
Abstract

Tiredness, fatigue and/or lethargy are common reasons for patients to present to GPs. In a large survey of psychiatric morbidity in the UK, the prevalence of unexplained chronic fatigue lasting over 6 months was estimated at 9%. Symptoms of fatigue are more common among women than men. Other studies have found that up to 50% of the population complains of tiredness at any time.
Almost any disease processes can cause tiredness—whether physical or psychological. The causes of tiredness can be regarded as falling into a spectrum with completely physical causes at one end of the spectrum, accounting for around 9% of cases, and purely psychological causes at the other end of the spectrum (Table 1). In the middle are the causes that may have some kind of physical basis and also have a strong psychological element, such as irritable bowel syndrome, fibromyalgia and chronic fatigue syndrome (CFS).
Common causes of fatigue in primary care

Initial assessment
When a patient presents with fatigue, lethargy or tiredness, take a careful history (Fig. 1). Ask about the onset and duration of the symptoms and pattern of fatigue. Enquire if there are any other associated symptoms and any exacerbating or relieving factors. Ask about the patient's sleep pattern and about intercurrent stressors and psychiatric history. Consider using depression and anxiety screening tools. It can be difficult to tease out physical from psychological symptoms. Chronic tiredness is depressing and often patients with chronic physical illness will have psychological symptoms. Patients with chronic psychiatric problems may neglect themselves and develop physical health problems as a result. Examine the patient carefully. Most examinations will be normal.

Assessment of patients presenting with fatigue.
Red flag features
Any patients presenting with any of the following features should be thoroughly investigated to exclude serious physical causes:
Localizing and/or focal neurological signs
Signs and symptoms of inflammatory arthritis or connective tissue disease
Signs and symptoms of cardio-respiratory disease
Significant weight loss
Sleep apnoea
Clinically significant lymphadenopathy.
The GP curriculum and fatigue
GP Curriculum Statement 13 (Care of people with mental health problems) states that GPs in training should be able to manage patients presenting to general practice with a history of chronic fatigue or ‘tired all the time’. In particular GPs in training should be able to do the following:
Manage people experiencing tiredness in primary care, bearing in mind that several interventions may be effective, including different forms of talking therapy, medication and self-help
Describe the need to check for psychological illness while avoiding the habit of checking extensively for physical illness
Show that they understand that ideas about the physical, psychological and social should be integrated in both consultation and investigation of illness
Understand that a model of mental illness that creates an artificial separation between mind and body is often unhelpful—particularly in understanding psychosomatic complaints, psychological consequences of physical illness and somatization
Describe how to enable people experiencing mental health problems to fully engage in delineating their difficulties and deciding on appropriate interventions
Describe the concept of concordance that is particularly important in care of people with chronic physical and mental health problems—this should include being able to present individuals with choices as to which intervention may work best for themselves and understanding that this ability to choose improves the effectiveness of the intervention
Demonstrate how to work in partnership with other agencies to secure appropriate social interventions for individuals.
Investigations
Consider other investigations according to the symptoms that the patient reports. Tests that should usually be carried out are listed in Fig. 1. Do not check serum ferritin in adults or test for vitamin B12 or folate deficiency unless a full blood count shows anaemia or micro- or macrocytosis. Do not routinely ask for serological testing, unless there is an indicative history of an infection; if so, consider tests for the following:
Chronic bacterial infections, such as borreliosis
Chronic viral infections, such as HIV or hepatitis B or C
Acute viral infections, such as infectious mononucleosis (heterophile antibody tests)
Latent infections, such as toxoplasmosis, Epstein—Barr virus or cytomegalovirus.
Management
Treat any physical causes found for the patient's symptoms or refer for further investigation and treatment. In most cases, no physical cause is found. Reassure the patient. If the fatigue is thought to be due to a self-limiting condition (such as an acute infection) or a treatable condition (such as hypothyroidism) but symptoms do not resolve as expected, listen to the patient's or carer's concerns and be prepared to reassess the patient and your original diagnosis.
