
Abstract
Bleeding in pregnancy up to 14 weeks of gestation is common, affecting as many as one in four pregnancies. GPs are expected to distinguish between those women who can be managed at home and those requiring admission.
The GP curriculum and bleeding in early pregnancy
Women-specific health matters account for over 25% of GP time. It is important that GPs in training know how to manage such conditions. GP Curriculum Statement 10.1: Women's health requires GPs in training to be able to
Demonstrate knowledge of women's health problems, conditions and diseases Demonstrate a reasoned approach to the diagnosis of women's symptoms in a manner that is comfortable for the patient and the GP using history, examination, incremental investigations and refer appropriately Perform a gentle and thorough pelvic examination, including digital and speculum examination, assessment of the size, position and mobility of the uterus, and the recognition of abnormality of the pelvic organs, paying attention to professional etiquette, patient consent, comfort and information Arrange appropriate investigations Provide primary care management of the common gynaecological problems Have knowledge of specialist treatments and surgical procedures including laparoscopy and medical and surgical management of termination of pregnancy Provide emergency care for bleeding in early pregnancy and suspected ectopic pregnancy Describe and implement the key national guidelines that influence health care provision for women's problems
Causes of bleeding in early pregnancy
The causes of bleeding in early pregnancy are
Bleeding in normal pregnancy — the largest group Miscarriage Ectopic pregnancy Trophoblastic disease and Non-obstetric causes, such as a friable cervix, a polyp or cervical cancer
Brief initial assessment
Box 1 summarizes the points to cover in the initial assessment of a woman presenting with bleeding in early pregnancy. Start by taking a history of the woman's symptoms. In particular, ask about her bleeding and whether there has been any pain.
If there has been vaginal bleeding, then ask about the nature of the bleeding and whether any clots or products of conception have been passed (these can be difficult to distinguish). Ask about time of onset of pain in relation to bleeding. If pain precedes bleeding, ectopic pregnancy is more likely, but consider any sexually active woman presenting with abdominal pain and vaginal bleeding after an interval of amenorrhoea to have an ectopic pregnancy until proved otherwise.
Summary of the initial assessment of a patient presenting with bleeding in early pregnancy in the community
Period of amenorrhoea Pregnancy test results Amount of bleeding Degree of pain Time of onset of pain in relation to bleeding Passage of products of conception Past medical/obstetric history of note
Temperature and cardiovascular status of the patient Abdominal findings State of the cervix Whether any products of conception are visible in the cervical os or vagina Uterine size should be equivalent to the expected size for the period of amenorrhoea
Ask the date of the woman's last menstrual period and about any pregnancy test results. Do a pregnancy test if one has not been done. Ask about previous pregnancies and their outcomes. Ask about risk factors for ectopic pregnancy and particularly pelvic inflammatory disease, previous ectopic pregnancy, tubal surgery, infertility or the presence of a copper-containing intrauterine device.
Check the woman's pulse, blood pressure and temperature. A pulse of over 100 beats per minute suggests shock. A fever may indicate uterine sepsis.
Examine her abdomen. Guarding, peritonism and/or unilateral tenderness suggest ectopic pregnancy. With the advent of Early Pregnancy Units (EPUs), the necessity of pelvic examination in primary care is debatable. Only perform a pelvic examination if it is likely to alter your management. If performed, assess the uterine size and the cervix, determining whether the cervix is open (a closed cervix admits only one fingertip in a multiparous woman) and checking to exclude non-obstetric causes of bleeding. If any products of conception are removed on examination, they should be sent for histology.
Initial management
If the woman has severe bleeding and/or pain or if she is shocked or toxic, admit to the nearest specialist unit or Accident and Emergency department as an emergency by ambulance. In most areas, admission is under the care of the gynaecologists. If the patient is shocked, if available and not contraindicated, give 1-ml Syntometrine by intramuscular injection and try to gain intravenous access.
In all other cases, refer as an outpatient to the EPU to check site and viability of the pregnancy (RCOG, 2008). EPUs offer same or next day appointments which can be booked over the telephone. The contact details for every EPU in the UK are listed on website: www.earlypregnancy.org.uk/FindUs1.asp.
Ultrasound scan (USS) is the definitive test of viability of pregnancy. Advise women that there is a strong possibility of a transvaginal USS, although in practice this is usually well tolerated. At 5-week gestation, a gestation sac and sometimes also a yolk sac are seen on scan; at 6 weeks, a foetal pole and foetal heart beat are usually visible (the foetal heart beat is occasionally not seen until 7 weeks). Blood group and rhesus status is also checked at the EPU.
