
Abstract
A full blood count is one of the common blood tests requested by GPs. Anaemia is frequently found, whether suspected or incidental. This article aims to guide your thinking about how to assess and investigate anaemia in adults and when to refer.
The GP curriculum and anaemia
There are no specific chapters on anaemia in the GP curriculum but anaemia may be a feature of many conditions, including renal disease, malignancy and pregnancy, and is common among older patients. Specific mentions of anaemia within the GP curriculum include
RCGP Curriculum statement 15.2 on digestive disorders includes the learning objective relevant to iron deficiency anaemia: Explain the indications for urgent referral to specialist services, especially for patients with suspected gastro-intestinal (GI) cancer.
RCGP Curriculum statement 6 on Genetics in Primary Care: Demonstrate an awareness of the genetic aspects of antenatal and newborn screening programmes (e.g. Down's syndrome, sickle cell and thalassaemia) and know their indications, uses and limitations.
Strategy for investigation of anaemia
The World Health Organization defines anaemia as haemoglobin less than 13 g/dl in men or less than 12 g/dl in women. The causes of anaemia (Table 1) include acute and chronic blood loss, increased destruction by haemolysis and decreased production due to haematinic deficiency, bone marrow failure, hereditary and congenital causes.
Types of anaemia

The key indices to consider are mean cell volume (MCV) and the time course of anaemia (see Table 2). A patient who had a normal blood count last month has a quite different differential diagnosis from someone who has become gradually anaemic over a year. A blood film gives additional information and can be diagnostic of some conditions. Your haematology laboratory will have a protocol to make a blood film on sufficiently abnormal blood counts.
Time course of anaemia
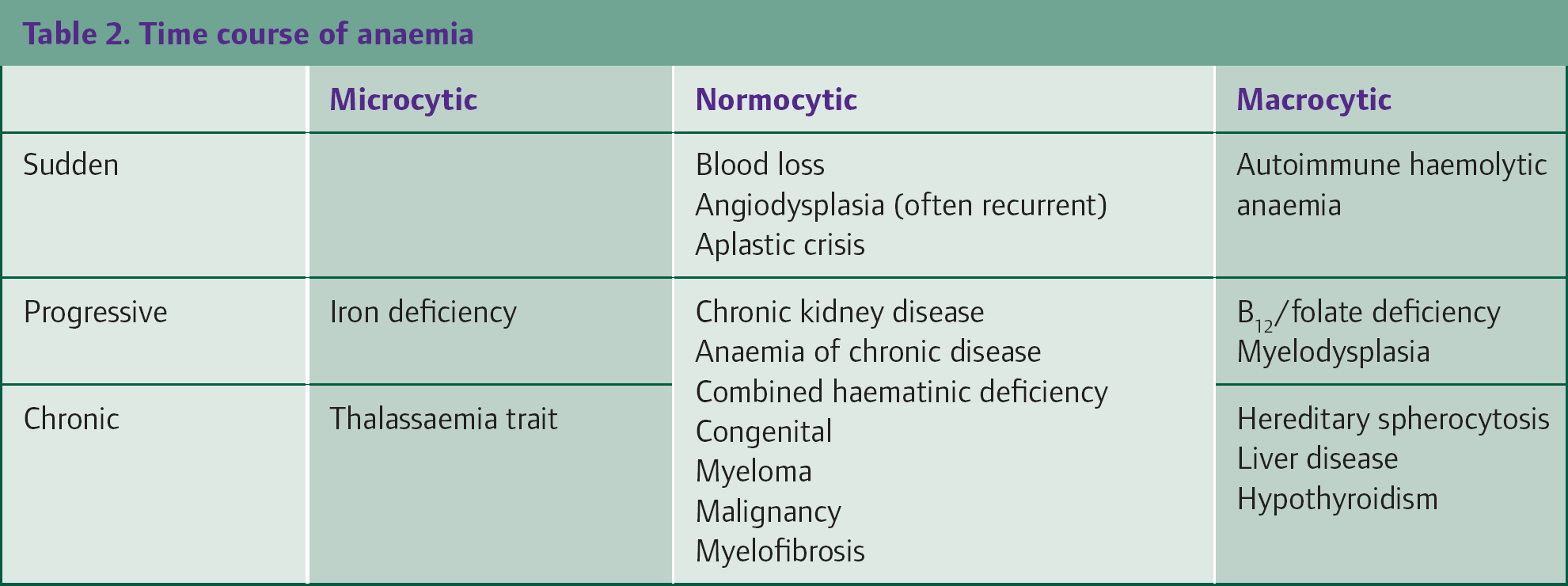
This article is intended as an outline guide only and is not exhaustive. Early forms of any cause of anaemia may start as normocytic. Microcytosis and macrocytosis do not cause any symptoms due to red cell size; their significance is in guiding further investigation.
Analysing a full blood count
A full blood count has a daunting array of figures and knowing how to understand these will assist an understanding of anaemia (Table 3). Be aware that ‘normal’ is defined as 95% of the test population. The precise normal levels will vary slightly between laboratories due to the different machines and calibration, but all reputable laboratories participate in National Quality Control Schemes and undergo inspection by Clinical Pathology Accreditation.
Red cell indices

The white cell count, white cell differential and the platelet count are significant if abnormal and increase the probability of an underlying bone marrow problem.
