
Abstract
Multiple sclerosis is a chronic disabling neurological disease due to an autoimmune process of unknown cause. It is characterized by the formation of patches of demyelination (plaques) throughout the brain and spinal cord. There is no peripheral nerve involvement.
The GP curriculum and multiple sclerosis
Statement 15.7 of the GP curriculum (neurological problems) lists management of multiple sclerosis (MS) within the knowledge base that GPs in training must gain.
Manage primary contact with patients who have a neurological problem Co-ordinate care with other primary care health professionals, such as occupational therapists, physiotherapists and district nurses to enable chronic disease management and rehabilitation Describe the indications for referral to a neurologist for chronic conditions requiring ongoing specialist management, such as MS
Communicate prognosis truthfully and sensitively to patients with incurable disabling neurological conditions, such as MS, and share uncertainty when the patient wants this information Demonstrate empathy and compassion towards patients with incurable disabling neurological conditions Describe the importance of continuity of care for patients with chronic neurological conditions
Describe the current medical standards of fitness to drive for neurological conditions Describe the key national guidelines that influence health care provision for neurological problems
Epidemiology
Multiple sclerosis (MS) is the most common neurological disorder of young adults in the UK with a lifetime risk of around 1 in 1000. The peak age of onset is between 20 and 40 years and about twice as many women as men develop the disease. Men who develop MS tend to present later and have greater disability.
MS does run in families. Approximately one in five people who develop MS have an affected relative, and 4% of individuals with a first-degree relative with MS go on to develop the disease themselves. For this reason, it has been proposed that MS is caused by the action of an environmental factor, for example a virus, on a genetically susceptible individual. However, as yet, neither a specific gene nor a specific environmental trigger has been identified.
The prevalence of MS varies considerably throughout the world, with prevalence increasing with latitude. In the UK, around 85000 people have a diagnosis of MS. Within countries, Caucasians have a higher prevalence of MS than other racial groups.
Presentation of MS
MS is not a diagnosis that can be made in primary care. If a patient presents with symptoms or signs suggestive of MS, then refer for a specialist neurological opinion. Urgent referral should be made if there is an ongoing unexplained neurological deficit.
Take a careful history. The presenting features of MS vary considerably according to the area of the central nervous system (CNS) affected and can be both vague and transitory. The most common presenting features are summarized in Box 1. Symptoms may be worsened by heat or exercise. Although a patient usually presents with a single symptom, the history may reveal other episodes that have gone unheralded.
Whether or not to tell a patient about your suspicions that they might have MS prior to referral is a contentious issue. More than half of those referred to a neurologist with a potential diagnosis of MS are not found to have the disease. The right course of action is a matter of judgement and will depend both on the level of suspicion that you have that the patient has MS and also on the individual patient.

Optic neuritis: the optic disc appears swollen.
Diagnosis
NICE states that ‘the diagnosis of MS should be made clinically by a doctor with specialist neurological experience on the basis of evidence of CNS lesions separated in space and time, primarily on the basis of the history and examination’. There is no specific diagnostic test available to diagnose MS but, along with history and examination, information from magnetic resonance imaging (MRI) scans is very useful in assisting the neurologist to establish a diagnosis of MS. Plaques are shown on MRI scans as white spots (Fig. 2). Other tests less commonly used include evoked potential tests, particularly visual evoked potential tests looking for evidence of optic nerve damage and lumbar puncture looking for oligoclonal bands of IgG antibodies, which are present in the cerebrospinal fluid of over 95% of people with MS.