Confusing ultrasound results
In up to 1 in 10 assessments, women will not be given a definitive diagnosis at the first visit to the EPU. This can be confusing for them and they may ask your advice. The most common reasons for this are
Pregnancy of unknown location—this means that there are no signs of either intra- or extrauterine pregnancy or retained products of conception in a woman with a positive pregnancy test. This may be because the pregnancy test has not yet returned to normal after a complete miscarriage or because the pregnancy is ectopic. Women are followed up by the EPU until the pregnancy test has reverted to negative or intrauterine or ectopic pregnancy is confirmed.
Pregnancy of uncertain viability—this means that there is an intrauterine sac of less than 20 mm mean diameter with no obvious yolk sac or foetus or a foetal crownrump length of less than 6 mm with no obvious foetal heart activity. In order to confirm or refute viability, a repeat scan at a minimal interval of 1 week is needed.
Bleeding in early normal pregnancy
Bleeding in early normal pregnancy is often termed ‘threatened miscarriage’. If the foetal heart is seen on USS, then there is a 97% chance of the pregnancy continuing to progress. There is no evidence that rest, or abstinence from sex, improves outcome.
Rarely bleeding in early pregnancy results in subchorionic haematoma. Significant subchorionic haematoma is associated with increased risk of premature rupture of membranes and intrauterine growth restriction. If this is detected on USS, refer for specialist antenatal care.
Miscarriage
Miscarriage is defined as a pregnancy loss occurring before 24 completed weeks of gestation. The miscarriage rate is difficult to assess, as miscarriages may go unreported in the community. However, miscarriage is estimated to occur in around one in five pregnancies. More than 80% of miscarriages occur early, before 12 weeks gestational age. Miscarriage rates are around 3% once foetal heart activity has been detected.
Risk factors and causes for miscarriage
Maternal risk factors for miscarriage include
Maternal age — the older the mother, the greater the risk of miscarriage Raised body mass index (over 29 kg/m2) —if body mass index is greater than 32 kg/m2, risk is increased by 30% Infertility treatment—25–30% of women who miscarry recurrently have a history of infertility treatment Smoking — advise all women not to smoke during pregnancy. For smokers, provide assistance to stop smoking as needed and preferably prior to conception. Excess alcohol intake — advise all women not to drink any alcohol during pregnancy. Provide problem drinkers with support to cut down their alcohol consumption.
Causes of spontaneous miscarriage are summarized in Box 2 and may relate to the foetus, the placenta or the mother. Often no cause for miscarriage is identified.
Causes of spontaneous miscarriage
Foetal abnormality (thought to account for about 50% of miscarriages) Multiple pregnancy Abnormalities of implantation or placental vasculature Uterine abnormality—fibroids, polyps, congenital abnormality, intrauterine adhesions Cervical incompetence — causes late second or early third trimester pregnancy loss Systemic disease—renal, autoimmune or connective tissue disease — particularly systemic lupus erythematosus, polycystic ovarian syndrome, diabetes mellitus or systemic infection Drugs—cytotoxics, stilboestrol
Complete miscarriage
Type of miscarriage is classified by history of bleeding and whether or not there are products of conception remaining in the uterus (Fig. 1). Miscarriages are termed ‘complete’ if there is a history of bleeding in pregnancy but there are no products of conception remaining in the uterus on assessment. Provide women who have suffered a complete miscarriage with psychological support.
