibility. 23 If multiple skin barrier function parameters are to be collected, it is suggested that TEWL should be measured first, followed by other parameters to avoid any bias introduced by previous measurements. 24 Ideally, three measurements per site should be taken to establish the average value. The number of measurements per site and lag time between measurements should be standardized. Because of the high variability observed in TEWL measurements, repeated measurements are valuable.
To measure TEWL properly, meticulous consideration of several factors before and during measurement is imperative. Table 1 categorizes23,25 these factors into four groups for use as a clinical checklist: environmental, experimental and instrumental, endogenous, and exogenous. Among the environmental factors, the season of measurement holds significance, with winter typically associated with higher TEWL values because of low ambient humidity levels.23,26 TEWL rate is influenced by the humidity gradient between the skin and its surroundings, where water vapor moves from areas of high to low concentration, thereby increasing TEWL during low humidity winter conditions. Conversely, high humidity during summer facilitates water vapor influx into the skin, albeit the effect may be moderated by elevated temperatures.23,27 TEWL rate is also influenced by temperature and atmospheric pressure. 15 A positive association between atmospheric pressure and TEWL and conversely, a negative association between temperature and TEWL has been reported.15,28
Factors to be considered while measuring and reporting TEWL
Endogenous factors such as anatomical site and skin health significantly impact TEWL. Considerable variations in TEWL rates across anatomical sites have been reported by multiple groups (Fig. 1).9,17,30–43 These variations are attributable to factors such as eccrine sweat gland activity and occlusion.23,37 Skin health, as elucidated by Proksch et al., affects TEWL, with diseased skin exhibiting higher TEWL values, particularly evident in AD lesions.23,44 Age, sex, and race may also impact TEWL measurement. 23
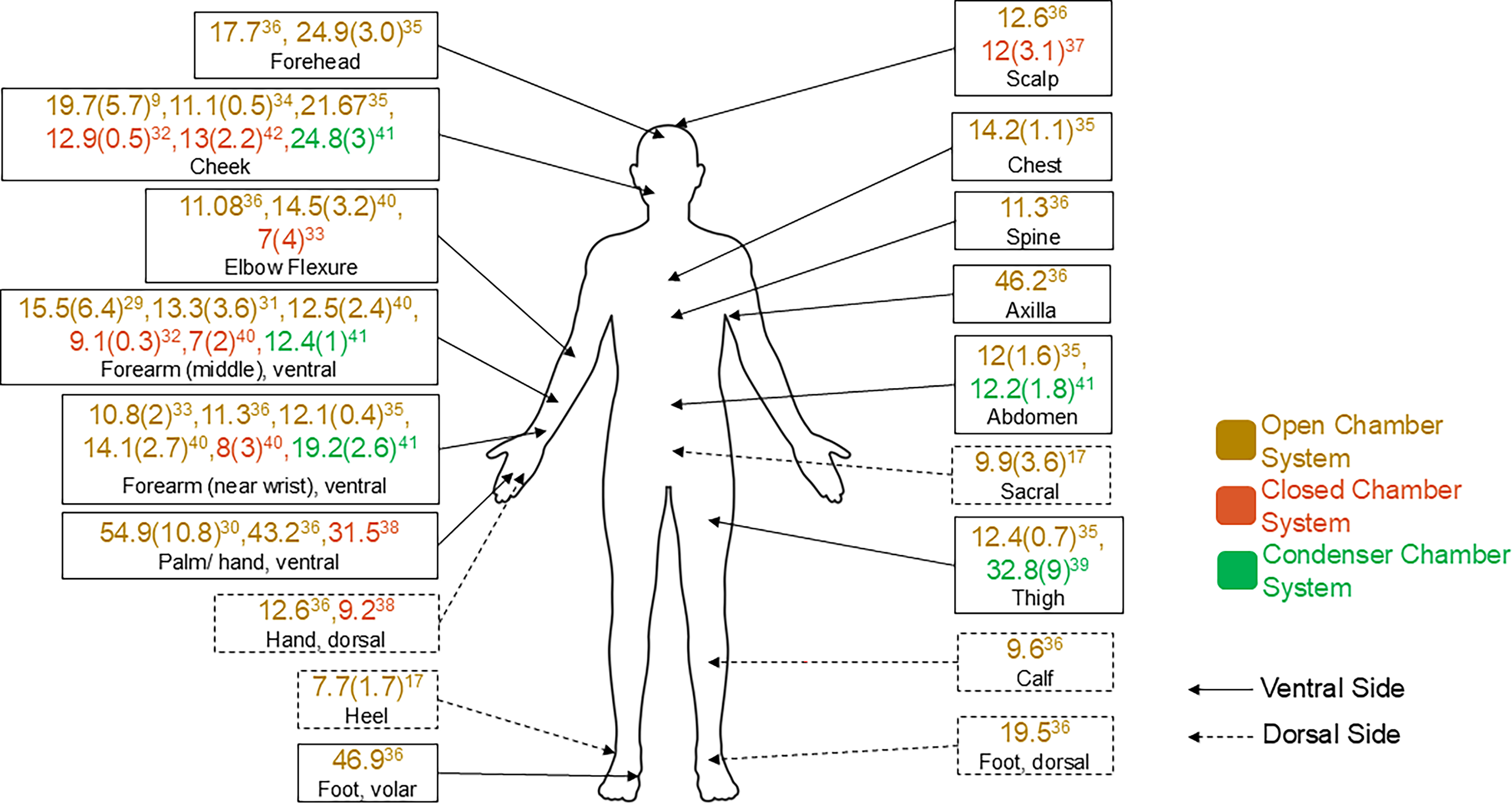
TEWL (g·m−2·h−1) at different anatomical locations in healthy adult humans. A search was conducted in the PubMed database using the keywords “TEWL” OR “Transepidermal Water Loss,” with the “Article Type” field set to “Clinical Trial” to identify relevant articles related to TEWL (last accessed: March 16th, 2025). The initial search yielded 784 articles, of which 726 were excluded by filtering out studies published before 2024, leaving 58 studies for screening. After manual screening, seven studies9,30–35 were included that met our predefined inclusion criteria by reporting baseline TEWL values (g·m−2·h−1) on healthy adult skin (between 18–65 years of age), with both the anatomical measurement site and the TEWL measuring device specified. These studies were categorized based on the type of TEWL measurement device used: open chamber, closed chamber, or condenser chamber. An additional nine studies17,36–43, identified through targeted searches and examination of reference lists that fulfilled the same inclusion criteria and were incorporated into the final review. Reported values represent the average baseline TEWL, and standard deviations are provided in parentheses where available. TEWL, transepidermal water loss.
Clinically closed wounds may not have fully re-established barrier function of the repaired skin as evident in patients who do not achieve functional wound closure.2,3 AD, acne, and other skin conditions are linked to compromised barrier function, increasing vulnerability to infections.
