
Abstract
Acute gastro-intestinal (GI) bleeding is defined as bleeding into the GI tract. GI bleeding is a common medical problem that can vary in presentation from being an insidious chronic blood loss to being potentially life threatening. Although 80% of acute GI bleeds stop spontaneously, it is essential to determine the source of bleeding and establish a diagnosis in order to attempt to prevent a recurrence and so that the most appropriate management may be given in future episodes. Also, an accurate diagnosis will allow a patient to be treated optimally for the underlying condition.
The GP curriculum and GI bleeding
GP curriculum statement 15.2 outlines the GP's roles and responsibilities in digestive problems and curriculum statement 7 outlines the GP's role and responsibilities in care of acutely ill people. From these statements, a GP must
Be able to manage primary contact with patients who have a digestive problem—this includes haematemesis, melaena and rectal bleeding Know about the symptoms of haematemesis, melaena and rectal bleeding Know about the acute management of haematemesis and melaena Be able to prioritize problems and establish a differential diagnosis, make the patient's safety a priority and consider the appropriateness of interventions according to patients' wishes, the severity of the illness and any chronic or co-morbid diseases Keep resuscitation skills up to date and act calmly in emergency situations, following agreed protocols Decide whether urgent action is necessary, thus protecting patients with non-urgent and self-limiting problems from the potentially detrimental consequences of being over-investigated, over-treated or deprived of their liberty
As a GP, it is important to distinguish whether a patient presenting with a gastro-intestinal (GI) bleed requires urgent admission or not. Initial triage and assessment are crucial to identify the sick patient with life-threatening haemodynamic compromise and initiate appropriate resuscitation. This article will review the causes of both upper and lower GI bleeding, risk factors and discuss how a GP might manage this condition appropriately.
Epidemiology
In the UK, acute upper GI bleeding accounts for approximately 25000 emergency hospital admissions each year. The incidence of acute upper GI bleeding in the UK ranges from 50 to 190/100 000/year and is highest in areas that are socially deprived. The mortality of patients admitted to hospital for acute GI bleeding is about 10%, rising to more than 30% in patients who bleed as inpatients. Most deaths occur in the elderly patient with significant co-morbidity.
Presentation
The presentation of GI bleeding depends on the acuteness and site of bleeding.
Chronic blood loss
Chronic slow blood loss from anywhere along the GI tract may present without any obvious bleeding and result in iron deficiency anaemia. This may be detected incidentally or present with symptoms or signs of anaemia, such as tiredness, pallor, weakness, shortness of breath or angina. Small amounts of blood loss in the stool can be detected by a faecal occult blood test.
Acute blood loss
Anatomically, upper GI bleeding originates proximally to the ligament of Treitz. In practice, this is from the oesophagus, stomach and duodenum. Lower GI bleeding originates from the small bowel and colon. Fig. 1 shows the position of the ligament of Treitz.
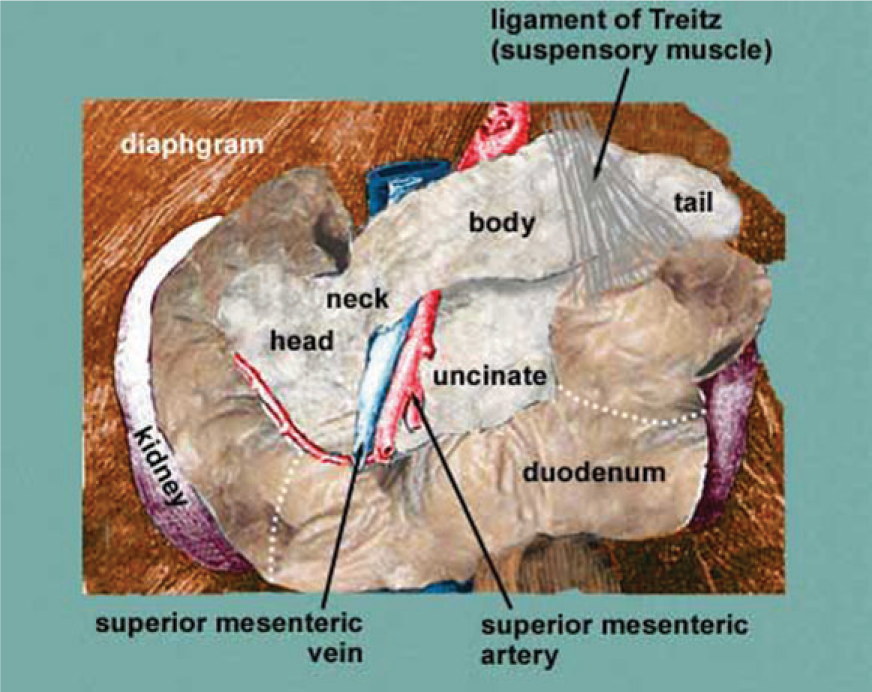
Position of the ligament of Treitz.
