
Abstract
Dyspnoea is the subjective sensation of breathlessness that is excessive for any given level of physical activity. Acute breathlessness is defined as severe dyspnoea evolving rapidly over minutes to hours. The sudden development of dyspnoea heralds, in most cases, a significant cardiopulmonary insult. The aim of this article is to give GPs in training a strategy to deal with acute breathlessness in primary care
The GP curriculum and acute breathlessness
The initial call for help
Most calls for assistance for acutely breathless patients will be made by telephone. It is important to ascertain as quickly as possible:
How breathless the patient is, and how that is affecting the patient When the breathlessness started Other associated symptoms such as sweating, nausea, chest pain and palpitations Past medical history, particularly of allergy or anaphylaxis, lung disease such as asthma or COPD and heart disease
In all cases, depending on the level of acute breathlessness, general state of the patient and social support available, either arrange to see the patient in the surgery or visit the patient. If there is likely to be a delay before assessment is possible and the patient is very breathless, has other sinister symptoms such as chest pain or is very distressed, call for emergency ambulance assistance immediately without seeing the patient.
On arrival
Whenever you are assessing a breathless patient, it is important to be calm and reassuring. Breathlessness is very frightening and panic only adds to the sensation of being breathless.
Direct the history and examination to finding the cause as quickly as possible (Box 1). Treat the patient according to the cause. Box 2 lists the differential diagnosis of acute breathlessness in adults. If no cause can be found and the patient is acutely and significantly breathless, do not delay and admit to hospital as an acute medical emergency.
Clinical assessment of an acutely breathless adult
What are the symptoms? Ask about breathlessness, cough, wheeze, sputum and other accompanying symptoms such as chest pain, fever, palpitations and sweating. When did the symptoms begin? How have the symptoms evolved? For example, did anything trigger the attack? Is the breathlessness getting worse? Has the patient had anything like this before? Does the patient have any past medical history of note? For example, asthma, COPD, anaphylaxis, cardiac disease, thromboembolism or diabetes Is the patient taking any medication? Does the patient have any allergies?
How breathless does the patient appear? Is the patient conscious? Is the patient distressed? Is the patient breathless at rest? Can the patient speak in full sentences?
Check:
Temperature—does the patient have fever? Colour—is there any central cyanosis? Respiratory rate and use of accessory muscles Blood pressure Pulse—rate and rhythm Jugular venous pressure Position of the trachea — central or deviated to one side? Chest — expansion (symmetrical or asymmetrical and overexpansion), percussion (dullness or hyperresonance), breath sounds (bronchial breathing and reduced breath sounds) and added sounds (pleural rub, wheeze and crepitations) Swelling of the legs and sacral oedema Peak flow rate if asthma is suspected Oxygen saturation with a pulse oximeter (if available)
Differential diagnosis of acute dyspnoea
Acute exacerbation of COPD Acute exacerbation of asthma Pneumonia Pneumothorax Pulmonary embolism (PE) Pleural effusion Large airway obstruction, for example choking, anaphylaxis, severe tonsillitis and epiglottitis
Acute left ventricular failure Arrhythmia Acute myocardial infarction Pericarditis
Pain Shock, for example hypovolaemic shock secondary to bleeding or septicaemic shock secondary to meningitis Metabolic acidosis, for example diabetic ketoacidosis Drugs, for example aspirin overdose Hyperventilation or panic attack Superior vena cava obstruction
Common causes of acute breathlessness
Case history 1
Anna is a 23-year-old student. She has a history of mild asthma, usually controlled with just a salbutamol inhaler used as required. She developed an upper respiratory tract infection 2 days ago and has become increasingly wheezy ever since. She presents as an emergency in the surgery one evening and the receptionist asks you to see her straight away as she seems very breathless.