Blood film comments
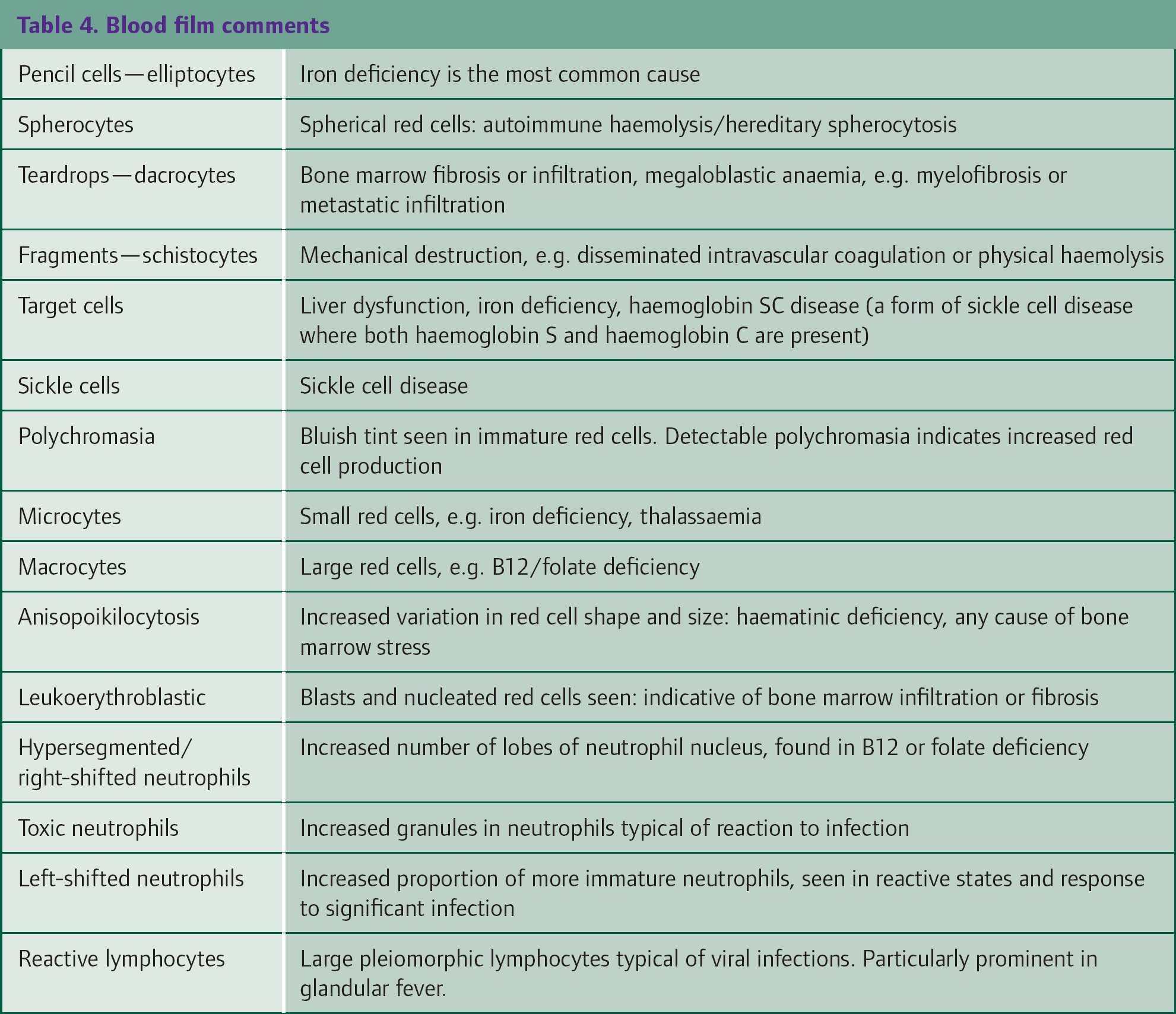
Comments on blood films use specific technical terms. Table 4 describes the commonly used terms and their significance.
Blood film comments
Microcytic anaemia
Iron deficiency
A low haemoglobin and microcytic or low MCV which have fallen in tandem from a previously normal level strongly suggests iron deficiency. The red cell distribution width (RDW) rises, and a blood film will show pale cells (hypochromia), elliptocytes (pencil cells) and target cells, with variability in red cell size and shape (anisopoikilocytosis). It affects as many as 2–5% of the Western population.
Iron deficiency starts with depletion of body stores, followed by functional iron deficiency in which there is inadequate iron for normal bone marrow and tissue function and sometimes mild anaemia. Further iron depletion causes frank iron deficiency anaemia. The causes of iron deficiency are summarized in Box 1.
Causes of iron deficiency
GI bleeding due to use of non-steroidal antiinflammatory drug (NSAID)/aspirin Colonic polyps/malignancy Gastric ulcers/polyps/malignancy Angiodysplasia Oesophageal malignancy Other GI tract bleeding Urinary tract bleeding Menorrhagia Coeliac disease Gastrectomy Severe epistaxis
Clinical assessment of the patient should include diet, weight loss, appetite, indigestion and bowel habit including steatorrhea, menorrhagia and abdominal symptoms. Poor dietary intake may be contributory if there is no red meat, poor vegetable intake or lots of junk food. Iron in haem molecules in meat is much better absorbed than the inorganic iron in vegetables, even spinach. Menstrual loss is the most common cause of iron deficiency anaemia in pre-menopausal women; in men and post-menopausal women, GI blood loss is the most frequent cause.
Clinical examination should include weight and nutritional status, abdominal examination for GI malignancy, uterine fibroids and renal masses and assessment of any lymphadenopathy including supraclavicular nodes. Koilonychia (spoon-shaped nails) is occasionally seen.
Investigation
Ferritin is the first-line test to confirm iron deficiency and a low level is diagnostic. However, a normal or high ferritin does not exclude iron deficiency. Ferritin is an acute phase protein synthesized by the liver, and its level rises in infection, inflammation and malignancy. It is good practice to check a C-reactive protein at the same time. If this is raised, the patient may still be iron deficient despite having a ferritin in the normal range.
