
Abstract
Bipolar affective disorder is a serious psychiatric condition characterized by episodes of elevated and depressed mood. Incidence peaks between the ages of 25 and 30 years and it has a lifetime prevalence of 1.3%. Bipolar disorder has significant morbidity and mortality, but early detection and good multidisciplinary management can reduce the impact of the disease. It is important that a GP can recognize the disorder, refer appropriately and provide good community care.
The GP curriculum and bipolar affective disorder
Manage people experiencing mental health problems in primary care, bearing in mind that several interventions may be effective for each mental health condition Describe specific interventions and guidelines for individual conditions, using where appropriate best practice as described in the Scottish Intercollegiate Guidelines Network (SIGN) or National Institute for Health and Clinical Excellence (NICE) guidelines Demonstrate how to screen and diagnose people experiencing mental health problems, using effective and reliable instruments where they are available Describe how to access health and social care organizations, both voluntary and statutory, that are an essential component of managing people with mental health problems Describe how to enable people experiencing mental health problems to fully engage in delineating their difficulties and deciding on appropriate interventions Describe the concept of concordance that is particularly important in mental health care Be able to present individuals with choices as to which intervention may work best for themselves Describe the importance of continuity of care for people with mental health problems Have an awareness of people at risk for mental health problems Be able to assess risk/suicidal ideation Demonstrate how to work in partnership with other agencies to secure appropriate social interventions for individuals Describe the impact that social circumstances can have on mental illness and that recovery is contingent on the effective management of those social circumstances
In both the International Classification of Disease (ICD-10) and the Diagnostic and Statistical Manual (DSM-IV-TR), bipolar disorder is conceptualized as a spectrum of disease in which mood fluctuates from abnormally high mood to abnormally low mood. Periods of elated mood may be associated with intense creativity, and many artists, including the artist Vincent van Gogh, are thought to have suffered from bipolar disorder.
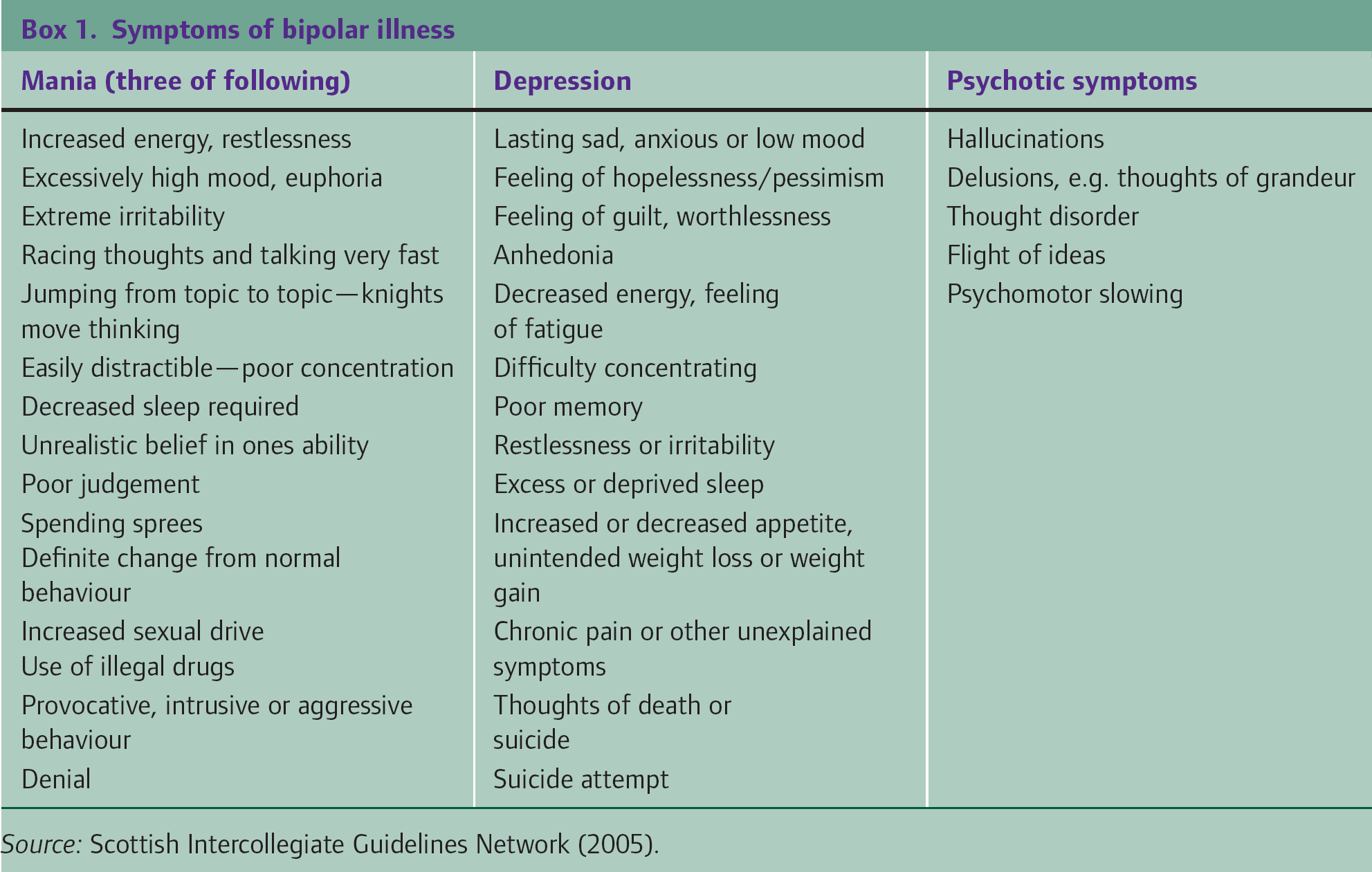
Most of us experience ups and downs in our mood according to the circumstances that we find ourselves in. Mania is characterized by a persistently high or euphoric mood out of keeping with circumstances. Other symptoms and signs are listed in Box 1. Hypomania is much more common than true mania. Patients with hypomania have some of the symptoms of mania, but these are less severe, with no psychotic symptoms. A key difference between hypomania and mania is that patients with hypomania do not have impaired function.
At least two major categories of bipolar disorder have been described—Bipolar I and Bipolar II. DSM-IV-TR defines Bipolar I as the presence or history of one or more manic episodes or mixed episodes with or without major depressive episodes (ICD-10 requires at least two episodes). A depressive episode is not required for diagnosis, but it is rare to suffer solely manic episodes, and a history of depression can found in at least 80% of sufferers.