Exogenous factors such as smoking and stress may also influence TEWL. Elevated TEWL rates have been reported in smokers, which could be associated with oxidative damage to the epidermis.23,45,46 Environmental stressors cause oxidative damage, delay wound healing, and affect skin barrier function recovery.23,47 Procedural variables including skin washing frequency and skin product application may affect TEWL. Excessive soap usage may disrupt the skin barrier, incrementally increasing TEWL. Application of skin moisturizers may lower and mitigate TEWL.23,48,49 Different skin moisturizer and their ingredients can also influence TEWL, for example, sodium lauryl sulfate may increase TEWL as it is a recognized skin irritant.50,51 Abrasive surface contact with the skin, including textile, may raise TEWL. 52
METHODS
A review of ClinicalTrials.gov identified registered studies measuring TEWL (last accessed: March 16, 2025). We selected ClinicalTrials.gov for our analysis because these are registered studies representing a higher level of rigor compared to unregistered human studies. ClinicalTrials.gov is a large, internationally diverse dataset that reports comprehensive study details and inclusion/exclusion criteria for subject enrollment. We used the keywords “TEWL” OR “Transepidermal Water Loss” to find studies that included TEWL measurements (Fig. 2). Initially, we found 435 studies (Table 2). Using the “Study Results” field as a filter, we excluded 385 studies that had not posted results, leaving 50 studies with available results for record screening.
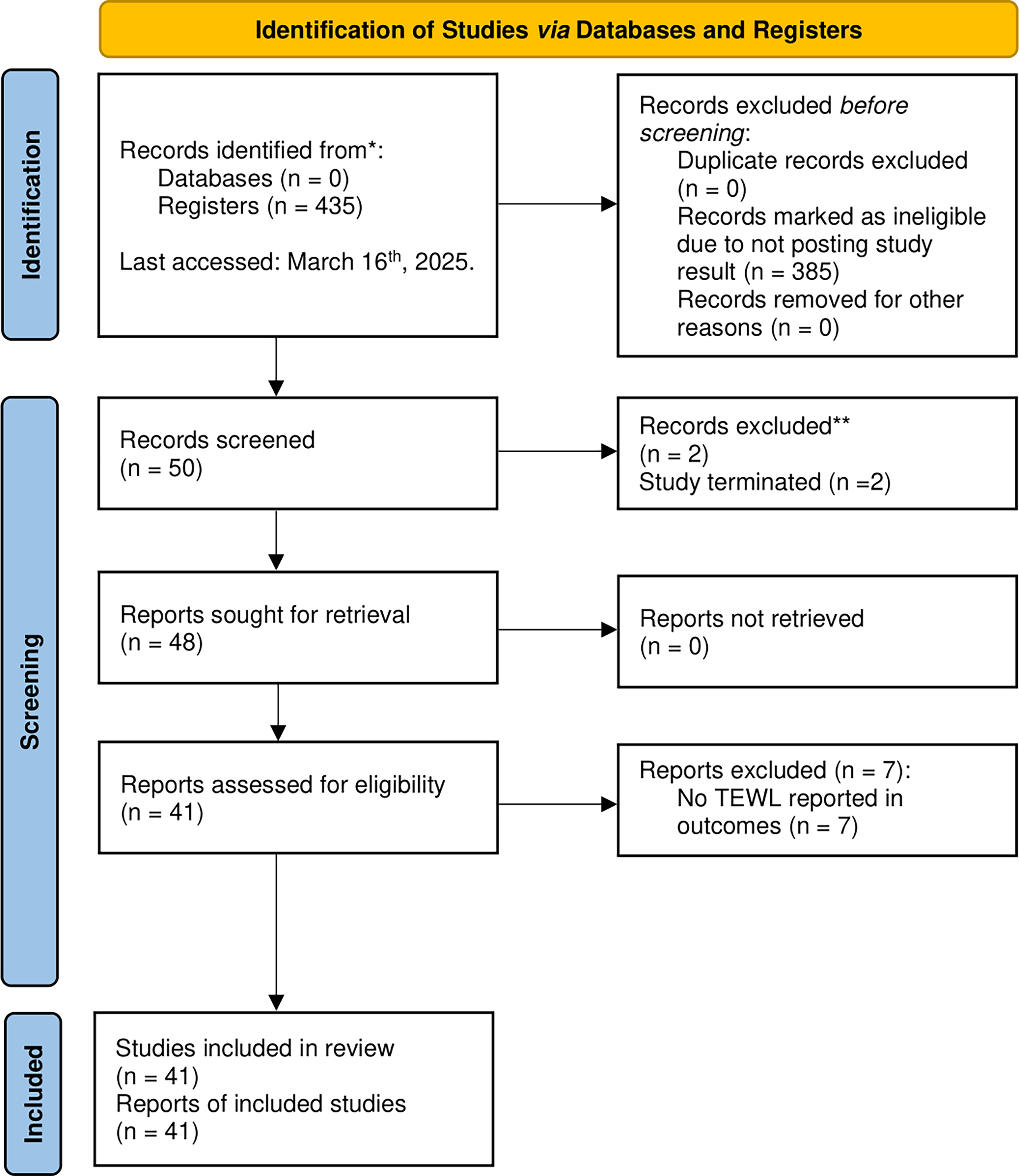
Systematic review flow diagram searched on ClinicalTrials.gov registers. The Preferred Reporting Items for Systematic Reviews and Meta‐Analysis (PRISMA) were used to guide the literature search and study selection process. A search was conducted on ClinicalTrials.gov to find studies relevant to TEWL. The search used the keywords “TEWL” OR “Transepidermal Water Loss” to identify studies incorporating TEWL measurements and last accessed on March 16th, 2025. Initially, 435 studies were identified (Table 2). Subsequently, the “Study Results” field was used as a filter to eliminate studies that had not posted their results, resulting in the exclusion of 385 studies and leaving 50 studies with results for further screening. During the initial screening, two clinical studies were found to be terminated and were therefore not included in the final analysis. In addition, seven studies were excluded for not including TEWL outcome measurements, leaving a total of 41 studies for full-text review. Below is the list of NCT numbers of the studies that are included in the review (n = 41): NCT06415292, NCT06034340, NCT05085730, NCT04718870, NCT04606134, NCT04559022, NCT04477187, NCT04447417, NCT04040933, NCT03927404, NCT03901144, NCT03804710, NCT03803059, NCT03743038, NCT03507036, NCT03370757, NCT03365934, NCT03332628, NCT03216265, NCT03197883, NCT03180645, NCT03119688, NCT03103906, NCT02930590, NCT02906566, NCT02839772, NCT02557698, NCT02216526, NCT02173054, NCT01963793, NCT01909713, NCT01856764, NCT01787461, NCT01375205, NCT01065714, NCT01015638, NCT00974480, NCT00964366, NCT00926367, NCT00819507, and NCT00097253. *To conduct the search for studies, the ClinicalTrials.gov register was used, using the search term “TEWL” or “Transepidermal Water Loss”. A total of 435 studies were identified and last accessed on March 16th, 2025. A supplementary list containing all NCT numbers for the total studies searched in ClinicalTrials.gov and the studies included in the review is provided. **After download, the study status was sorted and a two studies with the “TERMINATED” designator were excluded.
