
Abstract
Working with colleagues and in teams
In this part of the competence framework, we move beyond communication skills as applied to the consultation and into the area of communicating more widely with fellow professionals and members of the team. It is best not to see this as an entirely separate skill set to that required for consultation, but as a development of it.
Teamworking uses the skills acquired in consulting. Which of these do you feel are particularly important?
To answer this, think about the holistic dimension of patient care and how GPs involve the patient's family, friends, employer, etc. in the teamwork that is often needed to deal with more significant problems.
As for many other behaviours that we learn in order to become effective GPs, it helps to think about our attitudes. These often underpin our behaviour in the sense that if our attitude is appropriate, the behaviours often flow naturally. The converse is also true. This is not really surprising if we remember that our attitudes and our motivations are very closely related. If we have appropriate attitudes, our motivations, which we usually do not think about but which operate automatically beneath the surface, will drive our behaviour in a useful direction.
Just as teamworking skills are an extension of the communication skills developed in the consulting room, the mindset or attitude of teamworking is an extension of the ‘partnership’ mindset that we develop through our interactions with patients.
We need to move beyond thinking of team members as ancillary workers, called in to help at our request. Instead, we should think of them as partners with appropriate status and responsibility in helping to contribute to and shape the patient's management. Although we may have overall responsibility, this does not mean that we should also have exclusive ownership. Empowering the team through our personal attitude is strongly motivating for them and, through this, for ourselves.
The need for teamwork
It used to be the case that to achieve the targets that were required of it, a practice principally needed good decision making, strong leadership and a well-organized infrastructure. Many ‘teams’ began life with this pyramidal hierarchy in which doctors and managers were at the top, nurses in the middle and the receptionists of the bottom.
As we will explore below, this system does not encourage individuals, and therefore organizations, to grow into modern teams which are capable of moving from dealing with demands in firefighting mode, to anticipating and planning for change. Such growth is vital partly not only because of the increasing complexity and pace of change of primary care but also because ensuring others of the quality of our care (through clinical governance) and can only be achieved through joint planning and sharing of responsibilities.
Let us take the experience of the first National Service Framework on coronary heart disease (CHD) to illustrate this point. To deliver primary and secondary prevention in line with the framework may require members of the practice to contribute in the following ways:
This list is not exhaustive and does not include the involvement of public and patients who we could regard as members of the widest team. The traditional ‘top-down’ hierarchy is inappropriate because many of the tasks outlined above can be planned and delivered by the groups in an interdependent and coordinated fashion, with individuals being accountable to their groups and the wider team.
There are people with many talents within any general practice team, and it makes sense to use their skills, encourage their ideas and benefit from their ability to spot potential problems and prevent them happening. Think in terms of many hands making light work rather than too many cooks spoiling the broth!
What is a team?
In basic terms, a team is a group of individuals who work together to achieve a common purpose. We are good at defining the structure of a team in terms of the roles, responsibility and lines of accountability of those within it, but are less adept at looking at the environment within which teams operate. The latter is important because if we understand the factors that help or hinder teamwork, we are better able to understand why things go wrong and how they might be corrected or, better still, anticipated.
How can we build a successful team?
Teams exist at various levels. We are already familiar with unidisciplinary teams, many of which work well because they are composed of people who understand and respect each other, share common values and have common goals. Integrated nursing teams and successful GP partnerships are good examples of these. Multidisciplinary teams face not only the generic problems of working in groups but also the difficulties of relating to people who have different responsibilities, attitudes and priorities. Beyond multidisciplinary practice teams, there are locality teams such as commissioning groups that involve other practices whose circumstances, priorities and ways of working together may differ from our own.
For any of these teams to work well, they need to be able to
Share information Discuss and decide Prepare for change
The prospect of team development may seem daunting, but it need not be if we remember that the building blocks of every team are the individuals within it. If we spend time trying to ensure that our colleagues feel valued and are encouraged to contribute, then there will be much less need to spend time trying to solve the problems of a dysfunctional group; as we often say, prevention is better than cure.