Bipolar II consists of recurrent intermittent hypomanic and depressive episodes (DSM-IV-TR). Depressive episodes tend to be more frequent and intense than hypomanic episodes in Bipolar II and Bipolar II tends to have less effect on the patient's functioning in society than Bipolar I.
In both cases, manic/hypomanic episodes tend to last between 2 weeks and 4–5 months and depressive states about 6 months. Ninety percent of sufferers will experience at least one relapse that can, in many patients, be linked to a stressful event in their lives. The length of remission often decreases as the patient ages, but symptoms tend towards depression rather than mania. Between 10 and 15% of patients suffer from ‘rapid cycling’, which is described as four episodes of mania, hypomania, depression or mixed episodes occurring in 12 months.
Aetiology
Although a specific cause of bipolar disorder has not been determined, there is strong evidence that there is a genetic component and concordance between monozygotic twins can be up to 70%. Gradually, possible genes are beginning to be identified. There is also emerging evidence that there may be physical changes in the structures and the pathways of the brain although research is at the early stages. Inflammation is also suggested as a possible factor. Significant life events, such as family bereavement, pregnancy and birth, can precipitate episodes.
Initial presentation
Patients may present to primary care with a new diagnosis of bipolar disorder at several points in their illness. They may present
When a crisis occurs (when the GP may be called upon for an assessment with a view to treatment and/or detention under the Mental Health Act) If reports of abnormal behaviour are received from concerned friends or relatives In the surgery with depressive symptoms or when the mania starts to resolve or After discharge from secondary care.
As clinical presentation can vary dramatically from acute mania to a more modest change in behaviour, diagnosis can be difficult and is often delayed. It is not uncommon for adolescents who suffer from depression or attention deficit hyperactivity disorder (ADHD) to later be diagnosed with bipolar disorder.
Box 1 describes the presenting symptoms of bipolar disorder whether they be those of mania or depression. Symptoms of psychosis may also be present that can make the initial presentation difficult to distinguish from schizophrenia.
Patients suffering from mania rarely present to their GP. However, a relative or friend may present with concern, which should be taken seriously. They are more likely to present during a depressive episode or when the mania begins to resolve.
Occasionally, symptoms of mania and depression can occur together—a mixed affective state comprising agitation, difficulty sleeping, change in appetite and occasionally psychotic features and suicidal thoughts. For example, the patient may feel low and helpless, while still being energized.
Depending on the state of the patient at the time of assessment, it may be extremely difficult to take a history as the patient may lack insight, could be very irritable and excitable and unwilling to engage. A history from a friend or relative who knows the patient is particularly useful in these circumstances. Conversely, the patient may have no current symptoms as the episode has ended. As there is significant misdiagnosis of bipolar disorder, it is important to ask about overactive or disinhibited behaviour and symptoms of mania/hypomania in all patients who present with depressive episodes.