NCT numbers of all TEWL-related studies registered in ClinicalTrails.gov (n = 435)
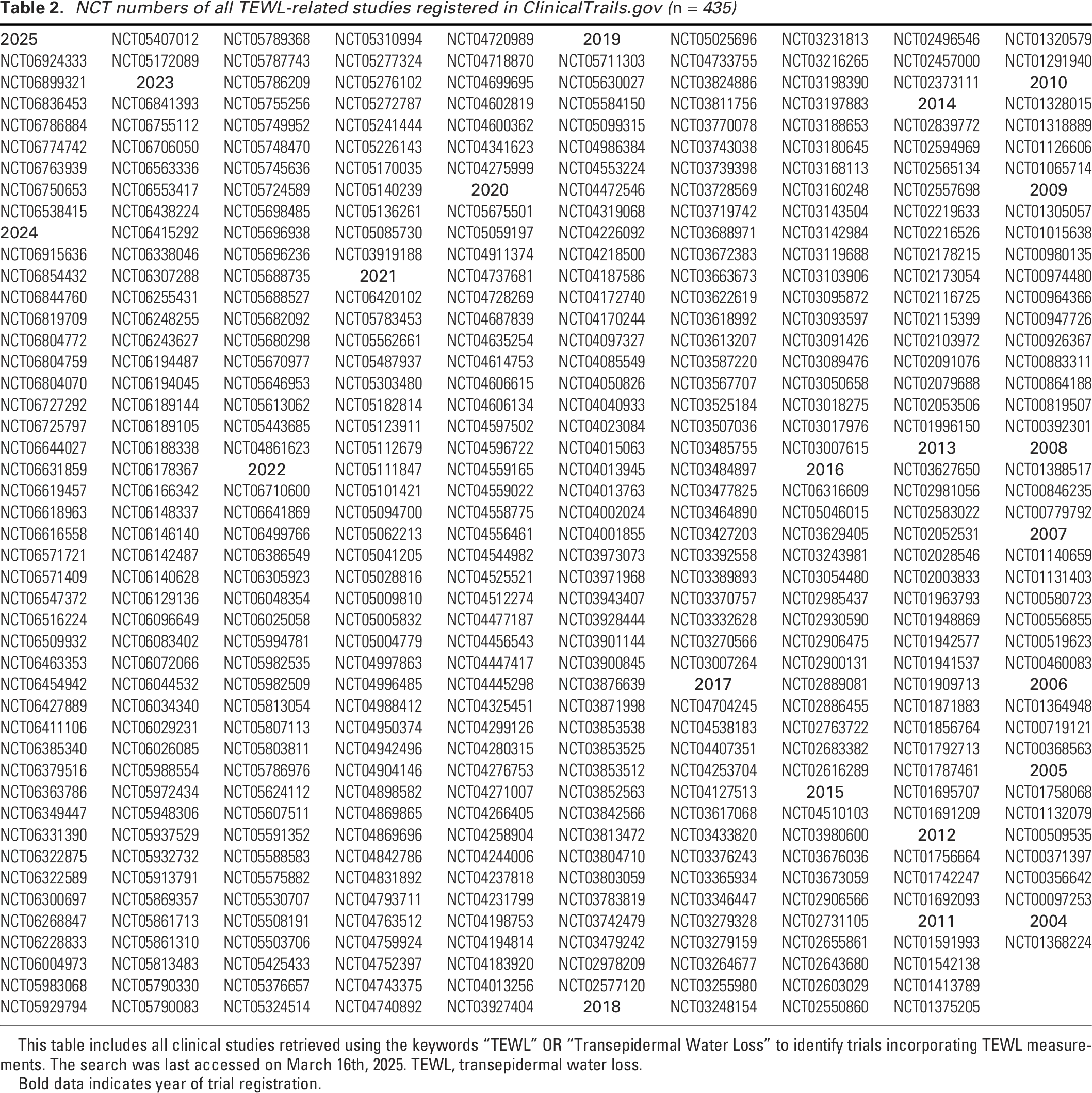
This table includes all clinical studies retrieved using the keywords “TEWL” OR “Transepidermal Water Loss” to identify trials incorporating TEWL measurements. The search was last accessed on March 16th, 2025. TEWL, transepidermal water loss.
Bold data indicates year of trial registration.
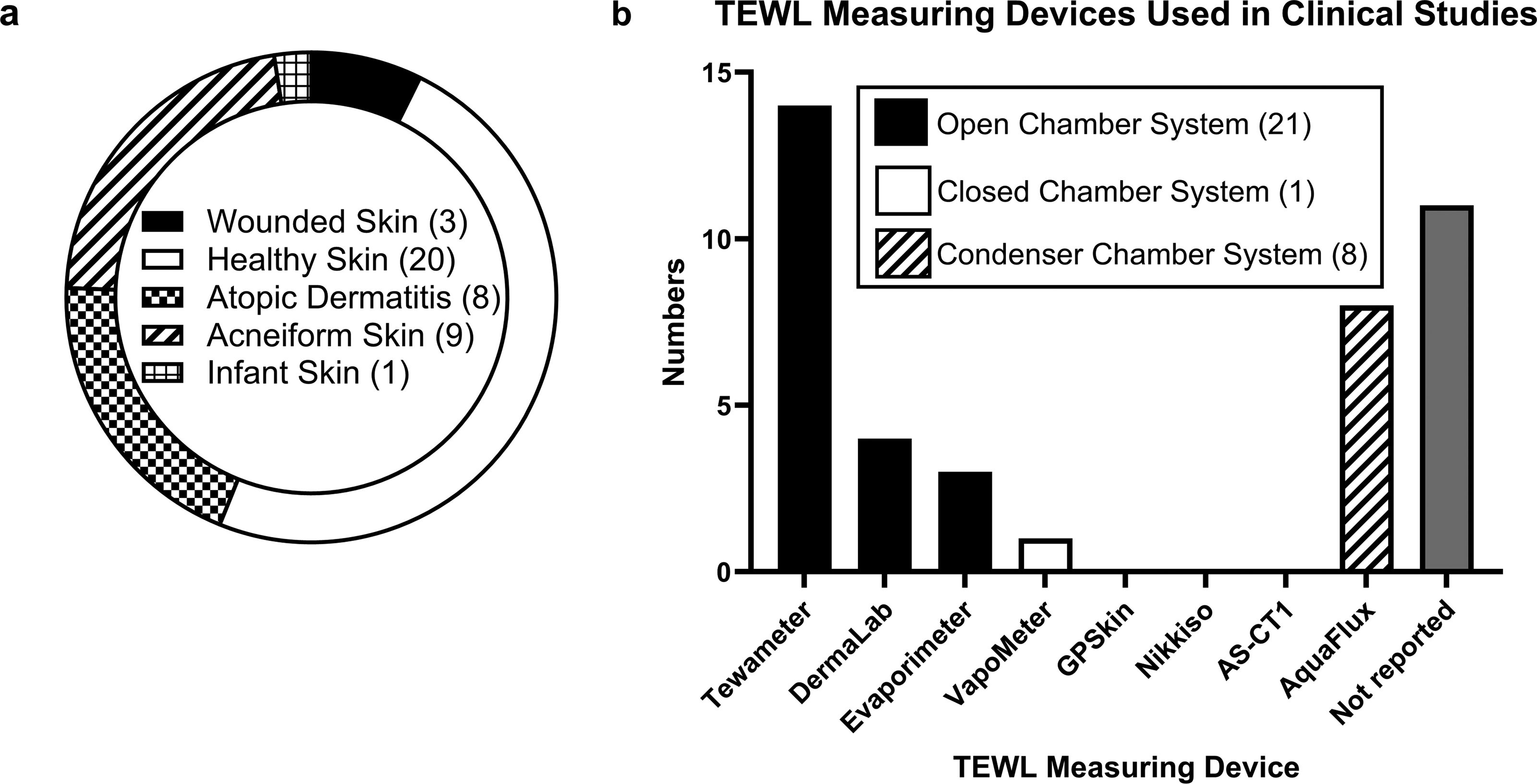
During the initial screening, we identified the clinical studies NCT03389893 and NCT04793711 related to AD skin; however, both trials were terminated and therefore excluded from our final synthesis. We excluded the following trials because TEWL results were not reported: NCT03255980, NCT00371397, NCT03622619, NCT00580723, NCT01941537, NCT03243981, and NCT00519623. Finally, 41 studies were included for full-text review in this work. These 41 studies were manually divided into five main groups based on their Study Details and Results Overview sections: (1) Wounded Skin; (2) Healthy Skin; (3) Atopic Dermatitis Skin; (4) Acneiform Skin; and (5) Infant Skin. The number of studies in each group is illustrated in Figure 3a. In addition, we categorized the studies by device type. Such categorization and division of the devices are illustrated in Figure 3b.