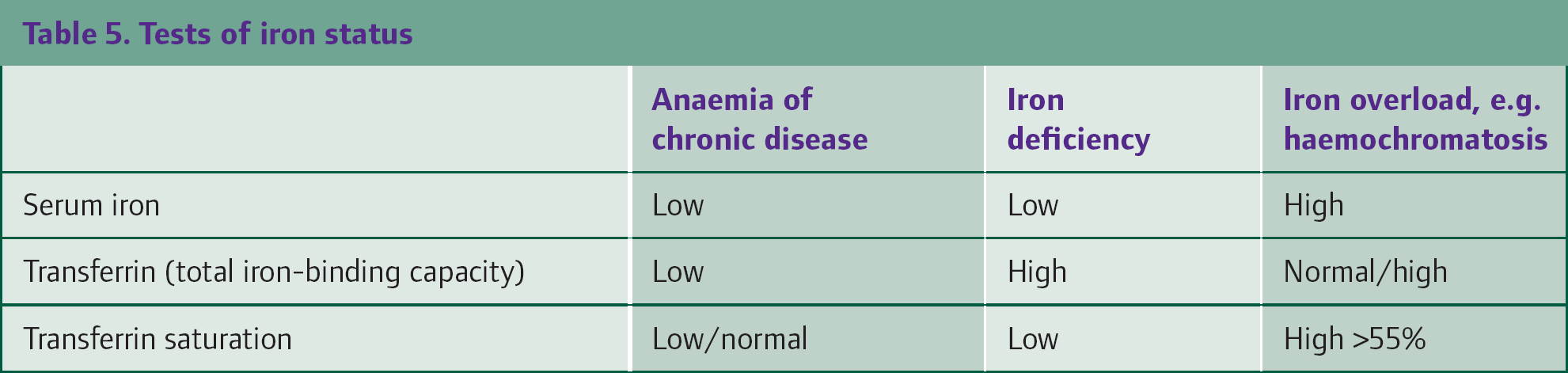
Where ferritin is not diagnostic, the next step is to test fasting serum iron and transferrin saturation. The patient must be fasting and avoid oral iron supplements or blood transfusion for several days before the test or the results can be erroneous. Interpretation of serum iron and transferrin values is summarized in Table 5. Transferrin may also be called total iron-binding capacity. Low transferrin saturation indicates low levels of iron available to the bone marrow.
Tests of iron status
There are other tests of iron status, not widely available, which may be performed by the local laboratory. The percentage of hypochromic red cells assesses the proportion of poorly haemoglobinized red cells, which rises in iron deficiency. Soluble transferrin receptors are increased in iron deficiency.
Investigation of GI causes
GI bleeding is the most common cause of iron deficiency. Small chronic blood loss may be symptomless: a few millilitres of blood loss a day is sufficient to cause iron deficiency. Any bowel lesion, polyp, ulcer or carcinoma may present with iron deficiency. Angiodysplasia (abnormal gut mucosal blood vessels) may also cause intermittent, but significant, GI bleeding.
Local referral pathways vary in referral criteria for endoscopy, gastroenterology clinics and provision of iron deficiency clinics. The British Society of Gastroenterology Guidelines on iron deficiency anaemia recommend that any level of iron deficiency anaemia should be investigated (Evidence Level B: good evidence from small or non-randomized clinical trials). National Institute of Clinical Excellence (NICE) recommends that urgent referral should be made for further investigation if haemoglobin is less than 11 g/dl in men or 10 g/dl in women (Box 2).
Investigations may not be appropriate in every patient due to severe co-morbidity or very advanced age. Computerized tomography pneumocolon is an alternative to colonoscopy for older frail patients, if locally available. Up to 10% of patients have more than more pathology, so the discovery of mild gastritis on oesophago-gastro-duodenoscopy (OGD) does not avoid the need for colonoscopy which might detect a more serious lesion such as caecal carcinoma as the cause.
Referral for GI investigation in patients with iron deficiency
The British Society of Gastroenterology Guideline (2005) recommends
Upper and lower GI investigations should be considered in all post-menopausal female and all male patients where iron deficiency has been confirmed, unless there is an overt, non-GI source of blood loss. All patients should be screened for coeliac disease. The NICE Guideline on referral for suspected cancer (2005) recommends Urgent referral to the specialist lower GI team if there is iron deficiency anaemia at any age with haemoglobin less than 11 g/dl (men) or less than 10 g/dl (women)
Coeliac disease
Coeliac disease is common and underdiagnosed, but may have a prevalence as high as one in 100 patients. Bowel symptoms may be minimal. Arthralgia and arthritis, depression and osteoporosis are also features. The diagnosis should always be considered in patients with recurrent iron deficiency, those patients unresponsive to iron and those patients with dual haematinic deficiency, such as iron and folate or B12 deficiency.
A convenient screening test is the blood test for antiendomysial, tissue transglutaminase or anti-gliadin antibodies, depending on the local laboratory repertoire. As with any autoantibody test, there can be a false-negative rate of 2–3%, so gastroenterology referral for OGD and duodenal biopsy is still required even with a negative antibody test if clinical suspicion is high. Ten per cent of first-degree relatives of patients with coeliac disease may have coeliac disease, but screening of asymptomatic relatives is not currently recommended unless symptomatic. The Primary Care Society for Gastroenterology has published guidance on coeliac disease in primary care.