In all cases, it is important to ascertain what the patient's symptoms are or were, the duration of illness and previous episodes. Box 2 describes possible differential diagnoses.
Differential diagnosis of bipolar disorder
Schizophrenia Drug-induced mania or psychosis Frontal-lobe lesions Thyrotoxicosis Schizoaffective disorder Psychotic depression
Referral of patients with suspected bipolar disorder
NICE (2006) recommends that GPs should normally refer patients with suspected bipolar disorder for a specialist mental health assessment and development of a care plan, if either of the following is present:
periods of overactive disinhibited behaviour lasting at least 4 days with or without periods of depression or three or more recurrent depressive episodes in the context of a history of overactive disinhibited behaviour.
All patients with new-onset mania or suffering an acute relapse should be seen by specialist services within a week of diagnosis and consider requesting same-day review if you consider the patient a danger to him-/herself or others. Early intervention services for people with psychosis should also be available to patients with bipolar disorder and should provide specialist expertise in diagnosis and pharmacological, psychological, social, occupational and educational interventions. If the patient refuses voluntary assessment and treatment, compulsory assessment and treatment under the terms of the Mental Health Act may be required.
Suicide risk
The suicide rate in patients suffering from bipolar disorder is 15–20% and a third of sufferers attempt suicide at some point. Attempted suicide can be the presenting feature of bipolar disorder. Most suicides occur during a depressive or mixed episode. NICE (2006) recommends that all patients with bipolar disorder should undergo a suicide risk assessment when
bipolar disorder is diagnosed the patient undergoes significant change in mental state or personal circumstances a patient is discharged or leaves inpatient care.
Management of acute episodes of mania
Initial management aims to ensure that the patient and those around him or her are safe and avoids as much anguish and harm as possible. Refer to the specialist mental health services. A crisis plan may already be in place if the patient has a pre-existing diagnosis of bipolar disorder.
For patients being treated in the community, advise patients and carers to avoid excessive stimulation, engage in calming activities, delay important decisions and establish a structured routine. Ensure adequate hydration.
Sedation with medication should be avoided if possible but benzodiazepines, in particular lorazepam and clonazepam or haloperidol, can be used. The latter can be given via an intra-muscular route if required. Sedatives should be used with caution in elderly patients who are more likely to suffer side effects such as respiratory depression or falls. Most Primary Care Trusts provide information about their preferred medication and GPs should be aware of local policies.
Specialist management
Decisions about medication will usually be made by the consultant psychiatrist who has responsibility for the patient. If the patient is already taking an antidepressant, this is usually stopped. Treatment decisions are based on whether the patient is already taking an antimanic preparation or not.
If the patient develops acute mania when not taking an antimanic preparation, treatment options are as follows:
an antipsychotic (e.g. olanzapine, quetiapine or risperidone)—especially if the patient has severe manic symptoms or marked behavioural disturbance semisodium valproate or lithium.
Valproate should be avoided in women of childbearing potential. Lithium should only be used as a first-line agent if symptoms are not severe as it has a slower action than either antipsychotics or valproate. Carbamazepine should not be routinely used and gabapentin, lamotrigine and topiramate are not recommended. If initial treatment with an antipsychotic is ineffective, effects may be augmented by the addition of either valproate or lithium.
Management of acute episodes in patients already on antimanic medication varies according to the agent being used:
For patients already taking antipsychotic medication, the dose should be increased if possible. If this is ineffective, either lithium or valproate can be added. For patients already taking lithium, a blood lithium level should be checked. If levels are suboptimal (less than 0.8 mmol/l), the dose of lithium should be increased to attain blood levels of 1 mmol/l. Addition of an antipsychotic should be considered on presentation if symptoms are severe or if lithium levels are optimal and the patient still has symptoms. For patients already taking valproate, the dose should be increased until symptoms improve or side effects prevent further increase in dose. Addition of an antipsychotic should be considered on presentation if symptoms are severe or if the dose of valproate cannot be increased further and the patient still has symptoms. For patients already taking carbamazepine, addition of an antipsychotic should be considered but it is important to consider drug interactions with carbamazepine.
For all patients, antimanic agents are often combined with a benzodiazepine (e.g. lorazepam) in the initial phase of management to help control acute behavioural disturbance or agitation. Electroconvulsive therapy (ECT) is also an option for rapid short-term treatment of severe symptoms if other treatments have proved ineffective.
Management of acute episodes of depression
In bipolar disorder, antidepressant medication may result in the patient ‘switching’ to a manic state (particularly tricyclic antidepressants) and may be involved in cycle acceleration (mood destabilization). For patients with mild depressive symptoms, a 2 week period of ‘watchful waiting’ is appropriate if the patient has not developed severe or chronic depression in the past, as symptoms may resolve spontaneously.