ClinicalTrial.gov studies categorized by type of
DISCUSSION
Figure 3 categorizes the studies by five major skin study groups and the devices used for measuring TEWL. Devices are further categorized into one of three operating modes: (1) Open Chamber System (n = 21); (2) Closed Chamber System (n = 1); and (3) Condenser Chamber System (n = 8), including the device names. Among the 41 studies, 30 specified the TEWL measuring device type and name, whereas 11 did not.
The wounded human skin
A wound in the skin is a structural and functional defect. Compared to healthy skin, which has an intact SC that serves as a barrier to protect underlying tissues and prevent water loss, wounded skin has compromised barrier function manifested as increased TEWL.53,54
Open-chamber device
Studies NCT04040933 55 and NCT02930590 56 measured TEWL using an open-chamber Tewameter device. Study NCT04040933 55 tested the wound healing efficacy of different adhesive bandages. The TEWL probe was held in place on the skin for one measurement, for 40 s, to ensure that a stable value had been established. The values of the last 10 s were averaged as the actual measurement values. Minor wounds were induced in different sections of the forearm using a laser. The recorded TEWL value at wound sites was 39.27 (±8.240 standard deviation [SD]) g·m−2·h−1. This analysis included 36 participants, and TEWL measurements were recorded over a 14-day period.
NCT0293059056,57 focused on evaluating the effects of different wound care products on wounds caused by pressure ulcers. Pressure ulcers represent severe injuries that significantly impact patients, caregivers, and healthcare systems globally. Effective prevention is crucial for maintaining skin and tissue integrity in individuals at risk. The relationship between the type of support surface and skin function after pressure application can help characterize and quantify the performance of these surfaces in protecting the skin. This exploratory study sought to measure skin responses at two common pressure ulcer sites, heel and sacral skin, after 2 h of loading on three different support surfaces. Sternal skin served as a control area. The study compared an alternating low-pressure mattress, a reactive support surface (gel mattress), and a standard mattress (basic foam). TEWL was measured using Tewameter TM300. The reported average TEWL values at the sacrum for the standard mattress were: 7.1 (6.8–8.8) g·m−2·h−1 at baseline, 14.5 (9.3–20.5) g·m−2·h−1 after 2 h of loading (p = 0.105, method: Friedman test), and 8.0 (6.8–9.0) g·m−2·h−1 20 min after off-loading. At the heel, the values were 8.6 (7.4–12.1) g·m−2·h−1 at baseline, 28.4 (15.9 to 32.3) g·m−2·h−1 after 2 h of loading (p = 0.155, method: Friedman test), and 11.1 (9.9–14.8) g·m−2·h−1 20 min after off-loading. It is thus evident how 2 h of loading changes TEWL values. Notably, the study showed that the alternating low-pressure mattress consistently exhibited lower TEWL levels compared to the reactive support surface and standard mattress, particularly after loading periods. These data sets support the use of alternating low-pressure mattresses to defend skin barrier integrity and moisture retention in elderly individuals.
The clinical study on TEWL biomarker study for diabetic foot ulcer (DFU) recurrence (TEWL) (NCT04558775 58 ) used a standardized protocol for measuring TEWL in wounds, using a multimeasurement technique illustrated in Figure 4. Triplicate TEWL measurements were taken at each individual point and four equidistant points at 12 o’clock (blue), 3 o’clock (red), 6 o’clock (green), and 9 o’clock (yellow), with one additional measurement in the middle of the closed wound site (center) marked by gray. The lag time between measurements was kept consistent throughout to ensure uniformity. The NIDDK Diabetic Foot Consortium TEWL Study found that DFUs appeared clinically closed but were deficient in the restoration of the skin barrier, exhibiting elevated TEWL at the wound site. DFU recurrence by week 16 occurred in 21.5% of participants. These closed wounds with higher TEWL levels were significantly associated with a greater risk of recurrence (p = 0.006). These findings demonstrate that TEWL measurement may serve as a valuable clinical tool for predicting DFU recurrence. TEWL may also be productive in measuring functional wound closure endpoint. 3 An exploratory observational pilot study 2 (CTRI/041766) studied diverse wound types to evaluate whether postclosure TEWL could serve as a functional biomarker for predicting chronic wound recurrence. It was reported that 39% of closed wounds recurred within 12 weeks. Wounds with higher post-closure TEWL values were significantly more likely to recur. A TEWL cutoff value of 24.1 g·m−2·h−1 was identified as predictive (AUC = 0.967) of recurrence with high sensitivity (92.8%) and specificity (90.9%). 2 These studies used the DermaLab open-chamber device to measure TEWL. Taken together, these findings open a new paradigm in wound care underscoring the significance of achieving functional wound closure. These studies highlight the clinical significance of post-closure TEWL measurement as a functional wound closure endpoint.