Acute asthma
Acute asthma presents with breathlessness and wheeze, usually in association with a past history of asthma, although asthma can present de novo. Regard each emergency asthma consultation as acute severe asthma until proved otherwise. Patients with severe or life-threatening attacks may not be distressed and may not have all the characteristic abnormalities of severe asthma. The presence of any should alert the doctor. An attack is severe if any of the following signs are present:
Peak flow rate of 33–50% of previous best or predicted value Respiratory rate of 25 breaths/minute or more Heart rate of 110 beats/minute or more Inability to complete sentences in a single breath
Life-threatening features include
Peak flow rate under a third of the predicted value or the patient's previous best Oxygen saturation of less than 92% or cyanosis Silent chest on auscultation Bradycardia, dysrhythmia and/or hypotension Poor respiratory effort Exhaustion, confusion or coma
Manage the patient in accordance with the current British Thoracic Society and Scottish Intercollegiate Guidelines Network (SIGN) guidance (Fig. 1). Admit to hospital if there are any life-threatening features, if there are any features of acute severe asthma remaining after initial treatment or if the patient has a past history of near-fatal asthma. Lower your threshold for admission if the attack is in the afternoon or evening, the patient has had a recent hospital admission with asthma or reports previous severe attacks of asthma. Concern about the patient's ability to assess their own asthma or social circumstances of the patient (e.g. if the patient lives alone) should also lower your threshold for admission.

Management of acute severe asthma in adults in general practice.
After treatment for a severe asthma attack in the surgery or admission for an asthma attack, it is important to review the patient within 2 days. Address any potentially preventable contributors to the severe asthma attack. Monitor symptoms and peak flow. Check inhaler technique. Provide a written asthma plan for the patient to follow should their symptoms deteriorate again and modify ongoing treatment according to the current guidelines for management of chronic asthma.
Case study 2
Jean, one of your receptionists, is known to have a severe allergy to peanuts. One morning she is sitting having coffee with some of the other practice staff. It is the practice nurse's birthday and she has brought some cakes in. Suddenly, Jean becomes very breathless and her lips start to swell. She feels light headed. She asks you to get her Epipen out of her handbag and rapidly injects herself with adrenaline.
Anaphylaxis
Patients presenting with anaphylaxis often have a past history of anaphylaxis or a severe allergic reaction. Anaphylaxis is likely if there is sudden onset or rapid progression of symptoms over minutes which include life-threatening problems:
These usually occur together with skin or mucosal changes (flushing, erythema, urticaria, angioedema, rhinitis and/or conjunctivitis). Other possible symptoms include abdominal symptoms (such as abdominal pain, vomiting or incontinence) and anxiety, often with a sense of impending doom.
If anaphylaxis is suspected, follow the algorithm in Fig. 2. Patients who have had a suspected anaphylactic reaction [i.e. an airway, breathing or circulation (ABC) problem] should be treated and then observed for at least 6 hours in a clinical area with facilities for treating life-threatening ABC problems, even if they are well. In practice, this means admission to hospital or observation in Accident and Emergency (A&E). This is because up to 20% of patients who have an anaphylactic reaction have a biphasic reaction with further symptoms appearing 4–10 hours after the initial reaction.
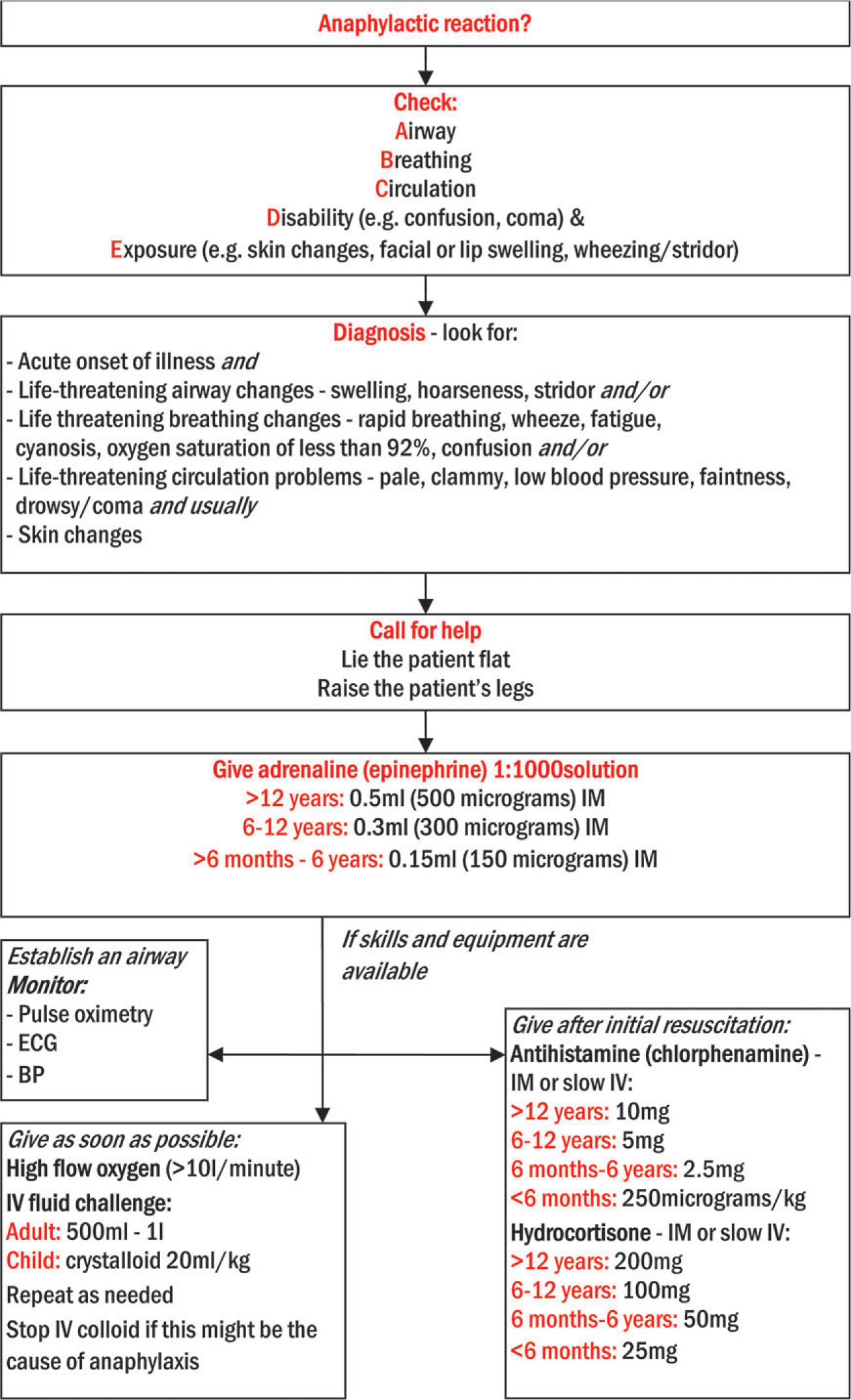
Emergency treatment of anaphylaxis.
All patients presenting with anaphylaxis for the first time should be referred to an allergy clinic to identify the cause (thereby reducing the risk of future reactions) and prepare the patient to manage future episodes themselves. There is a list of specialist clinics on the British Society for Allergy and Clinical Immunology website (www.bsaci.org).
Case study 3
Mr Harvey is a 79-year-old man with a long history of hypertension. He has been a bit breathless for a while, but has put it down to his age. He wakes up at 3 a.m. one morning fighting for his breath and calls the out-of-hours service for assistance. You are sent to visit him.
Acute left ventricular failure
Acute left ventricular failure presents as acute severe breathlessness secondary to pulmonary oedema and tends to occur at night. Some relief may be gained from sitting or standing. Other symptoms include fatigue and cough, sometimes accompanied by haemoptysis (usually pink and frothy). On examination, the patient is breathless, tachycardic (often a gallop rhythm is present) and has coarse, wet-sounding crackles at both lung bases. Blood pressure is normal or reduced. There may be ankle or sacral oedema if right heart failure is also present.
In all cases, urgent action is needed to save life. Sit the patient up and give 100% oxygen if available and there is no history of COPD (when give 24% oxygen). Call for ambulance assistance if symptoms are severe. Give
Intravenous furosemide 40–80 mg slowly (or bumetanide 1–2 mg) Intravenous morphine or diamorphine 2.5–5 mg over 5 minutes Intravenous metoclopramide 10 mg (can be mixed with diamorphine) Glyceryl trinitrate spray two puffs sublingually
The decision whether to admit the patient to hospital depends on the severity and cause of the attack, response to treatment and social support available. Always admit if the patient is alone at home or has inadequate social support, the suspected cause of left ventricular failure warrants admission (e.g. acute myocardial infarction), the patient remains very breathless and there is no improvement with treatment at home over half an hour or the patient is hypotensive or has an arrhythmia.