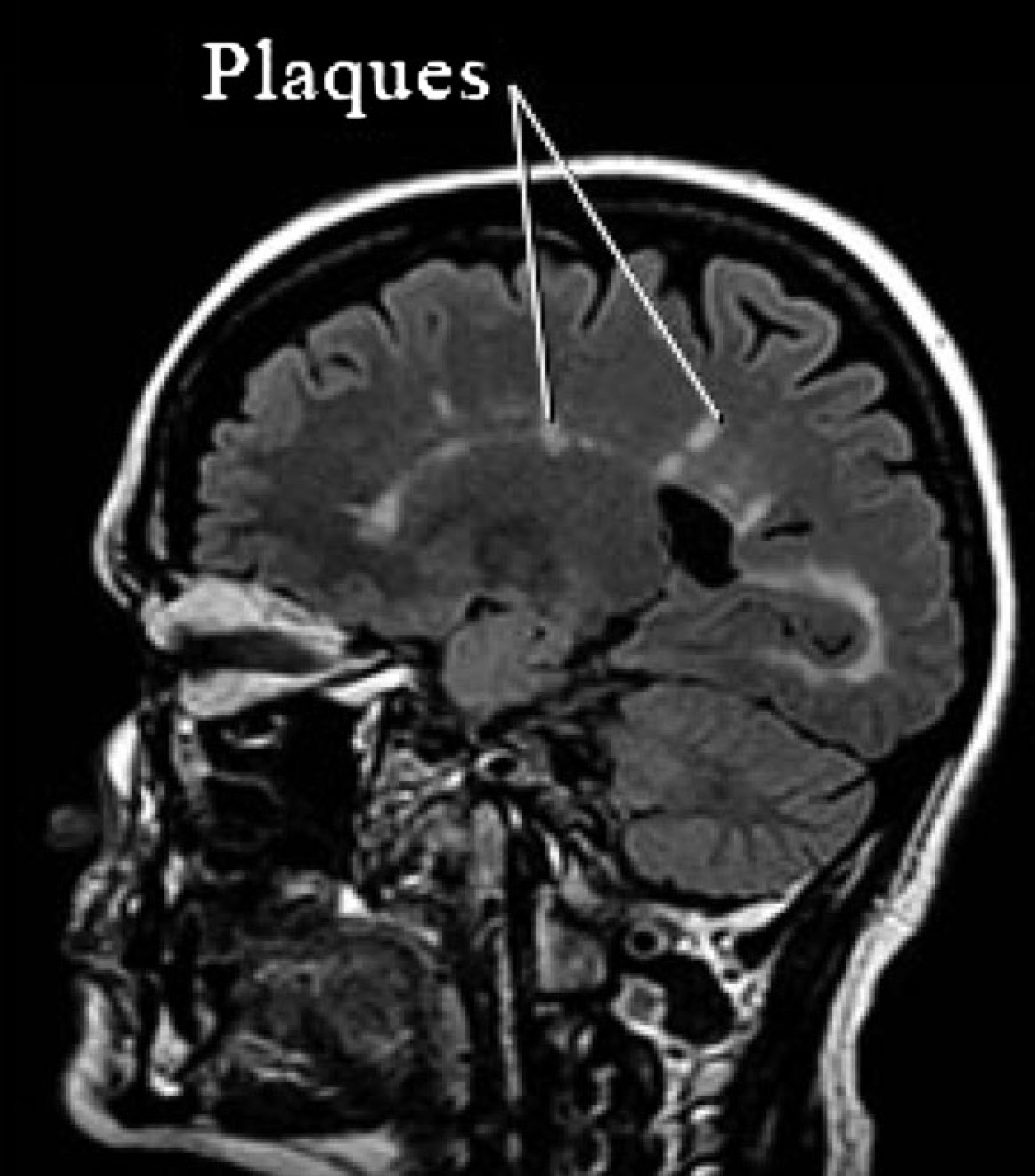
MRI scan of the brain of a patient with MS showing plaques.
Common presenting features of MS
Pain on eye movement and/or acute decline in visual acuity — this may suggest optic neuritis (Fig. 1). Optic neuritis is the presenting feature in 25% of patients with MS, and more than half of those who present with optic neuritis eventually go on to develop MS. National Institute of Clinical Excellence (NICE) recommends that anyone presenting with an acute reduction in visual acuity should be referred for urgent ophthalmology review. Double vision Poor balance or co-ordination Problems with speech — slurring or slow speech Dysphagia Sensory disturbances, such as numbness or tingling Pain —in particular, trigeminal neuralgia (intense stabbing pain in the trigeminal nerve distribution) may be associated with MS Motor disturbances—muscle weakness, stiffness or spasticity Transverse myelitis—inflammation of the spinal cord at a single level. Symptoms develop rapidly over days or weeks and include limb weakness, sensory disturbance, bowel and bladder disturbance, back pain and radicular pain. Bladder dysfunction—frequency, urgency or incontinence Constipation Sexual dysfunction—for example, erectile dysfunction Cognitive changes—for example, loss of concentration or memory problems Non-specific symptoms — for example, fatigue or depression
In the past, to make a diagnosis of MS, it was necessary to demonstrate a series of clinical neurological deficits distributed in time and space and not attributable to other causes. However, most plaques do not cause any new neurological symptoms or signs. Recent revisions in diagnostic criteria allow MRI evidence of new plaque formation to substitute for further clinical attacks, enabling earlier diagnosis.