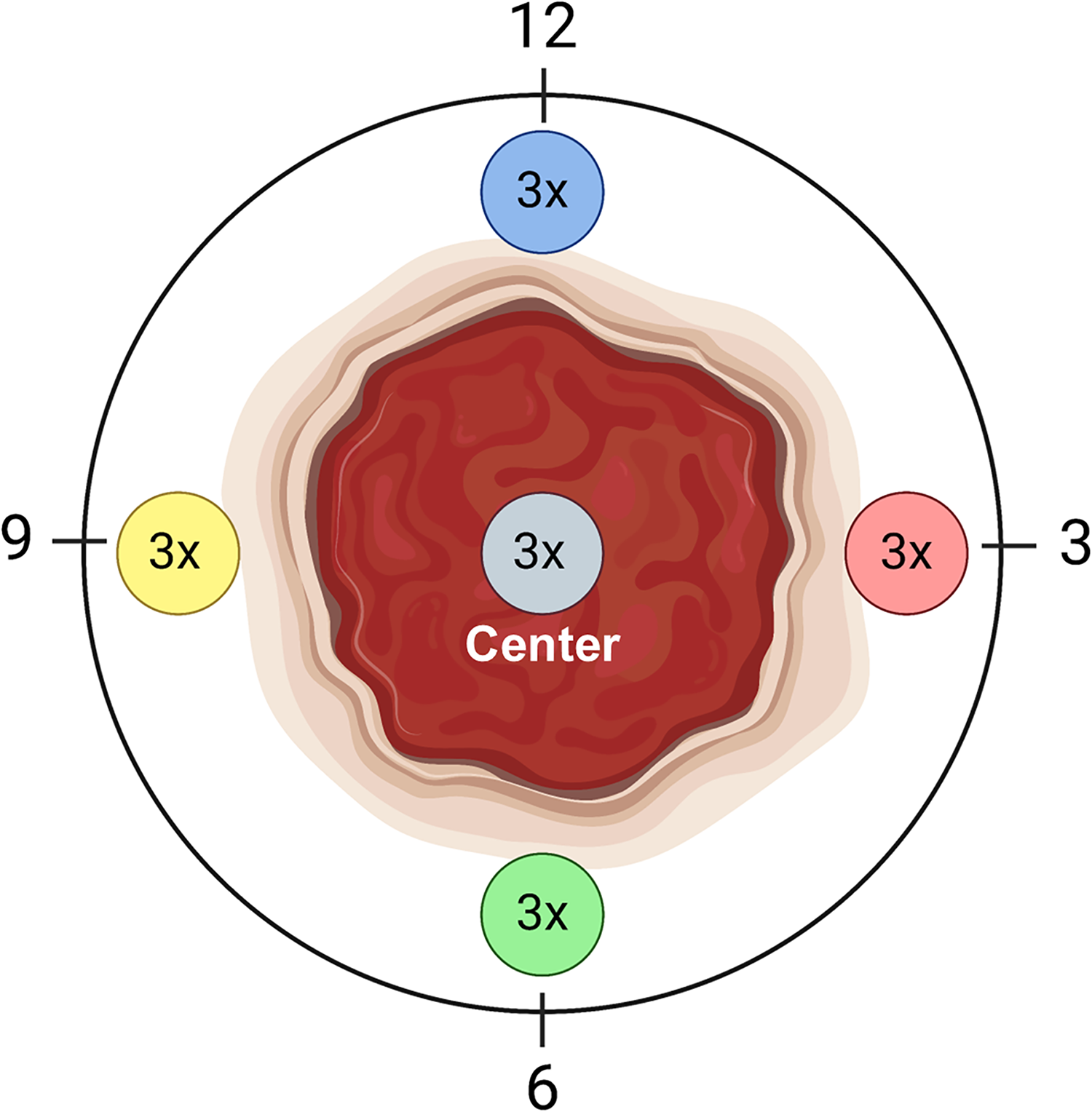
Post-closure wound TEWL measurement. The wound shown is where the wound was pre-closure based on historical clinical photo records. Each individual point and four equidistant points were subject to three consecutive TEWL measurements. These points were marked at 12 o’clock (blue), 3 o’clock (red), 6 o’clock (green), and 9 o’clock (yellow), with an extra measurement conducted at the midpoint of the wound, indicated by gray. Consistency in the lag-time between measurements was maintained to ensure uniformity. Illustrated using BioRender.com. TEWL, transepidermal water loss.
NCT03365934 59 aimed to assess changes in the skin microbiome of tape-stripped wounds for different adhesive bandages. Although the type of device used for measuring TEWL was not reported, the study found differences in TEWL measurements between wounded uncovered skin (96.94 ± 11.68 g·m−2·h−1) and intact skin (9.82 ± 6.72 g·m−2·h−1), as well as varying impacts of the tested products across the 14-day period in 35 human participants. On day 14, the TEWL value of wounded uncovered skin was 14.58 ± 13.01 g·m−2·h−1, whereas the third test product showed a lower TEWL value of 10.07 ± 4.16 g·m−2·h−1 (p = 0.005, method: ANCOVA), demonstrating product efficacy.
Healthy skin
Moisturizers are likely to play a role in maintaining and improving the skin barrier function in healthy skin.51,60,61 Current reports claim that moisturizers are effective in enhancing skin hydration, restoring the lipid barrier, and reducing TEWL. 62 By increasing water content in the SC and improving skin elasticity, in certain conditions, moisturizers may help to repair the skin barrier and prevent water loss, ultimately leading to softer, smoother, and more resilient skin. Whether such effects are directly because of the moisturizer itself as a physical barrier or improvement of the skin’s barrier function, or a mixture of both needs rigorous mechanistic studies. Active ingredients contained in skin moisturizers may be classified into three main categories: humectants (e.g., glycerin, panthenol), which draw and bind water; occlusives (e.g., petrolatum, lanolin), which prevent excessive water loss and maintain hydration; and emollients (e.g., fatty acids, ceramide), which smoothen and soften skin. In addition, additives such as vitamins or antioxidants are often included in the formulation of moisturizers.63,64 These ingredients are likely to work together to keep the skin hydrated and healthy. 65
Topical applications of moisturizers, creams, or gels are commonly used to enhance skin health and strengthen the skin barrier function. 66 In such studies, TEWL is tested as the primary outcome. Based on the type of device used to measure TEWL, values recorded in these studies from different anatomical positions of the human body are discussed below.
In the human foot, basal TEWL is different between plantar (sole) and dorsal surfaces.67–69 The plantar surface is thick, tough, and built to withstand a lifetime of pressure. With a SC up to 30 times thicker than the dorsal (top) foot, the sole acts like a biological fort, trapping moisture inside. The plantar skin is rich in ceramides and cholesterol, which form a watertight seal, lowering basal TEWL (<10 g·m−2·h−1). Though the sole has more sweat glands, the constant occlusion from ground contact and footwear keeps TEWL surprisingly low. The dorsal skin is thinner, softer, and far more prone to water loss. With a SC thickness closer to forearm skin, the dorsal foot allows 2–3 times more TEWL (15–25 g·m−2·h−1). Unlike the sole, the dorsal foot’s lipid matrix is less fortified, making it more vulnerable to dryness in low humidity.
Open-chamber device
Twelve studies have been reported using open chamber devices to record TEWL data. The studies NCT03103906 70 and NCT03197883 71 compared the effectiveness of moisturizers (such as moisturizing cream with sun protecting factor and a moisturizing facial cleanser) applied twice daily, versus a control group using only water and a small amount of facial cleanser. Measurements were performed in triplicate on the left cheek (below the cheekbone between the nose and ear) using a Tewameter device. TEWL measurements were performed with the participant lying horizontally on their back so that the probe was placed vertically to the skin surface. The reported baseline TEWL values at the cheek were 20.20 (±5.158 SD) g·m−2·h−1 and 20.22 (±6.181 SD) g·m−2·h−1, respectively.
Studies NCT03119688 72 and NCT0321626573,74 assessed the mean TEWL value difference between tested cosmetic products (such as Olay ProX cream) versus a control group at the volar forearm. During their TEWL measurement, the probe was held in place on the skin perpendicular to the skin for one measurement, for approximately 40 s to ensure that a stable value had been established using the Tewameter open-chamber device. The first part of the measurement belonged to the equilibration phase. The values of the last 10 s were averaged as the actual measurement values.
NCT0318064574,75 examined the effects of different treatments on TEWL in the sub-ocular/cheek area over 29 days. Measurements were taken in triplicate, and an average (mean) reading was calculated using Tewameter TM300. The TEWL probe was placed perpendicular to the skin. Three groups were compared: a test product (biomimetic lamellar cream formulation), a commercial moisturizer (positive control, Olay ProX cream), and a no-treatment group. Mean TEWL reductions compared to baseline were observed: −5.18 (±3.71 SD) g·m−2·h−1 for the test product, −6.62 (±5.79 SD) g·m−2·h−1 for the positive control, and −3.00 (±4.56 SD) g·m−2·h−1 for the no-treatment group (p = 0.0230, test product vs. no treatment group).
NCT00974480 76 evaluated the impact of different skincare treatments on TEWL measured on the human face over 24 weeks. Measurements were performed with the subject lying down on the back in a room with controlled temperature (20 ± 2°C) and relative humidity (45 ± 15%). All measurements were performed at least 30 min after the subject was transferred into a room equipped with a DermaLab device. Three treatment groups—Redermic, Rejuva-A, and a combination of both—were compared. At week 24, the Redermic group had the lowest mean TEWL (10.20 ± 3.12 g·m−2·h−1), followed by the combination group (12.45 ± 4.47 g·m−2·h−1) and the Rejuva-A group (12.64 ± 6.00 g·m−2·h−1).