Explaining the relationship of psychological and emotional factors to fatigue can help patients deal with symptoms, especially if they have significant stressors in their lives. If fatigue lasts for more than 2–3 months and there are other symptoms or signs of depression or anxiety, consider a trial of antidepressants such as sertraline 50 mg daily. Discontinue if there is no benefit after 4 weeks of treatment.
Refer children with fatigue to a paediatrician within 6 weeks of presentation. Refer adults with fatigue if:
Chronic or disabling fatigue with no identifiable cause
Suspected CFS or
If referral is requested by the patient.
For patients without any initial diagnosis, give tailored advice on managing symptoms, aiming to minimize their impact on daily life—for example advice on diet (Box 1), sleep management (Box 2), rest periods and relaxation (Box 3) and education and employment (Box 4). Do not delay advice until a definitive diagnosis is made.
Chronic fatigue syndrome
CFS is a debilitating and distressing condition affecting up to 1 in 40 of the population. It is also commonly known as myalgic encephalomyelitis or encephalopathy (ME). The cause is poorly understood. Viral infections (about 10% develop chronic fatigue after infection with the Epstein—Barr virus), immunization, chemical toxins (e.g. organophosphates and chemotherapy drugs) and many other factors have been implicated. In reality, CFS may be a heterogenous diagnosis with several different aetiologies.
Diet
Recommend that patients eat regularly and stick to a well-balanced diet including slow-release starchy foods in meals and snacks.
Manage nausea conventionally, with advice on eating little and often, snacking on dry starchy foods and sipping fluids (small amounts frequently). Consider anti-emetic drugs only if nausea is severe.
There is not a great deal of evidence for the use of exclusion diets, but many patients subjectively find them useful. Consider referring patients on exclusion diets to a dietician to ensure that the patient's diet is meeting the patient's nutritional requirements.