Case history 4
Mrs Raven is a 63-year-old smoker. She was diagnosed with COPD about 10 years ago but, despite repeated attempts to stop, continues to smoke. She calls the surgery one morning because she has become increasingly short of breath over the past 4 days. You arrange to visit her.
Acute exacerbation of COPD
Acute exacerbation or worsening of previously stable COPD can be associated with increased breathlessness, increased sputum volume and sputum purulence. Initial management should include increased frequency of bronchodilator, by a nebulizer if necessary. Add oral antibiotics if there is purulent sputum and prednisolone (30 mg daily) for 7 to 14 days if there is a significant increase in breathlessness.
Features that should prompt consideration of hospital admission are listed in Table 1. If managed at home, monitor with pulse oximetry if available, establish optimum therapy and arrange appropriate reviews. Hospital-at-home provision may be appropriate for some patients who would otherwise be admitted to hospital.
Deciding whether to treat acute exacerbations at home or admit for treatment in hospital
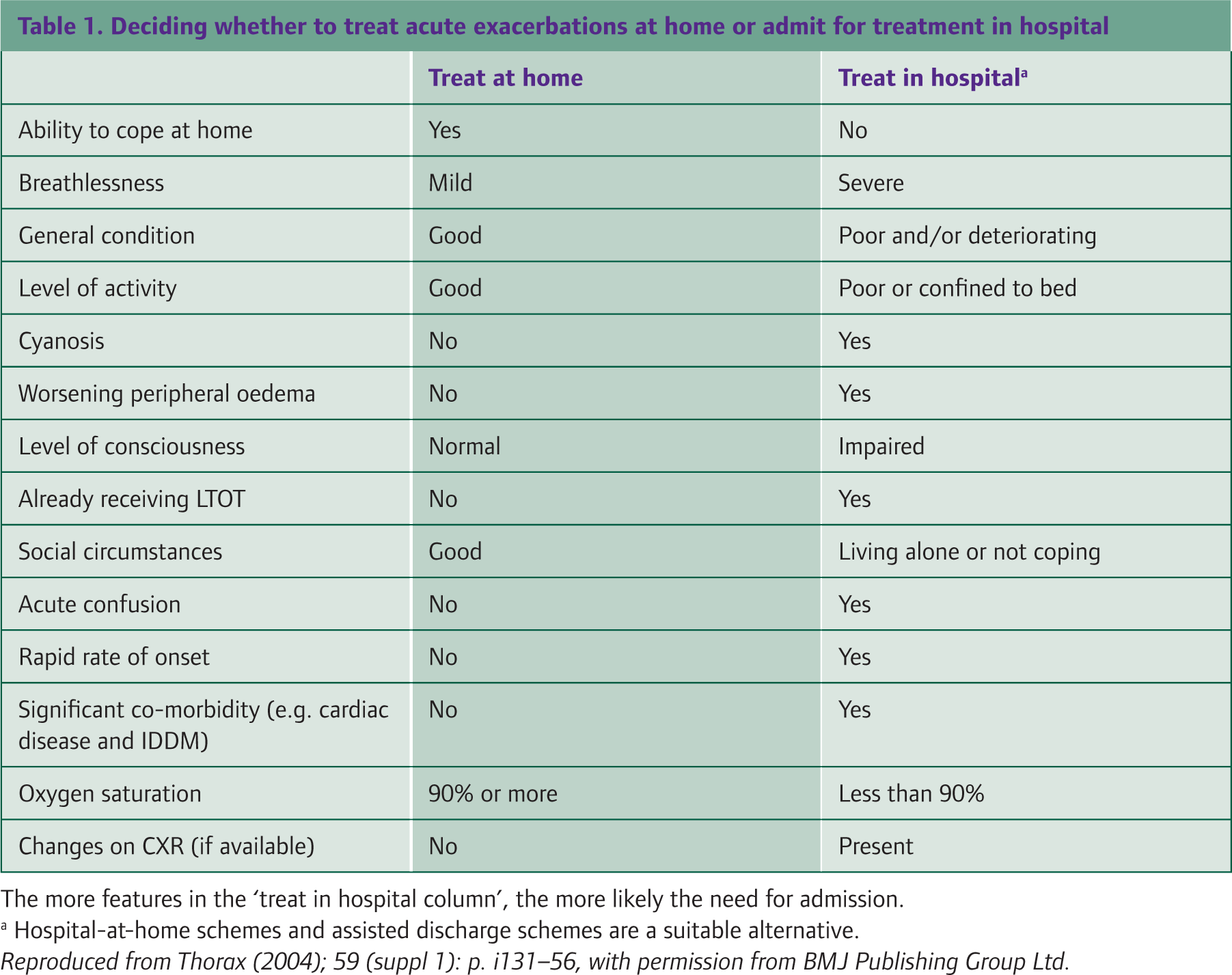
The more features in the ‘treat in hospital column’, the more likely the need for admission.