MRI scan evidence of plaques is also used to assess the risk that an individual might develop MS in the future. For example, if a patient presents with an isolated attack of optic neuritis and there are no plaques on MRI scanning, his risk of developing MS within the next 15 years is 15%. If three or more plaques are present, this risk rises to 75%.
Patterns of MS
One of the features of MS is that it follows an unpredictable course within the same person and from person to person. However, there are five well-described patterns of illness.
Relapsing—remitting multiple sclerosis
This is the typical pattern of disease for 85% of patients in the early stages of their disease. It is characterized by acute ‘attacks’. These attacks are episodes of sudden increase in neurological symptoms or development of new neurological symptoms, with virtually complete recovery after 4–6 weeks. Recovery occurs as inflammation caused by the autoimmune process subsides, remyelination takes place and the brain reroutes impulses through unaffected pathways. With time, remissions become less complete and residual disability accumulates.
Secondary progressive multiple sclerosis
Fifteen years after diagnosis, about 65% of those MS patients with relapsing — remitting multiple sclerosis (RRMS) will have begun a continuous, sustained neurological deterioration that is completely independent of the effect of acute relapses. A diagnosis of secondary progressive multiple sclerosis (SPMS) can be made after this progressive deterioration has been present for more than 6 months. Acute attacks may still occur in addition.
Benign MS
This pattern is found in roughly 1 in 10 patients diagnosed with MS. The individual has a few mild attacks and then complete recovery. There is no deterioration over time and no permanent disability. It is only possible to make this diagnosis in retrospect, after a period of 10–15 years when a patient has experienced little or no disability.
Primary progressive MS
This pattern of MS affects about 10% of patients. There is a steady progression of neurological symptoms and signs from the outset with increasing disability.
Malignant MS
This is a rare pattern of MS that has a rapidly progressive course resulting within 5 years in severe disability or death.
Management — the role of the GP
Patients with MS benefit from a holistic approach to care through a multidisciplinary team, which includes the patient's GP. Within this team, the GP is usually the health care professional with whom the patient with MS has most contact. The importance of the role of the GP in providing co-ordination and continuity of care is emphasized both in the NICE guidance on management of MS and also the National Service Framework for long-term conditions. Where a GP has a special interest in MS, more specialized services for patients with MS can be provided in primary care as a National Enhanced Service.
The aims of treatment of MS are to reduce symptoms, increase quality of life and limit side effects of treatment. Include carers wherever possible. At each GP review consider
Can physical symptoms be improved? Remember both neurological and non-neurological symptoms Can psychological symptoms be improved? Can functioning within the home be improved? Consider aids and adaptations within the home and extra help Can functioning in the community be improved? Consider mobility outside the home, work and social activities Can the patient's or carer's financial state be improved? Review benefits Does the carer need more support? Consider providing information about or referral to voluntary and self-help organizations or social services
Other members of the multidisciplinary team may include the patient's neurologist, other members of the primary health care team, the specialist neurological rehabilitation team, the social services and/or the palliative care team. MS nurse specialists are often a vital link between the hospital system and community for the patient. They are invaluable sources of advice and support for patients and often very helpful to GPs who have queries about management.
Acute relapses
A relapse is defined as the appearance of new neurological symptoms or the recurrence of old symptoms, lasting for more than 24 hours, in the absence of fever or infection. Discuss any acute relapses with the MS nurse specialist and/or neurologist supervising care. Episodes causing distressing symptoms or increased limitation are often treated in primary care with high-dose steroids, for example oral methylprednisolone 500 mg − 2 g daily for 3–5 days started as soon as possible after the onset of the relapse. Alternatively, the patient may be admitted for high-dose intravenous steroids. If there is any residual deficit following the relapse, refer for specialist rehabilitation.
