
Abstract
Each GP with an ‘average” list will have 20 patients who die every year. Five of those deaths will be from cancer, two will be from a sudden unexpected cause and the remaining 13 will result from chronic disease such as dementia, heart failure or chronic lung disease. Most GPs have one or two patients with terminal disease at any time, although these patients often require a disproportionate amount of GP involvement. On average, 47 weeks of the final year of life are spent at home. It is a sad fact that although most patients spend their final year of life at home and would prefer to die at home, the majority are admitted to a hospital or institution to die.
What is palliative care?
Palliative care starts when the emphasis changes from curing the patient and prolonging life to relieving symptoms and maintaining well-being or ‘quality of life’. The World Health Organization defines palliative care as ‘an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.’ Palliative care:
provides relief from pain and other distressing symptoms, affirms life and regards dying as a normal process, intends neither to hasten nor postpone death, focuses on enhancing quality of life, but may also positively influence the course of illness (though is not primarily concerned with producing long-term remission), is person oriented, not disease-oriented, is holistic in nature, integrates the psychological and spiritual aspects of patient care, offers a support system to help patients live as actively as possible until death, offers a support system to help the family cope during the patient's illness and in their own bereavement and uses a multidisciplinary team approach to address the needs of patients and their families.
The GP curriculum and palliative care
Helping patients to die with dignity and with minimal distress has been one of the most fundamental aspects of medicine, and over the past 50 years, specialist palliative care services have increasingly worked with general practice to develop more advanced knowledge and skill than ever before. Most GPs testify to this as being one of the more difficult, but most satisfying, parts of their job. Studies of patients and their carers have repeatedly shown that many terminally ill patients prefer the option of a death at home. Curriculum statement 12 ‘Care of People with Cancer and Palliative Care’ is the key curriculum statement relating to palliative care.
In relation to palliative care, a GP should be able to:
Demonstrate knowledge of the principles of palliative care and how it applies to both cancer and non-cancer illnesses Attend to the full range of physical, social and spiritual needs of the patient and carers, including bereavement needs Communicate effectively with the patient and carers regarding difficult information about the disease, its treatment or its prognosis Clinically, manage pain, use a syringe driver, initiate medication for symptom control, convert drug doses when changing route of administration and manage palliative care emergencies—major haemorrhage, hypercalcaemia, superior vena cava obstruction, spinal cord compression, bone fractures, anxiety or panic and use of emergency drugs Provide and manage 24-hour continuity of care through various clinical systems Demonstrate knowledge of the social benefits and services available to patients and carers Demonstrate awareness of the key health service policy documents that influence health care provision for palliative care Appreciate the ethical dimensions of treatment and investigation choices, in palliative and terminal care, and advanced directives and how their own personal attitudes and experiences can affect their attitude towards patients who are dying Define and apply evidence-based care in patients with palliative care needs Learn from clinical experience Work closely with other health care professionals in providing palliative care
Many of us think of palliative care being synonymous with care of patients dying with cancer. Palliative care is appropriate for all patients with active, progressive and far-advanced disease and not just patients with cancer—although the evidence base for the efficacy of interventions has been founded on experience with cancer patients.
Palliative care can be used in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiotherapy. It should dovetail into the ongoing active treatment of the patient's illness in the later stages of disease (Fig. 1). It should not be withheld until all treatment alternatives for the underlying disease have been exhausted.