Hospital-at-home schemes and assisted discharge schemes are a suitable alternative.
Case history 5
Sarah is a 46-year-old mother of two teenagers. You rarely see her in the surgery. She comes in to see you and seems breathless on walking down the corridor. She ways that she feels awful. She has had a high fever for 3 days accompanied by rigours. She has gone off her food completely and has a nasty cough productive of thick green sputum. She has tried treating herself with paracetamol and fluids but her symptoms are getting worse and she has now developed a sharp pain at the back of her chest on the left when she takes a deep breath. On examination, she is pyrexial and has coarse crepitations heard over the base of her left lung.
Pneumonia
Pneumonia is a common condition with annual incidence of eight cases per 1000 adult population. Incidence increases with age and peaks in the winter. Mortality for those managed in the community is less than 1%, but one in four patients with pneumonia are admitted to hospital, and mortality for those admitted is about 9%.
The acute illness is characterized by symptoms of an acute lower respiratory tract infection — cough and at least one other lower respiratory tract symptom, such as purulent sputum or pleurisy. On examination, there are new focal chest signs, for example consolidation or reduced air entry, coarse crackles and/or a pleural rub. Respiratory tract symptoms and signs are accompanied by systemic features such as fever, rigours or aches and pains. It is important to note that pneumonia may present atypically in the elderly, for example with acute confusion or ‘off legs’.
In all cases, consider the need for admission. The CRB-65 score (Fig. 3) may help. Have a low threshold for admission if the patient is ill but apyrexial, if the patient has concomitant illness (such as congestive cardiac failure, chronic lung disease, renal or liver disease, diabetes or cancer) or if the patient lives alone or has inadequate social support. Consider administering antibiotics prior to admission if the patient is very unwell or there will be a delay of more than 2 hours before admission.

Assessment of severity and management of acute pneumonia: the CRB-65 score.
If a decision is made to treat the patient at home, advise the patient not to smoke, to rest and to drink plenty of fluids. Start a broad-spectrum antibiotic such as amoxicillin 500 mg three times daily (erythromycin 500 mg four times daily or clarithromycin 500 mg twice daily is alternative for patients who are penicillin allergic). Treat pleuritic pain with simple analgesia such as paracetamol or ibuprofen. Review within 48 hours to reassess the patient's clinical state. If the patient is deteriorating or not improving despite treatment, consider requesting a chest X-ray and/or reassess the need for admission.
Case history 6
Martine is a 19-year-old student who returned yesterday from Australia where she has spent her gap year. She has no past medical history of note but has been seen in the past in the surgery for prescription of the combined oral contraceptive pill. She developed sudden onset sharp chest pain this morning and is slightly breathless at rest. She has booked a telephone appointment in your morning surgery to ask you for advice.
Pulmonary embolism
PE can be fatal and causes about 20 000 deaths per year in the UK. It occurs when venous thrombi — usually from a deep vein thrombosis (DVT) in the leg — pass into the pulmonary circulation and block blood flow to the lungs. Without treatment, 20% with proximal DVT develop PE. Risk factors for thromboembolism are listed in Box 3.