For patients with more severe symptoms, those who have mild symptoms but have had severe or chronic episodes of depression in the past and those who have not improved after a period of watchful waiting, consider seeking specialist advice and/or starting medication. Ask for same-day specialist review if you consider the patient a risk to him-/herself or others. If the patient refuses voluntary assessment and treatment, compulsory assessment and treatment under the terms of the Mental Health Act may be required.
Choice of medication will depend on whether the patient is already taking an antimanic preparation or not and what that preparation is:
For patients not taking an antimanic preparation, consider starting a selective serotonin reuptake inhibitor (SSRI) together with an antimanic agent (always seek specialist advice) For patients taking an antimanic preparation, check that this is being taken at an appropriate dose and adjust the dose if necessary before prescribing an antidepressant. If the antimanic agent is not an antipsychotic, consider adding quetiapine. If starting antidepressant medication, use an SSRI at the lowest dose that is effective for the patient.
Antidepressants should be avoided for patients with depressive symptoms who have recently had a hypomanic episode or suffer from rapid-cycling bipolar disorder or rapid mood fluctuations that impair functioning. For these patients, seek specialist advice. Treatment options include increasing the dose of their antimanic agent or adding a second antimanic agent (including lamotrigine).
Before starting any antidepressant medication, educate patients about side effects and likely course of action. It is particularly important to warn them about
the possibility of manic or hypomanic switching the delay in onset of effect and the gradual and fluctuating nature of improvement the need to take medication as prescribed and the risk of discontinuation or withdrawal symptoms the need to monitor for signs of akathisia, suicidal ideation and increased anxiety and agitation, particularly in the initial stages of treatment the possibility of gastro-intestinal side effects (consider prescribing a proton pump inhibitor concurrently if the patient is elderly, has a history of indigestion or peptic ulceration or is taking other medication such as non-steroidal anti-inflammatory drugs (NSAIDs) that may also cause stomach irritation) the need to seek help promptly if these side effects are distressing.
If optimal drug treatment does not improve symptoms, always refer for specialist review. Specialist medication review and/or specialist psychological therapies may be helpful. ECT is also an option for rapid short-term relief of severe symptoms of depression.
If antidepressant medication does help, and the patient recovers or has significantly less depressive symptoms for a period of 8 weeks, consider stopping the antidepressant medication gradually over a period of several weeks but maintain the antimanic medication. Monitor carefully. Patients are particularly at risk from discontinuation reactions when taking paroxetine or venlafaxine. There is no evidence that long-term treatment with antidepressants reduces relapse rates. It may be considered for patients with recurrent or chronic depression but cognitive behavioural therapy (CBT), quetiapine or lamotrigine are alternatives; take specialist advice.
Routine and ongoing care
People with bipolar disorder, whether managed in primary or secondary care, should have continuity of care (wherever possible) to improve long-term outcomes. In primary care, this may mean one particular GP acting as the patient's main point of contact with the practice. It is important to fully involve patients in decisions about and planning of their treatment and care. All patients with bipolar disorder should be entered on the practice mental health register for Quality and Outcomes Framework (QOF) purposes.
Regular review
QOF requires all patients on the mental health register to be reviewed annually. Currently 23 points are available (with payment stages from 40 to 90%) if a review is recorded in the preceding 15 months on the QOF assessment. In the review, there should be evidence that the patient has been offered routine health promotion and prevention advice appropriate to their age, gender and health status. If patients do not attend for their annual review, they should be identified and followed up by the practice team within 14 days of non-attendance. Three further QOF points are available for doing this (payment stages 40–90%). A further six points are available if a comprehensive care plan is documented in the records that has been agreed between individuals, their family and/or carers as appropriate (payment stages 25–50%).
Physical health monitoring
NICE (2006) recommends that patients with a new diagnosis of bipolar disorder should have a physical health review. This should include a baseline recording of
The patient's smoking status and alcohol use Height, weight and body mass index Blood pressure Baseline blood tests—renal function, liver function, thyroid function, full blood count, blood glucose and lipid profile.
These measurements establish a baseline against which future reviews can be compared and also may influence choice of drugs. Further investigations will usually be consultant led to exclude other causes of symptoms or relevant co-morbidities and establish baseline measures before drug initiation. These tests may include electroencephalogram (EEG), computed tomography (CT) or magnetic resonance imaging (MRI), drug screening, chest X-ray and/or electrocardiogram (ECG).