There is also considerable overlap between CFS and several other syndromes with symptoms of chronic tiredness and unknown aetiology, such as fibromyalgia and irritable bowel syndrome (Fig. 2). It is not clear how closely these conditions are related to each other. One study found that incidence rates of the specific diagnoses of CFS or ME, and fibromyalgia have risen in the past 10 years, against a background of little change in symptom reporting. This is likely to reflect fashions in diagnostic labelling rather than true changes in incidence.
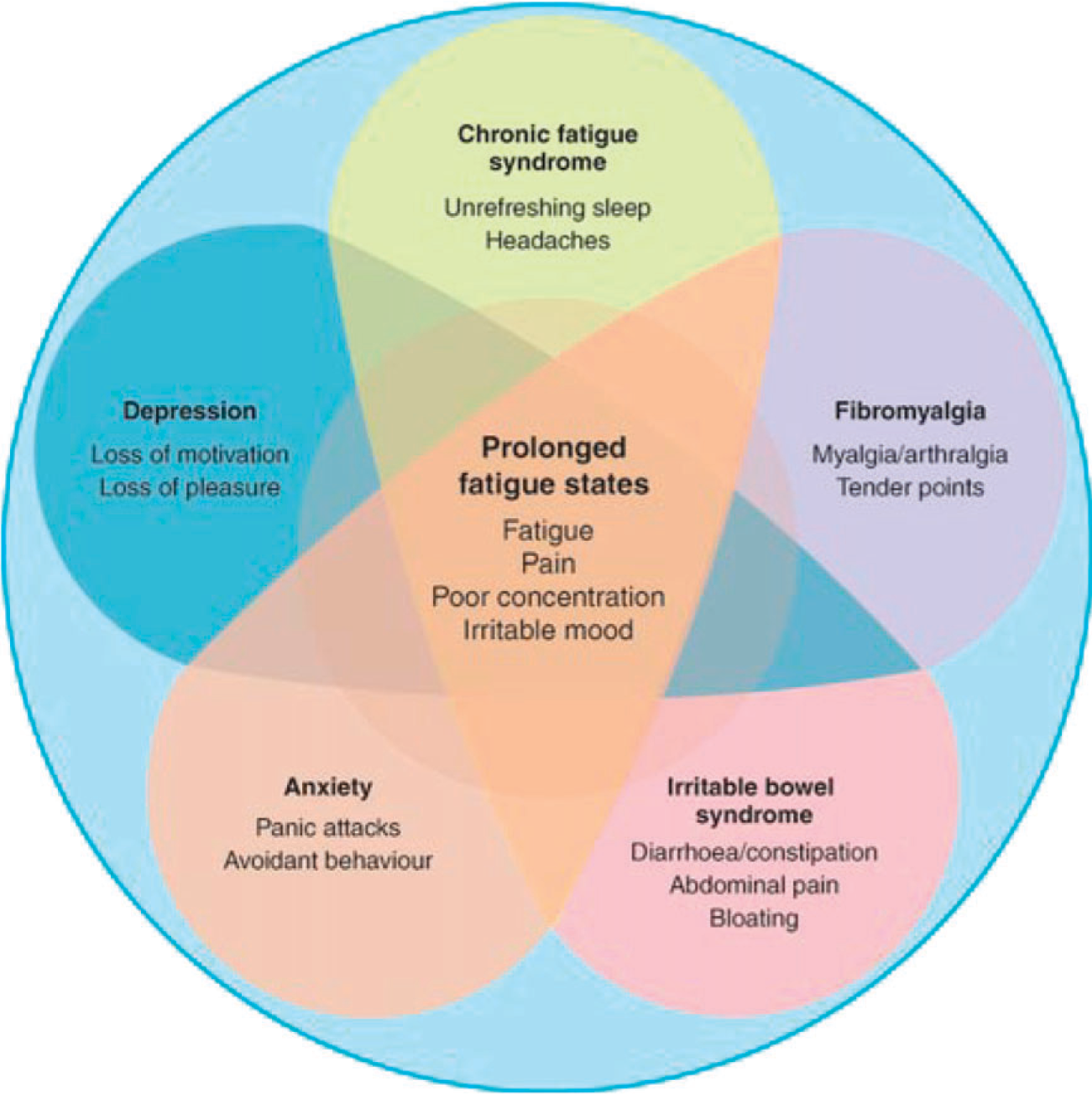
Overlap between CFS and other fatigue states.
Making the diagnosis
Consider the possibility of CFS if a person has fatigue that is:
new or had a specific point of onset (i.e. it is not life long)
persistent and/or recurrent
unexplained by other conditions
causing a substantial reduction in activity levels
characterized by post-exertional malaise and/or fatigue—typically delayed, for example by at least 24 hours, with slow recovery over several days.
The diagnosis is more likely if the person also has one or more of the following additional symptoms:
difficulty with sleeping, such as insomnia, hypersomnia, unrefreshing sleep or a disturbed sleep—wake cycle
muscle and/or joint pain that is multi-site and without evidence of inflammation
headaches
painful lymph nodes without pathological enlargement
sore throat
cognitive dysfunction, such as difficulty thinking, inability to concentrate, impairment of short-term memory, and difficulties with word finding, planning or organizing thoughts and information processing
physical or mental exertion makes symptoms worse
general malaise or ‘flu-like’ symptoms
dizziness and/or nausea
palpitations in the absence of identified cardiac pathology.
Sleep management
Patients with CFS often have changes in their sleep patterns that exacerbate fatigue—for example insomnia, hypersomnia, sleep reversal, altered sleep-wake cycle or non-refreshing sleep. Provide sleep management advice. Introduce changes to sleep patterns gradually and review advice regularly. If sleep does not improve, consider the possibility of an underlying sleep disorder.
Eliminate as far as possible any physical problems preventing sleep—for example treat asthma or eczema; give long-acting pain killers to last the whole night; consider hormone replacement in perimenopausal women having night-time sweats, refer if obstructive sleep apnoea is suspected.
Treat co-existent psychiatric problems such as depression or anxiety.