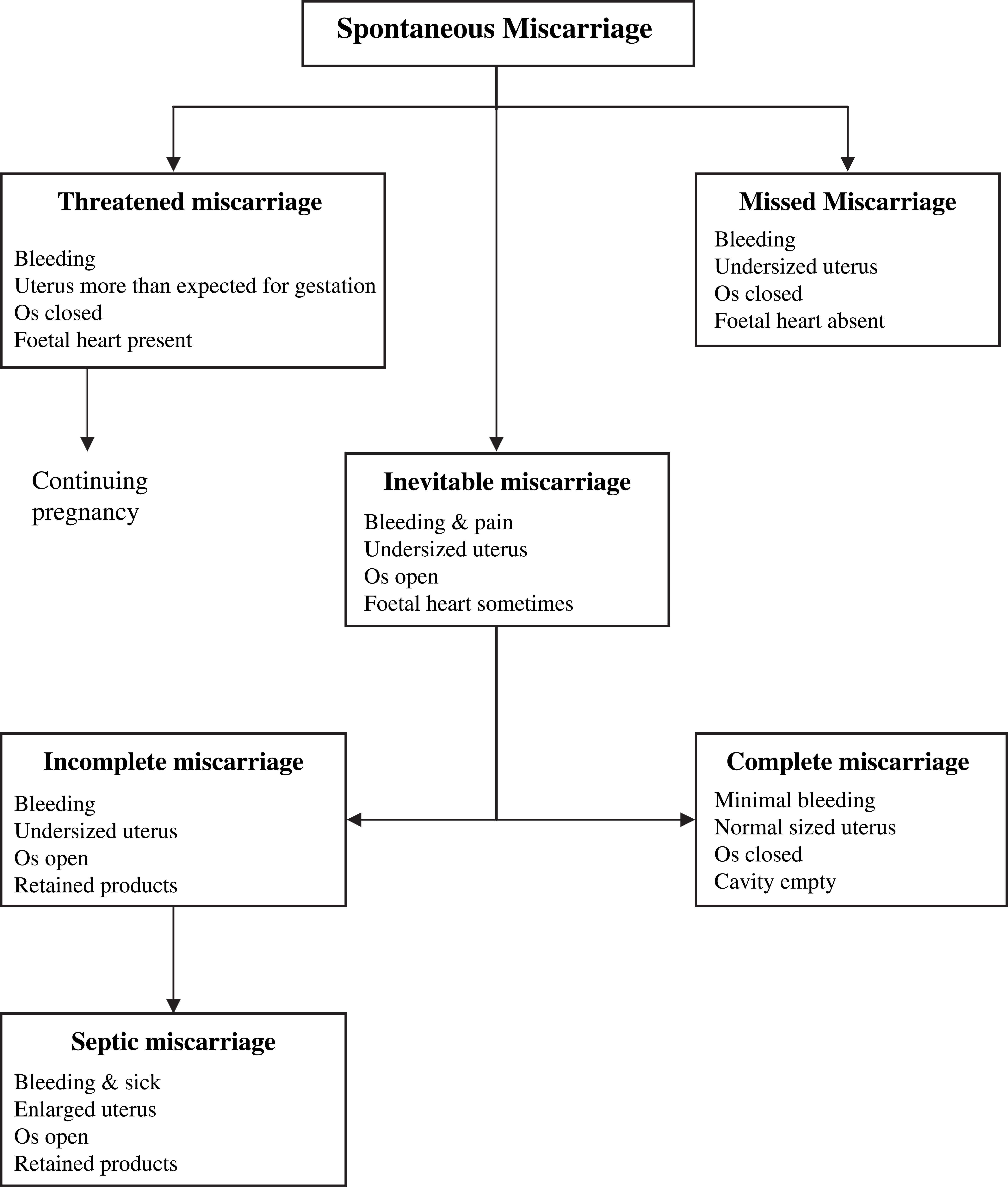
Classification of miscarriage.
Incomplete miscarriage
When a patient presents with bleeding and products of conception remain in the uterus, but no foetal heart is found, the miscarriage is termed ‘incomplete’. Specialist management options include surgical evacuation of retained products of conception (ERPC), medical treatment or a ‘watch-and-wait’ approach.
If surgical evacuation is to be used, suction curettage is the method of choice. Surgical evacuation is always an option, but necessary if there is excessive or persistent bleeding, haemodynamic instability, evidence of infected retained products or suspected gestational trophoblastic disease.
GPs should be aware of the complications of ERPC as these may present in the community after discharge. Early complications include uterine perforation, cervical tears, intra-abdominal trauma, haemorrhage or infection.
If the patient develops an offensive discharge or low-grade fever, suspect infection and treat with antibiotics (e.g. doxycycline 100 mg daily or co-amoxiclav 250/125 mg three times daily). Depending upon the clinical urgency, readmit or refer back for specialist reassessment if the patient
has a high fever (may suggest ‘septic miscarriage’) becomes shocked has worsening or severe pain has heavy bleeding or the bleeding is not settling within 10 days.
Delayed complications include infertility, Asherman's syndrome (intrauterine synechiae) and cervical incompetence.
Medical methods of treatment are an effective alternative to surgical intervention in the management of miscarriage and may be undertaken on an outpatient basis if adequate specialist back up is available. Various medical methods have been described using prostaglandin analogues (gemeprost or misoprostol) with or without antiprogesterone priming (mifepristone). Warn women that bleeding may continue for up to 3 weeks after treatment.
In incomplete miscarriage, a further option is ‘expectant management’ or a watch-and-wait approach. This is probably as effective as medical management for women with incomplete miscarriage and has less pain and bleeding associated with it. After 3 days, 86% of women presenting with an incomplete miscarriage will no longer have any products of conception remaining.