NICE guidance recommends that prolonged (for more than 3 weeks) or frequent (more than three times a year) steroid treatment should be avoided. Recent evidence has found that azathioprine is beneficial in reducing relapses and progression of MS and should be considered for patients requiring frequent doses of steroids.
Disease-modifying drugs
Patients who meet the Association of British Neurologists’ eligibility criteria (Table 1) may benefit from the disease-modifying drugs, beta interferon (Avonex, Rebif and Betaferon) or glatiramer acetate (Copaxone). These drugs reduce the frequency and/or severity of relapses by about 30% as well as slowing the course of MS. Prescription must be consultant led under the NHS risk sharing scheme. There is a Department of Health website (www.msdecisions.org.uk) designed to help patients decide which disease-modifying drug would be the best option for them.
Eligibility criteria for treatment of MS with disease-modifying drugs

New treatments
Natalizumab
Natalizumab (Tysabri) is a monoclonal antibody. It reduces the frequency and severity of relapses by about 68%. Natalizumab is recommended by NICE as an option for the treatment of rapidly evolving severe RRMS, defined by two or more disabling relapses in 1 year, together with specific MRI changes. Prescription must be consultant led. Administration of natalizumab is associated with an increased risk of opportunistic infection and progressive multifocal leucoencephalopathy (PML). If a patient on natalizumab develops new or worsening neurological symptoms or signs, it is important to refer immediately back to the neurologist supervising care to exclude PML.
Mitoxantrone
Mitoxantrone (Novantrone) is licensed in the USA for the treatment of aggressive RRMS and progressive forms of the disease. It is licensed in the UK for the treatment of leukaemia and lymphoma, but occasionally used ‘off licence’ by specialist neurologists for the treatment of severe MS. It works by suppressing the activity of the immune system and may reduce the freguency of relapses by up to 80%. However, its use is limited by nasty side effects-opportunistic infections, cardiotoxicity (after 2–3 years of use) and leukaemia (risk is 1 in 400).
Alemtuzumab
Alemtuzumab (CAMPATH-1H) is licensed in the UK for the treatment of chronic lymphocytic leukaemia. It works by destroying T cells. It is currently in the final phases of drug trials for treatment of MS and seems to be particularly effective for treatment of aggressive MS. It carries the risk of development of other autoimmune problems, in particular Graves’ disease.
Cannabinoids
There is a great deal of anecdotal evidence of the beneficial effects of cannabis in the treatment of the symptoms of MS, in particular spasticity, tremor, bladder problems and pain. In addition, claims have been made that cannabinoids might exert an overall neuroprotective effect. However, the largest study to date (the Cannabinoids in Mutiple Sclerosis Study) had mixed results and concluded that further research was needed.
Lamotrigine
It is thought that the anti-epileptic drug, lamotrigine, may have a neuroprotective effect that could be used in the treatment of SPMS. A preliminary trial is almost complete.
Diet
NICE recommends supplementing the diet with 17–23 g a day of linoleic acid (a polyunsaturated fat) on the basis that it might slow progression of disability. Rich sources of linoleic acid include sunflower, corn, soya and safflower oils. However, a more recent Cochrane review did not demonstrate any benefit.
Management of symptoms and disability
The GP has a major role to play in the detection and management of symptoms and disability in patients with an established diagnosis of MS through regular review. A disease register and call-recall system may help to achieve this goal. Always remember that you, as a GP, are part of the multidisciplinary team and liaise closely with the other members of that team.
New symptoms or limitations
If a patient with MS presents with new symptoms or signs, consider
Is it due to an unrelated disease? For example, extreme tiredness could be due to MS, but equally could be caused by anaemia or hypothyroidism Is it due to an incidental infection? For example, urinary tract or chest infection. Sometimes this is difficult to decide, as a viral infection may trigger a MS relapse Is it due to the MS? Is the patient having a relapse? Is it due to a side effect of treatment? Is it part of a gradual progression of the patient's MS?
Treat any cause of deterioration identified. If no cause is found, consider re-referring for specialist review and/or referring to the multidisciplinary rehabilitation team involved with the patient.