What, then, do individuals need to achieve this happy state, and how might we help them? To answer this question, the much-quoted work of the psychologist Abraham Maslow (Maslow, 1970) gives us some ideas. He suggested that individuals develop by meeting their needs in relation to a hierarchy. The sequential nature referred to the fact that meeting one need empowered the individual to develop at the next level. The word hierarchy was important because Maslow suggested that no matter how developmentally advanced an individual might be, progress would be impaired if a lower order need resurfaced. Hence, planning to become a GP trainer (a self-actualization need) might be put on hold if we became ill (a biological need). This hierarchy of development can also be used to consider how groups of individuals or, teams, grow. Let us do this by considering Table 1.
Maslow' hierarchy applied to team development
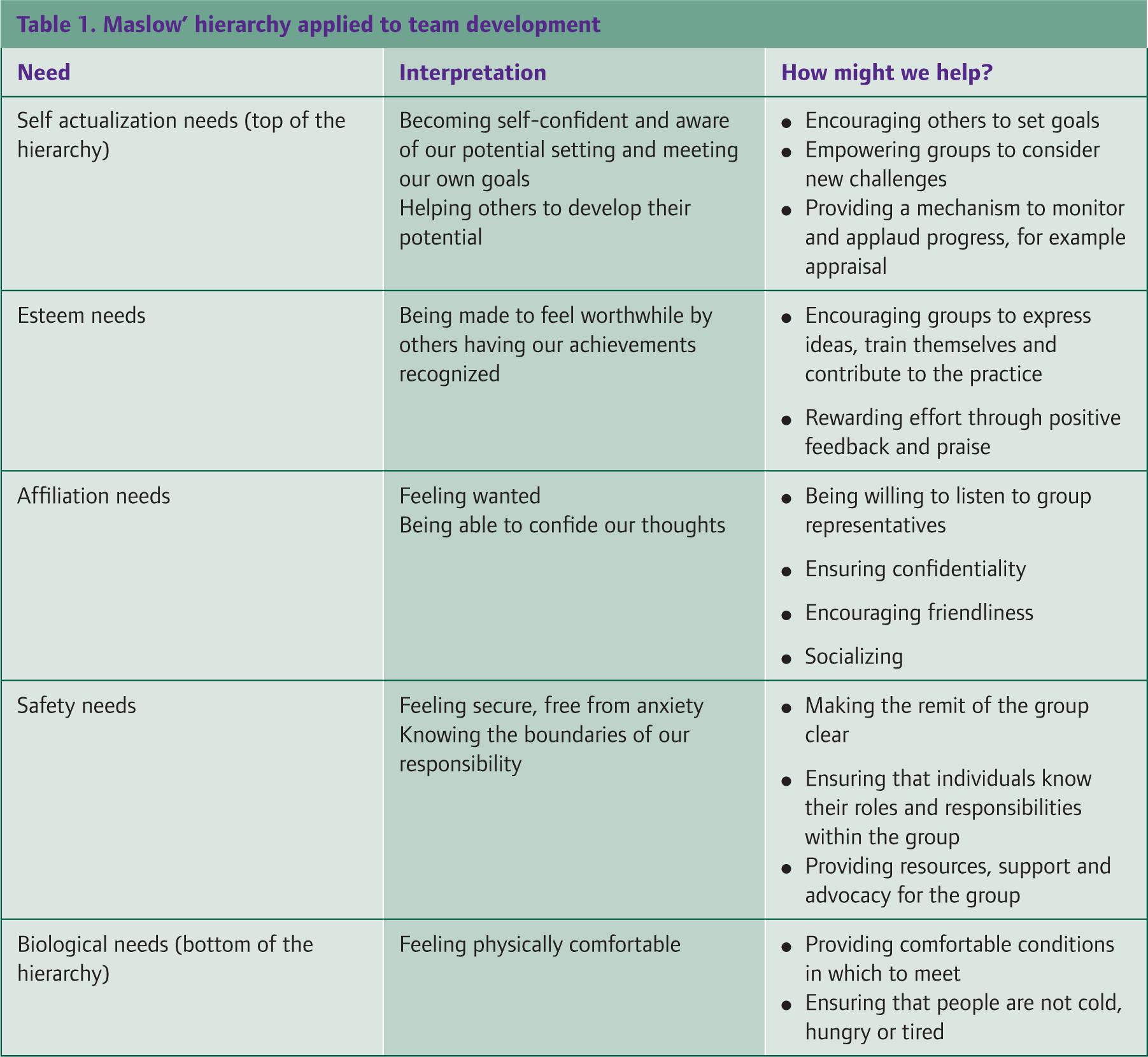
This framework presents the environment or culture within which successful teams grow. Many of the ideas that general practice use are borrowed from industry and in the commercial world, organizations known for their team building such as Asda, have no reservations about expressing a positive corporate culture. We might think of doing the same not in the rather meaningless manner of the mission statement where we promise to respect everyone and their budgie but in practical ways such as those illustrated in the tables.