Haematemesis is vomiting of blood from the upper GI tract. Bright red blood usually implies an active bleed from the oesophagus, stomach or duodenum. Coffee-ground vomitus is vomiting of altered black blood. This implies that the bleeding has ceased or has been relatively modest.
Melaena is the passage of black tarry stools due to an acute GI bleed but can very occasionally be from the small bowel or (very rarely) right side of the colon. Patients who present with haematemesis tend to have worse bleeding than those who present with melaena alone. Only about 50% present with haematemesis alone, 30% with melaena alone and 20% with both.
Haematochezia is the passage of fresh or altered blood per rectum usually due to colonic bleeding, but can occasionally be due to profuse upper GI or small bowel bleeding. Mixed blood and stool implies bleeding proximal to the sigmoid colon, blood around the stool implies a more distal bleed and blood on the toilet paper or in the pan not mixed with stool is often from anal bleeding due to haemorrhoids or an anal fissure.
Acute bleeding is much more likely to present with the signs of shock—on occasions before the bleeding becomes apparent. It is important to remember that anyone presenting with acute GI bleeding can deteriorate very suddenly, and someone who is initially haemodynamically stable can go into hypovolaemic shock without any warning. The absence of signs at presentation is no guide.
Causes of upper GI bleeding
A cause for upper GI bleeding is found in about 80% of cases (Table 1). The most common cause of a non-variceal upper GI bleed is peptic ulcer disease (Fig. 2) and accounts for up to half of all cases found at emergency endoscopy. Aspirin or non-steroidal anti-infl ammatory drug (NSAID) use is common in these patients, as is infection with Helicobacter pylori. Signifi cant haemorrhage results from the break down of an underlying artery and the magnitude of the bleed is related to the size of the arterial defect and the diameter of the artery. Large bleeding vessels cause faster blood loss and these are common in the lesser curvature of the stomach and the posteroinferior part of the duodenal bulb. Bleeds from gastric erosions, oesophagitis or arterio-venous malformations usually stop by themselves and are not life threatening.

Duodenal and gastric ulcers at endoscopy.
Summary of causes of GI bleeding

About 11% of patients undergoing endoscopy for upper GI bleeding have varices. Variceal bleeding occurs from dilated veins at the junction between the portal and systemic venous systems. These are most commonly found in the distal oesophagus (Fig. 3) but may alternatively or additionally be found in the proximal stomach. Variceal haemorrhage should be suspected when there is a history of previous variceal bleeding, known liver disease or when examination has revealed stigmata of chronic liver disease or portal hypertension. These include presence of jaundice, ascites, splenomegaly, encephalopathy, caput medusae and/or spider naevi. In patients with liver disease, the severity of the varices is closely related to the severity of the liver disease.

Oesophageal varices.
Other less common causes of upper GI bleeding include
Mallory-Weiss tears—these are common in the young, usually due to persistent coughing or severe retching and vomiting, often after an alcoholic binge. Bleeding often stops spontaneously without any need for active intervention. Aorto-duodenal fistula—consider in patients with a history of abdominal aortic aneurysm surgery who develop profuse bleeding A Dieulafoy's lesion—an aberrant submucosal artery erodes into the lumen of the stomach. This is a rare cause of upper GI bleeding.