Pain
Pain syndromes affect 45–65% of people with MS. Most pain arises from reduced mobility. Other causes include premorbid disease (such as osteoarthritis), central pain due to neurological damage and neuropathic pain. Chronic pain, especially central pain, may respond to gabapentin [up to 600 mg three times daily (tds)] or tricyclic antidepressants such as amitriptyline (10–75 mg daily). Peripheral pain may respond to simple analgesia and/or physiotherapy. Refer patients with intractable pain to the specialist pain management clinic.
The use of cannabinoids for relief of pain and muscle spasm in patients with MS is controversial. Savitex is a cannabisbased oromucosal spray for the relief of neuropathic pain. It may be imported from Canada for prescription to individual patients in the UK as an unlicensed medicine on a named patient basis. Contact the prescribing adviser at your Primary Care Organization for guidance on prescribing.
Motor problems
Muscle weakness may occur as a result of the neurological effects of MS. Ataxia is common and may affect the ability of the individual to perform everyday tasks. Tremor occurs typically 5–15 years after the first symptoms of MS appear and may take the form of either an intention or postural tremor.
In all cases, aim to maintain physical independence:
Involve physiotherapy — often only two or three visits are needed to improve motor functioning Involve occupational therapy—a task-oriented approach is used (e.g. learning how to dress). Occupational therapists can also supply and/or advise on aids and appliances, such as Velcro fasteners, wheelchairs, adapted cutlery, etc. Refer for social services occupational therapy assessment if aids, equipment or adaptations are needed for the home Refer for home care services as necessary Give information about driving and/or employment where appropriate
Spasticity and contractures
Patients with persistent spasticity or spasms should be referred for specialist physiotherapy assessment. Treatment is usually with passive exercises and splinting to prevent contractures.
First-line anti-spasticity drugs are baclofen (5 mg tds or rarely through a pump) or gabapentin (up to 600 mg tds). If these treatments are ineffective or side effects prohibit their use, second-line treatments include dantrolene [25 mg once daily (od)], tizanidine (2 mg od), diazepam (2–10 mg tds) and clonazepam (1–8 mg at night). Combinations of anti-spasticity drugs should only be used on consultant advice.
Botulinum toxin can be directed at specific muscles. Refer via the specialist rehabilitation team.
Communication problems
Among patients with MS, about 50% have some symptoms of dysarthria. Dysphasia is much rarer and usually occurs in association with severe cognitive problems. In all cases, speech and language therapy assessment is vital. Consider support via dysphasia groups and communication aids (take advice from speech therapy and occupational therapy).
Poor vision
Problems with vision are common among patients with MS. Many are self-limiting but in some cases, symptoms may persist:
If visual acuity is reduced, refer to an optician in the first instance. If corrected vision is still poor, refer for ophthalmology review If nystagmus is causing reduced visual acuity, refer to a specialist ophthalmologist or neurologist for a time-limited trial of treatment with oral gabapentin If the patient is unable to read or watch television despite treatment, refer to an ophthalmologist for consideration of registration of blindness or partial sight. This will enable access to the appropriate specialist social services team and assessment for low-vision equipment and adaptations
Bowel problems
Bowel dysfunction affects 60% of patients with MS. The most common bowel symptoms in MS are constipation and faecal incontinence. These frequently coexist. Constipation occurs when there is difficulty with defaecation or bowels open less than twice a week. Initially increase fluid intake and fibre in the diet. If there is no improvement with these measures, consider prescribing a regular oral laxative and/or regular suppositories or enemas. Involve the district nursing team as needed.
Faecal incontinence can be devastating both for the patient with MS and the carers. It is one of the most common reasons cited for breakdown of the home situation and the need for permanent admission to residential care. Exclude overflow incontinence secondary to constipation. Refer early for specialist continence advice.
Dysphagia is a symptom of brainstem dysfunction and is estimated to affect 43% of patients with MS at some point. Fluids are more difficult to swallow than semisolids. Formal assessment by a trained speech and language therapist is essential. Feeding through nasogastric tube or percutaneous endoscopic gastrostomy may be needed long or short term. In the terminal phases of MS, weigh provision of nutrition against prolongation of poor-quality life.