Patients with serious mental health problems are at considerably increased risk of physical ill-health than the general population, and 46% of people with bipolar disorder smoke compared to 33% of the general population. Antimanic drug side effects include weight gain and propensity of diabetes. QOF requires the review of physical health to include
an enquiry about smoking, alcohol and drug use a blood pressure check a cholesterol check where clinically indicated and in all patients over 40 years even if there is no other indication of risk (NICE, 2006) measurement of body mass index a check for the development of diabetes cervical screening where appropriate an enquiry about cough, sputum and wheeze.
Ongoing medication for bipolar disorder
Long-term treatment (or prophylaxis) for bipolar disorder is considered for patients who have suffered a manic episode associated with significant risk or adverse consequences or for patients who have suffered at least two or more acute episodes or have significant functional impairment or risk of suicide.
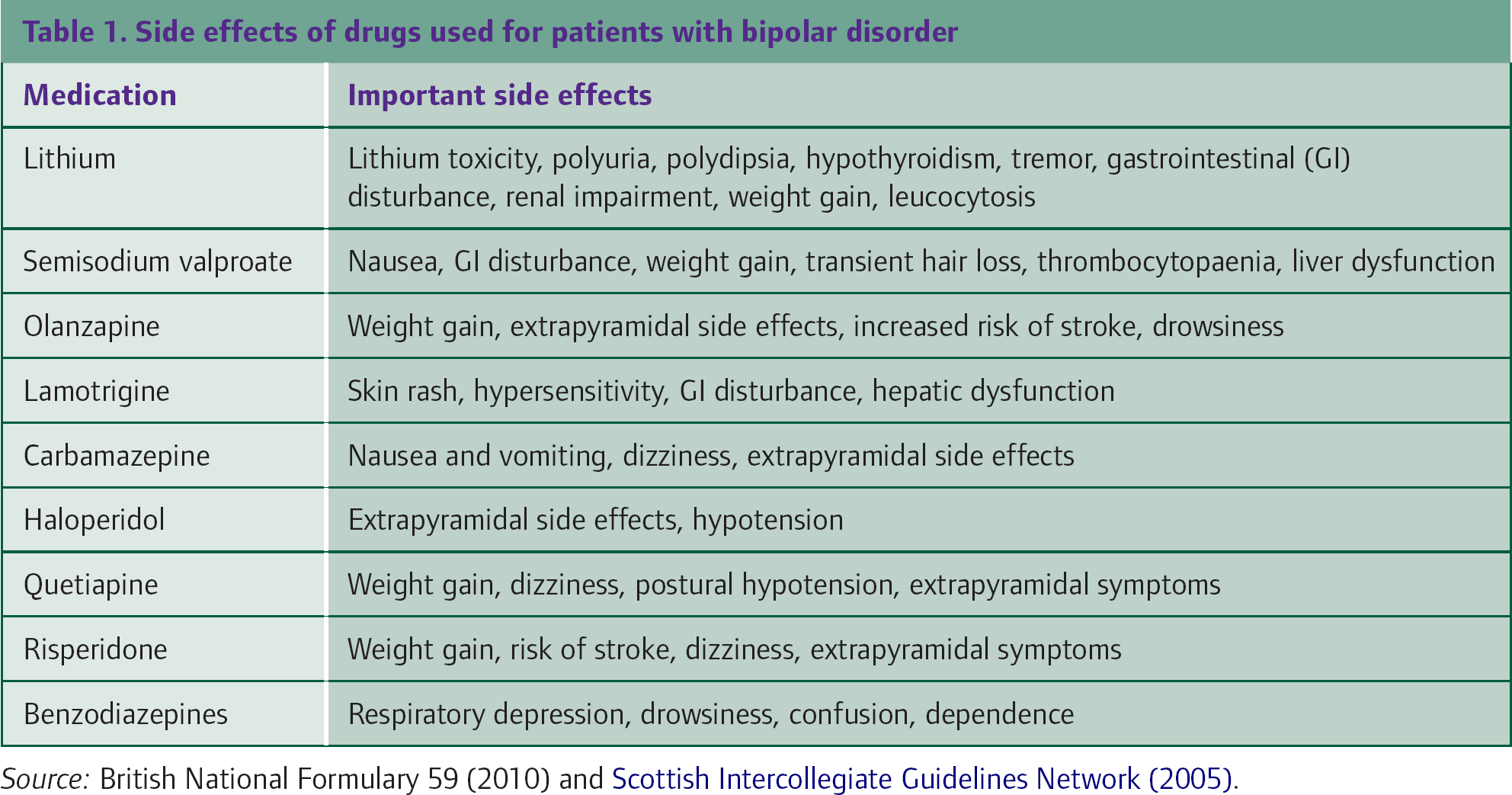
Lithium, olanzapine and valproate are the first-line drugs used. Choice of drug is a specialist decision and depends on response to previous treatments, pattern of illness, physical factors (such as impaired renal function, body mass index or diabetes), gender and patient preference. Other drugs used include carbamazepine and lamotrigine (which may be used as monotherapy for Bipolar II disorder). Common side effects of drugs used for patients with bipolar disorder are summarized in Table 1.