Causes of lower GI bleeding
It is important to note that about 15% of patients with acute severe haematochezia will have an upper GI source of bleeding. Lower GI bleeding is more prevalent in the elderly and in men. A large majority of lower GI bleeds stops spontaneously. Common causes of lower GI bleeding are diverticulae, angiodysplasia, colitis, neoplasia and benign anorectal diseases such as haemorrhoids and anal fissures (Table 1).
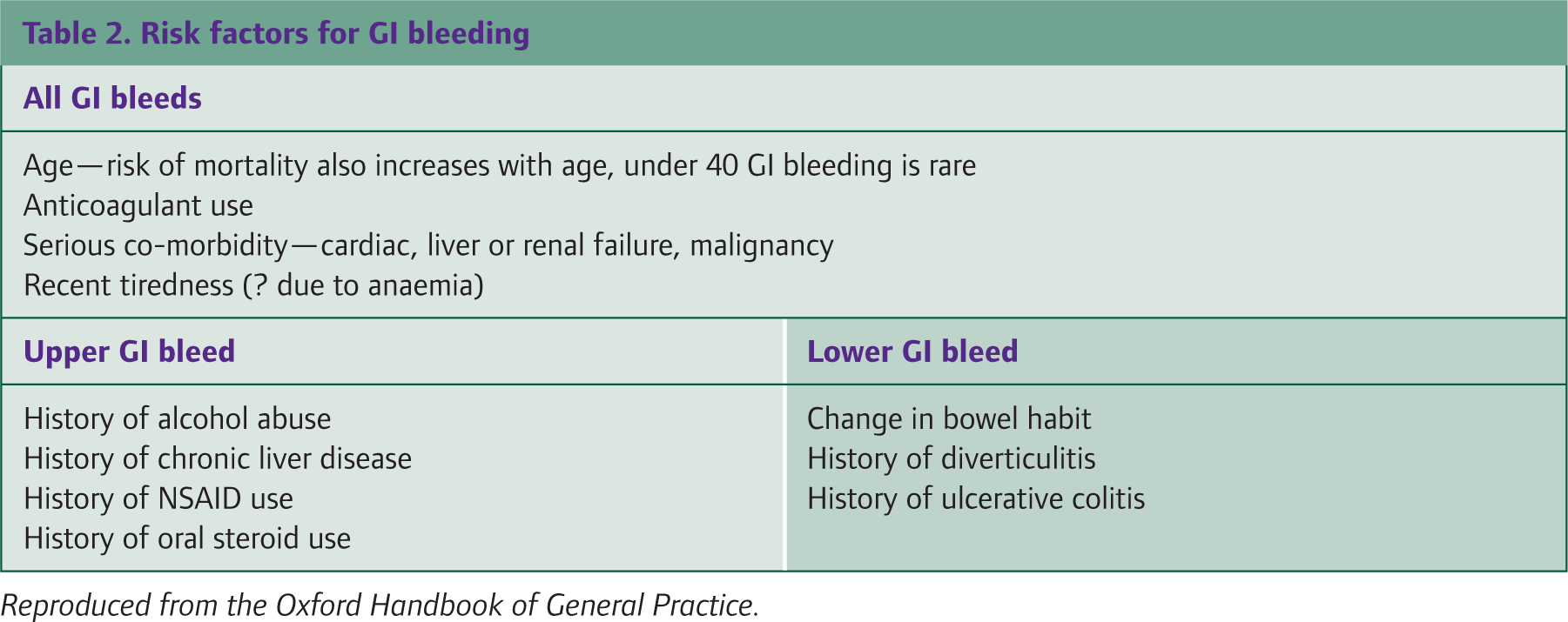
Risk factors for GI bleeding
There are various risk factors that are associated with both upper and lower GI bleeding specifically and then some that are common to both. These are related to the causes of bleeding and are summarized in Table 2.
Risk factors for GI bleeding
Assessment
In the assessment of patients with recognized or suspected upper GI haemorrhage, it is necessary to immediately identify those at highest risk, particularly those presenting with hypovolaemic shock. Take a history (Box 1) and examine the patient. Important clues as to the aetiology of a bleed may be available from the history, for example retching might suggest a Mallory-Weiss tear, weight loss may indicate malignancy and chronic alcohol excess suggests the possibility of varices.