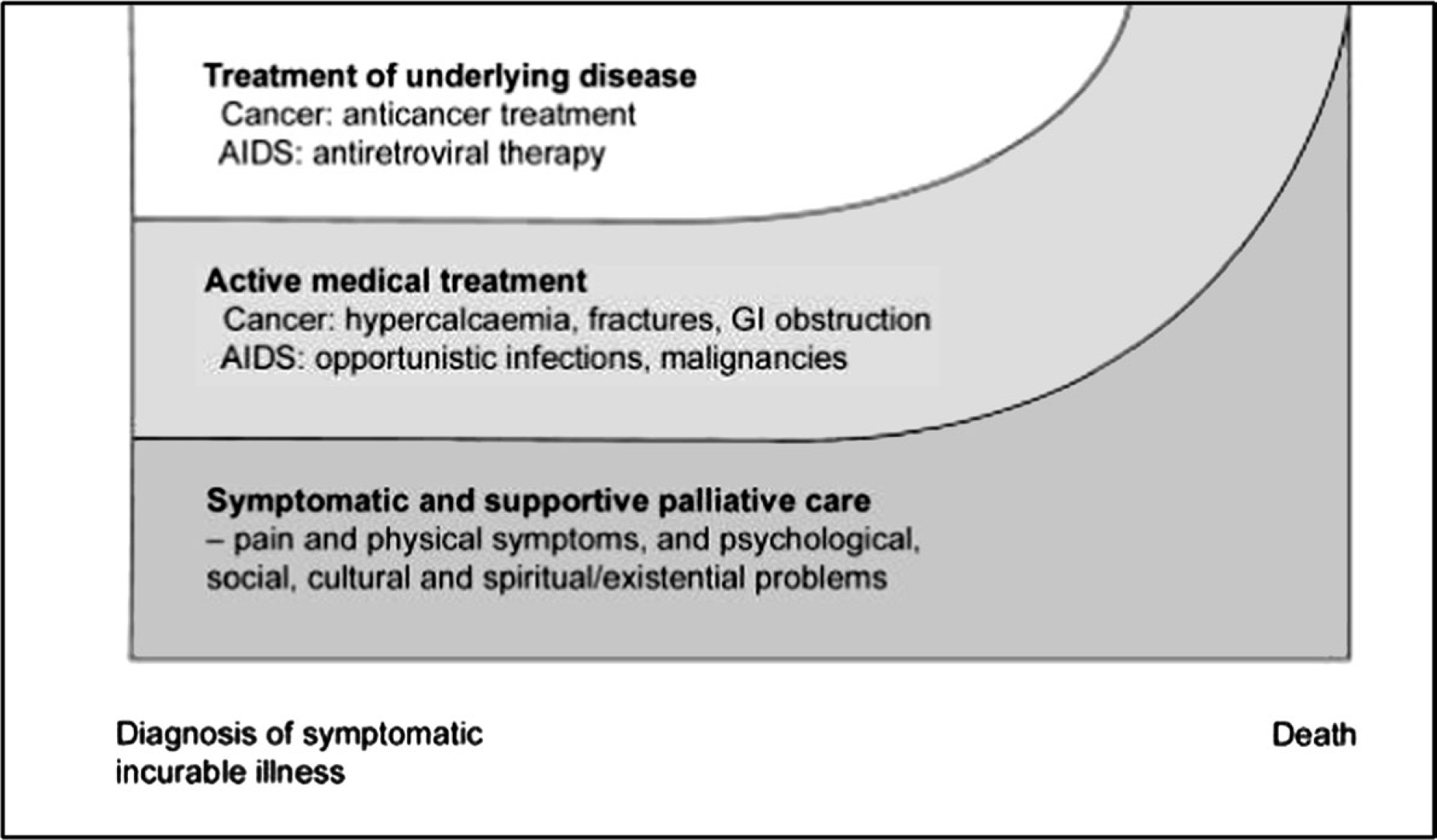
Model of active palliative care.
The role of the GP
GPs and the primary care team have always been, and will continue to be, the main providers of palliative care for most patients but we often find palliative care difficult. Even when specialist palliative care services are involved, GPs of patients receiving palliative care in the community are always team members—and often ‘the key’ to quality, co-ordinated care. Common concerns include the following:
Not knowing enough about controlling symptoms Being reluctant to use powerful drugs in effective doses Worrying about the time commitment involved Being afraid to expose oneself to painful emotions.
Additional qualifications for GPs are listed in Box 1.
Problems encountered
Problems arising in palliative care are a complex mix of physical, psychological and social factors involving both patients and carers (Fig. 2). Try to become familiar with a patient's disease even if it is rare. Keep up to date with hospital investigations and treatment. It is impossible to plan care without the knowledge of course and prognosis, and an easy way to lose a patient's confidence, if you appear ignorant of their condition, or the point in their illness that they have reached.