Missed or delayed miscarriage
A ‘missed’ or ‘delayed’ miscarriage occurs when there is no bleeding, but the foetal heart is absent on USS, and the pregnancy is non-viable as a result. Treatment options are the same as for incomplete miscarriage, but expectant management is less successful. Even after 4 weeks watching and waiting, only 66% of women who have suffered a delayed miscarriage will no longer have any products of conception remaining. In contrast, 80% success rates have been demonstrated within 3 days using medical treatment with vaginal misoprostol.
Recurrent miscarriage
Miscarriage is described as ‘recurrent’ if it occurs more than three times consecutively. Ensure that these are confirmed pregnancies, and not simply late, heavy periods. Recurrent miscarriages affect 1–2% of couples. Risk of further miscarriage is associated with both maternal age and the number of previous miscarriages that the woman has suffered (Table 1): the more miscarriages and the older the woman, the lower the chance of successful pregnancy.
Probability of successful pregnancy after miscarriage

In all cases, where a woman has suffered more than three consecutive miscarriages, refer for specialist assessment. No cause is found in more than half of those couples referred. In those cases, chance of a successful pregnancy in the future is around 70%. A chromosomal abnormality in one parent is the cause in 3–5% of those referred. Other common reasons for recurrent miscarriage include cervical incompetence and antiphospholipid antibodies (15% of those referred).
The diagnosis of cervical incompetence is usually made on the basis of history of suggestive symptoms in past pregnancies: one or more late second or early third trimester usually presenting with painless leaking of liquid or gradual painless dilatation of the cervix. Treatment is with cervical cerclage early in pregnancy. A stitch is placed high up around the cervix to keep it closed (e.g. a Shirodkar suture). The stitch is removed at around 37 weeks and labour ensues rapidly if the diagnosis was correct.
Antiphospholipid syndrome is an autoimmune disorder which may occur alone or in combination with other autoimmune disorders such as systemic lupus erythematosus. It results in increased tendency to thrombosis and pregnancy complications such as miscarriage and pre-eclampsia. Treatment with low-dose aspirin and low molecular weight heparin from 6- to 34-week gestation improves outcome.
Ectopic pregnancy
Ectopic pregnancy occurs when a fertilized egg implants outside the uterine cavity. In 95% of cases, implantation occurs within a Fallopian tube. The incidence of ectopic pregnancy is around one in every 100 pregnancies, and incidence is increasing. Risk factors for ectopic pregnancy are listed in Box 3.
Presentation
Ninety-seven per cent of women with an ectopic pregnancy present with abdominal pain. This may be unilateral or bilateral, often starts before any bleeding and may radiate to shoulder the tip. It may become worse when the woman passes urine or opens her bowels. Most women (79%) with an ectopic pregnancy also present with irregular vaginal bleeding. This is often described as looking like ‘prune juice’ but may be fresh, red blood. It is usually not heavy. Sometimes the woman may pass a decidual cast, which can be mistaken for products of conception. The peak incidence of ectopic pregnancy occurs after 7-week amenorrhoea, but in 25% of those presenting with ectopic pregnancy, there is no history of amenorrhoea.
On examination, the woman may be haemodynamically shocked (15–20%). Most women have abdominal tenderness and 71% have some rebound or guarding on examination of the abdomen. If pelvic examination is undertaken, this may reveal an enlarged or normal sized uterus, adnexal mass and/or cervical excitation.
Management
A suspected ectopic pregnancy is a surgical emergency as untreated; a ruptured ectopic may cause internal haemorrhage and death. Admit immediately for further investigation, resuscitating before admission as needed. Hospital management may be
Expectant—watch and the pregnancy resolves spontaneously Medical—with methotrexate or Surgical—with laparotomy or laparoscopic surgery.
Offer early USS in future pregnancies to confirm that the pregnancy is intrauterine. Pregnancy rate after an ectopic pregnancy is 66% with 10% having a further ectopic pregnancy.
Trophoblastic disease
Hydatidiform mole
A hydatidiform mole is a benign tumour of trophoblast containing 46 chromosomes all of paternal origin and no foetal material. It has an incidence in the UK of 1 in 2000 pregnancies and is more common in teenagers and women over the age of 40. Moles may become invasive and penetrate the uterus and/or metastasize to the lungs. One in 30 women with a hydatidiform mole go on to develop choriocarcinoma.
Risk factors for ectopic pregnancy
Pelvic inflammatory disease (a single episode increases risk by a factor of 7) Infertility (15%) Intrauterine copper-containing contraceptive device (14%) Previous ectopic pregnancy (11%) Tubal surgery Progesterone-only pill Age Smoking
Hydatidiform mole presents with bleeding in early pregnancy, often accompanied by exaggerated symptoms of pregnancy such as hyperemesis. There may be passage per vaginum of grape-like vesicles. Rarely, hydatidiform moles present with symptoms of metastatic spread, such as haemoptysis or pleurisy. The uterus is usually large for dates, and no foetal heart can be heard. USS has a typical appearance and serum β -human chorionic gonadotrophin (β -HCG) is very raised.