Examination
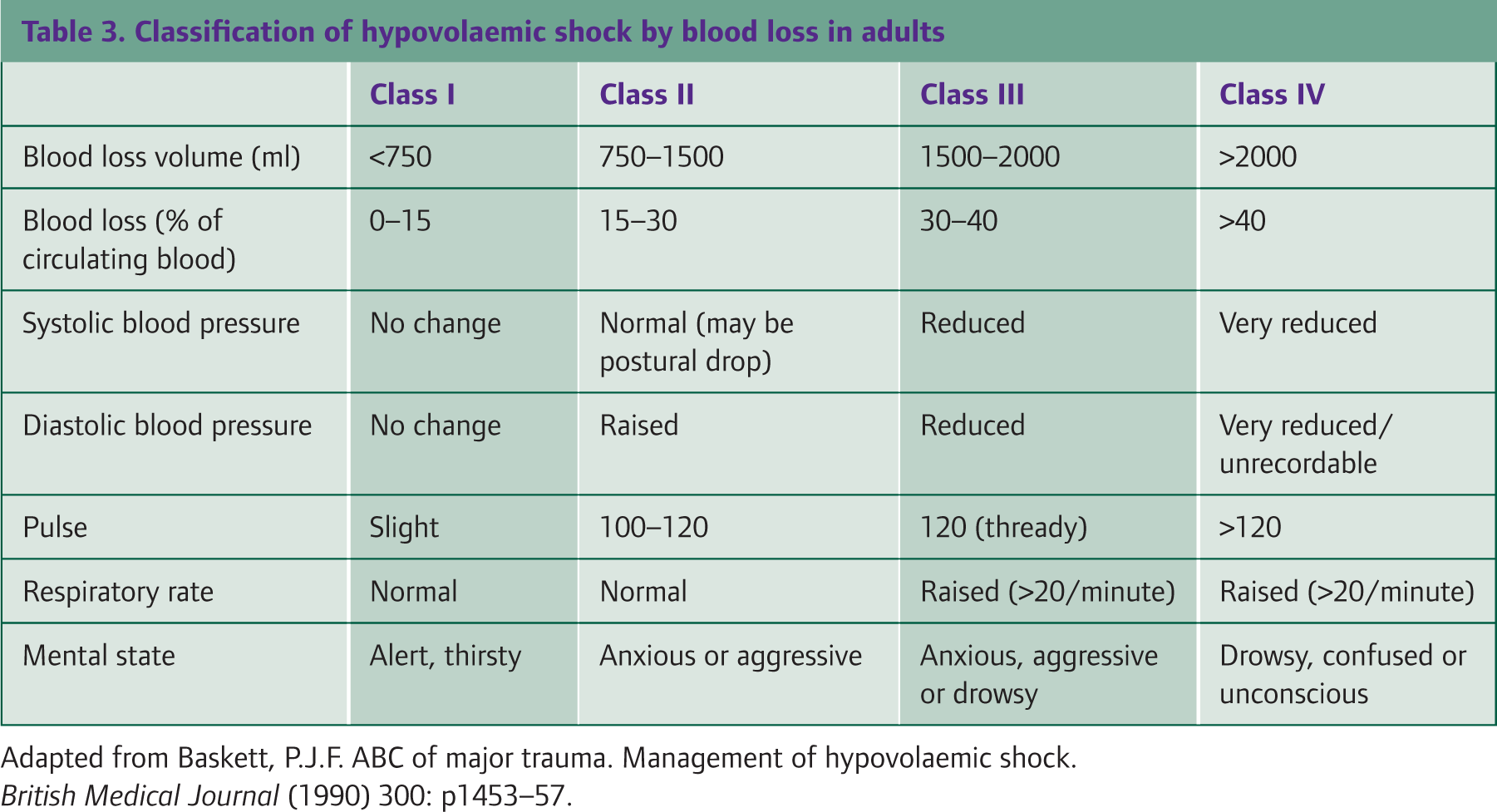
The aim of examination is not only to assess blood loss and signs of shock but also to look for signs of significant co-morbid conditions and underlying disease. Examine the vomitus or stool if possible. Measure and record the pulse, blood pressure (including postural drop if this is appropriate), respiratory rate and behaviour of the patient. Table 3 describes the expected changes in these parameters with increasing acute blood loss. All acute GI bleeding is considered major when accompanied by haemodynamic instability. In addition, and if clinically appropriate, check for
Pallor and signs of anaemia Other signs of shock such as chest pain, cool, clammy skin and oliguria Signs of dehydration such as sunken eyes, reduced skin turgor and dry mucosa Evidence of blood or melaena within the rectum, anal fissure, haemorrhoids or a rectal mass Stigmata of liver disease such as jaundice, ascites, spider naevi and liver flap Signs of a tumour such as an abdominal mass or hepatomegaly
Classification of hypovolaemic shock by blood loss in adults
Points to cover when taking a history
When did the bleeding begin? Where does the visible bleed originate from? Is there a history of GI disease? Is there any abdominal pain? Is there a history of other GI symptoms?