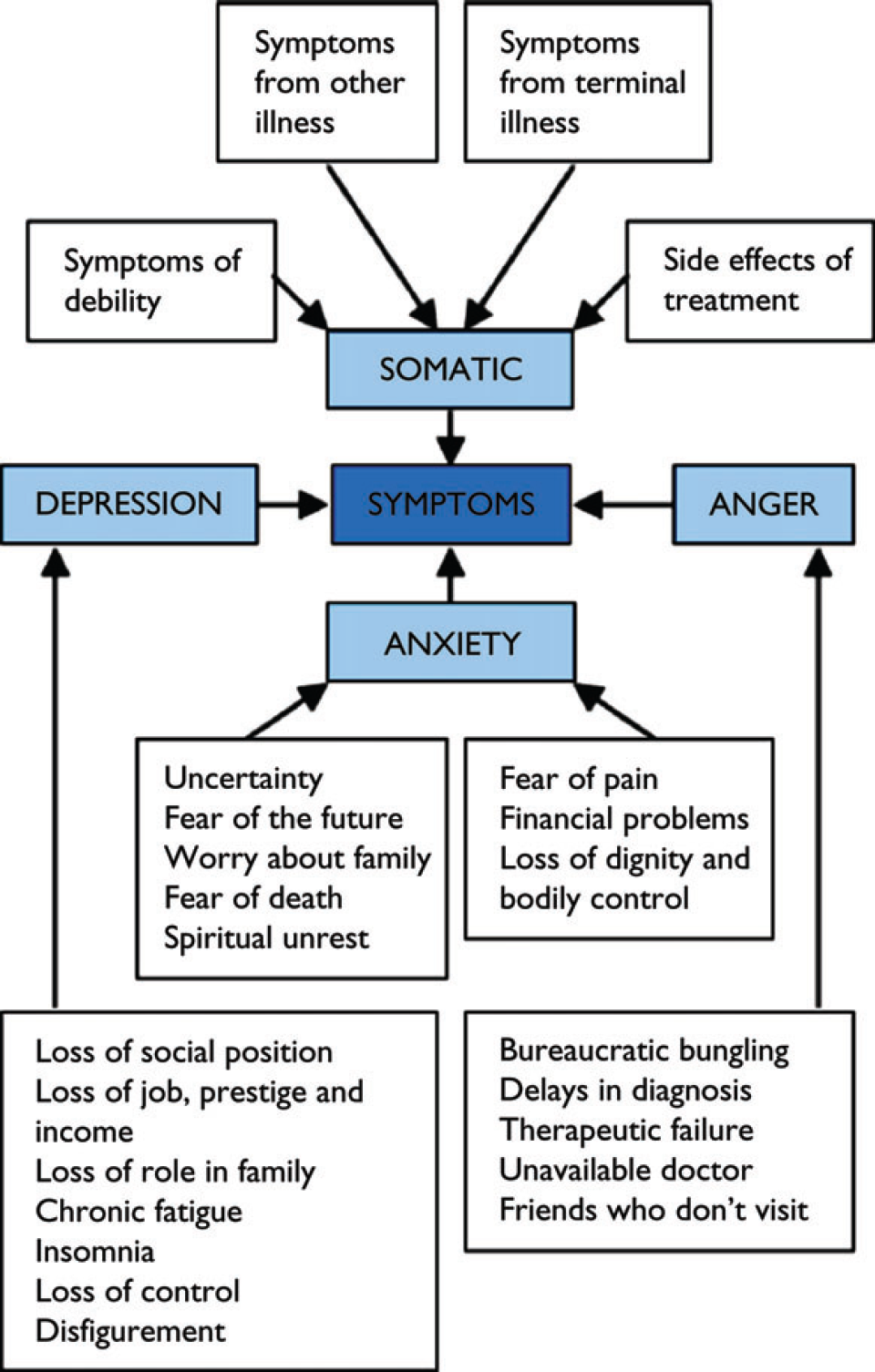
Interplay between different factors affecting patients with palliative care needs.
To respond adequately, maintain an open door policy and encourage patients and carers to seek help for problems early. Symptom control must be tailored to the needs of the individual. The basic rules of symptom control are as follows:
Carefully diagnose the cause of the symptom Explain the symptom to the patient Discuss treatment options Set realistic goals Anticipate likely problems Review regularly
Additional qualifications in palliative care available for GPs
Good lines of communication and close multidisciplinary teamwork are always needed to ensure optimal care. Local palliative care teams are invaluable sources of advice and support and frequently produce booklets with advice on aspects of palliative care for GPs.