Have a high level of suspicion. Patients may have minimal symptoms and signs apart from some pleuritic chest pain and dyspnoea. Other symptoms and signs to look for include haemoptysis, tachycardia, hypotension, pleural rub and raised jugular venous pressure. Look for a source of emboli, although often DVT is not clinically obvious.
If PE is suspected, give oxygen as soon as possible and admit as an acute medical emergency. In all cases of proven PE, anticoagulation is started in hospital or by a hospital-at-home service before discharge to general practice. Warfarin should be continued for 6 months. Aim to keep the international normalized ratio at around 2.5 (range 2–3).
Risk factors for venous thromboembolism
mmobility—long flight or bus journey, post-op and plaster cast Smoking Combined oral contraceptive pill Pregnancy or puerperium Malignancy Past history or family history of DVT, PE or clotting tendency
Case history 7
Selma is a 53-year-old lady whom you recently referred to the breast surgeons because she had found a breast lump. She calls you the day after she has seen the surgeon to update you. In passing, she mentions to you that she has been feeling rather breathless all day. You tell her to come down to the surgery and listen to her chest. She has reduced air entry on the right hand side of her chest, the side that the breast lump is on. You send her to the hospital for a chest X-ray and find a pneumothorax.
Pneumothorax
Pneumothorax simply means free air in the chest cavity. This may occur spontaneously or as a result of trauma. Clinically, the patient presents with sudden onset of breathlessness, often accompanied by pleuritic chest pain. Signs may be absent if the pneumothorax is small. Look for tachycardia, resonant percussion note and decreased or absent breath sounds.
Risk factors for spontaneous pneumothorax include previous pneumothorax, smoking or rapid changes of air pressure (e.g. ascent in an aeroplane or diving). In patients under the age of 40, spontaneous pneumothorax is usually due to rupture of a pleural bleb. The patient is typically tall, thin and male. In patients over 40, 70–80% presenting with spontaneous pneumothorax have a history of COPD. Spontaneous pneumothorax may also occasionally be associated with asthma, pneumonia, tuberculosis, lung cancer or pulmonary fibrosis.
If pneumothorax is suspected, refer for a chest X-ray (Fig. 4). If the diagnosis is confirmed, seek specialist advice about further management. Small pneumothoraces usually resolve spontaneously (a 50% collapse takes about 40 days to resorb). Monitor the patient until chest X-ray shows that the pneumothorax has completely resolved. Larger pneumothoraces may require admission for aspiration or a chest drain. Smoking cessation reduces risk of recurrence.
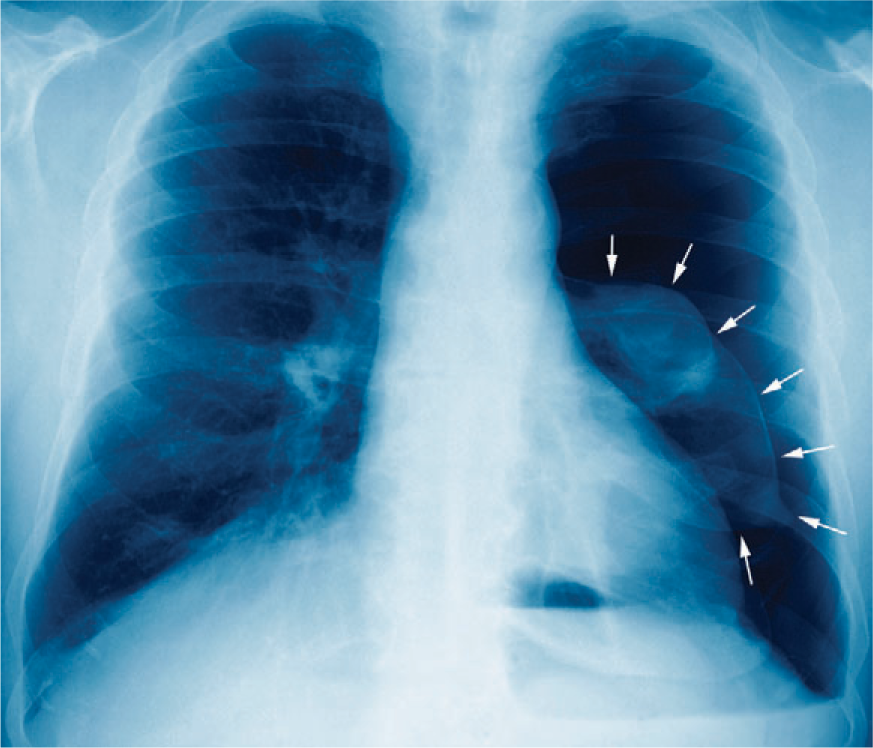
Chest X-ray showing a pneumothorax.