Sleep hygiene:
Don't go to bed until you feel sleepy
Don't stay in bed if you're not asleep
Avoid daytime naps—explain that excessive daytime sleep or frequent napping may further disrupt the sleep—wake cycle without improving physical or mental functioning
Establish a regular bedtime routine
Reserve a room for sleep only (if possible). Do not eat, read, work or watch TV in it
Make sure the bedroom and bed are comfortable, and avoid extremes of noise and temperature
Avoid caffeine, alcohol and nicotine
Have a warm bath and warm milky drink at bedtime
Take regular exercise but avoid late-night exercise (sex is OK)
Monitor your sleep with a sleep diary (record both the times you sleep and its quality)
Rise at the same time every morning regardless of how long you've slept.
Relaxation techniques—see Box 3.
Consider drug treatment. This is a last resort. Benzodiazepines (e.g. temazepam), zolpidem, zopiclone and low-dose tricyclic antidepressants (e.g. amitriptyline 25–50 mg) are all commonly prescribed to be taken at night for patients with insomnia. Only prescribe a few weeks' supply at a time due to potential for dependence and abuse. Benzodiazepines may be prescribed for insomnia ‘only when it is severe, disabling, or subjecting the individual to extreme distress’. Common side effects include amnesia and daytime somnolence. Most hypnotics do affect daytime performance and they may cause falls in the elderly. Warn patients about their affect on driving and operating machinery.
Rest and relaxation
Rest periods:
Advise people with CFS on the role of rest, how to introduce rest periods into their routine, and the frequency and length of rest periods. Review the use of rest periods regularly. Advice may include:
limiting the rest periods to 30 min at a time
introducing ‘low-level’ physical and cognitive activities (depending on the severity of symptoms)
using relaxation techniques.
Relaxation:
Offer relaxation techniques for managing pain, sleep problems and co-morbid stress or anxiety. Techniques such as guided visualization or breathing techniques can be incorporated into rest periods. Relaxation CDs can be borrowed from libraries or bought at pharmacies; relaxation classes are often offered by local recreation centres or adult education centres; many physiotherapists can teach relaxation techniques.
Education and employment
Having to stop work or education due to fatigue is generally detrimental to people's health and well-being. Address each person's ability to continue in education or work early and review it regularly.
Proactively advise about fitness for work and education and recommend flexible adjustments or adaptations to help people to return when they are ready and fit enough.
With the person's informed consent, liase with employers and occupational health services, disability services through Jobcentre Plus and social care and educational services as appropriate.
The symptoms of CFS fluctuate in severity and may change in nature over time. Additional symptoms should not predate the fatigue. A diagnosis of CFS can be made if symptoms have lasted 4 months (3 months for children and young people) and other diagnoses have been excluded. For adults, a diagnosis can be made in primary care. Children should be referred to a paediatrician for confirmation of diagnosis. Reconsider the diagnosis if the patient does not have post-exertional fatigue or malaise, cognitive difficulties, sleep disturbance and/or chronic pain.
Management of CFS
As with all chronic diseases, it is important that diagnosis and ongoing care is a partnership between the patient and the health professionals looking after them. Patients with CFS have no clear clinical signs and often start to doubt themselves and think that it is ‘all in the mind’. Acknowledge the reality and impact of their condition and their symptoms.
The key to success in chronic disease management is in empowerment of the patient to manage his or her own condition. In order to do this, patients must have some knowledge of their own condition, its possible treatments and how they can be applied to their own personal situations. Provide information tailored to the individual patient. Contact details of self-help organizations that provide information and support are included in Box 5. The NHS Expert Patients Programme can also provide information and support for both patients and their carers. Details are available on website: www.expertpatients.co.uk.
Symptom management
There is no known pharmacological treatment or cure for CFS. Manage symptoms of CFS on an individual basis. For children, do not initiate drug treatment in primary care, but consider providing ongoing prescriptions if you are happy to prescribe the drugs recommended by the consultant paediatrician in charge of the child's care. Treatment for adults can be initiated in primary care; however, many patients with CFS are concerned about adverse effects of drug treatment and often consider themselves to be hypersensitive to the effects of drugs. Research evidence does not show that patients with CFS are more sensitive to drugs or have more side effects than any other group of patients, but consider starting drugs at a lower dosage than normal and increasing the dose to normal therapeutic levels gradually in collaboration with the patient.