Menorrhagia
Menstrual blood losses cause many women to have borderline iron balance. Hypothyroidism, fibroids and the perimenopause may increase menstrual blood losses. Very heavy menorrhagia, for example passage of many clots for several days, needing to use a towel and tampon together or flooding, may need further investigation. NICE published guidance on the investigation and management of heavy menstrual bleeding in 2007. Tranexamic acid for the first few days of the period may be helpful, as may consideration of long-acting progestogen contraception such as the intrauterine system. Patients who have had severe menorrhagia since menarche may have mild von Willebrand's disease. Consider discussing such patients with a haematologist.
Treatment of iron deficiency
For patients with confirmed iron deficiency, iron supplements should be given and a number of preparations are available. Ferrous sulphate 200 mg three times daily orally is a cheap and popular first-line choice. Patients should be warned about its common side effects which are indigestion, constipation, diarrhoea and black stools. The adverse effects are due to the redox effects of the ferrous (Fe2+) iron being oxidized to ferric (Fe3+) iron. Side effects can be minimized by starting on 200 mg once daily, then increasing the dose after a few days as tolerated. Other iron preparations, such as ferrous fumarate or ferrous gluconate can be tried in turn. Syntron liquid is useful for those patients who dislike tablets. Orange juice and ascorbic acid assist iron absorption. Oral iron should be continued for at least 3 months after normalization of haemoglobin values to replenish body stores.
A minority of patients, particularly those with Crohn's disease or previous bowel surgery, are intolerant of all oral iron. Intravenous iron supplements should then be considered. Iron sucrose (Venofer) is administered up to three times a week as a short infusion until the required dose is reached. Iron dextran (Cosmofer) can be administered similarly or alternatively as a single total dose infusion over several hours, completely replenishing the patient's iron stores at one visit. All intravenous iron has a risk of anaphylaxis, although this is less common with modern preparations. Intravenous iron should only be administered by trained staff where resuscitation facilities are available. A consultant haematologist can usually advise on local provision and availability.
Treatment with iron is highly preferable to blood transfusion except in frank bleeding or haemodynamic compromise. Patients with chronic iron deficiency anaemia with a haemoglobin as low as 5 or 6 g/dl have become anaemic over many months and may be remarkably well compensated. Oral iron, normally absorbed, can increase haemoglobin by a gram a week and avoid the need for blood transfusion.
Thalassaemia trait and haemoglobinopathies
Lifelong low or very low MCV and mean cell haemoglobin (MCH), with a normal or near normal haemoglobin, strongly suggests a thalassaemia trait. The red cell count is often raised. Thalassaemia trait is the condition of having both normal and thalassaemia globin genes. Haemoglobin is comprised of two alpha globin and two beta globin proteins. The thalassaemic disorders are inherited disorders of reduced globin production, causing microcytosis and variable degrees of anaemia. Globally, they are among the most common inherited disorders and originated in areas where malaria was endemic but are now more widely dispersed due to migration and can be found occasionally even in ethnically British people due to mutation or long-forgotten foreign ancestors.
Alpha thalassaemia is the deletional loss of one to three of the four alpha globin genes. Loss of one or two alpha genes causes microcytosis; loss of three causes haemoglobin H disease, with a haemoglobin of 7–10 g/dl, mild splenomegaly, but compatible with normal life and activities. Beta thalassaemia is due to point mutations in one or both beta globin genes causing reduced protein synthesis or a truncated globin protein. This leads to much more phenotypic variability, between mild microcytosis in thalassaemia minor, occasional transfusions in thalassaemia intermedia and lifelong transfusion dependence in thalassaemia major.
The discrepancy between haemoglobin and low MCV is called disproportionate microcytosis, e.g. haemoglobin 12 g/dl, MCV 72 fl. In iron deficiency, the haemoglobin might be 8 g/dl with an MCV of 72 fl. If a patient with thalassaemia trait develops iron deficiency, both the haemoglobin and MCV will fall further. It can be particularly difficult to distinguish iron deficiency and thalassaemia trait or their combination in antenatal full blood counts, especially if there are few previous blood counts for comparison. Request advice from your haematologist. Conversely, it is important to avoid repeated courses of iron for a low MCV which is not due to iron deficiency.
Sickle cell disease is characterized by a moderate anaemia and painful crises. Sickle cell disease is one of the most common genetic disorders. Sickle cell trait, the heterozygous state, has minimal clinical significance except the risk of an affected pregnancy if the partner also has a haemoglobinopathy. It predominantly affects Afro-Caribbean people, but is also found across the Middle East and India. Antenatal or neonatal diagnosis allows children to be offered penicillin prophylaxis, pneumococcal immunization and transcranial doppler screening for stroke risk.
Testing for thalassaemia or haemoglobinopathy
Thalassaemia and haemoglobinopathy testing is performed on a normal full blood count specimen. Provide as much additional information as possible about ethnic background and family history to assist interpretation. Most haematology laboratories can test for common haemoglobinopathies and for beta thalassaemia trait. Confirmation of alpha thalassaemia trait requires more detailed genetic analysis by a specialist reference laboratory.
If a patient has a thalassaemia trait and is pregnant or considering pregnancy, there are implications for partner testing, particularly if the partner is of the same high-risk ethnic group. NICE Guidance on antenatal care recommends that all pregnant women should now be counselled and offered screening for haemoglobinopathy and thalassaemia. In areas of high sickle cell prevalence, all mothers should be offered laboratory testing; in low prevalence areas, mothers should be offered screening by a Family Origin Questionnaire, with further testing only if the mother is identified as at high risk or if the MCH is less than 27 pg. If the mother is identified as a carrier, the partner should be offered counselling and appropriate testing as soon as possible.
Macrocytic anaemia
Abnormal liver function, excess alcohol and hypothyroidism can all cause macrocytosis without anaemia. Some drugs, such as azathioprine, zidovudine, methotrexate and hydroxycarbamide, cause significant macrocytosis due to interference with DNA synthesis. When assessing patients with macrocytic anaemia
Ask about diet, alcohol consumption, personal or family history of jaundice Clinical examination should look for peripheral sensory neuropathy, signs of alcohol excess and chronic liver disease, jaundice and splenomegaly First-line tests for investigation of a macrocytic anaemia are B12, folate, thyroid function, liver function tests, gamma glutamyl transferase (gamma GT) and reticulocytes
A haematology laboratory will have a protocol to do a blood film on a significantly macrocytic result, but it is certainly reasonable to request a blood film when the MCV is greater than 105 fl.
Results from first line tests should guide you in further investigation, treatment and referral. B12 and folate deficiency treatment is discussed below. A raised reticulocyte count suggests haemolysis. A blood film may indicate features of myelodysplasia.
B12 deficiency
The lower level of a normal B12 is not well defined and varies between laboratories depending on the test method used. Levels are lower in pregnancy and severe folate deficiency. As a guide, where the lower limit of normal is 180 ng/l, levels down to 160 ng/l are indeterminate and of doubtful clinical significance unless there is macrocytosis or peripheral neuropathy. Lower levels of B12 should generally be treated. The dosage regimen for hydroxycobalamin is given in the British National Formulary. A total of 1 mg is administered intramuscularly, three times a week for 2 weeks, then every 3 months. A small minority of patients feel tired and symptomatic before the 3 monthly treatment is due and it is reasonable to administer B12 more frequently to these patients. Once a patient is on B12 injections, there is no need to recheck serum B12 again; levels are always very high. The majority of B12 circulates in an inactive form bound to transcobalamin-1; only the small proportion bound to transcobalamin-2 is bioavailable.
B12 neuropathy is a glove-and-stocking loss of fine touch sometimes described as walking on cotton wool. Neuropathy due to a very low B12 less than 50 ng/l can occasionally occur even with a normal blood count. B12 deficiency is also implicated in ataxia, depression and dementia.
Further investigations
Causes of B12 deficiency include pernicious anaemia, vegan diet, gastric surgery, malabsorption and Crohn's terminal ileitis. Gastric parietal cell antibodies are sensitive but non-specific and frequently found in older patients. However, a negative result has a good negative predictive value to exclude pernicious anaemia. Intrinsic factor antibodies are more specific. Consult with your local laboratory to see which tests they do. Historically, the Schilling test was used to further investigate B12 absorption, but the test reagent has been discontinued by the manufacturer, so the Schilling test will no longer be available.
Folate deficiency
The principal causes of folate deficiency are a poor diet lacking in fruit and vegetables or malabsorption. B12 is required for folate metabolism so a significantly low B12 can cause a mildly low folate. Where both B12 and folate are low, B12 should be administered first, as there is a theoretical risk of precipitating subacute combined degeneration of the cord if folate is given to a B12-deficient patient.
When a folate test is requested, most laboratories now test red cell folate. This is a much more accurate measure of folate status than serum folate, which varies widely with diet over the last few days.
Folate deficiency is treated with a daily dose of folic acid 5 mg orally and dietary advice if relevant. Consider investigating for coeliac disease or other causes of malabsorption particularly in patients without obvious dietary lack.
Haemolytic anaemia
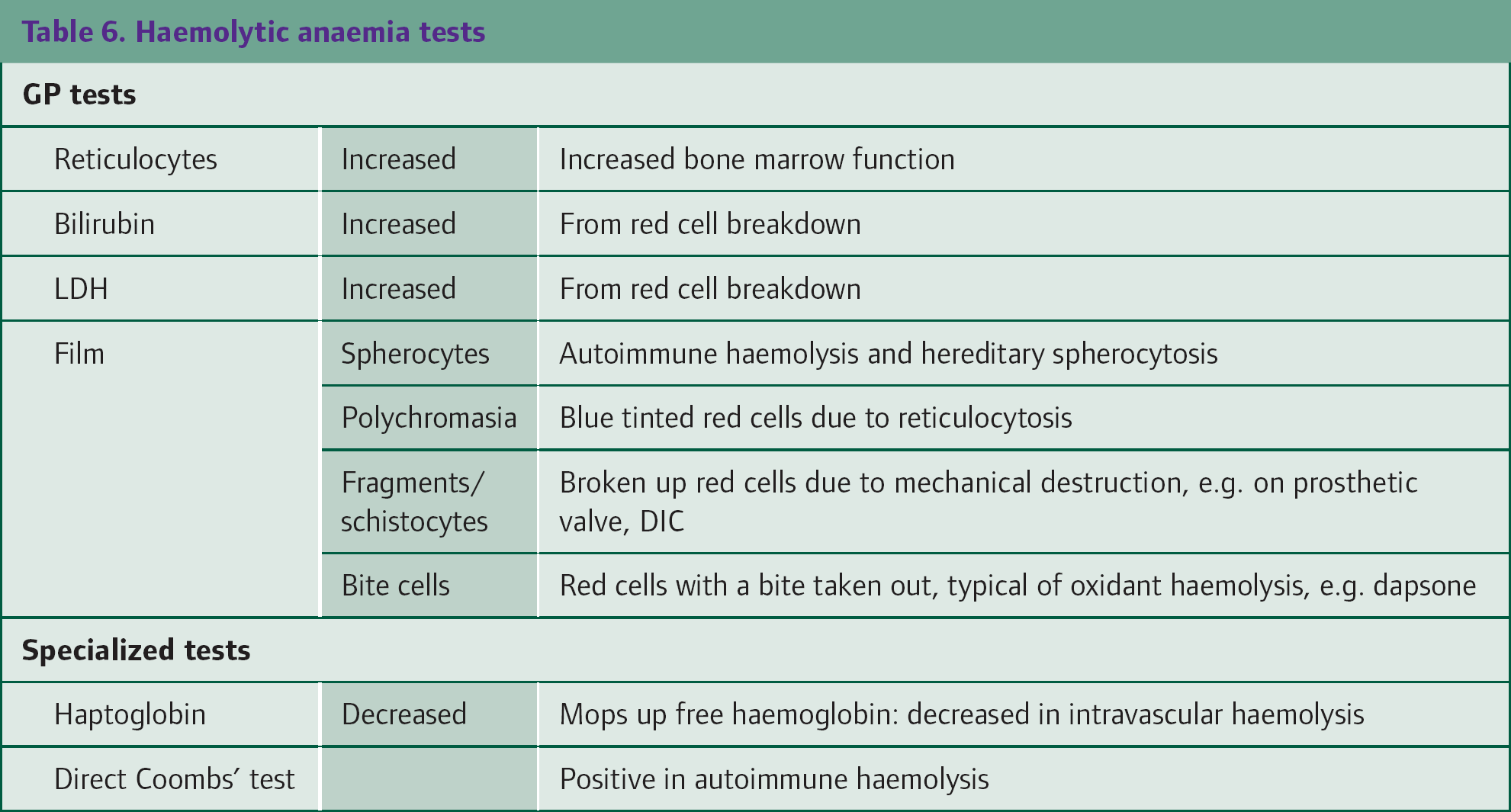
Elevated bilirubin and reticulocytosis suggest haemolytic anaemia. Haemolytic anaemia is defined as any cause of shortened red cell lifespan due to red cell breakdown. The most common causes are hereditary spherocytosis (HS) and autoimmune haemolytic anaemia (AIHA). Haemoglobinopathies also have a shortened red cell lifespan. The normal red cell lifespan is about 120 days (Table 6). sum marizes the tests used to diagnose haemolytic anaemia.
Haemolytic anaemia tests
Patients with haemolytic anaemia are at risk of aplastic crisis due to acute parvovirus B19 infection. This virus, the cause of slapped cheek syndrome or fifth disease, infects bone marrow red cell precursors. This is of no clinical consequence in normal individuals but causes a dramatic but transient severe anaemia in patients with haemolytic anaemia, particularly children.
Hereditary spherocytosis
HS is an autosomal dominant red cell disorder, with an incidence of 1 in 2000 in Caucasians. Normal red cells are biconcave discs, but in HS, the red cells are spherical due to inherited abnormalities in the proteins of the red cell cytoskeleton. The phenotype is variable. Some children present with anaemia and jaundice, others only have occasional jaundice or anaemia if unwell and some cases are only detected late in life or due to the diagnosis in other family members.
The full blood count shows variable anaemia, sometimes macrocytosis due to reticulocytosis and increased MCH concentration. A blood film usually shows some spherocytes. The Direct Coombs’ test is negative.
Patients with moderate or severe HS should have folate supplements to support the increased bone marrow red cell production. Severe cases need splenectomy, but it is advisable to avoid this before the age of 5 years due to the increased risk of infection.
Autoimmune haemolytic anaemia
This is an autoimmune disorder due to production of antibodies against a red cell antigen. A typical case presents with sudden onset jaundice and anaemia over a few days or weeks. It is often spontaneous, but sometimes associated with drugs, lymphoproliferative disorders, connective tissue disorders and atypical pneumonias such as mycoplasma. The most common kind is an IgG-associated haemolytic anaemia called a warm AIHA because the IgG antibody binds to red cells at 37°C. This is treated initially with high-dose prednisolone.
Cold haemolytic anaemia or cold haemagglutinin disease has an IgM antibody which binds red cells at temperatures below 20°C and can cause chronic haemolysis and jaundice to be worse in the winter months. It may be idiopathic or due to an underlying lymphoproliferative disorder or a sequelae of atypical pneumonia such as mycoplasma. Only a minority of patients with cold agglutinins noticed incidentally on a blood film have appreciable haemolysis.
Refer anyone with new onset jaundice and anaemia to Haematology. Refer urgently if the haemoglobin is less than 10 g/dl.
Mechanical haemolytic anaemia
Prosthetic or native heart valves with turbulent flow can cause red cell haemolysis through mechanical destruction. This may be suspected through the blood count showing increased RDW and the blood film showing fragmented red cells called schistocytes. This phenomenon may also cause iron deficiency due to urinary loss of the iron from the haemolysed cells. Disseminated intravascular coagulation also causes a mechanical haemolytic anaemia though thrombocytopenia and deranged clotting are usually more prominent features.
Myelodysplasia
Myelodysplasia should be suspected in patients with macrocytic anaemia or neutropenia or thrombocytopenia or any combination of these. Review of previous results may show a progressive change over months or years. Sometimes there has been a macrocytosis for many years but neutropenia or anaemia has now developed.
The blood film may be diagnostic if it shows abnormal neutrophils or misshapen red cells but in mild macrocytic anaemia there may be no diagnostic features on the film. Features of myelodysplasia on a blood film include anisopoikilocytosis (variation in size and shape), hypogranular neutrophils (lack the usual quantity of granules), pseudoPelger or bilobed neutrophils (neutrophils with only two nuclear lobes like pince-nez spectacles, instead of the usual 3, 4 or 5 nuclear lobes).