The first competency progression.
We will now look at the specifics of teamworking through the MRCGP competence framework.
This first indicator progression illustrates how we move from
Being around as required by our employment contract or partnership agreement, but not being more proactive in making ourselves more accessible to colleagues.

Being present, but also being available by letting colleagues know when the best times are to be contacted and by tailoring that availability according to the circumstances.

Looking ahead to periods when the usual availability may be disrupted, for example, through planned absence from work or through changes to the usual rota such as at Christmas and then making arrangements for teamwork to continue effectively particularly for patients such as the terminally ill.
Looking at fig.2, we will discuss each of the word pictures in turn
Even at this basic level, the curriculum encourages us to get to know other members of the team as people as well as practitioners. Obviously, it is important to know the roles of various team members so that we do not refer inappropriately. We also need to know where these roles overlap. For example, a patient with post-natal depression may be referred to the counsellor, but the health visitor may also need to know so that mother and child can be supported.
For some problems, a whole range of therapists may be available to choose from. For example, eye problems could involve optometrists, ophthalmologists, orthoptists, school health services, community eye clinics and social workers. To take an example from rheumatology, problems may require the help of the rheumatology GP with a special interest, physiotherapist, podiatrist, osteopath, chiropractor, orthopaedic surgeon or rheumatologist. Knowing who does what and in what timescale is no mean achievement and is important to get right partly not only for the patient's sake but also because inappropriate referrals use up scarce resources.
GPs have a vital role with chronic disease management and it is our job to ensure that the appropriate team is used and supported. To take diabetes as an example, the team would include diabetes nurse specialists, dieticians, district nurses, community matrons, chiropodists and opticians.
The word picture refers to the ‘abilities’ of team members in addition to their roles and this implies that we should be alert for how team members perform. To use team members appropriately and to assist their personal development, we should also find out what their particular areas of interest are. For example, the practice receptionists are the cornerstone of a well-functioning practice and having a broad range of skills may have particular areas of expertise such as knowing how to search the database for audit purposes.