Palliative care consultations
Wherever possible, meet the patient face-to-face. Avoid telephone discussions except for brief advice or when face-to-face meetings are not possible (e.g. if the patient is away and wants advice). Ensure privacy—turn your mobile phone off if possible and ask reception staff not to interrupt. Allow enough time and, wherever possible, ensure that the patient has a family member or friend with him/her for support. Always sit at the same level as the patient. Use trained interpreters if the patient does not have sufficient English to communicate freely.
Interview style
Problems are more likely to be detected if the doctor:
Gives good eye contact from the start Clarifies the presenting complaints Moves from open-ended to more closed questions Frequently makes empathic remarks Is sensitive to verbal cues to emotional problems Is sensitive to non-verbal cues Avoids reading, making written notes or computer entries Has strategies to keep the consultation focused
Do not underestimate the benefits of listening to patients. Patients value being listened to because they feel that their problems have been understood, it helps them to clarify or reframe their problems, it helps them to feel an integral part of the care team, it reassures them that they are not alone in their suffering, they feel reassured that treatment is available and can help and it helps them release pent-up feelings.
Background information
Start by introducing the discussion: ‘We need to talk about your illness, the problems you have now and what we want to aim for’. Then find out what the patient and his/her family understand: ‘Tell me what you know about your illness’. Next ask what they expect: ‘What do you think is going to happen with your illness in the future?’ and/or ‘What do you want us to do for you?’
Explore the current problems
When exploring the patients' and carers' problems, use open questions at the start becoming directive when necessary -listen, clarify, reflect and facilitate. Examine the patient as directed by the history. Consider:
Physical symptoms—‘Do you have any pain or discomfort?’; ‘Are there any other symptoms that bother you?’ Psychological and/or spiritual symptoms—‘How are you coping in yourself?’ Social well-being—‘How are you coping at home?’; ‘What do you do in the day?’; ‘Do you need any help around the house?’ Well-being of the rest of the family
Planning appropriate care
Summarize the history back to the patient and give an opportunity for the patient to fill in any gaps. Draw up a problem list with the patient and carer. Discuss possibilities for treatment. It can be useful to use a checklist to ensure that all aspects of care have been covered:
Can physical symptoms be improved? Can the psychological symptoms be improved (including self-esteem)? Can spiritual symptoms be improved? Can functioning within the home be improved? (aids and adaptations within the home, extra help) Can functioning in the community be improved? (mobility outside the home, work, social activities) Can the patient's or carer's financial state be improved? (benefits) Does the carer/family need more support? (voluntary and self-help organizations, extra help, sitting service, respite care, counselling)
Discuss realistic possibilities for treatment in the context of the patient's and your view of the present and future. If agreement is not reached, interventions can be trialled for a specified time. Explain the possible benefits and burdens (or futility) of any intervention. Never say ‘there is nothing more we can do’. There is always something more that can be done. Patients interpret a statement like this to mean that there is no treatment for any further symptoms and both the patient and family feel abandoned. You can tell patients that there is no further treatment for the underlying disease, but stress that you will still be providing continuing care and symptom control.
Outline a management plan with the patient with provision that it could be modified should circumstances change. Shared decision making between patient and doctor improves concordance and patient satisfaction as well as clinical outcome. Set a review date.
Sharing medical information
Give patients as much, or as little, information as they choose to receive—if you are unsure, ask them how much information they want. Share information in a sympathetic way—not abruptly or bluntly—and give information in a manner the patient can understand. Speak clearly and avoid medical jargon and euphemisms. Ask patients to repeat back what they understand to ensure that their understanding is correct. Respond kindly to emotional outbursts.
Discussing prognosis
Avoid giving precise prognoses. Explain the uncertainty in estimating prognosis but give a realistic time range as this enables the patient to deal with their affairs and attend to family relationships.
Discussing referral to the palliative care services
Patients have very variable experience of palliative care services. Some are terrified of referral as they see hospices as places to die and referral means to them that they are going to die—and soon. Others have more positive views of palliative care—either through past experience when such services have been involved with friends or relatives or because they have been involved in the hospice movement themselves, for example as volunteers.
Introduce the possibility of referral to palliative care service when it becomes clear that the patient is suffering from an incurable and progressive disease that will eventually lead to death, and gauge the patient's reaction. Discuss palliative care in the context of how it can help the patient achieve his/her goals. Stress that palliative care is about living as well as possible for as long as possible.