If suspected, refer urgently for specialist assessment. If a hydatidiform mole is confirmed, the woman will be followed up by a specialist centre. Treatment is with evacuation of the pregnancy, often combined with chemotherapy. Incidence in further pregnancies is roughly 1 in 120. Pregnancy is not advised for at least a year after a molar pregnancy, and any future pregnancies must be investigated early with ultrasound and β-HCG estimation. It is important to note that the combined oral contraceptive pill is contraindicated in women who have had a molar pregnancy.
Partial mole
A partial mole is a benign tumour of trophoblast containing 69 chromosomes, one maternal and two paternal sets, with some foetal tissue. Primary care management is identical to management of a hydatidiform mole but there is no increased risk of choriocarcinoma in these patients.
Choriocarcinoma
Choriocarcinoma is a rare, malignant tumour of trophoblast which follows molar (rarely normal) pregnancy — often many years after. It presents with vaginal bleeding and/or metastases (shadows on chest X-ray, dyspnoea and/or haemoptysis). It is treated with chemotherapy and prognosis is excellent. Pregnancy is possible after 2 years free from disease.
Rhesus-negative women
Fifteen per cent of women are rhesus negative (RhD — ve). Development of anti-D antibodies results from foetomaternal haemorrhage in RhD — ve women carrying a rhesus-positive foetus. In later pregnancies, these antibodies cross the placenta causing rhesus haemolytic disease of the foetus which gets successively worse with each pregnancy.
Immunoprophylaxis for RhD — ve mothers using anti-D immunoglobulin (anti-D Ig), to prevent them developing antibodies, is given intramuscularly into the deltoid muscle as soon as possible after any potential sensitizing event, preferably within 72 hours but there is evidence of benefit up to 9 days. Women already sensitized should not be given anti-D Ig. Box 4 summarizes the circumstances when anti-D Ig should be given when there has been bleeding in early pregnancy.
Giving anti-D Ig after bleeding in early pregnancy
If bleeding occurs before 12 weeks gestation, anti-D is not required for
Threatened miscarriage unless heavy or repeated bleeding and/or abdominal pain or Complete miscarriage where there is no medical or surgical uterine evacuation
Whether or not the pregnancy is lost, give anti-D to all non-sensitized RhD — ve women who have
Any bleeding after 12-week gestation Ectopic pregnancy Surgical or medical evacuation of the uterus at any gestation
If gestation is less than 20 weeks, the dose of anti-D Ig is 250 IU intramuscularly, preferably within 72 hours of the event.
If there is any clinical doubt, give anti-D Ig.
Psychological support after early pregnancy loss
Broach the subject of pregnancy loss with all women who have suffered a miscarriage or other early loss of pregnancy. Include the woman's partner if possible. Not all women are grieved, so adjust your approach accordingly.
Legitimize any grief and acknowledge it. Provide information about the condition which caused the loss and reassure the couple where appropriate about the future. For example, if a woman has had less than three consecutive miscarriages, risk of further miscarriage is not significantly increased, and risk of further ectopic pregnancy is approximately 1 in 10.
Discuss any worries and concerns of the woman and her partner. Warn them of the anniversary phenomenon —sadness at the baby's due date or anniversary of the pregnancy loss — or feelings of sadness or jealousy on the birth of another's baby. Inform them about self-help organizations, such as the Miscarriage Association and Ectopic Pregnancy Trust (Box 5) and provide ongoing support as needed. If the woman already has young children, inform the health visitor. Bear in mind that different women will want to discuss their feelings at different times after loss.
Sources of support for couples after early pregnancy loss
Further training
The Royal College of Obstetricians and Gynaecologists conducts the Diploma examination (DRCOG) which is aimed at doctors, and especially GPs, who wish to certify their knowledge and interest in Women's Health. The DRCOG curriculum includes Early Pregnancy care in Module 6.
Key points
Bleeding in early pregnancy is common Causes of bleeding in early pregnancy include bleeding in normal pregnancy, miscarriage, ectopic pregnancy and molar pregnancy Women with fever, heavy bleeding, severe or unilateral pain or signs of shock should be referred as emergencies for specialist management Other women can be managed as outpatients through referral to the EPU Miscarriage can be managed expectantly, medically or surgically depending on woman's choice and clinical condition Women with three or more miscarriages should be referred to a recurrent miscarriage clinic for detailed investigations