Myelodysplasia is an acquired clonal bone marrow disorder. The incidence rises sharply with age, reaching over 1 per 3000 per year in those over 70 years. Not all cases need referral. Mild macrocytosis or anaemia may simply be monitored. The laboratory haematologist may comment on the blood film about necessity for referral. Cases with neutropenia with neutrophils less than 1 × 109/l or pancytopenia should generally be referred.
Normocytic anaemia
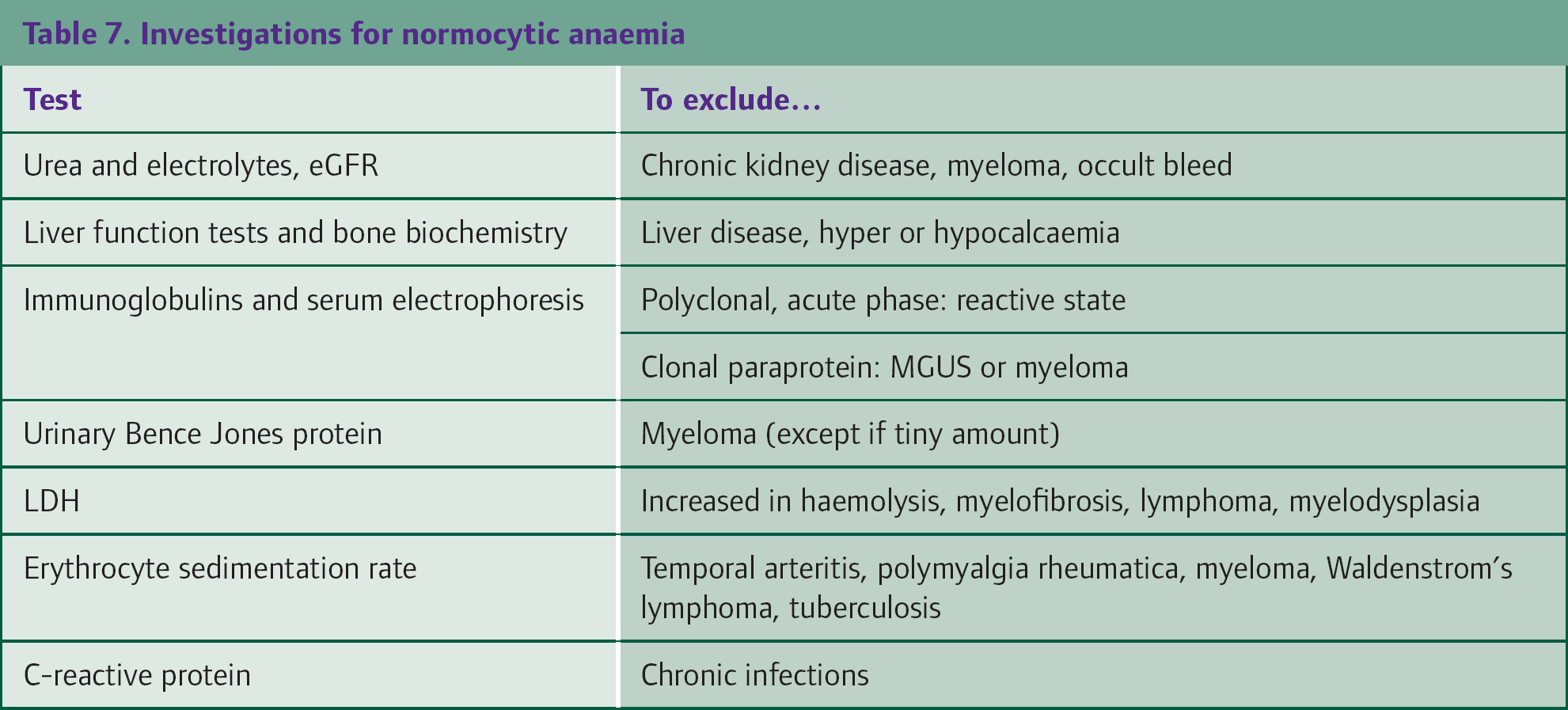
In patients with normocytic anaemia, clinical assessment is essential to guide further investigation. Table 7 lists investigations that should be considered. The early phase of any cause of anaemia may be normocytic, but a significant change in the MCV can suggest developing iron or B12 deficiency even while the MCV is still in the normal range. Underlying conditions include the acute blood loss, anaemia of chronic disease, renal disease and malignancy.
Investigations for normocytic anaemia
Clinical assessment
Ask about NSAIDs, fatigue, weight loss, night sweats, bony pain, bowel habit, melaena and prostatic symptoms. Examine for bruising, pallor, lymphadenopathy clubbing, breast lumps, abdominal masses, ulcers and abscesses.
Investigations
For all patients with normocytic anaemia, consider an abdominal ultrasound scan to look for splenomegaly, renal lesions, liver abnormalities, unsuspected malignancy and metastases. Consider a chest X-ray to look for malignancy and other pulmonary lesions.
Sudden blood loss
An acute GI bleed may present with anaemia. Older patients may not give a clear history of blood loss. One clue can be increased urea relative to creatinine over the next few days or a rise in MCV due to reticulocytosis. Angiodysplasia can cause significant anaemia recurring every few months.
Renal disease
Erythropoietin, synthesized by the kidney, is essential for red cell production and maturation. Levels fall in renal disease causing anaemia. The widespread introduction of estimated Glomerular Filtration Rate (eGFR) calculation has highlighted the hidden numbers of patients with significant chronic kidney disease. NICE guidance (CG39, September 2006) on the management of people with anaemia of renal disease states that treatment for anaemia due to chronic kidney disease, with an eGFR of less than 60 ml/minute (Stage 3 CKD or greater) should be considered when the haemoglobin is less than 11 g/dl and when other causes have been excluded. Local protocols may vary and you should seek advice from your local renal department.