Further information and support for patients
ME Association Tel: 0870 444 1836, Website: www.meassociation.org.uk
Action for ME Tel: 0845 123 2314, Website: www.afme.org.uk
Royal College of Psychiatrists information sheets, Website: www.rcpsych.ac.uk
Consider diet (Box 1), sleep (Box 2), rest and relaxation (Box 3), employment and education (Box 4), chronic disability support and whether referral to secondary care or other members of the primary health care team is needed.
Disability support
For people with moderate or severe CFS, consider providing or recommending equipment and adaptations, such as a wheelchair, blue badge or stairlift. The benefits of providing these services are maintenance of independence and improvements in quality in life. Weight this against the negative effects of less exercise. Refer as appropriate.
Review the benefits the patient is claiming. Consider incapacity benefit and benefits for chronic disability such as disability living allowance (more information is available from www.direct.gov.uk) and carers allowance. Patients with CFS often have difficulty claiming benefits as their condition does not fit the standard model of disability and there is often nothing specific to find on examination. Patients are often forced to appeal to obtain the benefits that they are entitled to. Support patients through this as it can be a very difficult time for them. Further information on benefits that may be available and the appeal process is available on the Citizens Advice Bureau website (adviceguide.org.uk).
Referral to secondary care
For children, offer referral to specialist services if symptoms have been present 6 weeks or more. For adults, make any decision to refer jointly with the person, depending on their symptoms and any co-morbidities. Continue primary care involvement after referral. Offer referral to specialist services:
within 6 months of presentation to people with mild CFS
within 3–4 months of presentation to people with moderate CFS symptoms
on presentation if severe CFS symptoms.
Specialist treatment options include cognitive behavioural therapy, activity management and graded exercise therapy.
Setbacks
Advise patients with CFS that setbacks and relapses are to be expected. Intercurrent infection, immunization, drugs, caffeine, alcohol and stress may all lead to setbacks.
Develop a plan with each person with CFS for managing setbacks and relapses, so that skills, strategies, resources and support are available when needed. This plan may be shared with the person's carers, if they agree.
During a setback or relapse, try to identify the causes of the setback or relapse, but recognize that this may not always be possible. If a trigger is identified, when the setback is over, discuss with the patient ways in which triggers can be managed in the future and put strategies in place to do that.
Review the management plan during the setback and adjust it to the new circumstances:
Maintain activity levels as far as possible, for instance by alternating activities with breaks and pacing activities. If that is not possible, reduce or even stop some activities and increase duration or frequency of rest periods to stabilize symptoms and re-establish a baseline activity level. After the setback, encourage a gradual return to previous exercise and functional routines.
Consider altering symptom control measures, for example put into place relaxation and breathing techniques.
Support the patient as it is natural to have feelings such as ‘this means that I'll never get better’ at times of setback and encourage optimism.
Prognosis of patients with CFS
Give honest and realistic information about CFS at diagnosis. Prognosis is variable but be cautiously optimistic. Children tend to recover although it may take years. More than half of adults presenting with tiredness have symptoms lasting in excess of 6 months. However most people with CFS will improve over time and some will recover and be able to resume work and normal activities. The risk of prolonged symptoms is increased three fold if there is a history of anxiety or depression. Short duration of fatigue with no anxiety or depression improves prognosis. Only 6% of adults with CFS attending specialist clinics return to pre-morbid functioning. Some patients with severe CFS may remain housebound long term.
Key points
Fatigue, tiredness and lethargy are common, nonspecific symptoms.
The causes can be divided into physical causes, psychological causes and the fatigue syndromes such as CFS, fibromyalgia and post-viral syndrome.
As diagnosis of the fatigue syndromes is a diagnosis of exclusion, assessment is aimed at excluding physical and psychological causes.
Management is aimed at the cause. Where no cause is found, consider a diagnosis of CFS.
Management of CFS involves patient-centred care. A management plan is formulated which includes symptom control, including management of setbacks and relapses, diet, sleep management, rest and relaxation, disability support and referral where appropriate.