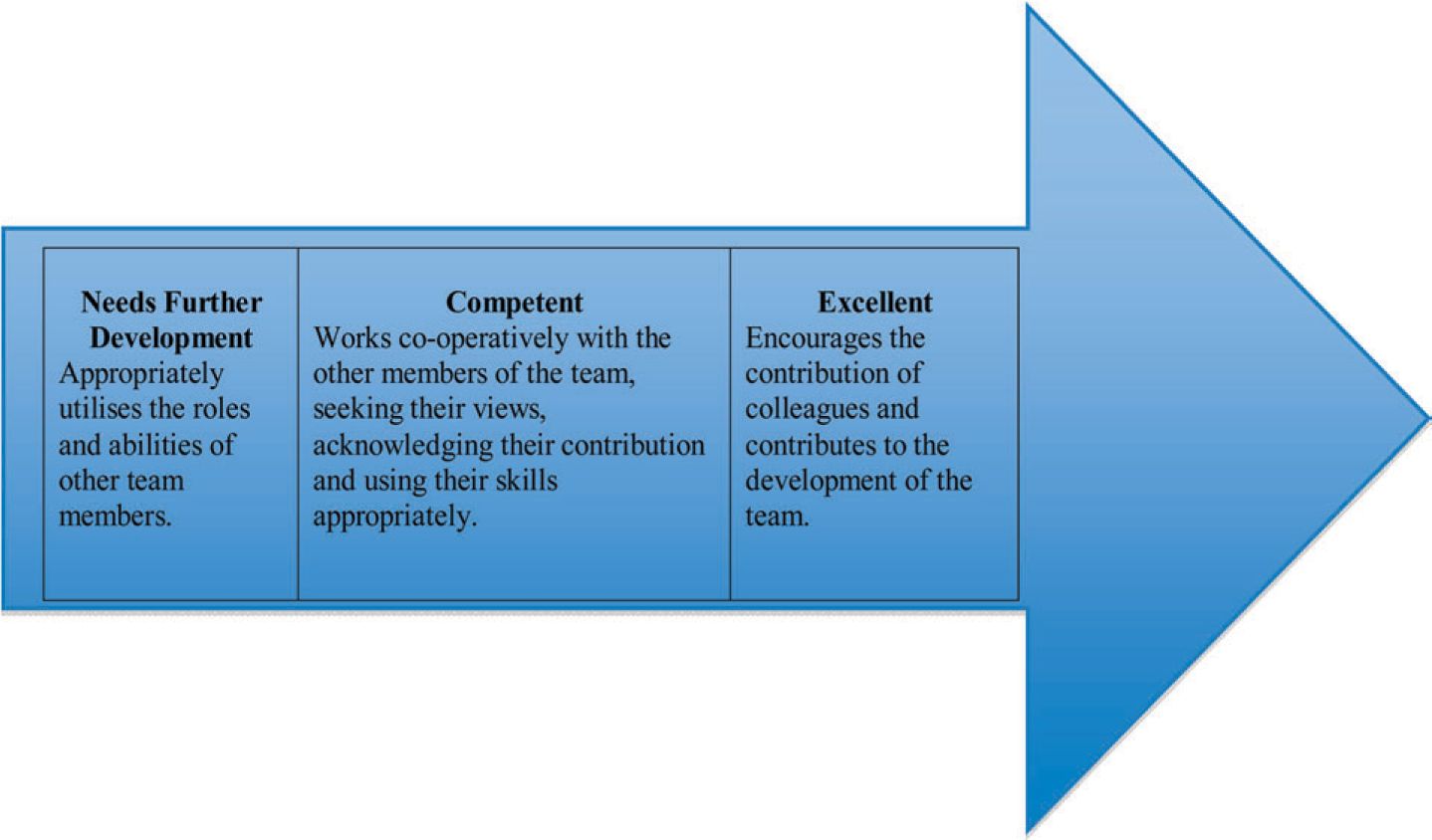
The second competency progression.
This behaviour is thought by many educators to be the most important in the teamworking area.
This competence is really about working in partnership with team members on patient management. At times, this may mean taking on the responsibilities of leading a team with a particular task. At others, it may mean responding to the requests of other team members, that is being delegated to.
In all situations, working cooperatively requires us to know how to communicate effectively, for example, by knowing how best to contact particular members of the team by telephone, e-mail message book and so on.
How would you find out whether you were using the skills of team members appropriately?
Many significant events involve a breakdown in communication. Think of significant events that you have been involved in and ask yourself whether better communication between team members might have made any difference. What do you think are your own teamworking weaknesses and how could you improve?