NCT01787461 77 compared the effects of the Imedeen supplement against a placebo, measuring TEWL at the cheek (baseline TEWL: 11.7 ± 5.27 g·m−2·h−1) over 24 weeks. NCT0255769878,79 tested the efficacy of skin oil. Means of triple measurements per skin area are measured using the Tewameter TM300 device. The reported mean TEWL at the left mid-volar forearm was 11.9 g·m−2·h−1, and at the right lateral lower leg it was 11.0 g·m−2·h−1. NCT03804710 80 tested the efficacy of two different types of developmental moisturizing cream applied to the human leg. The probe was held in place on the skin for 40 s to ensure that a stable value had been established. TEWL values were measured using the Tewameter TM300, and the values of the last 10 s were averaged as the actual measurement values. Reduction in TEWL of −5.077 g·m−2·h−1 was noted compared to standard cleanser reduction which was −3.692 g·m−2·h−1. NCT00097253 81 assessed the impact of odor-based skin oils (lavender and lemon) versus water (placebo). This study observed no significant (p = 0.60, method: mixed models’ analysis) TEWL differences between the placebo and test groups. NCT0221652682,83 compared Cetaphil® Restoraderm body wash with standard skincare and reported mean changes in TEWL at the lower leg using Tewameter TM300, from baseline to 8 weeks. TEWL increased by 1.8 g·m−2·h−1 in the test product group, which was not significantly different than the increase observed in the standard care group at 3.4 g·m−2·h−1 (p = 0.267, method: Kruskal–Wallis test). NCT03927404 2 evaluated residual limb circulation and skin health associated with the use of a prosthetic vacuum socket. TEWL was measured employing the DermaLab device. The reported value compared the ratio of the TEWL of the residual limb over the TEWL value of the sound side limb, which was 1.69 median, and the interquartile range was (1.12–2.85, p < 0.05).
Closed-chamber device
NCT0283977284,85 investigated the effects of different interventions on TEWL as an indicator of skin barrier function. Participants underwent daily washing, soaking, and application of topical agents to the legs and feet over three months. In the control group (standard intervention), TEWL decreased at the top of the outer lower legs, from 12.74 ± 4.73 SD g·m−2·h−1 to 8.76 ± 2.63 SD g·m−2·h−1 for the right leg; and from 13.52 ± 5.61 SD g·m−2·h−1 to 9.09 ± 2.63 SD g·m−2·h−1 for the left leg. Single TEWL measures were recorded using a VapoMeter closed-chamber device. Patients were asked to rest and equilibrate for at least 20 min with measurement sites exposed. This process was supported by the automatic recording of ambient temperature and humidity by the closed chamber device. The experimental group received a modified intervention that included glycerin, showing greater reductions in TEWL. At the same measurement point, TEWL decreased from 13.43 ± 5.56 SD g·m−2·h−1 to 7.06 ± 1.96 SD g·m−2·h−1 for the right leg and from 13.27 ± 4.91 SD g·m−2·h−1 to 7.53 ± 2.12 SD g·m−2·h−1 for the left leg (groups: control, experimental, p < 0.001, method: mixed model analysis). The application of glycerin was thus effective in lowering TEWL. How long such beneficial effects persist remains to be seen.
Condenser-chamber device
NCT05085730 86 evaluated a bipolar fractional radiofrequency device. TEWL consistently decreased from baseline to 3- and 6 months post-treatment of facial skin-baseline: 26.16 ± 4.97 SD g·m−2·h−1; month 3: 22.51 ± 6.87 SD g·m−2·h−1; month 6: 18.08 ± 2.81 SD g·m−2·h−1.
NCT03507036 87 evaluated the effectiveness of a similar device on suprapatellar skin. It reported a baseline TEWL value of 9.37 ± 2.05 SD g·m−2·h−1 at the suprapatellar region. NCT04477187 88 and NCT0380305989,90 reported baseline TEWL values of 14.084 ± 3.82 SD g·m−2·h−1 of facial skin and 15.56 ± 6.72 SD g·m−2·h−1 at neck, respectively. The exact face anatomical location is not reported in those studies. All these studies reportedly used AquaFlux condenser-chamber devices.
Unknown devices
NCT03332628 91 evaluated skin recovery following microneedle treatment in healthy subjects. NCT06034340 92 assessed the efficacy of a test-numbing gel (lidocaine-epinephrine-tetracaine) by comparing the percentage change in TEWL on the forearm between the test and control groups. Neither study specified the TEWL measuring device used, thus limiting reproducibility and comparison across studies.
NCT02906566 93 investigated the effects of retinol versus placebo treatment on TEWL in older participants, aged 55–75 years. Although the study reported a baseline TEWL value of 17.1 ± 10.2 SD g·m−2·h−1 on arm skin, it did not specify the device used for measurement.
TEWL studies of skin pathologies
Based on follow-up duration, TEWL studies may be split into these groups: short follow-up time, 2 weeks or less,29,70–72,94–98 between 2 weeks to 1 month,73,75,78,80,91,99–101 between 1 month to 3 months,81,82,84,89,93,102–104 and between 3 months to 12 months.76,77,86–88,105–107 Many of these studies included more than 50 participants.70,71,73,75–78,80–82,84,91,97,98,104–106 Six studies involved participants under 18 years of age,94,96–98,105,107 and five studies included participants over 65 years of age,82,84,87,93,94 while the remaining studies were on adults between 18 and 65 years of age. In addition to TEWL measurement, skin hydration,76,82,84,91,94,105 skin dryness,70–72,82,96–100,104 skin surface roughness,75,78,86,89 skin elasticity,76,87,88 skin erythema,101,108,109 skin surface pH,82,105 melanin content, 103 skin color, 87 skin laxity, 87 and epidermal and dermal thickness 87 were used to evaluate skin condition.
Atopic dermatitis
AD is a chronic disease that causes inflammation, redness, and irritation of the skin.110–112 It affects one in ten individuals throughout their lifetime. It has a prevalence of up to 3–4% of adults and up to 25% among children.110,111,113 The condition arises from a complex interplay of factors including immune dysregulation, genetic mutations within the epidermis, and environmental triggers, leading to disruptions in the skin barrier function. This disruption manifests in intensely itchy skin lesions, which, when scratched, initiate a self-perpetuating itch-scratch cycle. Consequently, this cycle can significantly impact the patient’s quality of life. 114 The distribution of AD lesions varies with age. In infants, the condition predominantly affects the face, neck, and shoulders, whereas in teenagers, it commonly occurs on the elbows, knees, neck, and ankles. Among adults, affected areas typically include hands, neck, elbows, knees (particularly in skin folds), skin around the eyes, ankles, and feet.
Understanding TEWL in the context of AD is of direct clinical value. AD involves a compromised epidermal barrier. Effective treatment hinges on restoring this barrier function. However, many topical medications and vehicles like 0.5% roflumilast cream, Vanos cream, Cetaphil Restoraderm, topical cream (2% urea, 20% glycerol), aprepitant 10 mg/gel commonly used in treatment may inadvertently exacerbate barrier impairment. Therefore, there is a pressing need to investigate and compare the impact of various vehicles on epidermal barrier maintenance in individuals with AD. 115 TEWL measurement is valuable in this regard. TEWL measurements conducted at the volar forearms showed significantly higher values at AD lesion sites (28.68 ± 14.28 g·m−2·h−1) compared with healthy skin (11.60 ± 7.78 g·m−2·h−1), with a p value <0.001. Measurements were performed using the Tewameter TM300 device. 13 TEWL values for AD patients are discussed below based on the type of TEWL device used.