Haematemesis including coffee-ground vomitus —colour, quantity and features of the bleed Melaena Haematochezia Syncope Pre-syncope Dyspepsia Epigastric pain Diffuse abdominal pain Weight loss Jaundice Any past history of any bleeding or of anaemia? Is there a history of bleeding disorder? Is there a history of liver disease or any abdominal surgery? What is the patient's alcohol intake? Is the patient on any medications? Particularly ask about anticoagulants, NSAIDs, aspirin (or other antiplatelet therapy), corticosteroids, selective serotonin reuptake inhibitors and bisphosphonates. Iron tablets and bismuth can mimic melaena. Calcium channel or beta blockers could mask tachycardia if the patient is in shock.
First aid
If you suspect a significant acute GI bleed and the patient does not have a terminal disease where this would be considered a terminal event, arrange immediate transfer to hospital. If the history of a significant GI bleed is given to you over the telephone, arrange an emergency ambulance for the patient immediately and before visiting. If you are with the patient or can get to the patient quickly, start initial resuscitation while awaiting the ambulance:
Position—lie the patient flat and lift his legs higher than his body, except if vomiting when place in the recovery position Airway—ensure that the airway is clear and free from vomitus. Give oxygen if available. Breathing—monitor respiratory rate Circulation—monitor skin colour, peripheral temperature, pulse rate, capillary refill time, blood pressure and electrocardiogram (if available). If at all possible, gain intravenous access with two wide-bore cannulae and take blood for a full blood count, clotting screen and cross match at the same time—the opportunity may be lost by the time the paramedic crew arrive. Give intravenous fluids, if available, to expand circulating volume with either colloid or crystalloid.
When to refer
If a patient presents with an acute severe GI bleed, then, unless it is the terminal event in a palliative care situation, admit immediately as an acute emergency by ambulance. Upper GI bleeds are usually considered a medical emergency and lower GI bleeds a surgical emergency. The decision about what to do is more difficult if either the bleeding was some time ago or the bleeding is minor and not compromising the patient.