Side effects of drugs used for patients with bipolar disorder
Long-term drug treatment is routinely continued for at least 2 years after an episode of bipolar disorder and up to 5 years if the person has risk factors for relapse, such as a history of frequent relapses or severe psychotic episodes, co-morbid substance misuse, ongoing stressful life events or poor social support. Discontinuation of drug therapy should only be undertaken with specialist guidance and support.
Drug monitoring
Many of the drugs used as prophylactic agents have side effects that should be monitored.
For patients taking antipsychotics, ensure that weight is measured every 3 months for the first year and more often if there is rapid weight gain. Measure fasting plasma glucose and lipids 3 months after the start of treatment (1 month if taking olanzapine) and more often if there is evidence of elevated levels.
In patients taking risperidone, prolactin levels should be measured if symptoms of raised prolactin develop. These include low libido, sexual dysfunction, menstrual abnormalities, gynaecomastia and/or galactorrhoea.
For patients taking valproate, liver function and a full blood count should be checked 6 months after treatment is started. Weight monitoring may be necessary if the patient gains weight rapidly. Routine measurement of valproate blood levels is not recommended unless there is evidence of ineffectiveness, poor adherence or toxicity (NICE, 2006).
Lithium treatment has a narrow therapeutic range and it is toxic in overdose. Lithium levels should be checked 1 week after starting and 1 week after each dose change until levels are stable. Box 3 summarizes the symptoms and signs of lithium toxicity. Intercurrent illness, declining renal function or co-prescription of drugs that reduce lithium excretion may precipitate lithium toxicity. Patients taking lithium should be advised to ensure that they maintain fluid intake (particularly after exercise, in hot weather or if they are ill with a fever) and seek medical attention if they develop diarrhoea and/or vomiting. They should also be warned not to take over-the-counter NSAIDs. Take care when prescribing prescription medication (such as NSAIDs, angiotensin converting enzyme inhibitors or diuretics) that may interact with lithium.
Symptoms and signs of lithium toxicity
Decreased appetite Diarrhoea Vomiting Ataxia Nystagmus Dysarthria Confusion Seizures Atrio-ventricular heart block
Lithium monitoring is essential and is a QOF target. There is no definitive evidence on the optimum frequency of lithium level checks. NICE (2006) recommends that lithium levels should be checked every 3 months when the patient is stable, but QOF awards 2 points (payment stage 40–90%) if a lithium level has been recorded in the preceding 6 months. Where a practice is prescribing the lithium, it is the responsibility of the practice to ensure that monitoring takes place and for following up patients who default from monitoring tests. Levels should be measured 12 hours after the last dose. The therapeutic range is usually 0.4–1.0 mmol/l, but NICE (2006) recommends a minimum therapeutic level of 0.6 mmol/l.
Overt hypothyroidism has been found in 8–15% of people taking lithium and deterioration of renal function increases the likelihood of lithium toxicity. For these reasons, NICE (2006) also recommends testing renal function and thyroid function every 6 months. Renal function should be checked more frequently if there is any renal impairment and specialist advice sought if there is a significant reduction in renal function. QOF requires annual checks of renal and thyroid function and a QOF point is available if serum creatinine and thyroid-stimulating hormone levels have been recorded within the previous 15 months (payment stages 40–90%).
Psychosocial support
People with mental health problems have fewer social networks than average, and many of their contacts are related to health services (40% have no social contacts outside the mental health services). In England, people with serious mental health problems have the lowest employment rate of any group of people with just 24% in work. This has ramifications for social interaction, feeling of self-worth and also financial implications.
Psychosocial support is very important in the management of patients with bipolar disorder. This may take the form of education and information provision, support through voluntary organizations, support groups, social services, the community mental health team or employment support.
Education and information provision are extremely important for not only the patient but also the whole family. Provide written information about bipolar disorder and information about self-help groups (such as the Bipolar Association www.mdf.org.uk or MIND www.mind.org.uk) and good-quality Internet sites. In addition, NICE (2006) recommends that advice should be given on
the importance of good sleep hygiene and a regular lifestyle the risks of shift work, night flying and flying across time zones and routinely working excessively long hours, particularly for patients with a history of relapse related to poor sleep hygiene or irregular lifestyle ways for patients and carers to monitor physical and mental state.
Support with respect to housing and work is also important. Disability advisors accessed through Jobcentre Plus can be very helpful in assisting patients with bipolar disorder to get back into employment. It is important to provide additional support with increased monitoring of mood and general well-being after significant life events such as relationship breakdown, bereavement or loss of work, as such events can trigger relapse. Encourage the patient to talk about difficulties with family and friends.