Open-chamber device.
NCT01856764 29 compared the effects of 0.5% roflumilast cream with a placebo vehicle cream. At each visit, three measurements of TEWL were taken per treatment area (at 3 different areas of the target lesion) with a Tewameter device. The average of these measurements represented the final TEWL value at each visit. TEWL reduction achieved in response to 0.5% roflumilast cream (−18.60 ± 2.46 SD g·m−2·h−1) versus vehicle cream (−12.69 ± 2.41 SD g·m−2·h−1) was comparable (p = 0.095).
NCT0106571494,115 evaluated skin barrier function in AD patients by measuring TEWL at targeted lesion sites. The average of three sequential readings was taken at a minimum of one-minute intervals on the targeted affected area of the body using a Tewameter TM300. Participants were divided into two groups. One received Eucerin lotion, while the other used a hydrogel vehicle. The Eucerin lotion group showed a median TEWL change of 21.4% (ranging from −66.8% to 214.8%), whereas the hydrogel vehicle group showed a median change of 4.2% (ranging from −76.9% to 57.9%).
NCT0081950795,116 assessed the efficacy of Vanos cream (fluocinonide 0.1%), a glucocorticoid cream, over 2 weeks in 25 participants. Two measurements per site were performed and reported at baseline lesional skin 31.33 ± 14.82 g·m−2·h−1 and nonlesional skin 11.84 ± 4.74 g·m−2·h−1. TEWL reduced by −14.35 ± 16 g·m−2·h−1 (p < 0.001) after 2 weeks at lesional skin. However, anatomical lesion locations were not consistently reported across these studies.
Condenser-chamber device.
NCT03901144102,117 compared glycerol cream, paraffin cream, and urea—glycerol cream in AD. TEWL reported after 31 days of studies were 19.790 ± 13.860 SD g·m−2·h−1 treated with urea—glycerol cream and 28.646 ± 13.668 SD g·m−2·h−1 (p < 0,001, method: ANCOVA) for the untreated area, respectively, at the volar forearm, collected from an AquaFlux device. This value is around double the TEWL reported for volar forearm in healthy individuals87,92,114 highlighting disrupted skin barrier function associated with AD.
NCT01375205 105 compared Cetaphil Restoraderm with Johnson & Johnson products as part of standard skin care in infants. Over a 12-month period, TEWL values were measured as an indicator of skin barrier function, using an Aquaflux device. In the Cetaphil Restoraderm group, TEWL decreased from 16.3 ± 7.1 SD g·m−2·h−1 (month 2) to 13.9 ± 2.3 SD g·m−2·h−1 (month 12). In the standard of care group, TEWL decreased from 18.3 ± 8.6 SD g·m−2·h−1 (month 2) to 16.7 ± 5.6 SD g·m−2·h−1 (month 12).
Unknown devices.
NCT01963793 103 evaluated the Aprepitant gel product on lesional skin. They reported a baseline TEWL value of 20.6 ± 13.6 SD g·m−2·h−1, which was marginally lower (19.4 ± 13.2 SD g·m−2·h−1) on day 42 of treatment, indicating no improvement in skin barrier function. The type of TEWL device used for measurement was not specified. Similarly, studies NCT04447417 106 and NCT04718870 107 also reported TEWL percentage change outcomes related to the effects of Dupilumab but did not mention the specific TEWL measuring device used in their protocols. These two studies followed up for 112 and 197 days, respectively, demonstrating large TEWL differences (33–54% reduction in TEWL) between baseline and end of the study in the lesional skin.
Acneiform skin
Acne vulgaris is a chronic inflammatory condition that primarily impacts the face, but it can also spread to the shoulders and the back. Its development is influenced by both internal and external factors. Acne exists as comedones, papules, pustules, nodules, and secondary signs including scars, erythema, and hyperpigmentation. Comedones are enlarged hair follicles filled with keratin squamae, bacteria, and sebum. 118 Acne may compromise skin barrier function, affecting both the follicular and surface of the skin.119,120 Some data suggest acne vulgaris itself might weaken the skin barrier, and that acne severity and deficiencies in skin barrier function are correlated. 121 Some topical anti-acne medications (most of them contain benzoyl peroxide) can further weaken the skin barrier function and increase the TEWL, causing irritation. 122 TEWL values of acne skin are reported below based on the types of TEWL devices used.
Open-chamber device.
NCT02173054104,123 compared the effects of three different moisturizing creams applied twice daily for 8 weeks. TEWL was measured with a Tewameter TM300. The facial skin of group 1 (Adapalene gel) had the baseline mean TEWL of 9.8 ± 3.3 SD g·m−2·h−1; TEWL 12.3 ± 4.8 SD g·m−2·h−1 at week 8 (p = 0.0002, method: paired t-test); while group 3 (Adapalene gel with Eucerin) had the baseline TEWL 10.6 ± 3.7 SD g·m−2·h−1; and TEWL 11.5 ± 3.3 SD g·m−2·h−1 at week 8 (p = 0.123, method: paired t-test). For group 2 (Adapalene gel with placebo moisturizer) baseline TEWL was 10.4 ± 4.6 SD g·m−2·h−1; and week 8 TEWL was 11.8 ± 5.4 SD g·m−2·h−1 (p = 0.007, method: paired t-test).
NCT00964366 98 examined two treatment groups: one using Clindamycin and benzoyl peroxide (BPO) gel and the other using Dapsone gel, with applications to one-half of the face daily for 2 weeks. The reported mean TEWL at baseline were 10.29 ± 3.06 SD g·m−2·h−1 and 10.4 ± 2.93 SD g·m−2·h−1 respectively, measured with a Evaporimeter open-chamber device. After treatment, the reported mean TEWL value was 13.88 ± 3.7 SD g·m−2·h−1 and 11.26 ± 3.08 SD g·m−2·h−1, respectively, on day 14.
NCT01015638 96 investigated two formulations: clindamycin and BPO 5% gel versus Clindamycin phosphate and BPO 2.5% gel. The reported mean TEWL at baseline were 10.82 ± 4.15 SD g·m−2·h−1 and 9.71 ± 3.14 SD g·m−2·h−1 respectively. After treatment, the reported mean TEWL value was 13.94 ± 4.1 SD g·m−2·h−1 and 13.59 ± 4.68 SD g·m−2·h−1 (p > 0.05), respectively, at day 14. TEWL was measured using an Evaporimeter device. Both groups experienced increased TEWL over 2 weeks indicating potentially greater skin dryness with the former formulation.
In NCT00926367, 97 the effects of Duac (a combination of a topical antibiotic and benzoyl peroxide) were compared with Epiduo (a formulation containing benzoyl peroxide and adapalene). Both groups experienced an increased TEWL over 2 weeks, but the Epiduo group consistently reported higher TEWL values than the Duac group at all measured time points, suggesting more adverse effects on skin barrier function.
Condenser-chamber device.