Upper GI bleeding
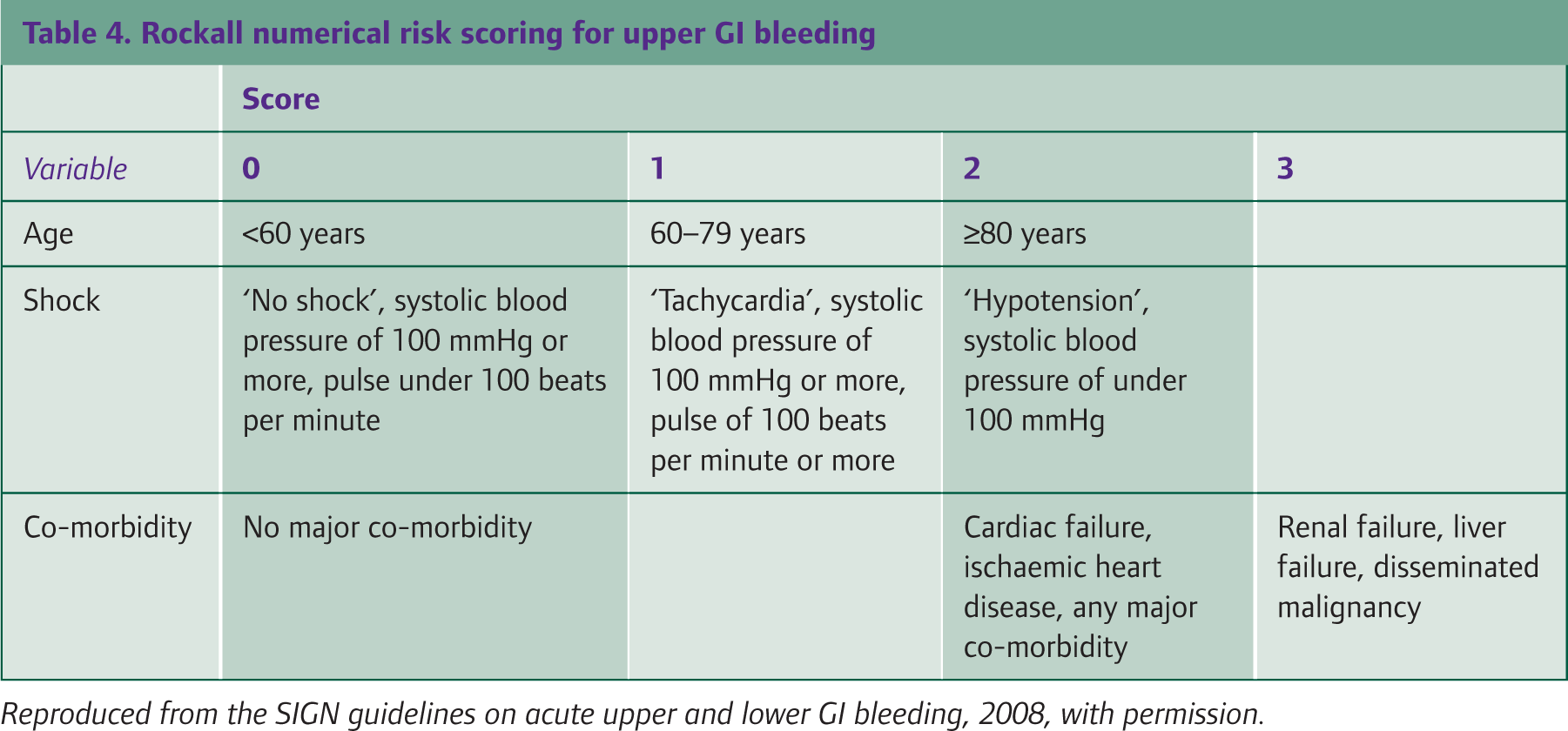
There are scoring systems for upper GI bleeding, such as the Rockall score (Table 4), for use in hospital settings to identify patients admitted with a history of upper GI bleeding at high risk of rebleeding and/or death. A Rockall score of a score of less than 3 has an excellent prognosis; however, a score of greater than 8 is associated with a high risk of death. One of the recommendations for future research in the 2008 SIGN Guidelines on GI bleeding is to determine whether an initial Rockall score of 0 or 1 could be used for GP triage to determine the patients not requiring admission.
Rockall numerical risk scoring for upper GI bleeding
Until then, there are no validated criteria for use in primary care; however, it would be reasonable to consider referral to the gastroenterology team for outpatient endoscopy and/or further investigation if
There is no evidence of haemodynamic disturbance (systolic blood pressure of 100 mmHg or more and pulse of less than 100 beats per minute) There is no significant co-morbidity (particularly liver disease, cardiac disease or malignancy) and There has been no haematemesis, haematochezia or melaena within the past 2 days
Have a lower threshold for admission if the patient is elderly or has poor social support. If you decide that the patient can remain at home, always advise the patient and/or carers to call for help, either by ringing the GP surgery or by dialling for an emergency ambulance, if there is any further bleeding or if the patient becomes unwell in any way. Consider starting a proton pump inhibitor (PPI) in patients remaining in the community, if the patient complains of symptoms of reflux or epigastric pain and does meet the criteria for urgent referral for endoscopy. PPIs should be discontinued 2 weeks prior to endoscopy.