Anaemia of chronic disease
The mechanisms of the anaemia of chronic disease, also called anaemia of inflammation, are becoming better understood. Pro-inflammatory cytokines such as tumour necrosis factor are increased. Increased levels of hepcidin, a regulator of iron transport, result in reduced availability of iron for haematopoiesis. There is decreased erythropoietin production and decreased response of red cell precursors in the bone marrow to erythropoietin.
Anaemia of chronic disease should be considered as a cause in patients with diabetes, heart failure, mild renal impairment, leg ulcers, inflammatory arthritis, polymyalgia rheumatica, etc. In practice, since the anaemia of chronic disease cannot be tested for directly, but is a diagnosis of exclusion, some patients are referred to a haematologist for further assessment, particularly if the haemoglobin is less than 10 g/dl and there is no overt cause.
Leukoerythroblastic anaemia
Leukoerythroblastic anaemia refers to the film appearances of immature myeloid cells and blasts, with nucleated red cells. It is generally a sign of a fibrotic or infiltrated bone marrow, for example myelofibrosis or metastatic malignancy. Occasionally, it is seen in marrow stress such as after cardiac arrest. In a patient with known metastatic disease or otherwise advanced cancer, it heralds bone marrow infiltration but does not need further investigation.
As a new finding, urgent investigation is necessary. Clinical assessment may detect breast lumps, abdominal masses, hepatomegaly or splenomegaly. Investigations may include tumour markers, Prostate Specific Antigen (PSA) and Lactate Dehydrogenase (LDH). Refer any suspected primary cancer to the appropriate specialist team. Refer urgently to a haematologist if there is splenomegaly or if there are no other diagnostic features. A bone marrow biopsy is likely to be necessary.
Myelofibrosis
Myelofibrosis is suggested by a leukoerythroblastic film in a patient with splenomegaly. Teardrop red cells are typically usually found on the blood film. Firm splenomegaly is usual and may be any size from just palpable or massive. Myelofibrosis is one of the few causes of massive splenomegaly filling the abdomen to the right iliac fossa. Large spleens may develop painful infarcts, typically a pleuritic type pain over the spleen.
Myelofibrosis is a clonal bone marrow disorder where the normal bone marrow is replaced by fibrosis. The median prognosis is about 3–5 years. Patients become transfusion dependent.
Malignancy: myeloma, lymphoma and renal carcinoma
Any advanced malignancy may cause anaemia, through the anaemia of chronic disease or by metastatic bone marrow infiltration. Anaemia may also be a presenting feature of malignancy. Renal carcinoma presents with anaemia and systemic symptoms in up to 25% of patients. Lymphoma should be suspected when there is chronic lymphadenopathy for more than 6 weeks or lymphocytosis. Myeloma should be considered if there is anaemia with bone pain, particularly vertebral pain or collapse, or new or worsening renal impairment.
First-line tests for myeloma are immunoglobulins and serum electrophoresis, urinary Bence Jones protein, bone biochemistry and renal function. Request radiographs of areas of bony pain. It is important to remember that
Most patients with a paraprotein do not have myeloma. Monoclonal gammopathy of unknown significance (MGUS) is present in 3% of 70-year-olds and becomes even more frequent with advancing age. The average risk of progression to myeloma is only 1% per year. An acute phase or polyclonal response indicates a reactive state, not myeloma IgM is associated with lymphoma, not myeloma Anaemia with a high erythrocyte sedimentation rate may also be due to polymyalgia rheumatica or reactive causes
About 30% of myeloma cases do not have a paraprotein but instead show hypogammaglobulinaemia (low serum immunoglobulins) and have detectable urinary light chains (Bence Jones protein). It is mandatory to check urine as well as serum in suspected myeloma. About 1% myeloma patients lack urine or serum paraprotein and tend to present late with bone marrow failure or bony disease. Serum-free light chains, the serum equivalent of Bence Jones protein, are increasingly used to monitor myeloma.
Referral
Refer urgently for suspected myeloma if a patient has anaemia, bone pain, renal impairment, or paraprotein greater than 30 g/dl. Asymptomatic patients with incidental paraproteins less than 15 g/dl, with normal full blood counts and stable renal function, are likely to have MGUS and may be referred routinely or monitored.
Pregnancy
The mild anaemia of later pregnancy is principally dilutional. The red cell mass increases by up to 32%, but the plasma volume expands even more by 40% at term. It is usual for the MCV to rise slightly in pregnancy. A tandem fall in haemoglobin and MCV suggests developing iron deficiency. NICE Clinical Guideline 62 (2008) on antenatal care recommends checking the full blood count at booking and again at 28 weeks. Haemoglobin below 11 g/dl at booking or 10.5 g/dl at 28 weeks should prompt investigation and treatment of anaemia. Iron deficiency constitutes 75% of cases of anaemia. Pregnant women should not be treated with iron routinely, only if iron deficient.
Summary of investigations
Figure 1 summarizes the investigation of anaemia in primary care

Assessment and investigation of anaemia in primary care.
Key points
Understand full blood count indices and common blood film comments Assess the time course and MCV of the anaemia Investigation of the cause of iron deficiency is mandatory: consider GI bleeding, menorrhagia, other bleeding and coeliac disease Offer thalassaemia and haemoglobinopathy screening to antenatal patients Investigation of macrocytic anaemia: B12, folate, thyroid function, liver function tests, gamma CT and reticulocytes. Ask about alcohol consumption The anaemic of chronic disease is due to increased hepcidin reducing iron utilization and to reduced response to erythropoietin.