NCT04606134 99 evaluated Alastin Regenerating Skin Nectar with TriHex Tech against Cetaphil face cream, measuring TEWL at the arm with an AquaFlux device. In the Alastin-treated group, reported TEWL decreased from 6.502 ± 6.65 SD g·m−2·h−1 at day 4 to 2.858 ± 7.23 SD g·m−2·h−1 at day 34, indicating improvement in skin barrier function. In contrast, the control group using Cetaphil face cream exhibited a TEWL increase from 21.59 ± 6.65 SD g·m−2·h−1 at day 4 to 39.07 ± 7.23 SD g·m−2·h−1 at day 34, suggesting a decline in skin barrier function.
Unknown devices.
NCT01909713, 100 NCT03743038, 101 NCT04559022, 108 and NCT06415292 109 did not specify the type of TEWL measuring device used in their protocols. NCT01909713100,124 evaluated a test foam wash and moisturizer SPF 30, and reported a TEWL value of 8.89 ± 3.01 SD g·m−2·h−1 on acneiform skin in the arm of children aged 7–11 years. NCT03743038, 101 NCT04559022, 108 and NCT06415292 109 presented TEWL percentage change outcomes following the application of their test products such as FMX101 vehicle, hydro-alcohol solution, Winlevi (clascoterone) 1% cream on acneiform skin.
Summary of observations.
TEWL measurements were taken after a topical was applied to assess skin barrier function.99,100 In these cases, baseline TEWL values were established at the face (average was 9.71–13 g·m−2·h−1) and arm (average 8.89 g·m−2·h−1) sites having a poor agreement with face or cheek values between trials and literature. 37 Although the reported face value in the trials does not specify the exact facial point, the literature reports three different locations on the face: cheek (21.66 g·m−2·h−1), forehead (17.7 g g·m−2·h−1 1), and scalp (12.66 g·m−2·h−1). 37 Differences in anatomical location could be a possible reason for disagreement of the TEWL values. Average TEWL values at faces for all studies were in poor agreement with reported literature values but were in good agreement (±15%) with each other. Several of these studies are limited by the lack of skin control on the patient. Since the entire face is affected by acne, it is not possible to get a healthy baseline of the subject’s face prior to acne. Furthermore, most studies evaluated TEWL measurement as secondary outcomes, as primary outcomes studies were skin erythema101,108,109 and skin dryness.96–100
Infant skin
As with adults, the skin barrier function in infants primarily involves the SC, which protects the body from external factors and maintains hydration by regulating water loss. 125 While full-term newborns have a well-defined SC, its maturation continues post-birth, only achieving adult-like properties by age two. Until then, infants have a thinner SC and epidermal layer compared to adults, leading to higher TEWL. The average TEWL value between 3–6 months infants is 26 g·m−2·h−1 (at upper ventral arm) compared to adults which is 8.2 g·m−2·h−1 (p = < 0.0005, 3–12 months vs. adult). 126 In addition, the acid mantle is not fully developed in infants. 89 Because of their immature skin barrier, infants are more susceptible to irritants, infections, and conditions such as diaper dermatitis and AD. Diapers create an occlusive environment, increasing the risk of hyperhydration and skin barrier impairment. The effects of baby wipes on the skin barrier, particularly their ingredients’ absorption and potential irritation, are crucial areas of concern in infant care. In general, infants exhibit higher TEWL than adults at all sites. Furthermore, infants aged 6 weeks to 3 months, 3 to 6 months, and 6 to 12 months show a linear decrease in TEWL at all sites. 127 Skin barrier function improves with adulthood. 127 Studying infant skin helps ensure the safety and efficacy of products such as diapers and baby wipes. These products must be carefully formulated to avoid ingredients that could damage the developing skin barrier or cause irritation.
Open-chamber device
NCT03370757128,129 explored the impact of bundling nursing care activities on the overall health of very low birthweight preterm infants. The study evaluated differences in infant skin health when diaper changes occur every 3 h versus every 6 h during 3 h bundled care. The study’s main purpose was to evaluate supportive care using a parallel assignment intervention model. In addition to TEWL, the study measured mean heart rate and microbiota diversity of the skin. The study included 46 infants aged 28 (±2.8) weeks, conducted in the United States with participants of multiple races. The analyses included TEWL estimates across all bundled care events for each group. TEWL values were collected using an open chamber system. Results showed that infants in the 3 h bundled care group had a mean TEWL of 38.48 g·m−2·h−1 (95% CI: 31.93 to 45.03), while those in the 6 h bundled care group had a slightly lower mean TEWL of 35.73 g·m−2·h−1 (95% CI: 29.67 to 41.79) at buttock measured employing a DermaLab device. These findings suggest that more frequent diaper changes, as in the 3 h bundled care group, may be associated with increased TEWL rates and barrier disruption, compared to less frequent changes. Understanding the skin barrier function in infants can guide the development of safer infant care products, such as material design for diapers and inform parents about the best practices for managing infant skin health and optimal diaper-changing frequency. 130
SUMMARY
Measuring TEWL is a valuable noninvasive method for assessing skin barrier function, providing critical insights into skin health and disease. Recent studies on human chronic wounds show that measurement of TEWL at the wound-site post-closure is highly valuable in testing whether functional wound closure is achieved i.e., whether skin barrier function has been re-established at the site of wound closure. If such functional wound closure is not achieved, i.e., TEWL values are high at the wound site postclosure, then that wound is likely to recur. Thus, TEWL measurement is critically important to determine wound healing clinical endpoint.
Elevated TEWL levels indicate compromised barrier integrity, which is associated with conditions such as AD, psoriasis, and irritant contact dermatitis. By quantifying water evaporation through the SC, TEWL helps evaluate the severity of skin disorders, monitor treatment efficacy, and guide the development of barrier-repair therapies. In addition, TEWL measurements are useful in dermatological research, cosmetic testing, and personalized skincare, making it a key tool for both clinical and experimental applications in skin science.
Finally, it is important to note that absolute TEWL values are expected to vary based on anatomical location, skin disease status, and participant characteristics. Such values may also vary based on the technology used to measure TEWL. Appropriate control of such conditions, measurement settings, and environmental factors is therefore necessary to ensure study rigor and reproducibility.
TAKE HOME MESSAGES
In wound care, structural wound closure is inadequate. It is important to achieve functional wound closure which includes restoration of skin barrier function at the wound-site post-closure. Functional wound closure can be measured at the point of care by clinical TEWL measurement.
Deficiencies in functional wound closure, as recorded by high TEWL, predict wound recurrence.
There are several factors that can affect TEWL rate and how it is measured. Among others, temperature, relative humidity, type of TEWL measuring device, and anatomical location are confounding variables that must be controlled when measuring TEWL.
Current wound-recurrence-related TEWL studies are based on the use of open-chamber DermaLab equipment.
AUTHORS’ CONTRIBUTIONS
D.K.: Conceptualization (supporting); writing— original draft (lead); formal analysis (lead); writing—review and editing (equal). A.J.: writing—original draft (supporting); Writing—review and editing (equal). C.K.S.: Conceptualization (lead), Methodology (lead); review, and editing (equal).
Footnotes
ACKNOWLEDGMENT
We acknowledge the contribution of Dr. J. Parker Evans to develop the first submission of the article.
FUNDING INFORMATION
TEWL studies in C.K.S.’ program are funded by R01-DK125835, R01-DK128845, R01-DK135447, R01-DK141513 and U01-DK119099.
AUTHOR DISCLOSURE AND GHOSTWRITING
No ghostwriters were used in the writing of this article. D.K., A.J., and C.K.S. have no conflicts that may inappropriately influence or affect the integrity of the submission.