If a patient is treated under the care programme approach (CPA), then they should have a documented care plan discussed with their community key worker, who is often a member of the community mental health team. However, up to half of people who have a serious mental illness are seen only in a primary care setting. For these patients, it is important that the primary care team takes responsibility for discussing and documenting a care plan in their primary care record. QOF recommends that the following information is included in the care plan:
The patient's current health status and social care needs including how needs are to be met, by whom and the patient's expectations How socially supported the individual is, e.g. friendships/family contacts/voluntary sector organization involvement Co-ordination arrangements with secondary care and/or mental health services and a summary of what services are actually being received Early warning signs that may indicate a possible relapse—many patients may already be aware of their early warning signs (or relapse signature) but it is important for the primary care team to also be aware of noticeable changes in thoughts, perceptions, feelings and behaviours leading up to their most recent episode of illness as well as any events the person thinks may have acted as triggers The patient's preferred course of action (discussed when well) in the event of a clinical relapse, including who to contact and wishes around medication.
A care plan should be accurate, easily understood, checked as part of the annual review and discussed with the patient, his or her family and/or carers. It should also be documented in the patient's general practice notes.
The role of psychological therapies
There is a significant role for the use of psychological therapies in bipolar disorder. CBT can be useful for treatment of depressive episodes. It can also be useful during the maintenance phase in preventing relapses, increasing social functioning and establishing positive routines (such as sleep patterns). As early warning signs monitoring can be included within the CBT programme, CBT can also help the patient to form an action plan for use if symptoms begin to deteriorate.
Family therapy is aimed at psychoeducation, communication training and problem-solving skills so that the family know what to do in case of deterioration. Patients who undertake family intervention have a longer interval between relapses and decreased morbidity. Group psychoeducation and befriending services also have a role to play.
Referral for secondary care support
Urgent referral to secondary care should be considered for any patient with an acute exacerbation of symptoms, whether mania or depression, and especially if severe. Consider urgent referral as well if there is an increase in the degree of risk (or change in the nature of risk) to the patient or other people (NICE, 2006).
Consider referring any patient with bipolar disorder who registers with your practice for assessment by the local specialist mental health services and, if appropriate, development of a care plan. For patients already registered with your practice who have a diagnosis of bipolar disorder but who are managed entirely in primary care, consider referral to secondary care if
functioning declines significantly the patient responds poorly to treatment concordance with the treatment plan is a problem there is actual or suspected co-morbid alcohol and/or drug misuse the patient would like to discuss stopping prophylactic medication after a period of relatively stable mood the patient is planning pregnancy or is pregnant.