Bladder problems
Urine storage and emptying problems are very common among patients with MS. These result in urgency, nocturia and incontinence. Patients often suffer from frequent urinary tract infections (UTIs). In any patient presenting with new or changed bladder symptoms, consider UTI and send a sample to the laboratory for microscopy, culture and sensitivity. Treat any infection present. If the patient has more than three proven UTIs within the space of a year, refer to the specialist incontinence service or a urologist for further assessment. If bladder symptoms continue once any UTI has been treated, measure the post-micturition residual bladder volume.
If the bladder volume is under 100 ml and the patient has symptoms of urgency, then consider a trial of anti-cholinergic medication such as tolterodine 2 mg twice daily or oxybutynin 5 mg tds. If symptoms are still not settling, then refer for specialist assessment If the bladder volume is greater than 100 ml, consider referral to a specialist continence service or urologist for advice about the possibility of intermittent self-catheterization
Nocturia can be effectively treated with desmopressin (100–400 mcg orally). Desmopressin can also be used if needed to control daytime frequency of micturition, for example to cover long journeys or exams, but must never be used more than once in 24 hours.
Incontinence can be a very distressing symptom and result in skin breakdown if the patient is immobile. Refer anyone with MS who has persistent incontinence, despite treatment of UTI and/or treatment of urgency, to a specialist continence service for advice and assessment.
Sexual and personal relationships
Problems with sexual and personal relationships are common among people with MS: 70–80% of men experience erectile dysfunction and 56–72% of women have sexual difficulties. For men, offer treatment with a phosphodiesterase type 5 inhibitor, such as sildenafil. Consider referral for specialist advice. A useful information sheet about sexual problems in patients with MS is available from website: www.outsiders.org.uk/leaflets/sex-and-ms.
Fatigue and weakness
Fatigue and weakness are a prominent feature in 85% of patients with MS and can be very debilitating. Explore the nature of the symptoms and controllable factors that might be contributing to it, such as depression, chronic pain, disturbed sleep or poor nutrition. Treat any exacerbating factors and review support and medication. Encourage graded aerobic exercise, involving the community and specialist rehabilitation services as appropriate.
Drug treatment of fatigue and weakness is of limited effectiveness. amantadine (unlicensed) has little effect over placebo. Modafinil is licensed to treat excessive daytime sleepiness in patients with MS and may have a useful effect.
Depression and anxiety
More than half of all patients with MS will experience a major depressive episode at some stage, and the suicide rate among MS patients is up to 7.5 times higher than that of the general population. Furthermore, around 40% of carers of patients with MS also have depression as measured with screening tools.
It can be difficult to detect depression in patients with MS as many of the symptoms of depression overlap with the symptoms of MS. For example, fatigue may be a symptom of both, as may poor concentration. The NICE depression screening questions (Box 2) are a useful tool for identifying patients who may be suffering from depression. A positive response to either question should prompt further investigation, for example with the PHQ-9 depression screening questionnaire.
NICE depression screening questions
During the last month, have you often been bothered by feeling down, depressed or hopeless? During the last month, have you often been bothered by having little interest or pleasure in doing things?
Give both the patient and his or her carers opportunities to talk about the impact of the illness on their lifestyle. Jointly identify areas where positive changes could be made, for example referral to day care to widen social contact. Consider referral for counselling or to a self-help or support group. Depending on the severity of symptoms and the patient's wishes, consider antidepressant medication and/or referral to psychiatric services.
Emotionalism
If the patient cries (or laughs) with minimal provocation, consider emotionalism — impairment in the control of crying. If emotionalism causes concern or distress to the person with MS or their family, consider treatment with a tricyclic antidepressant (e.g. amitriptyline 10–75 mg daily).
Cognitive impairment
About 50% of people with MS may have impaired ability to learn and remember, plan, concentrate and handle information. If this becomes apparent, review medication to ensure that there is no iatrogenic reason for reduced cognitive functioning. Assess for depression and treat if found. Consider referral for specialist assessment.
Respiratory infections
Respiratory infections are common in patients with significant neurological deficit. Treat any infection early with antibiotics unless the patient is in the terminal stages of MS. Offer a single pneumococcal vaccination and annual influenza vaccination to all patients with MS. If the patient has any ongoing disability, the patient's carer is also eligible for annual influenza vaccination.