Lower GI bleeding
Empirically rectal bleeding is a common symptom, particularly in general practice. Few patients with rectal bleeding require hospital admission. There are no criteria for deciding which patients with lower GI bleeding can be investigated as an outpatient and which need emergency admission. It is reasonable to consider management in the community if
There is no evidence of recent gross rectal bleeding and There is no evidence of haemodynamic disturbance (systolic blood pressure of 100 mmHg or more and pulse of less than 100 beats per minute)
Have a lower threshold for admission if the patient is elderly or has poor social support. If you decide that the patient can remain at home, always advise the patient and/or carers to call for help, either by ringing the GP surgery or by dialling for an emergency ambulance, if there is any further bleeding or if the patient becomes unwell in any way.
The National Institute of Clinical Excellence recommends referral (Fig. 4) to a team specializing in lower GI cancer for urgent outpatient investigation (within 2 weeks) if a patient
Of any age has unexplained iron deficiency anaemia (haemoglobin of 11 g/dl or less for a man or 10 g/dl or less for a non-menstruating woman) Aged 40 years or older reports rectal bleeding with a change of bowel habit towards looser stools and/or increased stool frequency that persists for 6 weeks or more Aged 60 years or older reports rectal bleeding persisting for 6 weeks or more Of any age where a rectal mass is found on rectal examination or abdominal mass is found on abdominal examination
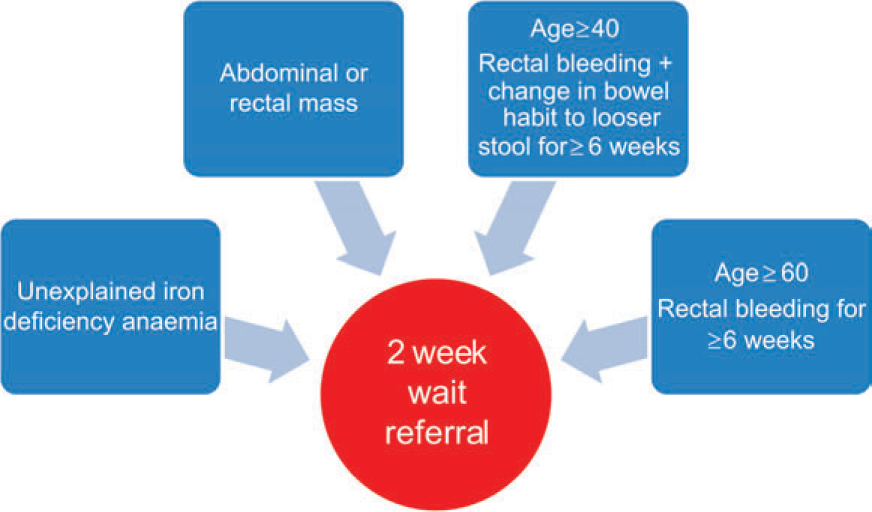
National Institute of Clinical Excellence urgent referral criteria for patients presenting with lower GI bleeding.
Otherwise, evaluate the patient on a case-by-case basis. If there is an obvious benign cause for the bleeding, such as an anal fissure or a bleeding haemorrhoid, then reassure the patient and provide appropriate treatment. If the cause of the rectal bleeding is not an anal fissure or haemorrhoids and the patient is otherwise well, refer for routine investigations.
Key points
GI bleeding, and particularly lower GI bleeding, is a common presenting complaint in general practice Initially, it is important to assess the severity of the bleed Rapid resuscitation and admission to hospital are vital in a patient with severe GI bleeding For less severe bleeding or delayed presentation, there are no clear criteria for deciding whether a patient should be admitted as an emergency or managed in the community, with outpatient referral as appropriate. Judge each case individually. Have a lower threshold for admission if the patient is elderly, has other co-morbidities or has poor social support Follow-up patients not admitted as needed with outpatient investigation