Presentation and management of traumatic pneumothorax are the same as for spontaneous pneumothorax. Trauma may not initially be obvious — ask about recent procedures in the vicinity of the chest wall, for example acupuncture to the neck and shoulders as well as chest and fine-needle aspiration of a breast lump.
Tension pneumothorax is a complication of traumatic pneumothorax. It is very rare after spontaneous pneumothorax. A valvular mechanism develops. Air is sucked into the pleural space during inspiration but cannot be expelled during expiration. The pressure within the pleural space increases, the lung deflates further, the mediastinum shifts to the opposite side of the chest and venous return reduces. Tension pneumothorax can be rapidly fatal.
Clinically, patients with tension pneumothorax tend to have a history of chest trauma and are agitated and distressed. On examination, there is tachycardia, signs of a large pneumothorax (decreased breath sounds and decreased chest movement on the affected side) and mediastinal shift, with the trachea deviated away from the side of the pneumothorax.
If tension pneumothorax is suspected, sit the patient upright if possible and insert a large bore cannula through the second intercostal space of the chest wall in the midclavicular line on the side of the pneumothorax to relieve the pressure in the pleural space. Transfer the patient to hospital as an emergency.
Case history 8
Adam is a 21-year-old man who has recently been having some problems at work and has just split up with his girlfriend. You are doing a shift at the local GP-run minor injuries unit and Adam walks in with his mother. Both of them are very agitated. Adam is breathing very rapidly and keeps repeating that he thinks that he is going to die.
Acute hyperventilation
The features of hyperventilation and acute panic attacks are fear, terror and a feeling of impending doom accompanied by some or all of the following:
Shortness of breath and/or a choking sensation Chest pain or discomfort Palpitations Sweating Dizziness Paraesthesiae or more rarely carpopedal spasm
On examination, the patient is distressed, may be tachycardic, and is occasionally hypertensive, but the chest is clear and there are no other abnormal findings.
Two techniques are useful for the management of patients who are hyperventilating. Try talking the patient down. Explain the nature of the symptoms to the patient. Racing of the heart is due to adrenaline produced by the panic. Paraesthesiae and feelings of dizziness are secondary to overbreathing due to panic. Count the breaths in and out, gently slowing the breathing rate.
Rebreathing techniques can also be useful. Place a paper bag over the patient's mouth and ask him or her to breath in and out through the mouth. A connected but not switched on oxygen or nebulizer mask is an alternative in the surgery. This raises the partial pressure of carbon dioxide in the blood and symptoms due to low partial pressure of carbon dioxide, such as tetany, paraesthesiae and dizziness, resolve. This also demonstrates the link between hyperventilation and symptoms.
Propranolol, 10–20 mg stat, may also be helpful. However, never give propranolol to patients who are asthmatic, patients with heart failure or those on verapamil.
Follow up the patient after recovery to explore the reasons for the panic attacks. Treat any depression or anxiety disorders.
Key points
Acute breathlessness is defined as severe dyspnoea evolving rapidly over minutes to hours. The sudden development of dyspnoea heralds, in most cases, a significant cardiopulmonary insult. In all cases, either arrange to see the patient or call for emergency ambulance assistance Whenever you are assessing a breathless patient, it is important to be calm and reassuring — breathlessness is very frightening and panic only adds to the sensation of being breathless. Direct the history and examination to finding the cause as quickly as possible. Treat the patient according to the cause. If no cause can be found and the patient is acutely and significantly breathless, do not delay and admit to hospital as an acute medical emergency.