Out of hours care
The GP surgery is not open for around 75% of every week. Patients in the terminal stages of their diseases may be inappropriately treated in the out-of-hours periods by doctors or nurses unfamiliar with their case and plan of care. This can result in inappropriate treatment, inappropriate hospital admissions and even inappropriate resuscitation attempts.
Anticipation and communication are the keys to preventing this from happening. Communicate with patients and carers about what might go wrong, what to do if it does and who to contact. Patient-held records kept in the patient's home and containing a clear and up-to-date plan of care can help ensure anyone unfamiliar with the patient follows the planned course of action. Leaving ‘just in case’ boxes of drugs in a patient's home, complete with nurse authorization forms, may be appropriate in some cases.
Liaison with out-of-hours providers is also important. Hand over palliative care patients to the local out-of-hours providers and provide a plan of care. Liaise with out-of-hours providers to ensure that a stock of appropriate drugs is available to those working for them to use for palliative care patients. Inform local ambulance services as well as out-of-hours providers about decisions not to resuscitate a patient. For those requiring admission, or admitted inappropriately, liaise with secondary care services to ensure rapid discharge home.
The Gold Standards Framework
The aim of the Gold Standards Framework (GSF) is to develop a locally based system to improve and optimize the organization and quality of care for patients and their carers in the last year of life both in primary care and in care homes. It consists of three basic processes as follows:
To identify patients in need of palliative/supportive care towards the end of life To assess their needs, symptoms, preferences and any issues important to them To plan care around patient's needs and preferences and enable these to be fulfilled, in particular support patients to live and die where they choose
The framework focuses on optimizing continuity of care, teamwork, advanced planning (including planning out-of-hours cover), symptom control and patient, carer and staff support. The Framework provides a toolkit for practices, which includes a structure for care and useful assessment and planning tools, together with training and support for involved practice staff. Further information can be obtained from the GSF website www.goldstandardsframework.nhs.uk. Evaluation data show that the framework increases the proportion of patients dying in their preferred place and improves quality of care as perceived by the practitioners involved.
Palliative care in the quality and outcomes framework
A total of six quality and outcomes framework (QOF) points out of a total of 1000 are available for palliative care for patients of over 18 years of age (Table 1). In order to achieve these points, practices must maintain a register of all patients in need of palliative care or support (palliative care 1) and review all those on the register at a multidisciplinary meeting at least every 3 months (palliative care 2). The practice reports the number of patients on its palliative care register and submits written evidence to the Primary Care Organization describing the system for initiating and recording review meetings.
QOF indicators for palliative care

Criteria for inclusion on the register are broad. Include patients if:
Their death in the next 12 months can be reasonably predicted and/or They have clinical indicators of need for palliative care that are prognostic clinical indicators of advanced or irreversible disease and contain one core and one disease-specific indicator and/or They are the subject of a DS1500 form (this can be issued if a patient is suffering from a progressive disease and is not expected to survive longer than 6 months for the purposes of claiming Disability Living Allowance or Attendance Allowance—which are then awarded immediately at highest rate without the need for further assessment).
Core predictors of the need for palliative care are:
Multiple co-morbidities More than 10% weight loss over 6 months General physical decline Serum albumin of less than 25 g/l Reducing performance status or Karnofsky score of less than 50% (Box 2) or dependence in most activities of daily living.
Disease-specific indicators are listed in Table 2.
Disease-specific clinical prognostic indicators for inclusion for the palliative care indicators of the QOF

The Karnofsky score
The Karnosky score measures patient performance of activities of daily living.

Key points
In the average practice, 20 patients a year die per full-time equivalent partner. Palliative care is appropriate for all patients with active, progressive and far-advanced disease and not just patients with cancer. Palliative care should dovetail into the ongoing active treatment of the patient's illness in the later stages of disease, and should not be withheld until all treatment alternatives for the underlying disease have been exhausted. Give patients as much or as little information as they choose to receive. Anticipation and communication are the keys to preventing inappropriate treatment, inappropriate hospital admissions and inappropriate resuscitation attempts. The GSF aims to help practices ‘identify’ patients with supportive and palliative care needs at an appropriate time, ‘assess’ those needs and ‘plan care’ around those needs. A total of six QOF points are currently available for palliative care for patients of over 18 years of age