Pregnancy and breastfeeding
The peak age of presentation of bipolar disorder is adolescence and early adulthood. For young women, this may have implications for childbearing.
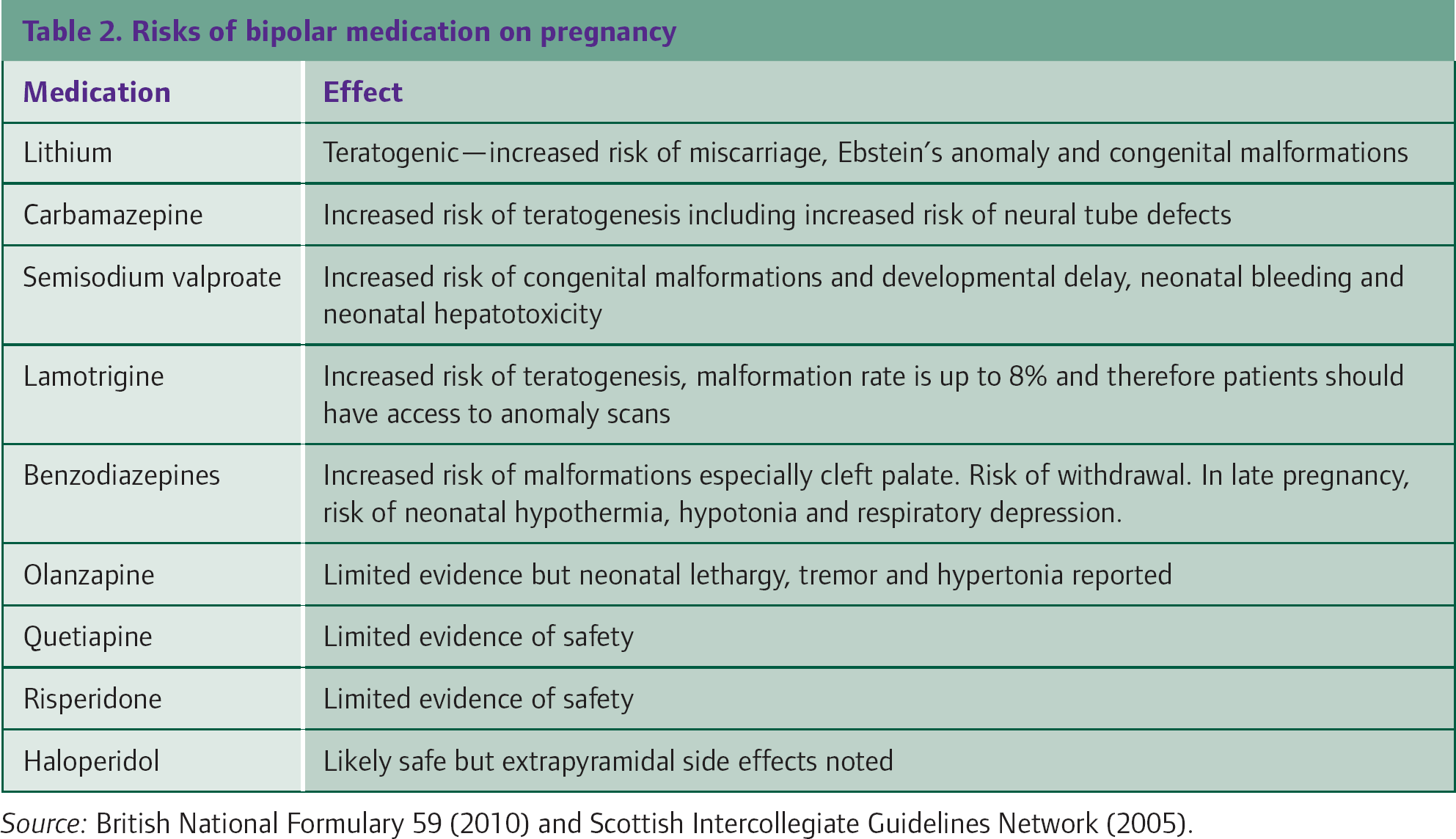
Drug treatment for young women should be chosen very carefully. NICE (2006) recommends avoidance of valproate for women of childbearing potential wherever possible because of its teratogenic effects.
Pre-pregnancy counselling is very important with advice on smoking, illicit drug use, diet, alcohol consumption and folic acid. Counselling should include discussion of the risks of bipolar disorder occurring in the child. Consider referral to specialist psychiatric services to optimize drug regimes before pregnancy and for further discussion of the risks of pregnancy and specialist support that can be provided. Table 2 highlights the risks to the baby of taking antimanic medication in pregnancy.
As soon as pregnancy is confirmed, women with bipolar disorder should be referred for both specialist obstetric and specialist psychiatric care. Once the child is born, the mother will need very close follow-up as the puerperal time is a very vulnerable one. The mother has increased risk of both relapse and puerperal psychosis. Patients taking lithium should not breast feed and other medication should only be prescribed after checking up-to-date information.
Contraception
Carbamazepine is an enzyme inducer. Patients taking carbamazepine for treatment of bipolar disorder should not use oral contraceptive methods or subcutaneous contraceptive implants as they may be ineffective. The Faculty of Family Planning and Reproductive Healthcare recommends contraception using an intrauterine device or intrauterine system (Mirena) or injectable contraception with Depo-Provera given every 10 weeks instead of the usual 12 weeks.
Risks of bipolar medication on pregnancy
Driving
The Driving and Vehicle Licensing Agency (DVLA) states that for people with Group 1 licences (motor car), driving must cease during an acute episode of bipolar disorder. It is the driver's responsibility to inform the DVLA. If the illness is not associated with drug or alcohol abuse, re-licensing can be considered when all the following conditions are met:
Has remained well and stable for at least 3 months (6 months if four or more episodes of mood swings in the previous 12 months) Is compliant with treatment Has regained insight Is free from adverse effects of medication that would impair driving Subject to a favourable specialist report.
For drivers with Group 2 (vocational) licences, driving must cease pending the outcome of medical enquiry. It is normally a requirement that the person should be well and stable for 3 years (i.e. to have experienced a good level of functional recovery with insight into their illness and to be fully adherent to the agreed treatment plan, including engagement with the medical services) before driving can be resumed. The DVLA usually requires a consultant report that specifically addresses the relevant issues before the licence can be considered.
Key points
Bipolar disorder is a serious psychiatric illness that causes significant mortality and morbidity Prompt assessment and treatment is essential in an acute episode, including assessment of suicide risk Appropriate referral to psychiatric services, especially in acute situations, is vital The medications used to treat the illness can have significant side effects and must be monitored carefully and used with caution in women of childbearing age Engagement of the multidisciplinary team is important in reducing and managing relapses