Venous thromboembolism
Venous thromboembolism is common in immobile patients, but clinically apparent in less than 5%. Ensure adequate hydration and encourage mobility. Consider the use of aspirin 75–150 mg od and compression stockings if the patient is immobile. Prophylactic anticoagulation does not improve outcome.
Skin breakdown
Every person with MS who uses a wheelchair should be assessed for risk of developing a pressure ulcer. Skin breakdown is prevented by positioning, mobilization, good skin care, management of incontinence and pressure-relieving aids (e.g. special mattresses and cushions). Involve the community nursing services.
Driving
Patients with MS must inform the Driving and Vehicle Licensing Authority and their insurance company of their diagnosis of MS. They can be licensed to drive a car if medical assessment confirms driving performance is not impaired — but a short period licence may be required. If the driver requires a restriction to certain controls, this must be specified on the licence. Patients with MS who have a Group 2 licence may be considered for licensing subject to a satisfactory medical report and annual review if they are stable and their driving is not impaired. A list of insurance companies that will cover a disabled driver is available from website: www.radar.org.uk.
People receiving the higher rate mobility component of Disability Living Allowance can claim road tax exemption for one vehicle, whether they drive the vehicle or will just be transported in it and access the Motability Scheme (www.motability.co.uk). Powered wheelchairs and mobility scooters are also available through the Motability Scheme.
Pregnancy
MS often affects women of child-bearing age and questions about the possibility of becoming pregnant once a diagnosis of MS has been made, and the effects that the pregnancy might have on the MS are common. MS does not affect fertility. In most cases, symptoms will stabilize or improve during the pregnancy, but there is some evidence that relapses are slightly more common in the first 3 months following delivery. There is no data on the safety of disease-modifying drugs in pregnancy, and it is advised that these drugs should be stopped at least 12 months prior to conception. Refer for pre-conceptual counselling to the patient's specialist neurologist.
The patient as an individual
A diagnosis of MS can be devastating. The patient is often young and has usually been previously fit and healthy. A diagnosis of MS not only threatens the individual with disability and loss of independence but also loss of social interaction, loss of work, loss of income and diminished potential.
Each patient with MS is part of a family unit. Everyone within that family will be affected by the patient's MS. The spouse, a parent or sometimes even a child becomes the patient's informal carer. Carer support is an important role for the GP and primary health care team.
The Multiple Sclerosis Society (telephone: 0808 800 8000; website: www.mssociety.org.uk) lists sources of information and support for both patients and families and also provides excellent information for health care professionals. Advise patients and carers to apply for all benefits that they may be eligible for. Up-to-date information about benefits for disabled people and carers is available from website www.direct.gov.uk/disability, and further information and advice on benefits, employment matters and many other topics is available from the Citizen's Advice website (www.adviceguide.org.uk).
Perhaps the most important role of the GP is to be supportive and open. Being approachable, together with explanation, information provision, prompt action when investigation or treatment is needed and honesty in situations where you cannot help, will make a major difference.
Prognosis
Factors associated with prognosis are listed in Box 3. However, none of these factors is a sufficiently robust predictor of outcome to be used to predict the course of the disease for any individual.
At onset, it is often impossible to predict the level of disability that a patient will suffer. As a rough guide, one in three patients with RRMS will still be working 15–20 years after diagnosis. When the primary diagnosis is RRMS, the average time from diagnosis until a wheelchair is needed is 20 years. This means that many patients never need a wheelchair. Even in patients with a diagnosis of primary progressive MS, the average time until a wheelchair is needed is 6–7 years. These figures are likely to improve with the increased use of disease-modifying drugs. Life expectancy for patients with MS is reduced by 6–11 years on average, although death is only rarely directly due to MS and is more usually as a result of urinary or chest infection.
Factors associated with prognosis for patients with MS

Key points
MS is a common, debilitating neurological condition, affecting women more frequently than men and with peak onset between the ages of 20 and 40 years MS is characterized by neurological deficits distributed in time and space and not attributable to any other process. Five distinct patterns of disease progression occur If a diagnosis of MS is suspected, refer for specialist confirmation and supervision of ongoing care through a multidisciplinary team Treatment of MS involves the management of acute relapses, reduction in disease progression using disease-modifying drugs and the assessment and management of symptoms and disability Ongoing management in primary care includes regular review of all patients with MS. A register of patients and call-recall system may help.