Really effective team members are not just part of a team waiting to take orders. They are proactive, taking steps to understand how well the team is working and how it can be made more effective in the future. This requires us to understand the different roles that comprise an effective team and know how to build confidence and ability in team members through training and feedback. We also need to understand our own preferences regarding our role and develop certain specific skills that help with teamworking such as
Delegating tasks appropriately Understanding how to motivate people Conducting an appraisal interview Organize an effective meeting Chairing a meeting Managing a project
Finally, we will discuss each of the word pictures shown in fig.3:

The third competency progression.
This basic level competence concerns our ability to respond appropriately to those team members in primary and secondary care who need to know about the patient's management. Increasingly, these days, this can include a variety of community workers and agencies such as community matrons, hospital at home practitioners, emergency care practitioners and so on. Part of our role is to ensure that information is shared appropriately and securely, which may mean taking extra steps to preserve confidentiality such as confirming that the request is coming from a legitimate source.
There are some basics about the information that is needed by the team. In an ideal world, team members
Are informed of those things that have a direct bearing on their work Do not receive information that they do not require (information overload and confidentiality risk) Are presented with information in an understandable form Do not get conflicting or inaccurate information Know where to get information when needed
To this list of ‘rights’, we could add one responsibility, which is for team members (i.e. all the team, not just ourselves) to pass on relevant information in an appropriate way to those who need to know.
Being proactive means thinking ahead and anticipating situations in which patient care could be compromised. This applies to any situation in which patient care is dependent on good teamworking, for example, chronic disease management and palliative care. Our responsibility as GPs is to make sure that continuity of care, communication between team members and clarity of responsibility is maintained.
To give a simple example from palliative care, we may need to let out-of-hours services know about the patient so that an inappropriate emergency visit or attempt at admitting the patient to hospital is avoided. Similarly, we may need to arrange for a colleague to take over medical responsibility while we are on holiday and to let the team know of this arrangement.
Although not explicitly mentioned, the patient and the patient's family/carers should be thought of as part of the team and kept informed to the appropriate degree. Good teamwork means that care is smooth, without unpleasant surprises. When this happens, patients and their families feel confident, which enhances trust and (importantly) promotes health by reducing avoidable distress.
Unfortunately, poor communication between team members is rife. This is partly because teams cross boundaries between hospital and community, have members who are answerable to different bosses and have cultures that do not always align. As GPs, we are usually the people with the most experience and understanding of teamworking and although challenging, we can therefore be the best people to take responsibility for ensuring (for the reasons stated above) that it happens well.
It can be all too easy to blame other people for not communicating well, for example hospital wards and outpatient departments. Once you have got over your irritation, what could you do to improve the situation? Which of your suggestions have you personally implemented?
In the simplest form, this may mean using the telephone and fax machines appropriately and securely. Depending on the urgency of the situation, we may choose to ring for an appointment rather than send a letter. Similarly, services are geared up to respond to different levels of urgency. We need to be aware of this so that we can use, for example, emergency services, rapid access clinics such as chest pain or suspected stroke and suspected cancer clinics appropriately.
In some situations, our skill depends upon recognizing situations where particular protocols come into play and where temporary teams need to be convened. For example, dealing effectively with suspected child abuse involves: recognizing the clinical features, knowing about local arrangements for child protection, referring effectively and playing a part in assessment and continuing management including prevention of further abuse in the patient and family. There are many communication issues that are involved in this scenario, including how to raise the issue with the family while maintaining their trust and how to raise awareness in colleagues without encouraging prejudice.
Sharing information also refers to jointly discussing patient management as part of professional development and risk management. We may therefore contribute to regular significant event audits and case reviews. Additionally, in some circumstances such as suspected adverse reactions to drugs and suspected infectious disease, we should consider reporting our experience more widely.
We have now completed the ‘Relationship’ cluster of the competence framework; as you can see, it was not too difficult to grasp. In the next article, we will start thinking about ‘Diagnostics’ which brings together our core clinical skills.
More details are available from: